
Bacteraemia Is Associated with Increased ICU Mortality in the Postoperative Course of Lung Transplantation

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
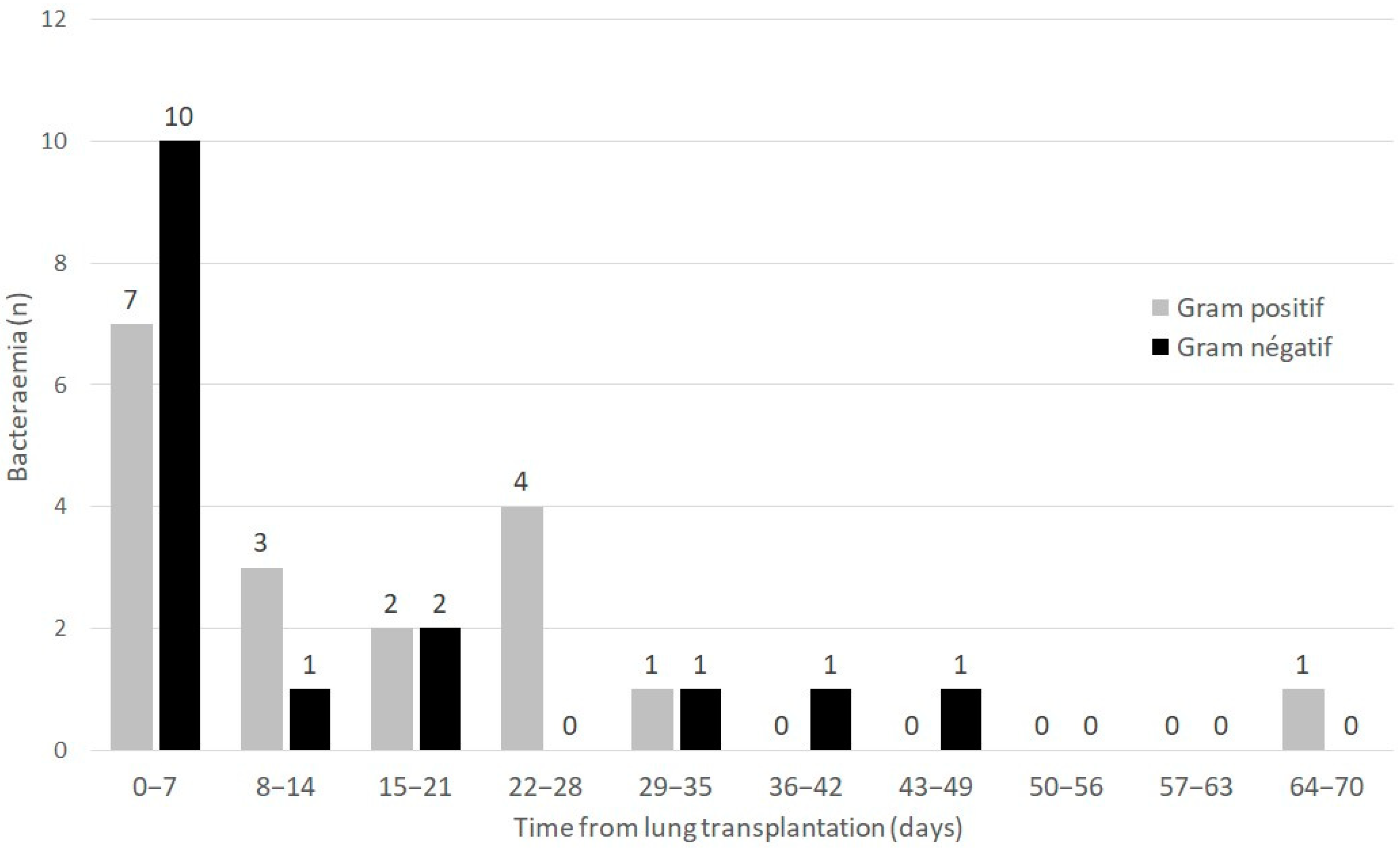
2.1. Prevalence of Bacteraemia and Characteristics
2.2. Pre-Existing Risk Factors at ICU Admission Associated with the Occurrence of Bacteraemia during the Postoperative ICU Stay
2.3. ICU Morbidity Associated with the Occurrence of Bacteraemia
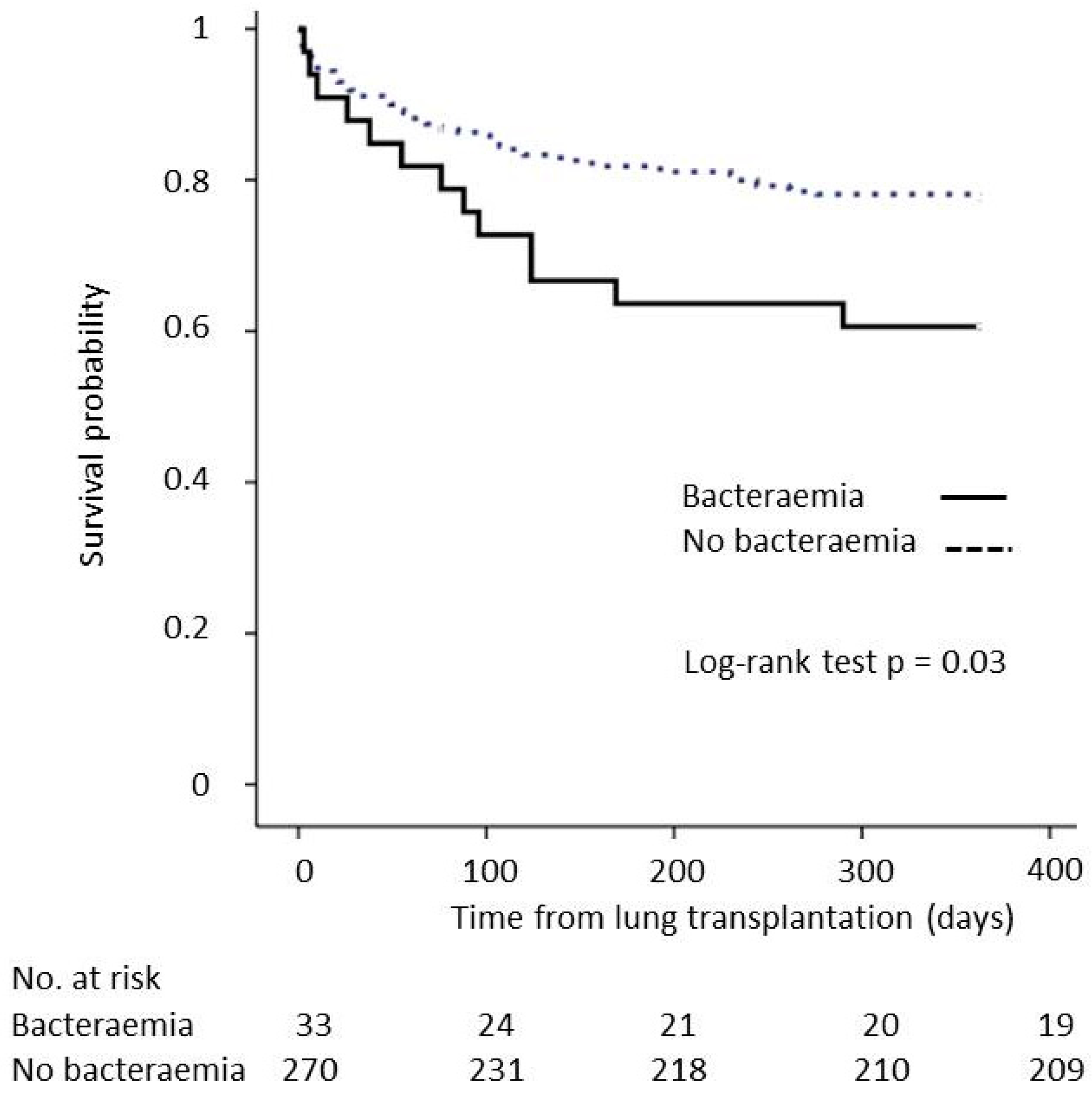
2.4. ICU and One-Year Mortality Rates Associated with the Occurrence of Bacteraemia
2.5. Impact of the Adequacy of 48 h Perioperative ABX to Bacteraemia Occurring during the First Week after LT on ICU Morbidity and Mortality
2.6. Comparison of ICU Morbidity and Mortality between Patients with Postoperative Bacteraemia Occurrence before 7 Days vs. after 7 Days
2.7. Comparison of ICU Morbidity and Mortality between Patients with Gram-Positive vs. Gram-Negative Postoperative Bacteraemia
2.8. Impact of Multidrug-Resistant Isolates on ICU Mortality of Recipients with Bacteraemia
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Microbiological Features and Definitions
4.3. Data Collection
- All positive blood cultures drawn during the posttransplant ICU stay; the time from LT to onset of bacteraemia, the type of bacterial species and the presence of MDR profiles were recorded [25].
- The demographic and pre-existing characteristics of patients before postoperative ICU admission, including the following: age, sex, body mass index (BMI), primary diagnosis of chronic pulmonary disease, cytomegalovirus mismatch (recipient/donor+), past medical history of diabetes and revascularized ischaemic heart disease, high-emergency LT, extracorporeal membrane oxygenation (ECMO) as a bridge to transplant and mean pulmonary arterial pressure (mPAP) measured by a right-heart catheterization at listing. High-emergency LT is a national prioritization system for the most severe patients with fibrosis, cystic fibrosis or pulmonary hypertension that was introduced in France in 2007 [26].
- Intraoperative characteristics: type of LT (i.e., single or bilateral), maximum graft cold ischaemic time, intraoperative blood transfusion of more than three packed red blood cells (PRBC) and intraoperative ECMO.
- Postoperative outcomes in ICU: simplified acute physiology score II (SAPS II) and sequential organ failure assessment (SOFA) score at ICU admission, acute kidney injury stage 3 of KDIGO (Kidney Disease: Improving Global Outcomes), renal replacement therapy, duration of mechanical ventilation, duration of norepinephrine support, ECMO in ICU, tracheotomy, ICU length of stay and mortality rates at day 30 and 1 year.
4.4. Perioperative Management
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chambers, D.C.; Cherikh, W.S.; Harhay, M.O.; Hayes, D.; Hsich, E.; Khush, K.K.; Meiser, B.; Potena, L.; Rossano, J.W.; Toll, A.E.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-Sixth Adult Lung and Heart-Lung Transplantation Report-2019; Focus Theme: Donor and Recipient Size Match. J. Heart Lung Transplant. 2019, 38, 1042–1055. [Google Scholar] [CrossRef]
- Goto, M.; Al-Hasan, M.N. Overall Burden of Bloodstream Infection and Nosocomial Bloodstream Infection in North America and Europe. Clin. Microbiol. Infect. 2013, 19, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Kritikos, A.; Manuel, O. Bloodstream Infections after Solid-Organ Transplantation. Virulence 2016, 7, 329–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, S.; Chan, K.M.; Palmer, S.M.; Hadjiliadis, D.; Humar, A.; McCurry, K.R.; Wagener, M.M.; Singh, N. Bacteremia in Lung Transplant Recipients in the Current Era. Am. J. Transplant. 2006, 6, 3000–3007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, S.M.; Alexander, B.D.; Sanders, L.L.; Edwards, L.J.; Reller, L.B.; Davis, R.D.; Tapson, V.F. Significance of Blood Stream Infection after Lung Transplantation: Analysis in 176 Consecutive Patients. Transplantation 2000, 69, 2360–2366. [Google Scholar] [CrossRef] [PubMed]
- Moreno, A.; Cervera, C.; Gavaldá, J.; Rovira, M.; de la Cámara, R.; Jarque, I.; Montejo, M.; de la Torre-Cisneros, J.; Miguel Cisneros, J.; Fortún, J.; et al. Bloodstream Infections among Transplant Recipients: Results of a Nationwide Surveillance in Spain. Am. J. Transplant. 2007, 7, 2579–2586. [Google Scholar] [CrossRef]
- Nosotti, M.; Tarsia, P.; Morlacchi, L.C. Infections after Lung Transplantation. J. Thorac. Dis. 2018, 10, 3849–3868. [Google Scholar] [CrossRef]
- Snell, G.I.; Yusen, R.D.; Weill, D.; Strueber, M.; Garrity, E.; Reed, A.; Pelaez, A.; Whelan, T.P.; Perch, M.; Bag, R.; et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, Part I: Definition and Grading—A 2016 Consensus Group Statement of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2017, 36, 1097–1103. [Google Scholar] [CrossRef]
- Crespo, M.M.; McCarthy, D.P.; Hopkins, P.M.; Clark, S.C.; Budev, M.; Bermudez, C.A.; Benden, C.; Eghtesady, P.; Lease, E.D.; Leard, L.; et al. ISHLT Consensus Statement on Adult and Pediatric Airway Complications after Lung Transplantation: Definitions, Grading System, and Therapeutics. J. Heart Lung Transplant. 2018, 37, 548–563. [Google Scholar] [CrossRef] [Green Version]
- Prowle, J.R.; Echeverri, J.E.; Ligabo, E.V.; Sherry, N.; Taori, G.C.; Crozier, T.M.; Hart, G.K.; Korman, T.M.; Mayall, B.C.; Johnson, P.D.R.; et al. Acquired Bloodstream Infection in the Intensive Care Unit: Incidence and Attributable Mortality. Crit. Care 2011, 15, R100. [Google Scholar] [CrossRef]
- Pittet, D.; Tarara, D.; Wenzel, R.P. Nosocomial Bloodstream Infection in Critically Ill Patients. Excess Length of Stay, Extra Costs, and Attributable Mortality. JAMA 1994, 271, 1598–1601. [Google Scholar] [CrossRef] [PubMed]
- Magret, M.; Lisboa, T.; Martin-Loeches, I.; Máñez, R.; Nauwynck, M.; Wrigge, H.; Cardellino, S.; Díaz, E.; Koulenti, D.; Rello, J.; et al. Bacteremia Is an Independent Risk Factor for Mortality in Nosocomial Pneumonia: A Prospective and Observational Multicenter Study. Crit. Care 2011, 15, R62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kraker, M.E.A.; Jarlier, V.; Monen, J.C.M.; Heuer, O.E.; van de Sande, N.; Grundmann, H. The Changing Epidemiology of Bacteraemias in Europe: Trends from the European Antimicrobial Resistance Surveillance System. Clin. Microbiol. Infect. 2013, 19, 860–868. [Google Scholar] [CrossRef] [Green Version]
- Dantes, R.; Mu, Y.; Belflower, R.; Aragon, D.; Dumyati, G.; Harrison, L.H.; Lessa, F.C.; Lynfield, R.; Nadle, J.; Petit, S.; et al. National Burden of Invasive Methicillin-Resistant Staphylococcus Aureus Infections, United States, 2011. JAMA Intern. Med. 2013, 173, 1970–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.Y.; Mojica, N.; Jiang, W.; Cosgrove, S.E.; Septimus, E.; Morgan, D.J.; Laxminarayan, R. Trends in Methicillin-Resistant Staphylococcus Aureus Hospitalizations in the United States, 2010–2014. Clin. Infect. Dis. 2017, 65, 1921–1923. [Google Scholar] [CrossRef] [Green Version]
- Giacobbe, D.R.; Giani, T.; Bassetti, M.; Marchese, A.; Viscoli, C.; Rossolini, G.M. Rapid Microbiological Tests for Bloodstream Infections Due to Multidrug Resistant Gram-Negative Bacteria: Therapeutic Implications. Clin. Microbiol. Infect. 2020, 26, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Salimnia, H.; Fairfax, M.R.; Lephart, P.R.; Schreckenberger, P.; DesJarlais, S.M.; Johnson, J.K.; Robinson, G.; Carroll, K.C.; Greer, A.; Morgan, M.; et al. Evaluation of the FilmArray Blood Culture Identification Panel: Results of a Multicenter Controlled Trial. J. Clin. Microbiol. 2016, 54, 687–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, R.; Komarow, L.; Virk, A.; Rajapakse, N.; Schuetz, A.N.; Dylla, B.; Earley, M.; Lok, J.; Kohner, P.; Ihde, S.; et al. Randomized Trial Evaluating Clinical Impact of RAPid IDentification and Susceptibility Testing for Gram-Negative Bacteremia: RAPIDS-GN. Clin. Infect. Dis. 2021, 73, e39–e46. [Google Scholar] [CrossRef]
- Desmard, M.; Benbara, A.; Boudinet, S.; Mal, H.; Dehoux, M.; Thabut, G.; Montravers, P. Post-Operative Kinetics of Procalcitonin after Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 189–194. [Google Scholar] [CrossRef]
- EUCAST: Disk Diffusion Methodology. Available online: https://www.eucast.org/ast_of_bacteria/disk_diffusion_methodology (accessed on 12 September 2022).
- Gajic, I.; Kabic, J.; Kekic, D.; Jovicevic, M.; Milenkovic, M.; Mitic Culafic, D.; Trudic, A.; Ranin, L.; Opavski, N. Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics 2022, 11, 427. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Bloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-Central Line Associated Bloodstream Infection), National Healthcare Safety Network, January 2022. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf (accessed on 12 September 2022).
- Weinstein, M.P.; Towns, M.L.; Quartey, S.M.; Mirrett, S.; Reimer, L.G.; Parmigiani, G.; Reller, L.B. The Clinical Significance of Positive Blood Cultures in the 1990s: A Prospective Comprehensive Evaluation of the Microbiology, Epidemiology, and Outcome of Bacteremia and Fungemia in Adults. Clin. Infect. Dis. 1997, 24, 584–602. [Google Scholar] [CrossRef] [PubMed]
- Al-Hasan, M.N.; Eckel-Passow, J.E.; Baddour, L.M. Recurrent Gram-Negative Bloodstream Infection: A 10-Year Population-Based Cohort Study. J. Infect. 2010, 61, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boussaud, V.; Mal, H.; Trinquart, L.; Thabut, G.; Danner-Boucher, I.; Dromer, C.; Raymond, C.S.; Reynaud-Gaubert, M.; Kessler, R.; Philit, F.; et al. One-Year Experience With High-Emergency Lung Transplantation in France. Transplantation 2012, 93, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery. Am. J. Health-Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [Green Version]
- Abbo, L.M.; Grossi, P.A.; The AST ID Community of Practice. Surgical Site Infections: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13589. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Patients (n = 303) | No Bacteraemia (n = 270) | Bacteraemia (n = 33) | Univariate Analysis OR [CI 95%] | p | |
|---|---|---|---|---|---|
| Demographics and preoperative characteristics | |||||
| Age, years | 57 (51–63) | 57 (51–63) | 55 (47–58) | 0.98 (0.95–1.01) | 0.13 |
| Male sex | 197 (65%) | 176 (65.2) | 21 (63.6) | 0.94 (0.44–1.98) | 0.86 |
| BMI, kg/m2 | 24 (20–27) | 24 (20–27) | 26 (22–29) | 1.07 (0.98–1.16) | 0.12 |
| Primary diagnosis | |||||
| COPD | 105 (34.7) | 98 (36.3) | 7 (21.2) | 0.47 (0.20–1.13) | 0.09 |
| ILD | 153 (50.5) | 133 (49.3) | 20 (60.6) | 1.59 (0.76–3.31) | 0.22 |
| Other | 46 (15.2) | 40 (14.8) | 6 (18.2) | 1.28 (0.50–3.29) | 0.61 |
| Revascularized ischaemic heart disease | 17 (5.6) | 16 (5.9) | 1 (3.0) | 0.50 (0.06–3.87) | 0.71 |
| Diabetes | 34 (11.2) | 29 (10.7) | 5 (15.2) | 1.48 (0.53–4.14) | 0.45 |
| mPAP, mmHg | 25 (20–30) | 25 (20–30) | 24 (17–29) | 0.96 (0.95–1.05) | 0.84 |
| Mismatch CMV (R−/D+) | 57 (18.8) | 50 (18.5) | 7 (21.2) | 1.19 (0.49–2.88) | 0.78 |
| Preoperative ECMO | 23 (7.6) | 19 (7.0) | 4 (12.1) | 1.82 (0.58–5.72) | 0.30 |
| High-emergency LT | 54 (17.8) | 48 (17.8) | 6 (18.2) | 1.03 (0.40–2.63) | 0.96 |
| Intraoperative characteristics | |||||
| Double LT | 202 (66.7) | 178 (65.9) | 24 (72.7) | 1.38 (0.62–3.09) | 0.43 |
| Thoracic epidural analgesia | 170 (56.1) | 154 (57.0) | 16 (48.5) | 0.71 (0.34–1.46) | 0.35 |
| Maximum cold graft ischaemic time, min | 330 (270–400) | 335 (270–400) | 330 (260–410) | 1.01 (0.98–1.05) | 0.43 |
| Intraoperative ECMO | 211 (69.6) | 184 (68.1) | 27 (81.8) | 2.10 (0.84–5.28) | 0.11 |
| Transfusion ≥ 3 PRBCs | 138 (45.5) | 120 (44.4) | 18 (54.5) | 1.50 (0.73–3.10) | 0.27 |
| Pneumonia | Pleural Infection | Chest Wall Infection | Intra-Abdominal Infection | Other | Unknown | Total (Bacteria) | ||
|---|---|---|---|---|---|---|---|---|
| Gram-negative bacilli | ||||||||
| Non-fermenting GNB | ||||||||
| Pseudomonas aeruginosa | 4 | 1 | 1 | - | 1 | - | 7 | |
| Pseudomonas putida | - | - | - | - | - | 1 | 1 | |
| Stenotrophomonas maltophilia | 1 | - | - | - | - | - | 1 | |
| Achromobacter xylosoxidans | 1 | - | - | - | - | - | 1 | |
| Enterobacterales | ||||||||
| Enterobacter cloacae | 1 | - | - | - | 1 | - | 2 | |
| Klebsiella pneumoniae | 3 | 1 | - | - | - | - | 3 | |
| Escherichia coli | - | 1 | - | 1 | - | - | 2 | |
| Proteus mirabilis | 1 | - | - | - | - | 1 | 2 | |
| Klebsiella aerogenes | 1 | - | - | - | - | 1 | 2 | |
| Anaerobes | ||||||||
| Bacteroides thetaiotaomicron | - | - | - | - | - | 1 | 1 | |
| Gram-positive cocci | ||||||||
| Staphylococcus aureus | 6 | - | - | - | 1 | 1 | 8 | |
| Staphylococcus epidermidis | - | 1 | - | 1 | - | - | 2 | |
| Staphylococcus haemolyticus | - | - | - | - | - | 2 | 2 | |
| Staphylococcus lugdunensis | 1 | - | - | - | - | - | 1 | |
| Enterococcus faecium | - | 1 | 1 | 1 | - | 5 | 7 | |
| Enterococcus faecalis | - | - | - | 1 | - | 3 | 4 | |
| Total (source) | 18 | 5 | 2 | 4 | 3 | 15 | 46 | |
| 47 | ||||||||
| Total Patients (n = 303) | No Bacteraemia (n = 270) | Bacteraemia (n = 33) | Univariate Analysis OR [CI 95%] | p | |
|---|---|---|---|---|---|
| At ICU admission | |||||
| SAPS II | 43 (38–50) | 43 (38–50) | 45 (42–55) | 1.03 (1–1.05) | 0.04 |
| SOFA score | 7 (6–9) | 7 (6–9) | 8 (6–10) | 1.14 (0.98–1.33) | 0.08 |
| During the ICU stay | |||||
| AKI stage 3 of KDIGO | 48 (15.8) | 37 (13.7) | 11 (33.3) | 3.15 (1.41–7.03) | 0.004 |
| RRT | 38 (12.5) | 29 (10.7) | 9 (27.3) | 3.12 (1.32–7.35) | 0.007 |
| Duration of mechanical ventilation, days | 3 (1–21) | 3 (1–13) | 30 (3–49) | 1.02 (1.01–1.03) | <0.001 |
| Duration of noradrenaline support, days | 2 (1–4) | 2 (1–4) | 4 (1–13) | 1.05 (1.01–1.09) | 0.01 |
| ECMO in ICU | 83 (27.4) | 70 (25.9) | 13 (39.3) | 1.86 (0.88–3.93) | 0.10 |
| Tracheotomy | 82 (27.1) | 59 (21.9) | 23 (69.7) | 8.26 (3.71–18.24) | <0.001 |
| ICU length of stay, days | 17 (11–35) | 16 (11–28) | 42 (20–88) | 1.03 (1.02–1.04) | <0.001 |
| ICU mortality | 46 (15.2) | 34 (12.6) | 12 (36.4) | 3.97 (1.79–8.79) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran-Dinh, A.; Guiot, M.; Tanaka, S.; Lortat-Jacob, B.; Atchade, E.; Zappella, N.; Mordant, P.; Castier, Y.; Mal, H.; Weisenburger, G.; et al. Bacteraemia Is Associated with Increased ICU Mortality in the Postoperative Course of Lung Transplantation. Antibiotics 2022, 11, 1405. https://doi.org/10.3390/antibiotics11101405
Tran-Dinh A, Guiot M, Tanaka S, Lortat-Jacob B, Atchade E, Zappella N, Mordant P, Castier Y, Mal H, Weisenburger G, et al. Bacteraemia Is Associated with Increased ICU Mortality in the Postoperative Course of Lung Transplantation. Antibiotics. 2022; 11(10):1405. https://doi.org/10.3390/antibiotics11101405
Chicago/Turabian StyleTran-Dinh, Alexy, Marion Guiot, Sébastien Tanaka, Brice Lortat-Jacob, Enora Atchade, Nathalie Zappella, Pierre Mordant, Yves Castier, Hervé Mal, Gaelle Weisenburger, and et al. 2022. "Bacteraemia Is Associated with Increased ICU Mortality in the Postoperative Course of Lung Transplantation" Antibiotics 11, no. 10: 1405. https://doi.org/10.3390/antibiotics11101405