

Pragmatic Comparison of Piperacillin/Tazobactam versus Carbapenems in Treating Patients with Nosocomial Pneumonia Caused by Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. ESBL-Producing K. pneumoniae Nosocomial Pneumonia
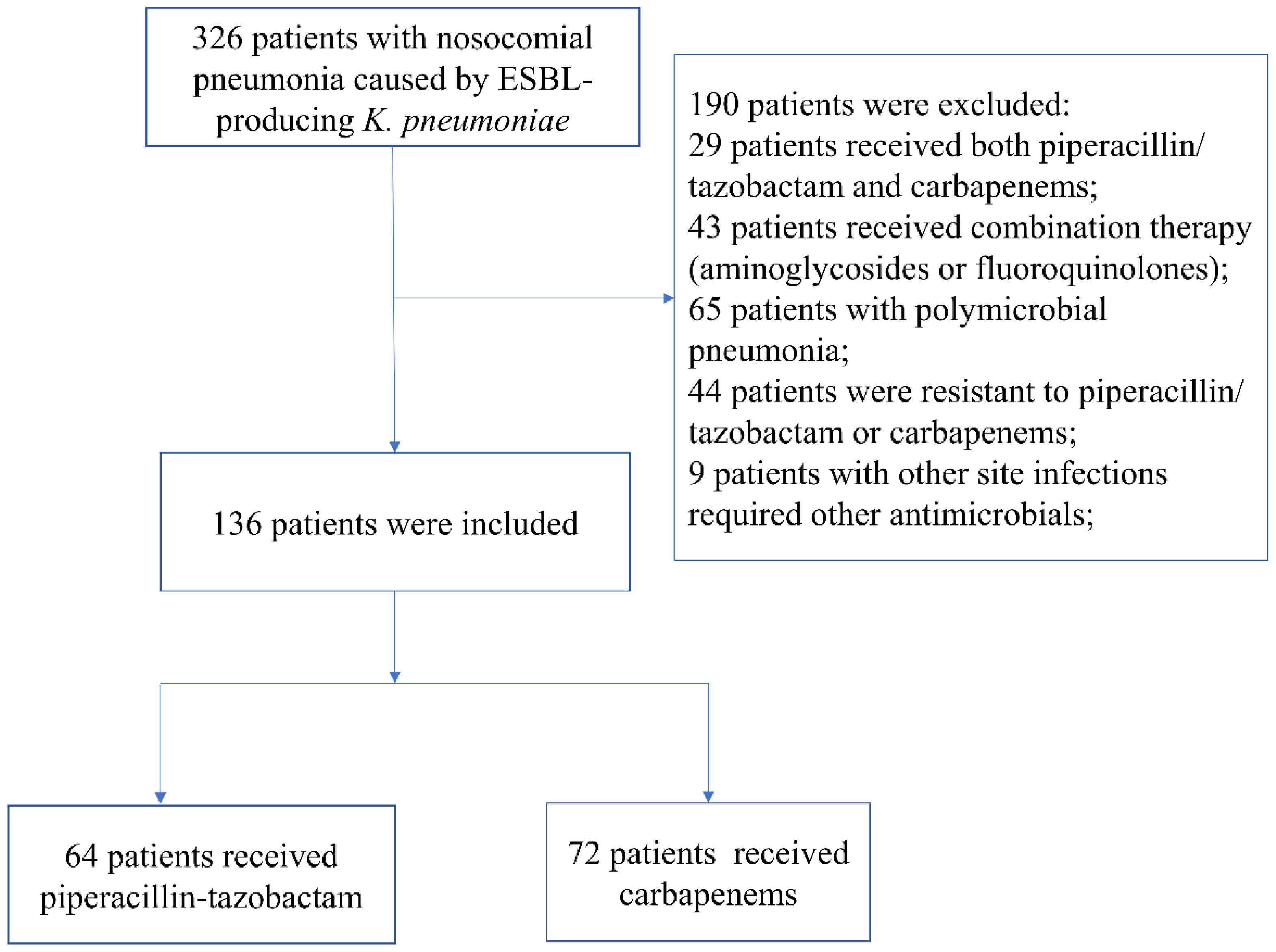
2.3. Participants
2.4. Outcomes and Definitions
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
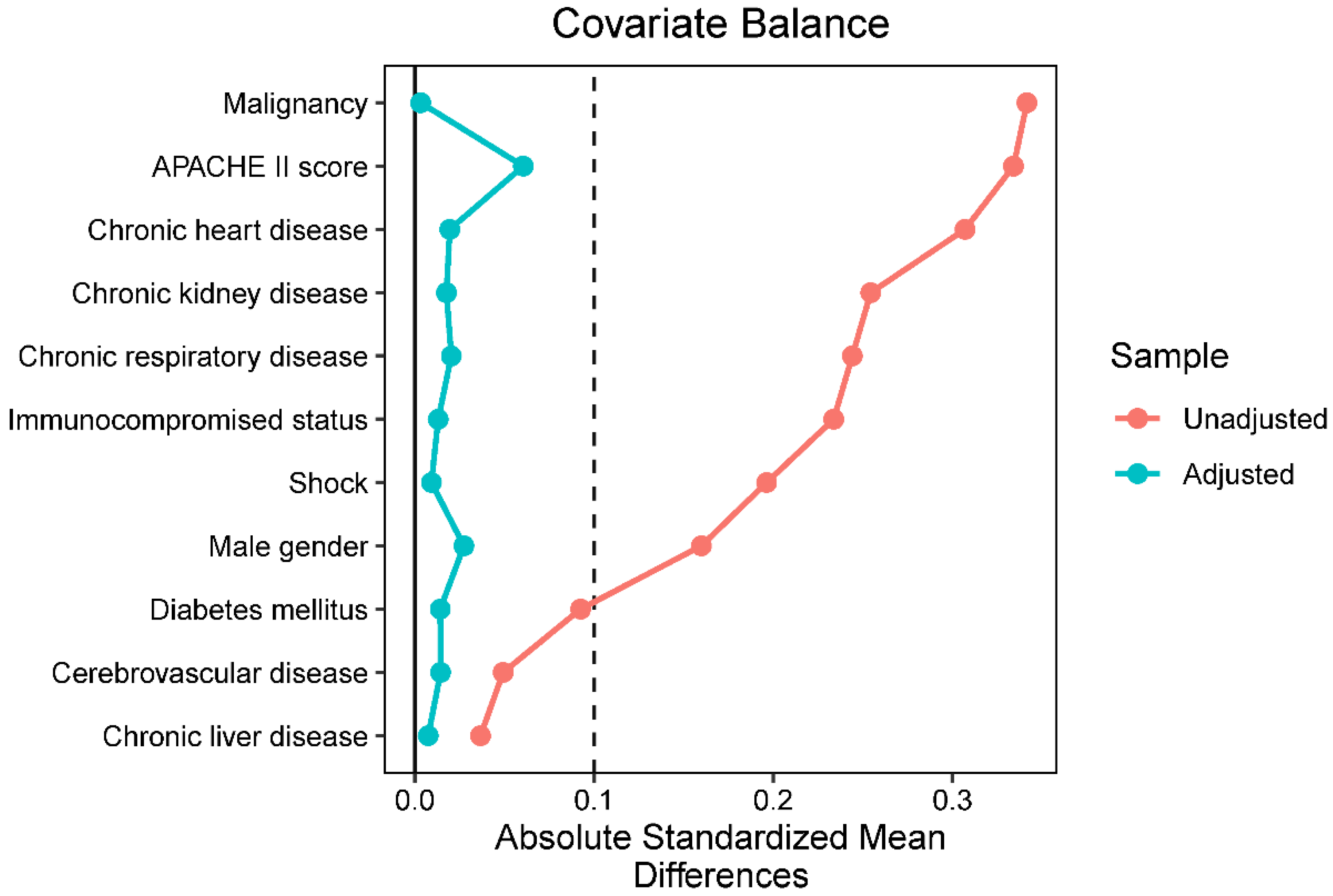
3.2. Inverse Probability of Treatment Weighted Cohort
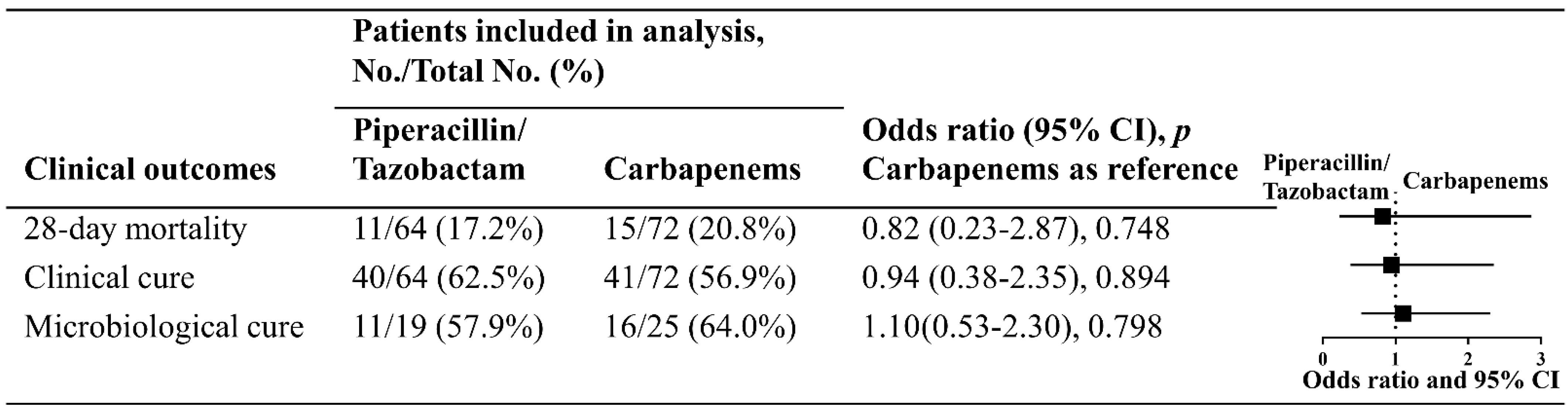
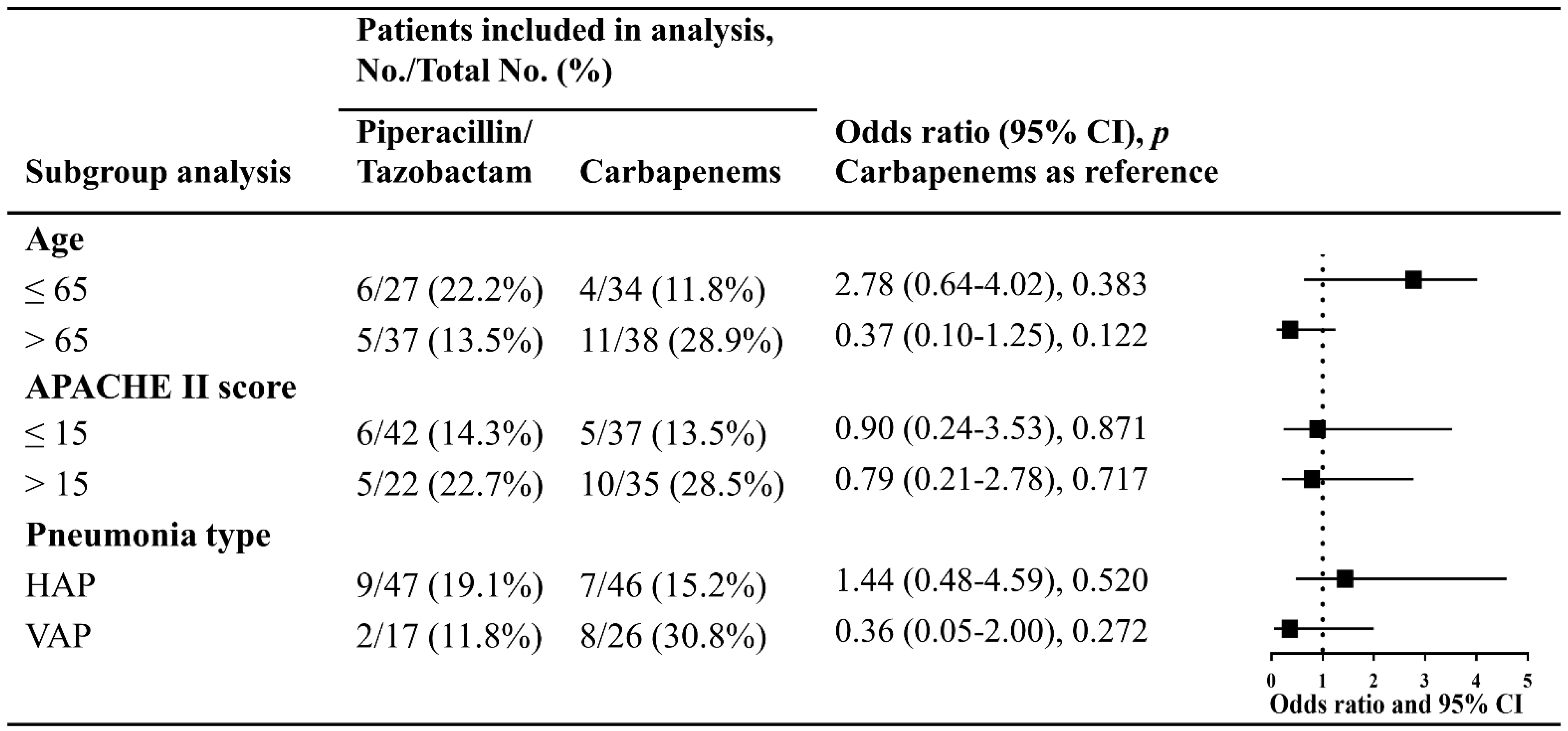
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castanheira, M.; Simner, P.J.; Bradford, P.A. Extended-spectrum β-lactamases: An update on their characteristics, epidemiology and detection. JAC-Antimicrobial Resist. 2021, 3, dlab092. [Google Scholar] [CrossRef] [PubMed]
- Pitout, J.D.; Laupland, K.B. Extended-spectrum β-lactamase-producing Enterobacteriaceae: An emerging public-health concern. Lancet Infect. Dis. 2008, 8, 159–166. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report 2019; ECDC: Stockholm, Sweden, 2020.
- Yang, Y.; Guo, Y.; Yin, D.; Zheng, Y.; Wu, S.; Zhu, D.; Hu, F. In Vitro Activity of Cefepime-Zidebactam, Ceftazidime-Avibactam, and Other Comparators against Clinical Isolates of Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter baumannii: Results from China Antimicrobial Surveillance Network (CHINET) in 2018. Antimicrob. Agents Chemother. 2020, 65, e01726-20. [Google Scholar] [CrossRef] [PubMed]
- Ling, W.; Furuya-Kanamori, L.; Ezure, Y.; Harris, P.N.A.; Paterson, D.L. Adverse clinical outcomes associated with infections by Enterobacterales producing ESBL (ESBL-E): A systematic review and meta-analysis. JAC-Antimicrob. Resist. 2021, 3, dlab068. [Google Scholar] [CrossRef]
- Shamsrizi, P.; Gladstone, B.P.; Carrara, E.; Luise, D.; Cona, A.; Bovo, C.; Tacconelli, E. Variation of effect estimates in the analysis of mortality and length of hospital stay in patients with infections caused by bacteria-producing extended-spectrum beta-lactamases: A systematic review and meta-analysis. BMJ Open 2020, 10, e030266. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2021, 72, 1109–1116. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults eith Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, M.; Giacobbe, D.R.; Robba, C.; Pelosi, P.; Vena, A. Treatment of extended-spectrum β-lactamases infections: What is the current role of new β-lactams/β-lactamase inhibitors? Curr. Opin. Infect. Dis. 2020, 33, 474–481. [Google Scholar] [CrossRef]
- Peirano, G.; Pitout, J.D.D. Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae: Update on Molecular Epidemiology and Treatment Options. Drugs 2019, 79, 1529–1541. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; Rodríguez-Baño, J. Current options for the treatment of infections due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in different groups of patients. Clin. Microbiol. Infect. 2019, 25, 932–942. [Google Scholar] [CrossRef]
- Belley, A.; Morrissey, I.; Hawser, S.; Kothari, N.; Knechtle, P. Third-generation cephalosporin resistance in clinical isolates of Enterobacterales collected between 2016–2018 from USA and Europe: Genotypic analysis of β-lactamases and comparative in vitro activity of cefepime/enmetazobactam. J. Glob. Antimicrob. Resist. 2021, 25, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.Q.; Li, Y.; Lv, Y.; Xue, F.; Liu, J.; Yang, W.W.; Zhang, J. Antimicrobial susceptibility surveillance of moxalactam against Enterobacteriaceae in China from 2004 to 2014. Chin. J. Clin. Pharmacol. 2016, 32, 813–817. [Google Scholar]
- Gandra, S.; Burnham, C.-A.D. Carbapenem-resistant Enterobacterales in the USA. Lancet Infect. Dis. 2020, 20, 637–639. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Q.; Yin, Y.; Chen, H.; Jin, L.; Gu, B.; Xie, L.; Yang, C.; Ma, X.; Li, H.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae Infections: Report from the China CRE Network. Antimicrob. Agents Chemother. 2018, 62, e01882-17. [Google Scholar] [CrossRef] [Green Version]
- Aslan, A.T.; Akova, M. Extended spectrum β-lactamase producing enterobacteriaceae: Carbapenem sparing options. Expert Rev. Anti-Infect. Ther. 2019, 17, 969–981. [Google Scholar] [CrossRef]
- Zhang, H.; Liang, B.; Wang, J.; Cai, Y. Non-carbapenem β-lactam/β-lactamase inhibitors versus carbapenems for urinary tract infections caused by extended-spectrum β-lactamase-producing Enterobacteriaceae: A systematic review. Int. J. Antimicrob. Agents 2021, 58, 106410. [Google Scholar] [CrossRef]
- Sharara, S.L.; Amoah, J.; Pana, Z.D.; Simner, P.J.; Cosgrove, S.E.; Tamma, P.D. Is Piperacillin-Tazobactam Effective for the Treatment of Pyelonephritis Caused by Extended-Spectrum β-Lactamase–Producing Organisms? Clin. Infect. Dis. 2019, 71, e331–e337. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Kim, J.H.; Sohn, J.W.; Yang, K.S.; Kim, M.J. Role of piperacillin/tazobactam as a carbapenem-sparing antibiotic for treatment of acute pyelonephritis due to extended-spectrum β-lactamase-producing Escherichia coli. Int. J. Antimicrob. Agents 2017, 49, 410–415. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; Pérez-Galera, S.; Salamanca, E.; de Cueto, M.; Calbo, E.; Almirante, B.; Viale, P.; Oliver, A.; Pintado, V.; Gasch, O.; et al. A Multinational, Preregistered Cohort Study of β-Lactam/β-Lactamase Inhibitor Combinations for Treatment of Bloodstream Infections Due to Extended-Spectrum-β-Lactamase-Producing Enterobacteriaceae. Antimicrob. Agents Chemother. 2016, 60, 4159–4169. [Google Scholar] [CrossRef] [Green Version]
- Henderson, A.; Paterson, D.L.; Chatfield, M.D.; Tambyah, P.A.; Lye, D.C.; De, P.P.; Lin, R.T.P.; Chew, K.L.; Yin, M.; Lee, T.H.; et al. Association Between Minimum Inhibitory Concentration, Beta-lactamase Genes and Mortality for Patients Treated with Piperacillin/Tazobactam or Meropenem from the MERINO Study. Clin. Infect. Dis. 2020, 73, e3842–e3850. [Google Scholar] [CrossRef]
- John, R.; Colley, P.; Nguyen, H.L.; Berhe, M. Outcomes analysis in patients with extended-spectrum beta-lactamase bacteremia empirically treated with piperacillin/tazobactam versus carbapenems. Bayl. Univ. Med. Cent. Proc. 2019, 32, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.-H.; Lee, N.R.; Joo, E.-J.; Moon, S.-Y.; Choi, J.-K.; Park, D.A.; Peck, K.R. Appropriate non-carbapenems are not inferior to carbapenems as initial empirical therapy for bacteremia caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae: A propensity score weighted multicenter cohort study. Eur. J. Clin. Microbiol. 2017, 37, 305–311. [Google Scholar] [CrossRef]
- Nasir, N.; Ahmed, S.; Razi, S.; Awan, S.; Mahmood, S.F. Risk factors for mortality of patients with ceftriaxone resistant E. coli bacteremia receiving carbapenem versus beta lactam/beta lactamase inhibitor therapy. BMC Res. Notes 2019, 12, 611. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Han, J.; Rock, C.; Harris, A.D.; Lautenbach, E.; Hsu, A.J.; Avdic, E.; Cosgrove, S.E.; for the Antibacterial Resistance Leadership Group. Carbapenem Therapy Is Associated with Improved Survival Compared with Piperacillin-Tazobactam for Patients with Extended-Spectrum-Lactamase Bacteremia. Clin. Infect. Dis. 2015, 60, 1319–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ofer-Friedman, H.; Shefler, C.; Sharma, S.; Tirosh, A.; Tal-Jasper, R.; Kandipalli, D.; Sharma, S.; Bathina, P.; Kaplansky, T.; Maskit, M.; et al. Carbapenems Versus Piperacillin-Tazobactam for Bloodstream Infections of Nonurinary Source Caused by Extended-Spectrum Beta-Lactamase–Producing Enterobacteriaceae. Infect. Control Hosp. Epidemiol. 2015, 36, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.N.A.; Tambyah, P.A.; Lye, D.C.; Mo, Y.; Lee, T.H.; Yilmaz, M.; Alenazi, T.H.; Arabi, Y.; Falcone, M.; Bassetti, M.; et al. Effect of Piperacillin-Tazobactam vs Meropenem on 30-Day Mortality for Patients with E coli or Klebsiella pneumoniae Bloodstream Infection and Ceftriaxone Resistance: A Randomized Clinical Trial. JAMA 2018, 320, 984–994. [Google Scholar] [CrossRef] [Green Version]
- Son, S.K.; Lee, N.R.; Ko, J.-H.; Choi, J.K.; Moon, S.-Y.; Joo, E.J.; Peck, K.R.; Park, D.A. Clinical effectiveness of carbapenems versus alternative antibiotics for treating ESBL-producing Enterobacteriaceae bacteraemia: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2018, 73, 2631–2642. [Google Scholar] [CrossRef]
- Sfeir, M.M.; Askin, G.; Christos, P. Beta-lactam/beta-lactamase inhibitors versus carbapenem for bloodstream infections due to extended-spectrum beta-lactamase-producing Enterobacteriaceae: Systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 52, 554–570. [Google Scholar] [CrossRef]
- Magill, S.S.; Klompas, M.; Balk, R.; Burns, S.M.; Deutschman, C.S.; Diekema, D.; Fridkin, S.; Greene, L.; Guh, A.; Gutterman, D.; et al. Developing a New, National Approach to Surveillance for Ventilator-Associated Events. Crit. Care Med. 2013, 41, 2467–2475. [Google Scholar] [CrossRef]
- EUCAST. Breakpoint Tables for Interpretation of Mics and Zone Diameters, Version 9.0; EUCAST: Växjö, Sweden, 2019. [Google Scholar]
- Spanu, T.; Sanguinetti, M.; Tumbarello, M.; D’Inzeo, T.; Fiori, B.; Posteraro, B.; Santangelo, R.; Cauda, R.; Fadda, G. Evaluation of the New VITEK 2 Extended-Spectrum Beta-Lactamase (ESBL) Test for Rapid Detection of ESBL Production in Enterobacteriaceae Isolates. J. Clin. Microbiol. 2006, 44, 3257–3262. [Google Scholar] [CrossRef] [Green Version]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; 24th Informational Supplement; CLSI: Wayne, PA, USA, 2017. [Google Scholar]
- Niewiński, G.; Starczewska, M.; Kański, A. Prognostic scoring systems for mortality in intensive care units—The APACHE model. Anaesthesiol. Intensive Ther. 2014, 46, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Huang, Y.; Zhang, T.-T.; Cao, B.; Wang, H.; Zhuo, C.; Ye, F.; Su, X.; Fan, H.; Xu, J.-F.; et al. Chinese guidelines for the diagnosis and treatment of hospital-acquired pneumonia and ventilator-associated pneumonia in adults (2018 Edition). J. Thorac. Dis. 2019, 11, 2581–2616. [Google Scholar] [CrossRef]
- Kyriacou, D.N.; Lewis, R.J. Confounding by Indication in Clinical Research. JAMA 2016, 316, 1818–1819. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, N.; Marston, L.; Walters, K.; Wood, J.; Reynolds, M.R.; Petersen, I. Making inferences on treatment effects from real world data: Propensity scores, confounding by indication, and other perils for the unwary in observational research. BMJ 2013, 347, f6409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Pascual, A. CON: Carbapenems are NOT necessary for all infections caused by ceftriaxone-resistant Enterobacterales. JAC-Antimicrob. Resist. 2021, 3, dlaa112. [Google Scholar] [CrossRef]
- Paterson, D.L.; Isler, B.; Harris, P.N.A. PRO: Carbapenems should be used for ALL infections caused by ceftriaxone-resistant Enterobacterales. JAC-Antimicrob. Resist. 2021, 3, dlab013. [Google Scholar] [CrossRef]
- Karaiskos, I.; Giamarellou, H. Carbapenem-Sparing Strategies for ESBL Producers: When and How. Antibiotics 2020, 9, 61. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, A.N.; Reyes, S.; Tamma, P.D. Point-Counterpoint: Piperacillin-Tazobactam Should Be Used to Treat Infections with Extended-Spectrum-Beta-Lactamase-Positive Organisms. J. Clin. Microbiol. 2018, 56, e01917-17. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef] [Green Version]
- MacGowan, A. Breakpoints for extended-spectrum β-lactamase-producing Enterobacteriacae: Pharmacokinetic/pharmacodynamic considerations. Clin. Microbiol. Infect. 2008, 14 (Suppl. 1), 166–168. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Baño, J.; Navarro, M.D.; Retamar, P.; Picón, E.; Pascual, Á. Extended-Spectrum Beta-Lactamases–Red Española de Investigación en Patología Infecciosa/Grupo de Estudio de Infección Hospitalaria Group. β-Lactam/β-lactam inhibitor combinations for the treatment of bacteremia due to extended-spectrum β-lactamase-producing Escherichia coli: A post hoc analysis of prospective cohorts. Clin. Infect. Dis. 2012, 15, 167–174. [Google Scholar] [CrossRef]
- Harris, P.N.A.; Yin, M.; Jureen, R.; Chew, J.; Ali, J.; Paynter, S.; Paterson, D.L.; Tambyah, P.A. Comparable outcomes for β-lactam/β-lactamase inhibitor combinations and carbapenems in definitive treatment of bloodstream infections caused by cefotaxime-resistant Escherichia coli or Klebsiella pneumoniae. Antimicrob. Resist. Infect. Control 2015, 4, 14. [Google Scholar] [CrossRef] [Green Version]
- Lodise, T.P.; Lomaestro, B.; Rodvold, K.A.; Danziger, L.H.; Drusano, G.L. Pharmacodynamic Profiling of Piperacillin in the Presence of Tazobactam in Patients through the Use of Population Pharmacokinetic Models and Monte Carlo Simulation. Antimicrob. Agents Chemother. 2004, 48, 4718–4724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, M.G.; Thorsted, A.; Storgaard, M.; Kristoffersson, A.N.; Friberg, L.; Öbrink-Hansen, K. Population Pharmacokinetics of Piperacillin in Sepsis Patients: Should Alternative Dosing Strategies Be Considered? Antimicrob. Agents Chemother. 2018, 62, e02306-17. [Google Scholar] [CrossRef] [Green Version]
- Guet-Revillet, H.; Tomini, E.; Emirian, A.; Join-Lambert, O.; Lécuyer, H.; Zahar, J.-R.; Jullien, V. Piperacillin/tazobactam as an alternative antibiotic therapy to carbapenems in the treatment of urinary tract infections due to extended-spectrum β-lactamase-producing Enterobacteriaceae: An in silico pharmacokinetic study. Int. J. Antimicrob. Agents 2017, 49, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, E.; Spapen, H.; Piérard, D. Prolonged vs intermittent infusion of piperacillin/tazobactam in critically ill patients: A narrative and systematic review. J. Crit. Care 2014, 29, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, J.R.; Bulman, Z.P. Inoculum effect of β-lactam antibiotics. J. Antimicrob. Chemother. 2019, 74, 2825–2843. [Google Scholar] [CrossRef]
- Henderson, A.; Humphries, R. Building a Better Test for Piperacillin-Tazobactam Susceptibility Testing: Would that It Were So Simple (It’s Complicated). J. Clin. Microbiol. 2020, 58, e01649-19. [Google Scholar] [CrossRef] [Green Version]
- Livermore, D.M.; Day, M.; Cleary, P.; Hopkins, K.L.; Toleman, M.A.; Wareham, D.W.; Wiuff, C.; Doumith, M.; Woodford, N. OXA-1 β-lactamase and non-susceptibility to penicillin/β-lactamase inhibitor combinations among ESBL-producing Escherichia coli. J. Antimicrob. Chemother. 2019, 74, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Conen, A.; Frei, R.; Adler, H.; Dangel, M.; Fux, C.A.; Widmer, A.F. Microbiological Screening Is Necessary to Distinguish Carriers of Plasmid-Mediated AmpC Beta-Lactamase-Producing Enterobacteriaceae and Extended-Spectrum Beta-Lactamase (ESBL)-Producing Enterobacteriaceae because of Clinical Similarity. PLoS ONE 2015, 10, e0120688. [Google Scholar] [CrossRef]
- Meini, S.; Tascini, C.; Cei, M.; Sozio, E.; Rossolini, G.M. AmpC β-lactamase-producing Enterobacterales: What a clinician should know. Infection 2019, 47, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Arena, F.; Giani, T.; Becucci, E.; Conte, V.; Zanelli, G.; D’Andrea, M.M.; Buonocore, G.; Bagnoli, F.; Zanchi, A.; Montagnani, F.; et al. Large Oligoclonal Outbreak Due to Klebsiella pneumoniae ST14 and ST26 Producing the FOX-7 AmpC β-Lactamase in a Neonatal Intensive Care Unit. J. Clin. Microbiol. 2013, 51, 4067–4072. [Google Scholar] [CrossRef] [Green Version]
- Peter-Getzlaff, S.; Polsfuss, S.; Poledica, M.; Hombach, M.; Giger, J.; Böttger, E.C.; Zbinden, R.; Bloemberg, G.V. Detection of AmpC Beta-Lactamase in Escherichia coli: Comparison of Three Phenotypic Confirmation Assays and Genetic Analysis. J. Clin. Microbiol. 2011, 49, 2924–2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohlmann, R.; Bähr, T.; Gatermann, S.G. Species-specific mutation rates for ampC derepression in Enterobacterales with chromosomally encoded inducible AmpC β-lactamase. J. Antimicrob. Chemother. 2018, 73, 1530–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Nelson, B.C.; Mehta, M.; Seval, N.; Park, S.; Giddins, M.J.; Shi, Q.; Whittier, S.; Gomez-Simmonds, A.; Uhlemann, A.-C. Piperacillin-Tazobactam versus Other Antibacterial Agents for Treatment of Bloodstream Infections Due to AmpC β-Lactamase-Producing Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e00276-17. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.G.; Paterson, D.L.; Young, B.; Lye, D.C.; Davis, J.S.; Schneider, K.; Yilmaz, M.; Dinleyici, R.; Runnegar, N.; Henderson, A.; et al. Meropenem Versus Piperacillin-Tazobactam for Definitive Treatment of Bloodstream Infections Caused by AmpC β-Lactamase–Producing Enterobacter spp, Citrobacter freundii, Morganella morganii, Providencia spp, or Serratia marcescens: A Pilot Multicenter Randomized Controlled Trial (MERINO-2). Open Forum Infect. Dis. 2021, 8, ofab387. [Google Scholar] [CrossRef]
- Robin, F.; Delmas, J.; Schweitzer, C.; Bonnet, R. Evaluation of the Vitek-2 extended-spectrum β-lactamase test against non-duplicate strains of Enterobacteriaceae producing a broad diversity of well-characterised β-lactamases. Clin. Microbiol. Infect. 2008, 14, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Jean, S.-S.; Hsueh, P.-R.; SMART Asia-Pacific Group. Distribution of ESBLs, AmpC β-lactamases and carbapenemases among Enterobacteriaceae isolates causing intra-abdominal and urinary tract infections in the Asia-Pacific region during 2008–14: Results from the Study for Monitoring Antimicrobial Resistance Trends (SMART). J. Antimicrob. Chemother. 2017, 72, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.-H.; Handigund, M.; Hwang, J.-H.; Cho, Y.G.; Kim, D.S.; Lee, A.J. Clinical Features and Risk Factors Associated With 30-Day Mortality in Patients with Pneumonia Caused by Hypervirulent Klebsiella pneumoniae (hvKP). Ann. Lab. Med. 2020, 40, 481–487. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Original Cohort | Inverse Probability of Treatment Weighted Cohort | |||||
|---|---|---|---|---|---|---|---|
| Piperacillin/tazobactam, n = 64, 47% | Carbapenems, n = 72, 53% | p | Piperacillin/Tazobactam, 50.5% | Carbapenems, 49.5% | p | Standardized Mean Differences | |
| Age, years, median (IQR) | 68 (56–75) | 68 (54–76) | 0.929 | 69 (56–75) | 68 (53–77) | 0.911 | 0.006 |
| Male Gender, n (%) | 53 (82.8) | 55 (76.4) | 0.476 | 77.6 | 78.7 | 0.884 | 0.028 |
| Reasons for Admission, n (%) | 0.051 | 0.181 | |||||
| Traumatic Brain Injury | 0 (0.0) | 10 (13.9) | 0.0 | 12.0 | |||
| Coronary Heart Disease | 2 (3.1) | 7 (9.7) | 6.1 | 7.8 | |||
| Cancer Therapy | 9 (14.1) | 5 (6.9) | 10.2 | 10.6 | |||
| Respiratory Failure | 17 (26.5) | 10 (13.9) | 26.3 | 12.3 | |||
| Renal Failure | 2 (3.1) | 3 (4.2) | 3.2 | 3.8 | |||
| Sepsis | 1 (1.6) | 2 (2.8) | 1.7 | 2.0 | |||
| Stroke | 15 (23.4) | 20 (27.8) | 22.9 | 29.8 | |||
| Scheduled Surgery | 14 (21.9) | 12 (16.7) | 22.5 | 18.1 | |||
| Trauma | 4 (6.2) | 3 (4.2) | 7.2 | 3.6 | |||
| Preexisting Medical Conditions, n (%) | |||||||
| Immunocompromised Status | 9 (14.1) | 5 (6.9) | 0.280 | 10.2 | 10.6 | 0.942 | 0.013 |
| Hypertension | 24 (37.5) | 30 (41.7) | 0.749 | 37.6 | 41.9 | 0.631 | 0.088 |
| Cerebrovascular Disease | 26 (40.6) | 31 (43.1) | 0.910 | 43.1 | 42.4 | 0.936 | 0.015 |
| Diabetes Mellitus | 12 (18.8) | 11 (15.3) | 0.757 | 17.1 | 16.6 | 0.938 | 0.014 |
| Malignancy | 22 (34.4) | 14 (19.4) | 0.076 | 25.4 | 25.5 | 0.985 | 0.003 |
| Chronic Respiratory Disease | 8 (12.5) | 4 (5.6) | 0.262 | 8.8 | 8.0 | 0.879 | 0.028 |
| Chronic Kidney Disease | 6 (9.4) | 13 (18.1) | 0.226 | 14.3 | 14.3 | 0.989 | 0.003 |
| Chronic Liver Disease | 6 (9.4) | 6 (8.3) | 1.000 | 8.5 | 6.4 | 0.617 | 0.081 |
| Chronic Heart Disease | 7 (10.9) | 16 (22.2) | 0.128 | 17.6 | 17.1 | 0.948 | 0.013 |
| Shock | 5 (7.8) | 10 (13.9) | 0.393 | 10.2 | 10.6 | 0.938 | 0.015 |
| APACHE II score, median (IQR) | 13 (10–17) | 15 (11–20) | 0.071 | 14 (11–19) | 14 (10–19) | 0.772 | 0.044 |
| Nosocomial Pneumonia, n (%) | 0.312 | 0.793 | 0.049 | ||||
| With Mechanical Ventilation | 17 (26.6) | 26 (36.1) | 34.2 | 31.9 | |||
| Without Mechanical Ventilation | 47 (73.4) | 46 (63.9) | 65.8 | 68.1 | |||
| Antibiotic duration, day, median (IQR) | 9 (6–13) | 7 (5–10.25) | 0.160 | 9 (6–13) | 7 (5–10.25) | 0.073 | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zha, L.; Li, X.; Ren, Z.; Zhang, D.; Zou, Y.; Pan, L.; Li, S.; Chen, S.; Tefsen, B. Pragmatic Comparison of Piperacillin/Tazobactam versus Carbapenems in Treating Patients with Nosocomial Pneumonia Caused by Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae. Antibiotics 2022, 11, 1384. https://doi.org/10.3390/antibiotics11101384
Zha L, Li X, Ren Z, Zhang D, Zou Y, Pan L, Li S, Chen S, Tefsen B. Pragmatic Comparison of Piperacillin/Tazobactam versus Carbapenems in Treating Patients with Nosocomial Pneumonia Caused by Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae. Antibiotics. 2022; 11(10):1384. https://doi.org/10.3390/antibiotics11101384
Chicago/Turabian StyleZha, Lei, Xiang Li, Zhichu Ren, Dayan Zhang, Yi Zou, Lingling Pan, Shirong Li, Shanghua Chen, and Boris Tefsen. 2022. "Pragmatic Comparison of Piperacillin/Tazobactam versus Carbapenems in Treating Patients with Nosocomial Pneumonia Caused by Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae" Antibiotics 11, no. 10: 1384. https://doi.org/10.3390/antibiotics11101384