
Adjunctive Effect of Systemic Antibiotics in Regenerative/Reconstructive Periodontal Surgery—A Systematic Review with Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Eligibility Criteria
- -
- Population: patients with periodontitis with ID or FI treated with regenerative surgery.
- -
- Intervention: adjunctive use of systemic antibiotics.
- -
- Comparison: no use of systemic antibiotics.
- -
- Outcomes: clinical attachment level (CAL) gain, probing pocket depth (PPD) reduction, bone gain.
- -
- Studies: RCTs testing a regenerative technique at least in one arm and including at least 10 patients/arm and at least 1-year follow-up.
2.3. Information Sources, Search and Study Selection
2.4. Study Characteristics and Data Items
2.5. Risk of Bias Analysis
2.6. Summary Measures and Planned Method of Analysis
3. Results
3.1. Risk of Bias
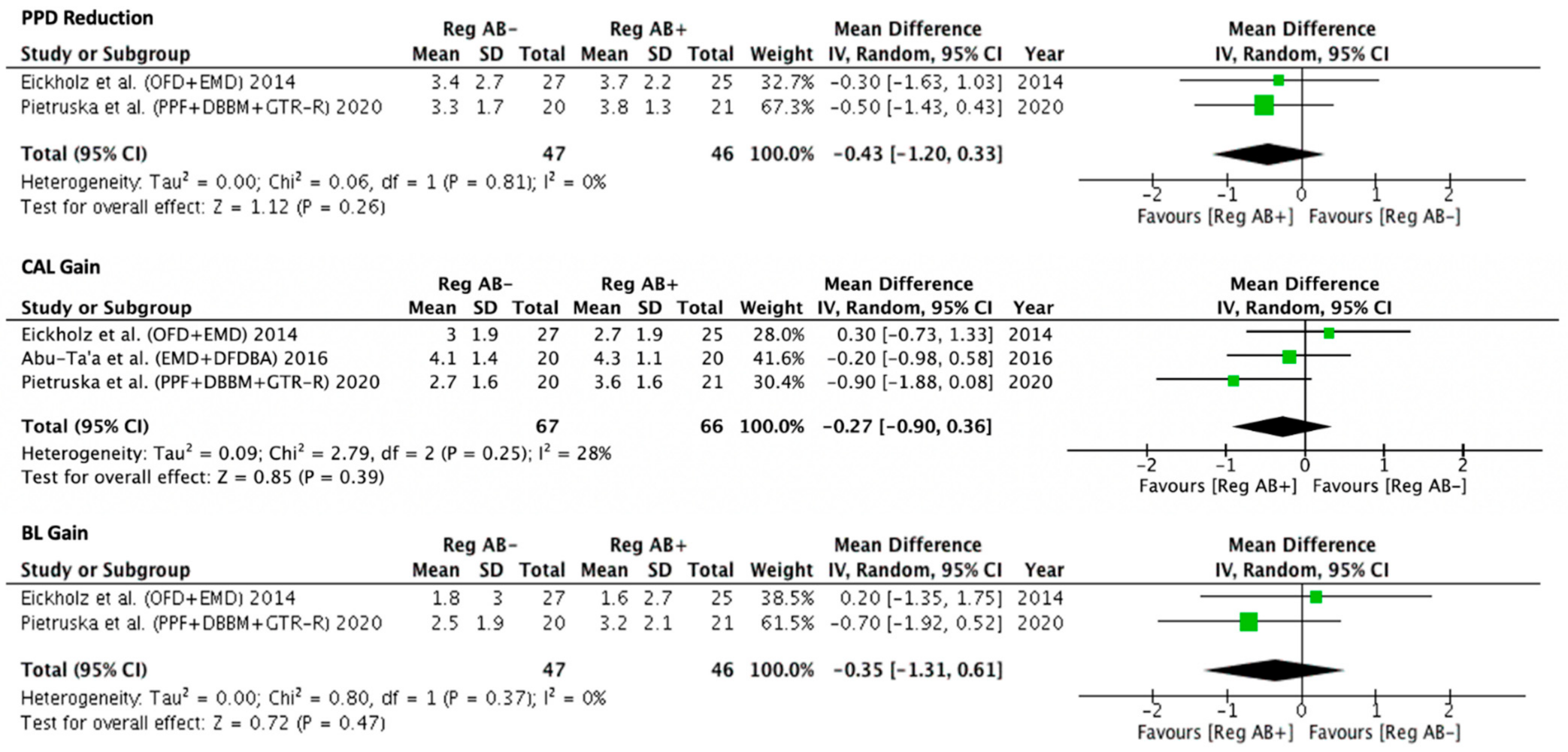
3.2. Pair-Wise Meta-Analyses
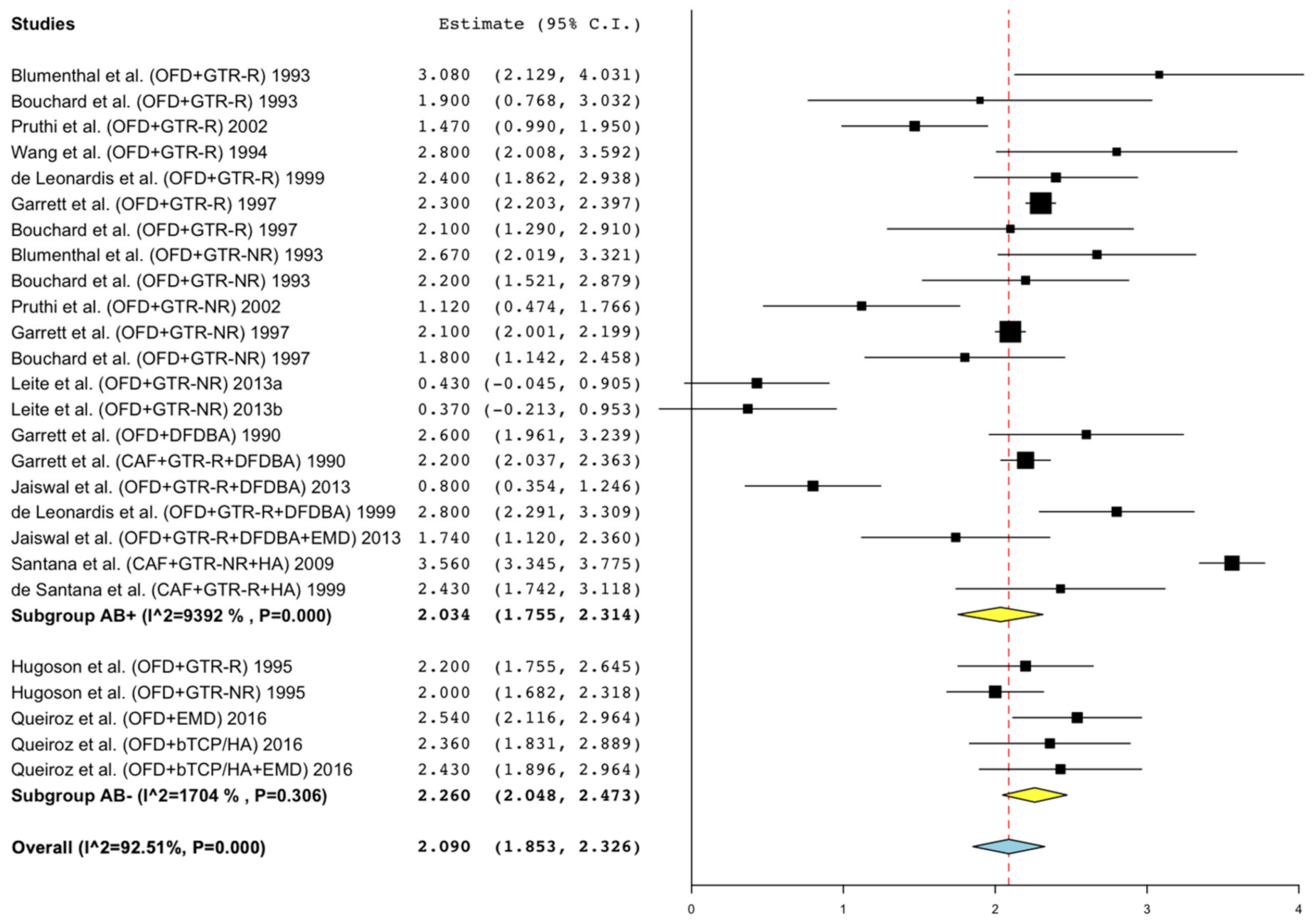
3.3. Single-Arm Meta-Regression for Intrabony Defects
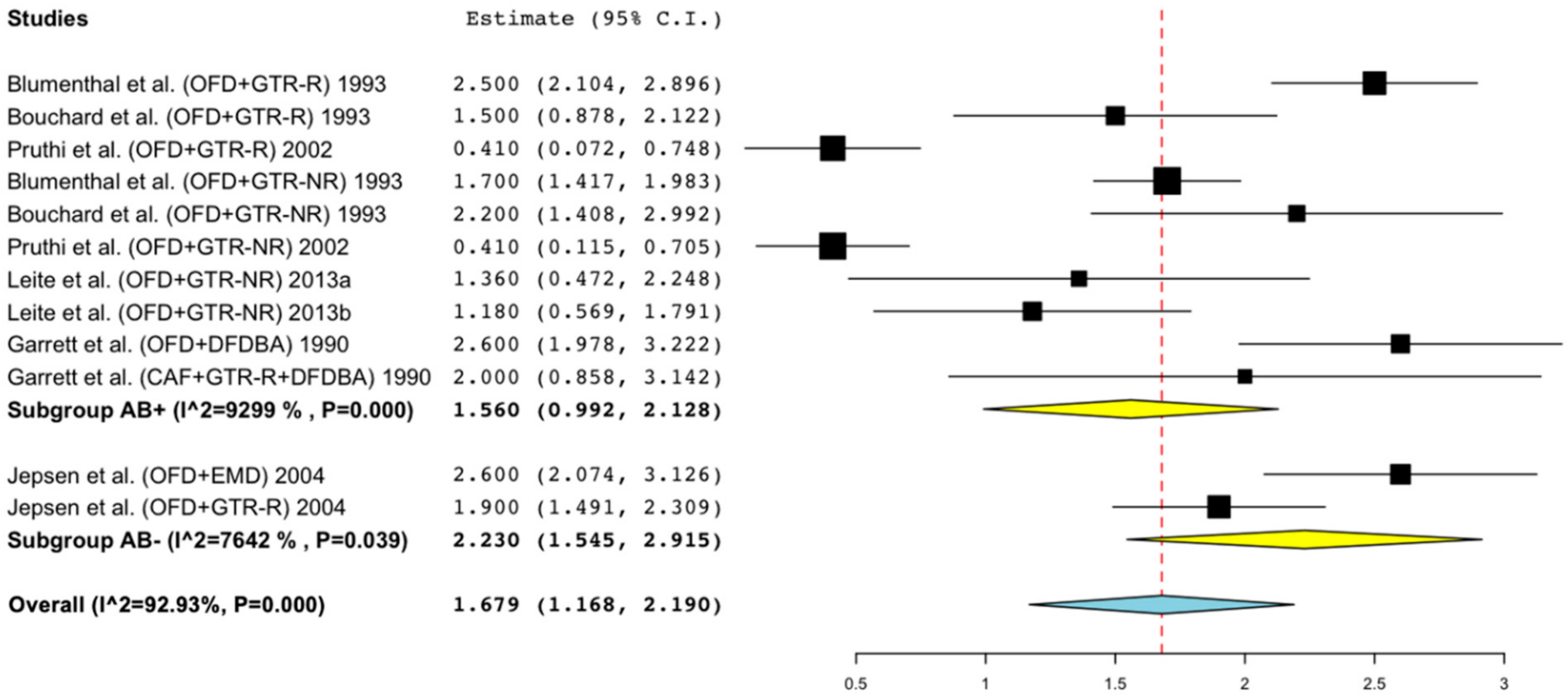
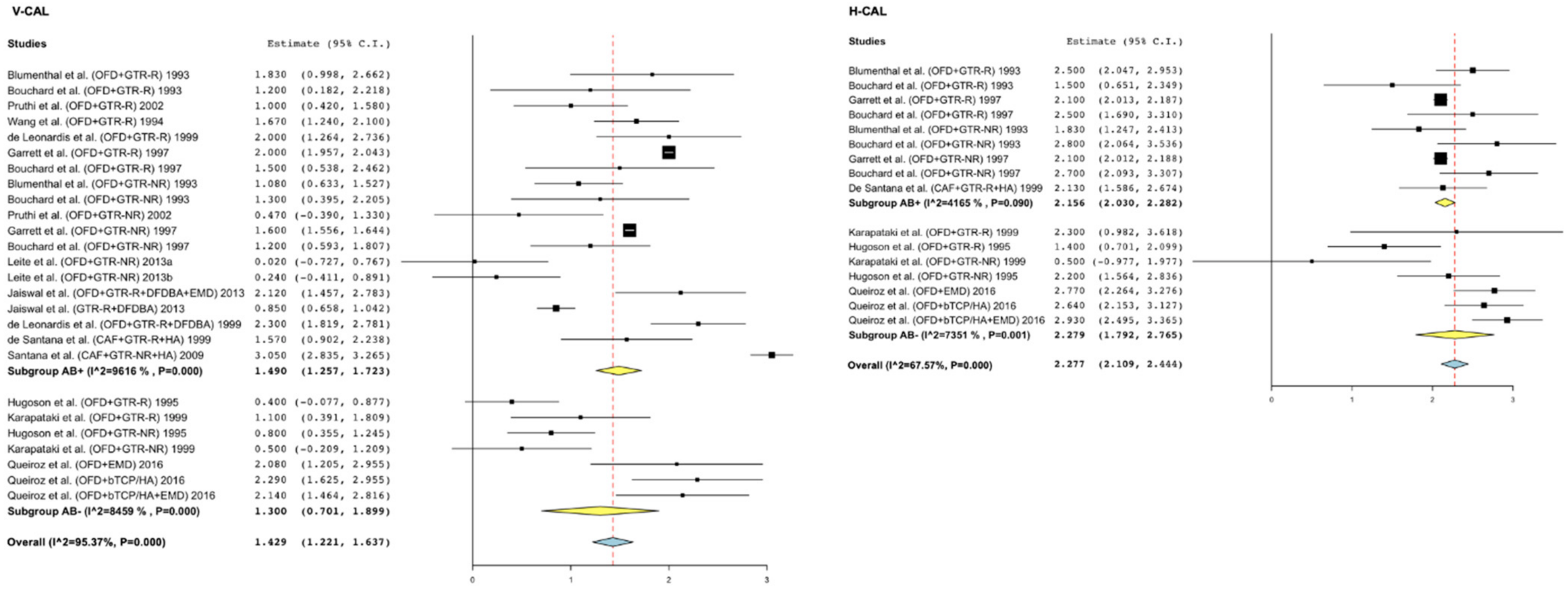
3.4. Single-Arm Meta-Regression for Furcation Defects
3.5. Adverse Events/Post-Operative Infections
3.5.1. Pair-Wise Meta-Analysis Studies (ID)
3.5.2. Single-Arm Meta-Regression Studies (ID)
3.5.3. Single-Arm Meta-Regression Studies (FI)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Baer, P.N.; Socransky, S.S. Periodontosis: Case report with long-term follow-up. Periodontal Case Rep. Publ. Northeast. Soc. Periodontists 1979, 1, 1–6. [Google Scholar]
- van Winkelhoff, A.J.; Rodenburg, J.P.; Goene, R.J.; Abbas, F.; Winkel, E.G.; de Graaff, J. Metronidazole plus amoxycillin in the treatment of Actinobacillus associated periodontitis. J. Clin. Periodontol. 1989, 16, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Teughels, W.; Feres, M.; Oud, V.; Martín, C.; Matesanz, P.; Herrera, D. Adjunctive ef-fect of systemic antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 257–281. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, K.; Jepsen, S. Antibiotics/antimicrobials: Systemic and local administration in the therapy of mild to moderately advanced periodontitis. J. Periodontol. 2000 2016, 71, 82–112. [Google Scholar] [CrossRef]
- WHO Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2017–2018; WHO: Geneva, Switzerland, 2018.
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; Aass, A.M.; Aimetti, M.; et al. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Nibali, L.; Koidou, V.P.; Nieri, M.; Barbato, L.; Pagliaro, U.; Cairo, F. Regenera-tive surgery versus access flap for the treatment of intraos- seous periodontal defects. A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 320–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jepsen, S.; Gennai, S.; Hirschfeld, J.; Kalemaj, Z.; Buti, J.; Graziani, F. Regenerative surgical treatment of furcation defects: A systematic review and Bayesian network meta-analysis of randomized clinical trials. J. Clin. Periodontol. 2020, 47, 352–374. [Google Scholar] [CrossRef]
- Sculean, A.; Blaes, A.; Arweiler, N.; Reich, E.; Donos, N.; Brecx, M. The effect of postsurgical antibiotics on the healing of intrabony defects following treat-ment with enamel matrix proteins. J. Periodontol. 2001, 72, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Minabe, M.; Kodama, T.; Kogou, T.; Fushimi, H.; Sugiyama, T.; Takeuchi, K.; Miterai, E.; Nishikubo, S. Clinical significance of antibiotic therapy in guided tissue regenera-tion with a resorbable membrane. Periodontal Clin. Investig. 2001, 23, 20–30. [Google Scholar]
- Loos, B.G.; Louwerse, P.H.G.; Van Winkelhoff, A.J.; Burger, W.; Gilijamse, M.; Hart, A.A.M.; Van Der Velden, U. Use of barrier membranes and systemic antibiotics in the treatment of intraosseous defects. J. Clin. Periodontol. 2002, 29, 910–921. [Google Scholar] [CrossRef]
- Liu, Y.; Duan, D.; Xin, Y.; Bai, L.; Li, T.; Li, C.; Xu, Y. A review of the literature: Antibiotic usage and its relevance to the infection in periodontal flaps. Acta Odontol. Scand. 2017, 75, 288–293. [Google Scholar] [CrossRef]
- Hai, J.H.; Lee, C.; Kapila, Y.L.; Chaffee, B.W.; Armitage, G.C. Antibiotic prescribing practices in periodontal surgeries with and without bone grafting. J. Periodontol. 2020, 91, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic; Reviews of Interventions Version 5.1.0.; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 1 July 2021).
- Abu-Ta’A, M. Adjunctive Systemic Antimicrobial Therapy vs Asepsis in Conjunction with Guided Tissue Regeneration: A Randomized, Controlled Clinical Trial. J. Contemp. Dent. Pract. 2016, 17, 3–6. [Google Scholar] [CrossRef]
- Eickholz, P.; Röllke, L.; Schacher, B.; Wohlfeil, M.; Dannewitz, B.; Kaltschmitt, J.; Krieger, J.K.; Krigar, D.M.; Reitmeir, P.; Kim, T.-S. Enamel Matrix Derivative in Propylene Glycol Alginate for Treatment of Infrabony Defects with or Without Systemic Doxycycline: 12- and 24-Month Results. J. Periodontol. 2014, 85, 669–675. [Google Scholar] [CrossRef]
- Pietruska, M.; Dolińska, E.; Milewski, R.; Sculean, A. Effect of systemic antibiotics on the outcomes of regenerative periodontal surgery in intrabony defects: A randomized, controlled, clinical study. Clin. Oral Investig. 2021, 25, 2959–2968. [Google Scholar] [CrossRef]
- Silvestri, M.; Ricci, G.; Rasperini, G.; Sartori, S.; Cattaneo, V. Comparison of treatments of infrabony defects with enamel matrix derivative, guided tissue regeneration with a nonresorbable membrane and Widman modified flap. A pilot study. J. Clin. Periodontol. 2000, 27, 603–610. [Google Scholar] [CrossRef]
- Silvestri, M.; Sartori, S.; Rasperini, G.; Ricci, G.; Rota, C.; Cattaneo, V. Comparison of infrabony defects treated with enamel matrix derivative versus guided tissue regeneration with a nonresorbable membrane. J. Clin. Periodontol. 2003, 30, 386–393. [Google Scholar] [CrossRef]
- Rösing, C.K.; Aass, A.M.; Mavropoulos, A.; Gjermo, P. Clinical and radiographic effects of enamel matrix derivative in the treatment of intrabony periodontal defects: A 12-month longitudinal placebo-controlled clinical trial in adult periodontitis patients. J. Periodontol. 2005, 76, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Guida, L.; Annunziata, M.; Belardo, S.; Farina, R.; Scabbia, A.; Trombelli, L. Effect of autogenous cortical bone particulate in conjunction with enamel matrix derivative in the treatment of periodontal intraosseous defects. J. Periodontol. 2007, 78, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.K.; Chai, J.K.; Cho, K.S.; Moon, I.S.; Choi, S.H.; Sottosanti, J.S.; Wikesjo, U.M. Periodontal repair in intrabony defects treated with a calcium sulfate implant and calcium sulfate barrier. J. Periodontol. 1998, 69, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Zybutz, M.D.; Laurell, L.; Rapoport, D.A.; Persson, G.R. Treatment of intrabony defects with resorbable materials, non-resorbable materials and flap debridement. J. Clin. Periodontol. 2000, 27, 169–178. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Lang, N.P.; Cortellini, P.; Susan, J.E.; Adriaens, P.; Dubravec, D.; Fonzar, A.; Fourmousis, I.; Mayfield, L.; Rossi, R.; et al. Enamel matrix proteins in the regenerative therapy of deep intrabony defects. J. Clin. Periodontol. 2002, 29, 317–325. [Google Scholar] [CrossRef]
- Mengel, R.; Soffner, M.; Flores-de-Jacoby, L. Bioabsorbable membrane and bioactive glass in the treatment of intrabony defects in patients with generalized aggressive periodontitis: Results of a 12-month clinical and radiological study. J. Periodontol. 2003, 74, 899–908. [Google Scholar] [CrossRef]
- Sanz, M.; Tonetti, M.S.; Zabalegui, I.; Sicilia, A.; Blanco, J.; Rebelo, H.; Rasperini, G.; Merli, M.; Cortellini, P.; Suvan, J.E. Treatment of Intrabony Defects with Enamel Matrix Proteins or Barrier Membranes: Results from a Multicenter Practice-Based Clinical Trial. J. Periodontol. 2004, 75, 726–733. [Google Scholar] [CrossRef]
- Fickl, S.; Thalmair, T.; Kebschull, M.; Bohm, S.; Wachtei, H. Microsurgical access flap in conjunction with enamel matrix derivative for the treatment of intra-bony defects: A controlled clinical trial. J. Clin. Periodontol. 2009, 36, 784–790. [Google Scholar] [CrossRef]
- Jepsen, S.; Topoll, H.; Rengers, H.; Heinz, B.; Teich, M.; Hoffmann, T.; Al-Machot, E.; Meyle, J.; Jervøe-Storm, P.M. Clinical outcomes after treatment of intra-bony defects with an EMD/synthetic bone graft or EMD alone: A multicentre randomized-controlled clinical trial. J. Clin. Periodontol. 2008, 35, 420–428. [Google Scholar] [CrossRef]
- Meyle, J.; Hoffman, T.; Topoll, H.; Heinz, B.; Al-Machot, E.; Jevrøe-Storm, P.M.; Meiss, C.; Eickholz, P.; Jepsen, S. A multi-centre randomized controlled clinical trial on the treatment of intra-bony defects with enamel matrix derivatives/synthetic bone graft or enamel matrix derivatives alone: Results after 12 months. J. Clin. Periodontol. 2011, 38, 652–660. [Google Scholar] [CrossRef] [Green Version]
- Christgau, M.; Schmalz, G.; Wenzel, A.; Hiller, K.A. Periodontal regeneration of intrabony defects with resorbable and non-resorbable membranes: 30-month results. J. Clin. Periodontol. 1997, 24, 17–27. [Google Scholar] [CrossRef]
- Francetti, L.; Del Fabbro, M.; Basso, M.; Testori, T.; Weinstein, R. Enamel matrix pro-teins in the treatment of intra-bony defects. A prospective 24-month clinical trial. J. Clin. Periodontol. 2004, 31, 52–59. [Google Scholar] [CrossRef]
- Siciliano, V.I.; Andreuccetti, G.; Siciliano, A.I.; Blasi, A.; Sculean, A.; Salvi, G.E. Clinical Outcomes After Treatment of Non-Contained Intrabony Defects with Enamel Matrix Derivative or Guided Tissue Regeneration: A 12-Month Randomized Controlled Clinical Trial. J. Periodontol. 2011, 82, 62–71. [Google Scholar] [CrossRef]
- Bouchard, P.; Ouhayoun, J.P.; Nilvéus, R.E. Expanded polytet-rafluoroethylene membranes and connective tissue grafts support bone regeneration for closing mandibu-lar Class II furcations. J. Periodontol. 1993, 64, 1193–1198. [Google Scholar] [CrossRef]
- Bouchard, P.; Giovannoli, J.-L.; Mattout, C.; Davarpanah, M.; Etienne, D. Clinical evaluation of a bioabsorbable regenerative material in mandibular class II furcation therapy. J. Clin. Periodontol. 1997, 24, 511–518. [Google Scholar] [CrossRef]
- Garrett, S.; Polson, A.M.; Stoller, N.H.; Drisko, C.L.; Caton, J.G.; Harrold, C.Q.; Bogle, G.; Greenwell, H.; Lowenguth, R.A.; Duke, S.P.; et al. Comparison of a Bioabsorbable GTR Barrier to a Non-Absorbable Barrier in Treating Human Class II Furcation Defects. A Multi-Center Parallel Design Randomized Single-Blind Trial. J. Periodontol. 1997, 68, 667–675. [Google Scholar] [CrossRef]
- Hugoson, A.; Ravald, N.; Fornell, J.; Johard, G.; Teiwik, A.; Gottlow, J. Treatment of Class II Furcation Involvements in Humans with Bioresorbable and Nonresorbable Guided Tissue Regeneration Barriers. A Randomized Multi-Center Study. J. Periodontol. 1995, 66, 624–634. [Google Scholar] [CrossRef]
- Karapataki, S.; Falk, H.; Hugoso, A.; Olsson, G.; Slotte, C. Treatment of class II fur-cation defects using resorbable and non-resorbable GTR barriers. Swed. Dent. J. 1999, 23, 173–183. [Google Scholar]
- Jepsen, S.; Heinz, B.; Jepsen, K.; Arjomand, M.; Hoffmann, T.; Richter, S.; Reich, E.; Sculean, A.; Gonzales, J.R.; Bödeker, R.H.; et al. A Randomized Clinical Trial Comparing Enamel Matrix Derivative and Membrane Treatment of Buccal Class II Furcation Involvement in Mandibular Molars. Part I: Study Design and Results for Primary Outcomes. J. Periodontol. 2004, 75, 1150–1160. [Google Scholar] [CrossRef] [Green Version]
- Rams, T.E.; Degener, J.E.; Van Winkelhoff, A.J. Antibiotic Resistance in Human Chronic Periodontitis Microbiota. J. Periodontol. 2014, 85, 160–169. [Google Scholar] [CrossRef]
- Ardila, C.-M.; Bedoya-García, J.-A. Antimicrobial resistance of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis and Tannerella forsythia in periodontitis patients. J. Glob. Antimicrob. Resist. 2020, 22, 215–218. [Google Scholar] [CrossRef]
- Jepsen, K.; Falk, W.; Brune, F.; Fimmers, R.; Jepsen, S.; Bekeredjian-Ding, I. Prevalence and antibiotic susceptibility trends of periodontal pathogens in the subgingival microbiota of German periodontitis patients: A retrospective surveillance study. J. Clin. Periodontol. 2021, 48, 1216–1227. [Google Scholar] [CrossRef]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Bianco, A.; Cautela, V.; Napolitano, F.; Licata, F.; Pavia, M. Appropriateness of Antibiotic Prescription for Prophylactic Purposes among Italian Dental Practitioners: Results from a Cross-Sectional Study. Antibiotics 2021, 10, 547. [Google Scholar] [CrossRef]
- Buonavoglia, A.; Leone, P.; Solimando, A.; Fasano, R.; Malerba, E.; Prete, M.; Corrente, M.; Prati, C.; Vacca, A.; Racanelli, V. Antibiotics or No Antibiotics, That Is the Question: An Update on Efficient and Effective Use of Antibiotics in Dental Practice. Antibiotics 2021, 10, 550. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Treatment | Country | N° Patients | N° Defects | Antibiotic Regimen | CAL Gain | PPD Reduction | Bone Gain |
|---|---|---|---|---|---|---|---|
| EMD | |||||||
| Silvestri et al. (OFD + EMD) 2000 | Italy | 10 | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4.5 ± 1.6 | 4.8 ± 1.6 | - |
| Heijl et al. (OFD + EMD) 1997 | Sweden | 26 | 27 | Doxycycline 200 mg day one, then 100 mg q.d. for 3 weeks | 2.2 ± 1.1 | 3.1 ± 1 | 2.6 ± 1.7 |
| Okuda et al. (OFD + EMD) 2000 | Japan | 16 | 18 | Cafaclor 750 mg q.d. 5 days | 1.72 ± 1.07 | 3 ± 0.97 | - |
| Crea et al. (OFD + EMD) 2008 | Italy | 19 | 19 | Amoxicillin 500 mg b.i.d. for 7 days | 2.4 ± 1.1 | 3.1 ± 1.4 | 2.7 ± 1 |
| Iorio-Siciliano et al. (OFD + EMD) 2011 | Italy | 20 | 20 | No antibiotic | 2.4 ± 2.2 | 2.9 ± 2.1 | - |
| Silvestri et al. (OFD + EMD) 2003 | Italy | 49 | 49 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4.1 ± 1.8 | 5.3 ± 1.9 | - |
| Pontoriero et al. (OFD + EMD) 1999 | Sweden | 10 | 10 | 3G amoxicillin 1 h before surgery | 2.9 * | 4.4 * | - |
| Sanz et al. (OFD + EMD) 2004 | Spain | 35 | 35 | No antibiotics | 3.1 ± 1.8 | 3.8 ± 1.5 | - |
| Minabe et al. (OFD + EMD) 2002 | Japan | - | 22 | Cefaclor 750 mg q.d. for 4 days | 2.6 ± 1 | 3.8 ± 0.9 | - |
| Guida et al. (OFD + EMD) 2007 | Italy | 14 | 14 | Amoxicillin 875 + clavulanic 125 b.i.d. for 6 days | 4.6 ± 1.3 | 5.6 ± 1.7 | 4.3 ± 2.4 |
| Yilmaz et al. (OFD + EMD) 2010 | Turkey | 20 | 20 | Amoxicillin 500 mg t.i.d. for 7 days | 3.4 ± 0.8 | 4.6 ± 0.4 | 2.8 ± 0.8 |
| Losada et al. (OFD + EMD) 2016 | Spain | 23 | 23 | Amoxicillin 750 or Clindamycin 300 mg t.i.d. for 7 days | 2.65 ± 2.18 | 3.3 ± 1.89 | 2.6 ± 2.03 |
| Meyle et al. (OFD + EMD) 2011 | Germany | 35 | 35 | No antibiotics | 1.93 ± 1.7 | 2.9 ± 1.8 | 2.81 ± 1.6 |
| Pietruska et al. (OFD + EMD) 2011 | Poland | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | § | § | - |
| Sculean et al. (OFD + EMD) 2005b | Netherlands/Poland | 15 | 15 | No antibiotics | 3.9 ± 1.8 | 4.5 ± 2 | - |
| Zucchelli et al. (OFD + EMD) 2003 | Italy | 30 | 30 | Amoxicillin 875 + clavulanic 125 q.d. for 6 days | 4.9 ± 1 | 5.8 ± 0.8 | 4.3 ± 1.5 |
| Sipos et al. (OFD + EMD) 2005 | Netherlands | 11 | 12 | No antibiotics | 1.28 ± 2.04 | 2.86 ± 0.75 | 1.63 ± 1.21 |
| Leknes et al. (OFD + EMD) 2009 | Norway | 13 | 13 | No antibiotics | 0.6 ± 1 | 2.5 ±1.9 | - |
| Al Machot et al. (OFD + EMD) 2014 | Germany | 19 | 19 | No antibiotics | 1.4 ± 1.8 | 2.6 ± 1.8 | 1.6 ± 1.2 |
| Eickholz et al. (OFD + EMD) 2014a | Germany | 28 | 28 | Doxycycline 200 mg q.d. for 7 days | 2.74 ± 1.89 | 3.69 ± 2.23 | - |
| Eickholz et al. (OFD + EMD) 2014b | Germany | 29 | 29 | No antibiotics | 2.95 ± 1.92 | 3.4 ± 1.73 | - |
| De Leonardis et al. (PPF + EMD) 2013 | Italy | 34 | 34 | Amoxicillin 2 g q.d for 6 days | 2.95 ± 0.74 | 3.76 ± 0.74 | 2.61 ± 0.49 |
| Fickl et al. (PPF + EMD) 2009 | Germany | 19 | 35 | No antibiotics | 3.7 ± 0.4 | 4.2 ± 0.3 | 2.5 ± 0.4 |
| Francetti et al. (PPF + EMD) 2004 | Italy | 11 | 11 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 5 days | 4.29 ± 1.38 | 4.86 ± 1.95 | 3.44 ± 1.18 |
| Tonetti et al. (PPF + EMD) 2002 | UK | 83 | 83 | No antibiotics | 3.1 ± 1.5 | 3.9 ± 1.7 | - |
| Zucchelli et al. (PPF + EMD) 2002 | Italy | 30 | 30 | Amoxicillin 875 mg + clavulanic 125 mg q.d for 7 days | 4.2 ± 0.9 | 5.1 ± 0.7 | - |
| Francetti et al. (PPF + EMD) 2005 | Italy | 64 | 82 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 5 days | 3.51 * | 4.02 * | - |
| Wachtel et al. (PPF + EMD) 2003 | Germany | 11 | 26 | No antibiotics | 3.6 ± 1.6 | 3.9 ± 1.4 | - |
| Grusovin et al. (PPF + EMD) 2009 | UK | 15 | 15 | No antibiotics | 3.4 ± 1.1 | 4.2 ± 1.6 | 2.5 ± 1.2 |
| Rosing et al. (PPF + EMD) 2005 | Norway | 14 | 14 | Penicillin 500 mg t.i.d for 5 days | § | § | § |
| Bokan et al. (PPF + EMD) 2006 | Germany | 19 | 19 | Doxycycline 100 mg q.d. for 7 days | 3.7 ± 1 | 3.9 ± 1.3 | - |
| Aslan et al. (PPF + EMD) 2020 | Turkey | 15 | 15 | Doxycycline 100 mg b.i.d. for 7 days | 6.3 ± 2.5 | 6.5 ± 2.65 | - |
| Mazzonetto et al. (PPF + EMD) 2020 | Brazil | 20 | 20 | No antibiotics | 2.4 ± 1 | 2.3 ± 1.2 | 1.24 ± 1.14 |
| EMD + graft | |||||||
| Paolantonio et al. (PPF + EMD + AB) 2020 | Italy | 22 | 22 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 6 days | 3.29 ± 0.85 | 3.96 ± 1.04 | 2.67 ± 1.06 |
| Guida et al. (OFD + EMD + AB) 2007 | Italy | 13 | 14 | Amoxicillin 875 + clavulanic 125 b.i.d. for 6 days | 4.9 ± 1.8 | 5.1 ± 1.7 | 4.3 ± 1.3 |
| Yilmaz et al. (OFD + EMD + AB) 2010 | Turkey | 20 | 20 | Amoxicillin 500 mg t.i.d. for 7 days | 4.2 ± 1.1 | 5.6 ± 0.9 | 3.9 ± 1 |
| Sculean et al. (OFD + EMD + BG) 2005b | Netherlands/Poland | 15 | 15 | No antibiotics | 3.2 ± 1.7 | 4.2 ± 1.4 | - |
| Sculean et al. (OFD + EMD + BG) 2002b | Germany | 14 | 14 | Amoxicillin 500 mg t.i.d. for 7 days | § | § | - |
| Ghezzi et al. (PPF + EMD + DBBM) 2016 | Italy | 10 | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4.4 ± 1.17 | 4.9 ± 1.2 | - |
| Sculean et al. (OFD + EMD + DBBM) 2002a | Germany | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.7 ± 1.9 | 5.7 ± 1.5 | - |
| Iorio-Siciliano et al. (OFD + EMD + DBBM) 2014 | Italy | 20 | 20 | No antibiotics | 3.8 ± 1.6 | 4.6 ± 1.9 | - |
| Döri et al. (OFD + EMD + DBBM) 2005 | Hungary | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.3 ± 0.8 | 4.8 ± 0.9 | - |
| Döri et al. (OFD + EMD + DBBM) 2008b | Hungary | 13 | 13 | Amoxicillin 500 mg t.i.d. for 7 days | 5 ± 0.9 | 5.9 ± 1.3 | - |
| Zucchelli et al. (OFD + EMD + DBBM) 2003 | Italy | 30 | 30 | Amoxicillin 875 + clavulanic 125 q.d. for 6 days | 5.8 ± 1.1 | 6.2 ± 0.4 | 5.3 ± 1.1 |
| Aspriello et al. (OFD + EMD + DFDBA) 2011 | Italy | 28 | 28 | Ceftibuten 400 mg q.d. for 6 day | 4 * | 5 * | 4 * |
| Abu-ta et al. (OFD + EMD + DFDBA) 2016 | Palestine | 20 | 20 | Amoxicillin 1 g pre-operative and 2 g q.d. for two days | 4.3 ± 1.1 | 3.4 ± 1.2 | - |
| Abu-ta et al. (OFD + EMD + DFDBA) 2016 | Palestine | 20 | 20 | No antibiotics | 4.1 ± 1.4 | 3.7 ± 1.3 | - |
| Döri et al. (OFD + EMD + bTCP) 2005 | Hungary | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.1 ± 0.8 | 4.6 ± 0.8 | - |
| Losada et al. (OFD + EMD + HA/bTCP) 2016 | Spain | 21 | 21 | Amoxicillin 750 or Clindamycin 300 mg t.i.d. for 7 days | 2.38 ± 2.17 | 3.14 ± 1.95 | 2.71 ± 1.79 |
| Meyle et al. (OFD + EMD + HA/bTCP) 2011 | Germany | 38 | 38 | No antibiotics | 1.69 ± 2.1 | 2.8 ± 2.1 | 2.65 ± 1.9 |
| Pietruska et al. (OFD + EMD + HA/bTCP) 2011 | Pietruska | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | § | § | - |
| Bokan et al. (PPF + EMD + bTCP) 2006 | Germany | 19 | 19 | Doxycycline 100 mg q.d. for 7 days | 4 ± 1 | 4.1 ± 1.2 | - |
| Lee et al. (OFD + EMD + DPBM) 2020 | Korea | 20 | 20 | Amoxicillin 500 mg t.i.d. for 5 days | § | § | - |
| GTR-NR | |||||||
| Silvestri et al. (OFD + GTR-NR) 2000 | Italy | 10 | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4.8 ± 1.6 | 5.9 ± 1.1 | - |
| Mora et al. (OFD + GTR-NR) 1996 | France | 10 | 10 | Tetracycline 500 mg q.d. 8 days | 3.85 ± 0.9 | 5.35 ± 1.1 | 2.95 ± 1.3 |
| Crea et al. (OFD + GTR-NR) 2008 | Italy | 20 | 20 | Amoxicillin 500 mg b.i.d. for 7 days | 2 ± 1.1 | 3.2 ± 1.1 | 2.7 ± 1.2 |
| Iorio-Siciliano et al. (OFD + GTR-NR) 2011 | Italy | 20 | 20 | No antibiotics | 4.1 ± 1.4 | 5.5 ± 1 | - |
| Silvestri et al. (OFD + GTR-NR) 2003 | Italy | 49 | 49 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4.3 ± 1.9 | 5.6 ± 1.5 | - |
| Pontoriero et al. (OFD + GTR-NR) 1999 | Sweden | 10 | 10 | 3G amoxicillin 1 h before surgery | 2.9 * | 4.7 * | - |
| Christgau et al. (OFD + GTR-NR) 1997 | Germany | 10 | 10 | Doxycycline 100 mg q.d. for 10 days | 3.7 ± 3 | 3.9 ± 2.3 | - |
| Zybutz et al. (OFD + GTR-NR) 2000 | USA | 14 | 14 | The day of surgery. Molecule and dosage not specified | 2.4 ± 0.8 | 3.1 ± 1.2 | 2.2 ± 1.7 |
| Zucchelli et al. (PPF + GTR-NR) 2002 | Italy | 30 | 30 | Amoxicillin 875 + clavulanic 125 q.d. for 7 days | 4.9 ± 1.6 | 6.5 ± 1.6 | - |
| GTR-R | |||||||
| Mayfield et al. (OFD + GTR-R) 1998 | Sweden | 20 | 20 | No antibiotics | 1.5 ± 1.9 | 2.9 ± 1.8 | 0.6 ± 1.2 |
| Paolantonio et al. (OFD + GTR-R) 2008 | Italy | 17 | 17 | Ampicillin 1 g b.i.d. for 7 days | 3.1 * | 5.2 * | 2.4 * |
| Loos et al. (OFD + GTR-R) 2002 | Netherlands | 13 | 13 | Amoxicillin 375 mg and metronidazole 250 mg t.i.d. 8 days | 1.3 * | - | - |
| Loos et al. (OFD + GTR-R) 2002 | Netherlands | 12 | 12 | No antibiotics | 1.5 * | - | - |
| Blumenthal et al. (OFD + GTR-R) 1990 | USA | 15 | 15 | Tetracycline 250 mg q.d. for 10 days | 1.17 ± 0.1 | 1.99 ± 0.3 | 1.83 ± 0.2 |
| Pontoriero et al. (OFD + GTR-R) 1999 | Sweden | 10 | 10 | 3G amoxicillin 1 h before surgery | 3 * | 4.1 * | - |
| Pontoriero et al. (OFD + GTR-R) 1999 | Sweden | 10 | 10 | 3G amoxicillin 1 h before surgery | 3.4 * | 4.8 * | - |
| Sanz et al. (OFD + GTR-R) 2004 | Spain | 32 | 32 | No antibiotics | 2.5 ± 1.9 | 3.3 ± 1.5 | - |
| Minabe et al. (OFD + GTR-R) 2002 | Japan | - | 24 | Cefaclor 750 mg q.d. for 4 days | 2.8 ± 0.9 | 3.7 ± 1.2 | - |
| Christgau et al. (OFD + GTR-R) 1997 | Germany | 10 | 10 | Doxycycline 100 mg q.d. for 10 days | 3.8 ± 1.9 | 4 ± 1.4 | - |
| Zybutz et al. (OFD + GTR-R) 2000 | USA | 15 | 15 | The day of surgery. Molecule and dosage not specified | 2.4 ± 1.9 | 3.3 ± 2.1 | 2.4 ± 3.7 |
| Trejo et al. (OFD + GTR-R) 2000 | USA | 14 | 14 | Doxycycline 100 mg q.d. for 10 days | 3.27 ± 1.1 | 4.12 ± 0.84 | 5.35 ± 2.91 |
| Paolantonio et al. (OFD + GTR-R) 2002 | Italy | 17 | 17 | Ampicillin 1 g b.i.d. for 7 days | 4 ± 1.27 | 5.58 ± 1 | 3.82 ± 1.28 |
| Mengel et al. (OFD + GTR-R) 2003 | Germany | - | 22 | No antibiotics | 3.4 ± 2.3 | 4 ± 2.1 | - |
| Tonetti et al. (PPF + GTR-R) 1998 | Switzerland | 69 | 69 | Doxycycline 100 mg b.i.d. for 7 days | 3.04 ± 1.64 | 4.03 ± 1.81 | - |
| Cortellini et al. (PPF + GTR-R) 2001 | Italy | 55 | 55 | Doxycycline 200 mg q.d. for 7 days | 3.5 ± 2.1 | 4.4 ± 2.4 | - |
| Stravopolous et al. (PPF + GTR-R) 2003 | Denmark | 14 | 14 | Amoxicillin 750 mg + metronidazole 250 mg q.d. for 5 days | 2.9 * | 3.9 * | 3.1 * |
| Graft + GTR-R | |||||||
| Sculean et al. (OFD + DBBM + GTR-R) 2003 | Germany | 14 | 14 | Amoxicillin 500 mg t.i.d. for 7 days | 4 ± 1.3 | 5.3 ± 1.6 | - |
| Sculean et al. (OFD + DBBM + GTR-R) 2005a | Netherlands | 16 | 16 | No antibiotics | 4.1 ± 0.9 | 5.4 ± 0.9 | - |
| Tonetti et al. (OFD + DBBM + GTR-R) 2004 | UK | 61 | 61 | Doxycycline 200 mg q.d. for 7 days | 3.3 ± 1.7 | 3.7 ± 1.8 | - |
| Iorio-Siciliano et al. (OFD + DBBM + GTR-R) 2014 | Italy | 20 | 20 | No antibiotics | 3.7 ± 1.2 | 4.4 ± 1.7 | - |
| Döri et al. (OFD + DBBM + GTR-R) 2007b | Hungary | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.6 ± 0.8 | 5.7 ± 1.2 | - |
| Paolantonio et al. (OFD + DBBM + GTR-R) 2002 | Italy | 17 | 17 | Ampicillin 1 g b.i.d. for 7 days | 5.05 ± 1.56 | 5.76 ± 1.6 | 5.23 ± 1.3 |
| Stravopolous et al. (PPF + DBBM + GTR-R) 2003 | Denmark | 15 | 15 | Amoxicillin 750 mg + metronidazole 250 mg q.d. for 5 days | 2.5 * | 3.8 * | 2.8 * |
| Ghezzi et al. (OFD + DBBM + GTR-R) 2016 | Italy | 10 | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 7 days | 4 ± 1.82 | 4.7 ± 2.36 | - |
| Pietruska et al. (PPF + DBBM + GTR-R) 2020 | Poland | 21 | 21 | Amoxicillin 2 g q.d. for 7 days | 3.6 ± 1.6 | 3.8 ± 1.3 | 3.2 ± 2.1 |
| Pietruska et al. (PPF + DBBM + GTR-R) 2020 | Poland | 20 | 20 | No antibiotics | 2.7 ± 1.6 | 3.3 ± 1.7 | 2.5 ± 1.9 |
| Kim et al. (OFD + DFDBA + CS barrier) 1998 | Korea | 13 | 13 | Tetracycline 250 mg q.d. for 7 days | 2.9 ± 0.8 | 4.3 ± 0.5 | 2.9 ± 1.4 |
| Trejo et al. (OFD + DFDBA + GTR-R) 2000 | USA | 16 | 16 | Doxycycline 100 mg q.d. for 10 days | 2.29 ± 0.61 | 3.37 ± 1.16 | 4.73 ± 1.18 |
| Christgau et al. (OFD + bTCP + GTR-R) 2006 | Germany | 25 | 25 | Doxycycline 100 mg q.d. for 19 days | 5.2 ± 1.6 | 6 ± 1.1 | - |
| Orsini et al. (OFD + AB + CSM) 2008 | Italy/Spain | 12 | 12 | Antibiotic for 1 week. The molecule and dosage were not specified | 2.6 ± 1.2 | 3.3 ± 1.6 | - |
| Orsini et al. (OFD + AB + GTR-R) 2008 | Italy/Spain | 12 | 12 | Antibiotic for 1 week. The molecule and dosage were not specified | 2.4 ± 1.1 | 4.2 ± 1.2 | - |
| Cetinkaya et al. (OFD + BG + GTR-R) 2014 | Turkey | 11 | 11 | No Antibiotics | 2.64 ± 1.12 | 3.45 ± 0.93 | 3 ± 1.48 |
| Yamamiya et al. (OFD + HA + HCPC) 2008 | Japan | 15 | 15 | Cefaclor 750 mg q.d. for 5 days | 2.7 ± 1.3 | 4.3 ± 1.1 | 3.2 ± 1.1 |
| Graft + GTR-NR | |||||||
| Nygaard-Østby et al. (OFD + AB + GTR-NR) 2010 | Norway | 13 | 13 | Amoxicillin 500 mg b.i.d. for 10 days | 3.8 ± 0.5 | 4.2 ± 0.5 | 3.9 ± 0.8 |
| Döri et al. (OFD + bTCP + GTR-NR) 2008a | Hungary | 14 | 14 | Amoxicillin 500 mg t.i.d. for 7 days | 3.9 ± 0.2 | 5.4 ± 0.7 | - |
| Döri et al. (OFD + DBBM + GTR-NR) 2007a | Hungary | 15 | 15 | Amoxicillin 500 mg t.i.d. for 7 days | 4.6 ± 1.1 | 5.5 ± 1.7 | - |
| Graft | |||||||
| Nygaard-Østby et al. (OFD + AB) 2010 | Norway | 13 | 13 | Amoxicillin 500 mg b.i.d. for 10 days | 2.2 ± 0.7 | 2.7 ± 0.5 | 1.3 ± 0.9 |
| Leknes et al. (OFD + BG) 2009 | Norway | 13 | 13 | No Antibiotics | 1.2 ± 0.2 | 2.6 ± 1.1 | - |
| Mengel et al. (OFD + BG) 2003 | Germany | - | 20 | No Antibiotics | 2.8 ± 1.8 | 3.8 ± 1.9 | - |
| Sculean et al. (OFD + BG) 2002b | Germany | 14 | 14 | Amoxicillin 500 mg t.i.d. for 7 days | § | § | - |
| Yassibag-Berkman et al. (OFD + bTCP) 2007 | Turkey | - | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 5 days | 2.5 * | 4.1 * | - |
| Pietruska et al. (OFD + HA) 2012 | Poland | 15 | 15 | Amoxicillin 1 g b.i.d. for 7 days | 2 ± 2.7 | 2.9 ± 2.5 | 1.9 ± 1.5 |
| Al Machot et al. (OFD + HA) 2014 | Germany | 19 | 19 | No Antibiotics | 2.1 ± 1.6 | 3.2 ± 1.8 | 1.6 ± 1.2 |
| Kasaj et al. (OFD + HA/p-15) 2008 | Germany | 13 | 13 | No antibiotics | 3.9 ± 1.7 | 4.3 ± 1.3 | - |
| Okuda et al. (OFD + HA + saline) 2005 | Japan | 35 | 35 | Cefaclor 750 mg q.d. for 5 days | 2 ± 1.2 | 3.7 ± 2 | 2.7 ± 1.6 |
| De Leonardis et al. (PPF + HA/bTCP) 2013 | Italy | 34 | 34 | Amoxicillin 2 g q.d. for 6 days | 3.63 ± 0.91 | 4.25 ± 0.63 | 3.35 ± 0.8 |
| Scabbia et al. (PPF + HA/collagen/chondroitin sulfate) 2004 | Italy | 13 | 13 | No Antibiotics | 2.9 ± 1.9 | 4.2 ± 2.1 | 2.5 ± 1.4 |
| Slotte et al. (OFD + DBBM) 2012 | Sweden | 16 | 16 | Phenoxymethylpenicillin 2 g or clindamycin 300 mg b.i.d. for 7 days | 2.3 ± 0.8 | 3.2 ± 0.7 | 3.4 ± 2.3 |
| Sculean et al. (OFD + DBBM) 2002a | Germany | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.9 ± 2.1 | 6.5 ± 2 | - |
| Döri et al. (OFD + DBBM) 2009 | Hungary | 15 | 15 | Amoxicillin 500 mg t.i.d. for 7 days | 4.7 ± 1.6 | 5.3 ± 1.7 | - |
| Qiao et al. (OFD + DBBM) 2016 | China | - | 16 | Amoxicillin 500 mg t.i.d. for 7 days | 2.4 ± 1.1 | 3 ± 1.6 | 2.1 ± 1.5 |
| Scabbia et al. (PPF + DBBM) 2004 | Italy | 11 | 11 | No Antibiotics | 4 ± 2.4 | 4.4 ± 2.3 | 3.1 ± 1.8 |
| Agarwal et al. (OFD + DFDBA) 2014 | India | 24 | 24 | Amoxicillin 500 mg t.i.d. for 7 days | 2.4 ± 0.61 | 3.65 ± 0.52 | 2.37 ± 0.47 |
| Piemontese et al. (OFD + DFDBA) 2008 | Italy | 30 | 30 | Ceftibuten 400 mg q.d. for 5 days | 2.4 ± 2.2 | 3.5 ± 1.9 | 2.6 ± 1.8 |
| Agarwal et al. (OFD + DFDBA) 2015 | India | 30 | 30 | Amoxicillin 500 mg t.i.d. for 7 days | 2.61 ± 0.68 | 3.6 ± 0.51 | 2.49 ± 0.64 |
| Aspriello et al. (OFD + DFDBA) 2011 | Italy | 28 | 28 | Ceftibuten 400 mg q.d. for 6 days | 3.25 * | 4 * | 3.5 * |
| Blumenthal et al. (OFD + AAA) 1990 | USA | - | 14 | Tetracycline 250 mg q.d. for 10 days | 1.43 ± 0.1 | 2.03 ± 0.1 | 2.06 ± 0.1 |
| Shirakata et al. (OFD + CPC) 2008 | Japan | 15 | 15 | The molecule and dosage were not specified. | 2.3 ± 1 | 3.4 ± 1.2 | 1.2 ± 0.8 |
| Paolantonio et al. (OFD + CS) 2008 | Italy | 17 | 17 | Ampicillin 1 g b.i.d. for 7 days | 2.7 * | 4.4 * | 2.3 * |
| Lee et al. (OFD + DPBM) 2020 | Korea | 22 | 22 | Amoxicillin 500 mg t.i.d. for 5 days | § | § | - |
| Minenna et al. (OFD + PLA/PGA) 2005 | Italy | 16 | 16 | No antibiotics | 3.6 ± 1.5 | 4.6 ± 2 | - |
| PRP/PRF | |||||||
| Thorat et al. (OFD + PRF) 2017 | India | 15 | 15 | Amoxicillin 500 mg +metronidazole 400 mg q.d. for 7 days | 4 ± 0.63 | 4 ± 0.63 | - |
| Patel et al. (OFD + PRF) 2017 | India | 13 | 13 | Amoxicillin 500 mg t.i.d. for 7 days | 3.7 ± 0.67 | 4.2 ± 1.69 | - |
| Graft + PRP/PRF | |||||||
| Döri et al. (OFD + DBBM + PRP) 2009 | Hungary | 15 | 15 | Amoxicillin 500 mg t.i.d. for 7 days | 4.6 ± 1.7 | 5.2 ± 1.6 | - |
| Qiao et al. (OFD + DBBM + PRP(CGF)) 2016 | China | - | 15 | Amoxicillin 500 mg t.i.d. for 7 days | 3.7 ± 1.3 | 4.2 ± 1.3 | 3.3 ± 1.5 |
| Agarwal et al. (OFD + DFDBA + PRF) 2015 | India | 30 | 30 | Amoxicillin 500 mg t.i.d. for 7 days | 3.73 ± 0.74 | 4.15 ± 0.84 | 3.5 ± 0.67 |
| Agarwal et al. (OFD + DFDBA + PRP) 2014 | India | 24 | 24 | Amoxicillin 500 mg t.i.d. for 7 days | 3.15 ± 0.5 | 3.64 ± 0.63 | 3.02 ± 0.5 |
| Piemontese et al. (OFD + DFDBA + PRP) 2008 | Italy | 30 | 30 | Ceftibuten 400 mg q.d. for 5 days | 3.6 ± 1.8 | 4.6 ± 1.3 | 3.3 ± 1.5 |
| Okuda et al. (OFD + HA + PRP) 2005 | Japan | 35 | 35 | Cafaclor 750 mg q.d. for 5 days | 3.4 ±1.7 | 4.7 ± 1.6 | 3.5 ± 1.5 |
| Yamamiya et al. (OFD + HA + PRP) 2008 | Japan | 15 | 15 | Cafaclor 750 mg q.d. for 5 days | 3.9 ± 1.6 | 4.8 ± 1.1 | 4.9 ± 1.2 |
| Yassibag-Berkman et al. (OFD + bTCP + PRP) 2007 | Turkey | - | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 5 days | 2.1 * | 3.6 * | - |
| Paolantonio et al. (PPF + AB + l-PRF) 2020 | Italy | 22 | 22 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 6 days | 3.43 ± 0.74 | 4.21 ± 1.1 | 2.92 ± 0.71 |
| Other Combinations | |||||||
| Blumenthal et al. (OFD + AAA + CG) 1990 | USA | - | 12 | Tetracycline 250 mg q.d. for 10 days | 1.88 ± 0.2 | 2.61 ± 0.1 | 2.88 ± 0.2 |
| Blumenthal et al. (OFD + AAA + CG + GTR-R) 1990 | USA | - | 15 | Tetracycline 250 mg q.d. for 10 days | 2.01 ± 0.1 | 2.73 ± 0.1 | 3.71 ± 0.1 |
| Döri et al. (OFD + bTCP + GTR-NR + PRP) 2008a | Hungary | 14 | 14 | Amoxicillin 500 mg t.i.d. for 7 days | 4.1 ± 0.7 | 5.8 ± 0.6 | - |
| Christgau et al. (OFD + bTCP + GTR-R + PRP) 2006 | Germany | 25 | 25 | Doxycycline 100 mg q.d. for 19 days | 5 ± 1.5 | 6.3 ± 1.2 | - |
| Yassibag-Berkman et al. (OFD + bTCP + PRP + GTR-R) 2007 | Turkey | - | 10 | Amoxicillin 875 + clavulanic 125 b.i.d. for 5 days | 2.4 * | 4 * | - |
| Döri et al. (OFD + DBBM + EMD + PRP) 2008b | Hungary | 13 | 13 | Amoxicillin 500 mg t.i.d. for 7 days | 4.8 ± 1.3 | 5.8 ± 1.8 | - |
| Döri et al. (OFD + DBBM + GTR-NR + PRP) 2007a | Hungary | 15 | 15 | Amoxicillin 500 mg t.i.d. for 7 days | 4.5 ± 1.1 | 5.5 ± 1.3 | - |
| Döri et al. (OFD + DBBM + GTR-R + PRP) 2007b | Hungary | 12 | 12 | Amoxicillin 500 mg t.i.d. for 7 days | 4.7 ± 1.1 | 5.5 ± 1.2 | - |
| Minabe et al. (OFD + EMD + GTR-R) 2002 | Japan | - | 23 | Cefaclor 750 mg q.d. for 4 days | 3 ± 1.3 | 4.3 ± 1.6 | - |
| Sipos et al. (OFD + EMD + GTR-R) 2005 | Netherlands | 11 | 12 | No antibiotics | 1.65 ± 1.29 | 3.02 ± 1.55 | 1.58 ± 1.92 |
| Cetinkaya et al. (OFD + PP + GTR-R) 2014 | Turkey | 11 | 11 | No antibiotics | 2.36 ± 0.92 | 2.91 ± 0.94 | 3.45 ± 1.81 |
| Aoki et al. (PPF + DBBM + rhFGF-2) 2020 | Japan | 20 | 20 | Amoxicillin 750 mg or cefdinir 300 mg q.d. for 4 days | 3.11 ± 1.46 | 3.58 ± 1.53 | - |
| Ferrarotti et al. (PPF + DPSCs) 2018 | Italy | 15 | 15 | Amoxicillin 875 + clavulanic 125, 1 g q.d. for 6 days | 4.5 ± 1.9 | 4.9 ± 1.4 | 3.9 ± 1.5 |
| Aoki et al. (PPF + rhFGF-2) 2020 | Japan | 18 | 18 | Amoxicillin 750 mg or cefdinir 300 mg q.d. for 4 days | 3.35 ± 1.28 | 3.58 ± 1.21 | - |
| Santana et al. (PPF + rhFGF-2/HyAc) 2015 | Brazil | 30 | 30 | Doxycycline 200 mg before surgery and 100 mg q.d. for 19 days | 4.8 ± 0.2 | 5.5 ± 1.4 | - |
| Author/Treatment | Country | N° Patient | N° Defect | Antibiotic Regimen | V-CAL Gain | H-CAL Gain | PPD Reduction | H-BL Gain |
|---|---|---|---|---|---|---|---|---|
| GTR−R | ||||||||
| Blumenthal et al. (OFD + GTR-R) 1993 | USA | 12 | 12 | Amoxicillin 500 mg t.i.d for 7 days | 1.83 ± 1.47 | 2.5 ± 0.8 | 3.08 ± 1.68 | 2.5 ± 0.7 |
| Bouchard et al. (OFD + GTR-R) 1993 | France | 12 | 12 | Doxycycline 100 mg q.d. for 14 days | 1.2 ± 1.8 | 1.5 ± 1.5 | 1.9 ± 2 | 1.5 ± 1.1 |
| Maragos et al. (OFD + GTR-R) 2002 | USA | - | 11 | Doxycycline 100 mg q.d. for 10 days | 1.4 ± 0.4 | - | - | 0.9 ± 0.12 |
| Pruthi et al. (OFD + GTR-R) 2002 | Canada | 17 | 17 | Doxycycline 200 mg day of surgery and 100 mg q.d for 13 days | 1 ± 1.22 | - | 1.47 ± 1.01 | 0.41 ± 0.71 |
| Wang et al. (OFD + GTR-R) 1994 | USA | 12 | 12 | Doxycycline 100 mg q.d. for 14 days | 1.67 ± 0.76 | - | 2.8 ± 1.4 | - |
| de Leonardis et al. (OFD + GTR-R) 1999 | Italy/USA | 12 | 12 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 7 days | 2 ± 1.3 | - | 2.4 ± 0.95 | - |
| Garrett et al. (OFD + GTR-R) 1997 | USA | 66 | 66 | Doxycycline 100 mg b.i.d. the day of surgery and q.d. for 13 days | 2 ± 0.2 | 2.1 ± 0.4 | 2.3 ± 0.45 | - |
| Bouchard et al. (OFD + GTR-R) 1997 | France | 15 | 15 | Amoxicillin + clavulanic 1.5 g q.d. for 14 days | 1.5 ± 1.9 | 2.5 ± 1.6 | 2.1 ± 1.6 | - |
| Hugoson et al. (OFD + GTR-R) 1995 | Sweden | 38 | 38 | No Antibiotics | 0.4 ± 1.5 | 1.4 ± 2.2 | 2.2 ± 1.4 | - |
| Karapataki et al. (OFD + GTR-R) 1999 | Sweden | 11 | 11 | No antibiotics | 1.1 ± 1.2 | 2.3 ± 2.23 | - | - |
| Jepsen et al. (OFD + GTR-R) 2004 | Germany | 45 | 45 | No Antibiotics | - | - | - | 1.9 ± 1.4 |
| GTR-NR | ||||||||
| Blumenthal et al. (OFD + GTR-NR) 1993 | USA | 12 | 12 | Amoxicillin 500 mg t.i.d for 7 days | 1.08 ± 0.79 | 1.83 ± 1.03 | 2.67 ± 1.15 | 1.7 ± 0.5 |
| Bouchard et al. (OFD + GTR-NR) 1993 | France | 12 | 12 | Doxycycline 100 mg q.d. for 14 days | 1.3 ± 1.6 | 2.8 ± 1.3 | 2.2 ± 1.2 | 2.2 ± 1.4 |
| Pruthi et al. (OFD + GTR-NR) 2002 | Canada | 17 | 17 | Doxycycline 200 mg day of surgery and 100 mg q.d for 13 days | 0.47 ± 1.81 | - | 1.12 ± 1.36 | 0.41 ± 0.62 |
| Garrett et al. (OFD + GTR-NR) 1997 | USA | 64 | 64 | Doxycycline 100 mg b.i.d. the day of surgery and q.d. for 13 days | 1.6 ± 0.2 | 2.1 ± 0.4 | 2.1 ± 0.45 | - |
| Bouchard et al. (OFD + GTR-NR) 1997 | France | 15 | 15 | Amoxicillin + clavulanic 1.5 g q.d. for 14 days | 1.2 ± 1.2 | 2.7 ± 1.2 | 1.8 ± 1.3 | - |
| Hugoson et al. (OFD + GTR-NR) 1995 | Sweden | 38 | 38 | No Antibiotics | 0.8 ± 1.4 | 2.2 ± 2 | 2 ± 1 | - |
| Karapataki et al. (OFD + GTR-NR) 1999 | Sweden | 11 | 11 | No antibiotics | 0.5 ± 1.2 | 0.5 ± 2.5 | - | - |
| Leite et al. (OFD + GTR-NR) 2013 * | Brazil | 12 | 12 | Amoxicillin + clavulanic 500 mg t.i.d for 10 days starting the day before surgery | 0.02 ± 1.32 | - | 0.43 ± 0.84 | 1.36 ± 1.57 |
| Leite et al. (OFD + GTR-NR) 2013 | Brazil | 12 | 12 | Amoxicillin + clavulanic 500 mg t.i.d for 10 days starting the day before surgery | 0.24 ± 1.15 | - | 0.37 ± 1.03 | 1.18 ± 1.08 |
| Villaça et al. (OFD + GTR-NR) 2004 | Brazil | 10 | 10 | Amoxicillin + clavulanic 500 mg t.i.d for 10 days starting the day before surgery | § | - | § | § |
| Villaça et al. (OFD + GTR-NR) 2004 † | Brazil | 10 | 10 | Amoxicillin + clavulanic 500 mg t.i.d for 10 days starting the day before surgery | § | - | § | § |
| Combinations | ||||||||
| Maragos et al. (OFD + GTR-R + DFDBA) 2002 | USA | - | 14 | Doxycycline 100 mg q.d. for 10 days | 2.6 ± 0.3 | - | - | 2.2 ± 0.15 |
| Jaiswal et al. (OFD + GTR-R + DFDBA) 2013 | India | 10 | 10 | Amoxicillin 500 mg t.i.d for 7 days | 0.85 ± 0.31 | - | 0.8 ± 0.72 | - |
| de Leonardis et al. (OFD + GTR-R + DFDBA) 1999 | Italy | 12 | 12 | Amoxicillin 875 mg + clavulanic 125 mg b.i.d. for 7 days | 2.3 ± 0.85 | - | 2.8 ± 0.9 | - |
| Garrett et al. (CAF + GTR-R + DFDBA) 1990 | USA | 13 | 15 | Penicillin or erythromycin 250 mg q.i.d. for 14 days | - | - | 2.2 ± 0.3 | 2 ± 2.1 |
| Garrett et al. (OFD + DFDBA) 1990 | USA | 12 | 16 | Penicillin or erythromycin 250 mg q.i.d. for 14 days | - | - | 2.6 ± 1.13 | 2.6 ± 1.1 |
| Gantes et al. (OFD + DFDBA) 1991 | USA | 13 | 13 | Tetracycline 250 mg q.i.d for 14 days | ∫ | - | ∫ | - |
| Jaiswal et al. (OFD + GTR-R + DFDBA + EMD) 2013 | India | 10 | 10 | Amoxicillin 500 mg t.i.d for 7 days | 2.12 ± 1.07 | - | 1.74 ± 1 | - |
| de Santana et al. (CAF + GTR-R + HA) 1999 | USA | 15 | 15 | Doxycycline 200 mg day of surgery and 100 mg q.d for 19 days | 1.57 ± 1.32 | 2.13 ± 1.52 | 2.43 ± 1.36 | - |
| Santana et al. (CAF + GTR-NR + HA) 2009 | Brazil | 30 | 30 | Doxycycline 200 mg day of surgery and 100 mg q.d for 19 days | 3.05 ± 0.6 | - | 3.56 ± 0.6 | - |
| Jepsen et al. (OFD + EMD) 2004 | Germany | 45 | 45 | No Antibiotics | - | - | - | 2.6 ± 1.8 |
| Queiroz et al. (OFD + EMD) 2016 | Brazil | 13 | 13 | No Antibiotics | 2.08 ± 1.61 | 2.77 ± 0.93 | 2.54 ± 0.78 | - |
| Queiroz et al. (OFD + bTCP/HA) 2016 | Brazil | 14 | 14 | No Antibiotics | 2.29 ± 1.27 | 2.64 ± 0.93 | 2.36 ± 1.01 | - |
| Queiroz et al. (OFD + bTCP/HA + EMD) 2016 | Brazil | 14 | 14 | No Antibiotics | 2.14 ± 1.29 | 2.93 ± 0.83 | 2.43 ± 1.02 | - |
| Treatment | Number of Arms | Outcome | Difference | CI | p−Value |
|---|---|---|---|---|---|
| Overall/any treatment | AB− (32 arms) | PPD | −0.91 mm | −1.3 to −0.51 | <0.001 |
| AB+ (82 arms) | |||||
| AB− (32 arms) | CAL | −0.92 mm | −1.32 to −0.52 | <0.001 | |
| AB+ (82 arms) | |||||
| AB− (15 arms) | BG | −1.1 mm | −1.63 to −0.53 | <0.001 | |
| AB+ (39 arms) | |||||
| EMD | AB− (13 arms) | PPD | −0.98 mm | −1.65 to −0.32 | 0.004 |
| AB+ (15 arms) | |||||
| AB− (13 arms) | CAL | −0.98 mm | −1.77 to −0.19 | 0.015 | |
| AB+ (15 arms) | |||||
| BRG + GTR-R | AB− (10 arms) | PPD | −0.22 mm | −0.94 to 0.5 | 0.553 |
| AB+ (23 arms) | |||||
| AB− (10 arms) | CAL | −0.15 mm | −0.91 to 0.6 | 0.688 | |
| AB+ (23 arms) | |||||
| Type of AB | Tetracycline (17 arms) | PPD | −0.25 mm | −0.79 to 0.29 | 0.360 |
| Penicillin (55 arms) | |||||
| Tetracycline (17 arms) | CAL | −0.24 mm | −0.73 to 0.25 | 0.338 | |
| Penicillin (55 arms) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nibali, L.; Buti, J.; Barbato, L.; Cairo, F.; Graziani, F.; Jepsen, S. Adjunctive Effect of Systemic Antibiotics in Regenerative/Reconstructive Periodontal Surgery—A Systematic Review with Meta-Analysis. Antibiotics 2022, 11, 8. https://doi.org/10.3390/antibiotics11010008
Nibali L, Buti J, Barbato L, Cairo F, Graziani F, Jepsen S. Adjunctive Effect of Systemic Antibiotics in Regenerative/Reconstructive Periodontal Surgery—A Systematic Review with Meta-Analysis. Antibiotics. 2022; 11(1):8. https://doi.org/10.3390/antibiotics11010008
Chicago/Turabian StyleNibali, Luigi, Jacopo Buti, Luigi Barbato, Francesco Cairo, Filippo Graziani, and Søren Jepsen. 2022. "Adjunctive Effect of Systemic Antibiotics in Regenerative/Reconstructive Periodontal Surgery—A Systematic Review with Meta-Analysis" Antibiotics 11, no. 1: 8. https://doi.org/10.3390/antibiotics11010008