
Long-Term Outcomes in Patients on Life-Long Antibiotics: A Five-Year Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics
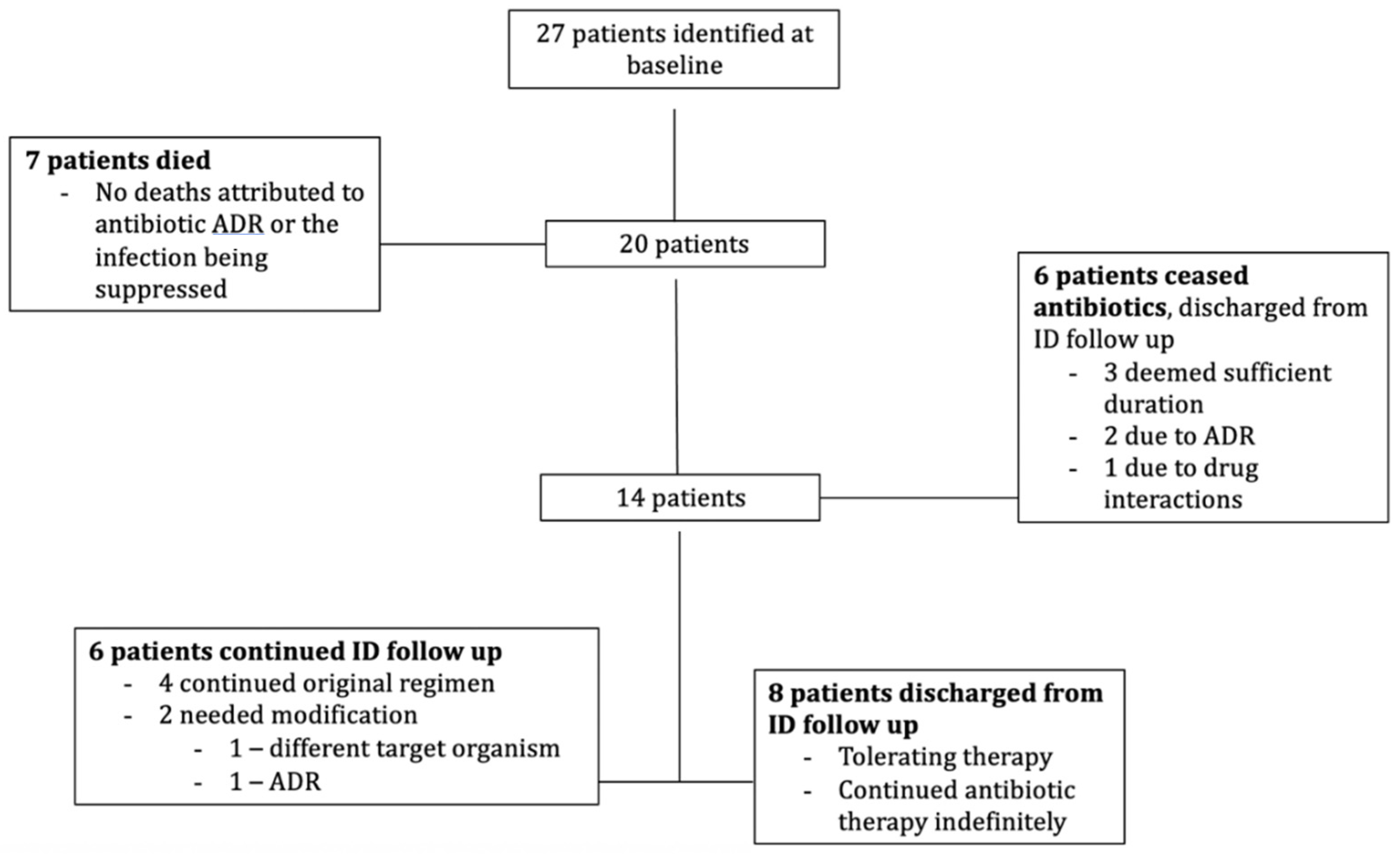
2.2. Patient Outcomes
2.3. Follow Up
2.4. Adverse Events
2.5. MRO Colonisation
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chain, E.; Florey, H.W.; Adelaide, M.B.; Gardner, A.D.; Heatley, N.G.; Jennings, M.A.; Orr-Ewing, J.; Sanders, A.G. Penicillin as a chemotherapeutic agent. Clin. Orthop. Relat. Res. 1940, 236, 226–228. [Google Scholar] [CrossRef]
- Lau, J.S.Y.; Korman, T.M.; Woolley, I. Life-long antimicrobial therapy: Where is the evidence? J. Antimicrob. Chemother. 2018, 73, 2601–2612. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.S.Y.; Bhatt, S.; Streitberg, R.; Bryant, M.; Korman, T.M.; Woolley, I. Surveillance of life-long antibiotics-A cross-sectional cohort study assessing patient attitudes and understanding of long-term antibiotic consumption. Infect. Dis. Health 2019, 24, 179–186. [Google Scholar] [CrossRef] [PubMed]
- CDC. Antibiotic Resistance Threats in the United States, 2019; U.S. Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019.
- Lau, J.S.; Kiss, C.; Roberts, E.; Horne, K.; Korman, T.M.; Woolley, I. Surveillance of life-long antibiotics: A review of antibiotic prescribing practices in an Australian Healthcare Network. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leijtens, B.; Weerwag, L.; Schreurs, B.W.; Kullberg, B.J.; Rijnen, W. Clinical Outcome of Antibiotic Suppressive Therapy in Patients with a Prosthetic Joint Infection after Hip Replacement. J. Bone Jt. Infect. 2019, 4, 268–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Byren, I.; Bejon, P.; Atkins, B.L.; Angus, B.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Berendt, A. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): Antibiotic duration and outcome. J. Antimicrob. Chemother. 2009, 63, 1264–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segreti, J.; Nelson, J.A.; Trenholme, G.M. Prolonged suppressive antibiotic therapy for infected orthopedic prostheses. Clin. Infect. Dis. 1998, 27, 711–713. [Google Scholar] [CrossRef] [PubMed]
- Erb, S.; Sidler, J.A.; Elzi, L.; Gurke, L.; Battegay, M.; Widmer, A.F.; Weisser, M. Surgical and antimicrobial treatment of prosthetic vascular graft infections at different surgical sites: A retrospective study of treatment outcomes. PLoS ONE 2014, 9, e112947. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Age | Sex | Antibiotic Regimen | Indication | Targeted Organism/s | Charlson Comorbidity Index Baseline End | MRO—Isolate Site | Cause of Death | Hospital Admission Days (Total/Infection Related/ICU) | Ongoing ID Follow Up | Duration of Follow Up (Years) | Regimen Adjustment/Reason | Adverse Drug Reactions ^ | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 70 | M | Amoxycillin | PVI | E. faecalis | 13 | 13 | ESBL E. coli—Urine | Lung Cancer | 13/7/0 | N/A | 5 months | N/A | |
| 76 | F | Rifampicin, Fusidic Acid, Pristinamycin | Chronic hip osteomyelitis (OM) | MRSA | 3 | 7 | MRSA—hip tissue VRE—Screening swab | Unknown (coroner’s case) | 109/64/5 | N/A | 7 | N/A | |
| 79 | M | amoxicillin/clavulanic acid, Ciprofloxacin | PJI | S. marcescens | 11 | 12 | VRE—Screening swab | Heart failure | 64/30/0 | N/A | 4 | Ceased amoxicillin/Deemed unnecessary + ADR | Oral Thrush |
| 56 | F | Flucloxacillin | PJI | MSSA | 4 | 6 | VRE—Screening swab ESBL E. coli—urine | Unknown (coroner’s case) | 106/102/14 | N/A | 4 | Added ciprofloxacin/Relapsed infection | Reflux |
| 70 | M | Cephalexin | Recurrent MSSA bacteraemia | MSSA | 6 | 7 | VRE—Screening swab | Chest sepsis | 17/15/15 | N/A | 4 | N/A | |
| 87 | F | Rifampicin, Fusidic Acid, ciprofloxacin | PJI | MRSA | 10 | 10 | MRSA—joint tissue | Myocardial Infarction | 7/0/0 | N/A | 2 | N/A | |
| 63 | F | Rifampicin, Amoxycillin, Doxycycline | PJI | C. amycolatum, E. faecalis, S. epidermidis | 2 | 2 | ESBL E. coli—urine | Intra-abdominal haemorrhage | 22/22/2 | N/A | 2 | N/A | |
| 65 | M | Cephalexin | Recurrent MSSA bacteraemia | MSSA | 3 | 7 | No | N/A | 86/79/2 | No | 5 | Ceased/deemed unnecessary | |
| 65 | M | Rifampicin, Fusidic Acid | PJI | MRSA | 5 | 5 | MRSA—joint tissue | N/A | 9/8/0 | No | 5 | Ceased/projected medication interactions | |
| 68 | M | Pristinamycin, Cotrimoxazole, Ciprofloxacin, Fluconazole | VGI | S. maltophilia, VRE, P. moteilii, C. albicans | 4 | 7 | VRE—abdominal pus ESBL K. pneumoniae—screening swab | N/A | 4/4/0 | No | 4 | Ceased/ADR | Acute kidney and liver injury |
| 70 | M | Amoxycillin | PJI | S. agalactiae | 6 | 8 | ESBL E. coli—urine | N/A | 7/2/0 | No | 1 | Ceased/Deemed unnecessary | |
| 56 | F | Cephalexin | PJI | MSSA | 4 | 7 | No | N/A | 0/0/0 | No | 3 | Ceased/Deemed unnecessary | Vaginal thrush |
| 59 | F | Cephalexin | PJI | S. agalactiae | 6 | 6 | MRSA—wound swab | N/A | 41/36/0 | No | 4 | Ceased/Inefficacy + ADR | Vaginal thrush |
| 65 | F | Flucloxacillin, Ciprofloxacin | PJI | MSSA, C. aurimucosum | 5 | 5 | VRE—screening swab | N/A | 360/314/8 | Yes | 7 | Changed to doxycycline/Failed definitive surgery, new target organism | |
| 69 | F | Rifampicin, Fusidic Acid | PJI | MRSA | 3 | 4 | MRSA—joint tissue | N/A | 25/0/0 | Yes | 5 | N/A | |
| 74 | M | amoxicillin-clavulanic acid Pristinamycin | VGI | S. typhimurium, VRE | 6 | 10 | VRE, CRE, E. cloacae—screening swab | N/A | 3/0/0 | Yes | 5 | Changed amoxicillin/clavulanic acid to amoxicillin/ADR | Diarrhoea |
| 78 | M | Rifampicin, Fusidic Acid | PJI | MRSA | 5 | 13 | MRSA, ESBL K. pneumoniae—Knee tissue | N/A | 12/9/0 | Yes | 6 | N/A | |
| 45 | F | Rifampicin Fusidic Acid | PJI | S. epidermidis, MSSA | 1 | 2 | No | N/A | 30/30/0 | Yes | 6 | N/A | |
| 69 | M | Rifampicin, Fusidic Acid | PJI | MRSA | 2 | 3 | MRSA—joint tissue | N/A | 0/0/0 | Yes | 9 | N/A | |
| 77 | M | Cephalexin | PJI | MSSA | 4 | 5 | No | N/A | 0/0/0 | No | 5 months | N/A | |
| 73 | F | Amoxycillin | Infected spinal metalware | PSSA | 9 | 9 | No | N/A | 0/0/0 | No | 2 months | N/A | |
| 45 | F | Penicillin | PVI | C. acnes | 1 | 3 | No | N/A | 0/0/0 | No | 1 | N/A | |
| 42 | F | Nitrofurantoin | Recurrent urinary tract infection | E. faecalis | 1 | 1 | No | N/A | 29/0/0 | No | 1 | N/A | |
| 59 | M | Clindamycin, Amoxycillin | VGI | S. epidermidis | 3 | 4 | No | N/A | 0/0/0 | No | 1 | N/A | |
| 88 | F | Cephalexin | Recurrent MSSA bacteraemia, OM | MSSA | 7 | 7 | MRSA, VRE—screening swab | N/A | 0/0/0 | No | 1 | N/A | |
| 86 | F | Rifampicin, Fusidic Acid | PJI | MRSA | 9 | 9 | MRSA—joint tissue | N/A | 34/26/0 | No | 4 | N/A | |
| 71 | M | Ciprofloxacin | Post laminectomy infection | E. cloacae, P. mirabilis | 7 | 7 | No | N/A | 2/0/0 | No | 1 | N/A | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiss, C.; Connoley, D.; Connelly, K.; Horne, K.; Korman, T.; Woolley, I.; Lau, J.S.Y. Long-Term Outcomes in Patients on Life-Long Antibiotics: A Five-Year Cohort Study. Antibiotics 2022, 11, 62. https://doi.org/10.3390/antibiotics11010062
Kiss C, Connoley D, Connelly K, Horne K, Korman T, Woolley I, Lau JSY. Long-Term Outcomes in Patients on Life-Long Antibiotics: A Five-Year Cohort Study. Antibiotics. 2022; 11(1):62. https://doi.org/10.3390/antibiotics11010062
Chicago/Turabian StyleKiss, Christopher, Declan Connoley, Kathryn Connelly, Kylie Horne, Tony Korman, Ian Woolley, and Jillian S. Y. Lau. 2022. "Long-Term Outcomes in Patients on Life-Long Antibiotics: A Five-Year Cohort Study" Antibiotics 11, no. 1: 62. https://doi.org/10.3390/antibiotics11010062