2. Materials and Methods
The patients who entered the hospital’s ICU of Botucatu Medical School from August 2016 to July 2017 and initiated vancomycin in the preceding 48 h were included in a prospective cohort study. The quick-SOFA tool was used to identify patients with sepsis [
2]. The initial dose of vancomycin was 25 mg/kg at a maintenance of 15 mg/kg. The dosing interval was 12/12 h up to 96/96 h, varying according to the serum concentration.
The following patients were excluded: patients who developed AKI in less than 48 h from the start of vancomycin use, patients with installed AKI before the introduction of vancomycin, patients with AKI of other etiologies (obstructive, vascular, glomerular, or ischemic AKI), kidney transplant, or stage V of chronic kidney disease (with estimated or measured serum creatinine clearance less than 15 mL/min), patients who were pregnant, or under 18 years old.
This study was registered in the Brazilian Registry of clinical trials (ReBEC) under Number RBR-4zrwtz and was approved by the Research Ethics Committee of Botucatu School of Medicine with number CAAE 65827117.4.0000.5411. All the research was performed following current regulations and a written informed consent statement was obtained from all participants or their legal guardians.
The patient included in the study had his clinical and laboratory evaluation taken daily by the same observer, who consulted his electronic medical record until his treatment with vancomycin or his clinical outcome ended.
The lowest value baseline creatinine was considered in 6 months if the prior creatinine or lower creatinine were available during hospitalization since the patient was not on dialysis. KDIGO used the AKI definitions as any of the following: increase in serum creatinine by 0.3 mg/dL or more within 48 h, or increase in serum creatinine to 1.5 times baseline or more within the last 7 days, or urine output less than 0.5 mL/kg/h for 6 h [
5].
The serum toxic, subtherapeutic, and therapeutic concentrations were defined as trough concentrations higher than 20 mg/L, lower than 15 mg/L, and between 15 and 20 mg/L, respectively, in two consecutive dosages.
Frequency and measures of central tendency and dispersion were calculated for the categorical and continuous variables, respectively, and established as outcome variables: AKI and death. Student’s t-test was used to compare parametric variables between two groups and the Mann–Whitney test was used for non-parametric variables. Categorical variables were compared with the chi-square or Fisher’s exact test. Variables with significant univariate associations were considered as candidates for Cox regression analysis, which was performed using backward variable selection, with the exit criteria set at p < 0.20.
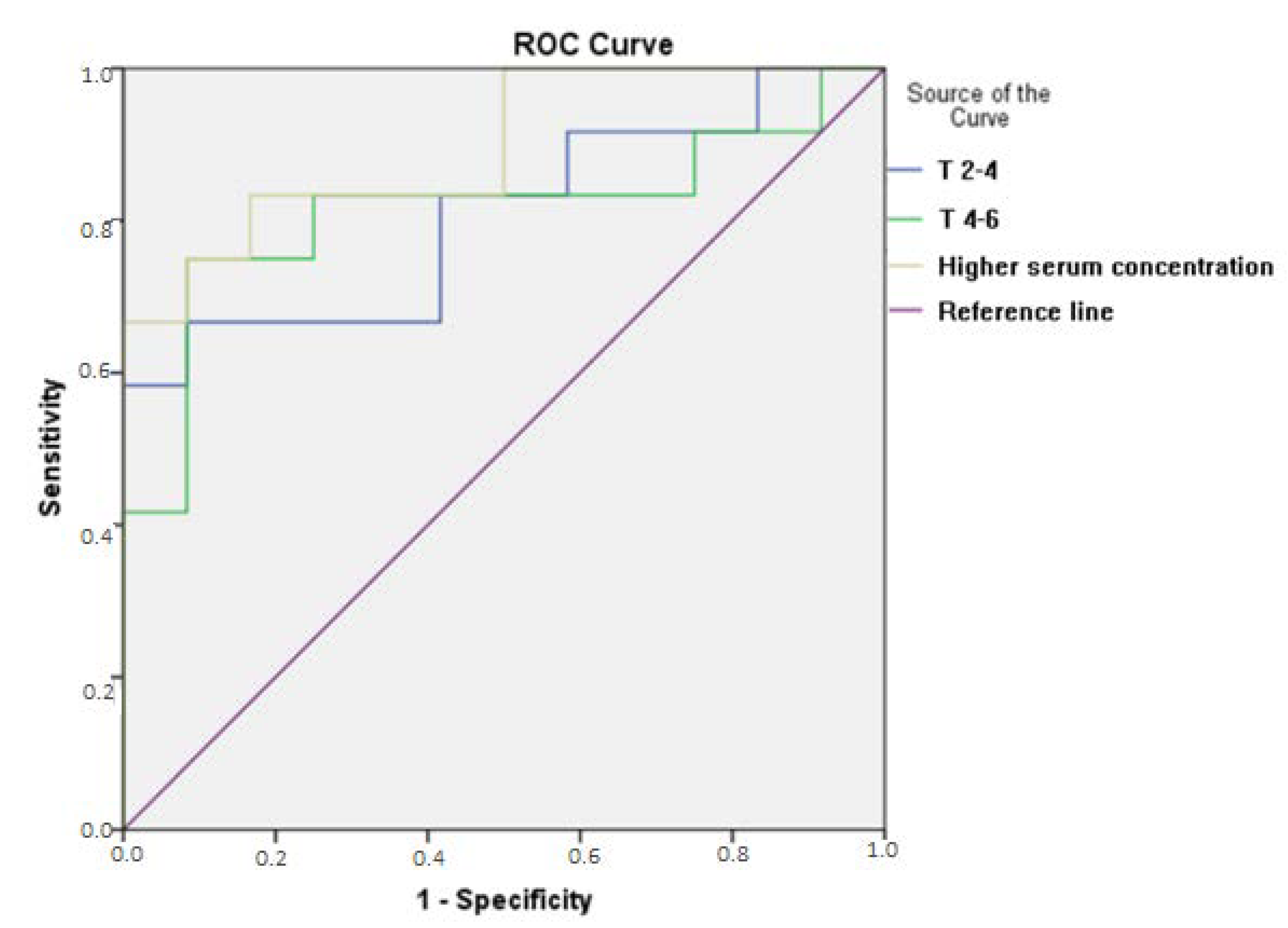
ROC curves were built to evaluate the cutoff points of serum concentration of vancomycin as predictors of the diagnosis and prognosis of AKI in the moments until the second day (T0-2), between the second and the fourth days (T2-4), and between the fourth and the sixth days (T4-6).
Areas under the curve (AUC) between 0.7 and 0.79 were considered a satisfactory performance and between 0.8 and 0.89 an optimum performance.
Using Lee Formula for an alpha error of 0.05 and study power of 80%, the sample size calculation was performed, and considering that the prevalence of the AKI outcome would be 30% higher in patients with a toxic concentration of vancomycin [
12], 30 patients were estimated with toxic concentrations and 30 without toxic concentrations (total of 60 patients).
3. Results
We evaluated 63 patients (
Figure 1), aged 54.67 ± 18.7 years, with a male predominance (66.7%), BMI 26.1 ± 6.8, and the use of vancomycin for 11.4 ± 7.33 days. The vast majority of patients (92%) had performed the serum vancomycin measurement, the number of serum concentrations dosages and the number of posologic adjustments were 3.87 and 1.84, respectively; 53.96% were in concentrations considered toxic (higher than 20 mg/L), an average of 25.5 ± 11.90 mg/L. AKI prevalence was 44.4%, with the stage KDIGO 3 being most common (46.4%), and 46% died.
Clinical and laboratory variables are shown in
Table 1, and vancomycin characteristics are shown in
Table 2, distinguishing patients who developed AKI or not.
The only variable identified as a risk factor for AKI was the vancomycin concentration between the second and the fourth days (T2-4) in the Cox regression analysis (HR = 1.086,
p = 0.009), without statistically significant differences in other variables, as shown in
Table 3.
Vancomycin serum concentration in T2-4 days higher than 17.53 was a predictor of AKI with a sensitivity of 79.7% and specificity of 83.3% by ROC curve analysis, with an AUC of 0.806 (IC 95% 0.624–0.987,
p = 0.011), as shown in
Figure 2. AKI occurred on average on the sixth day of vancomycin use, and the founded value preceded the diagnosis of AKI by two days.
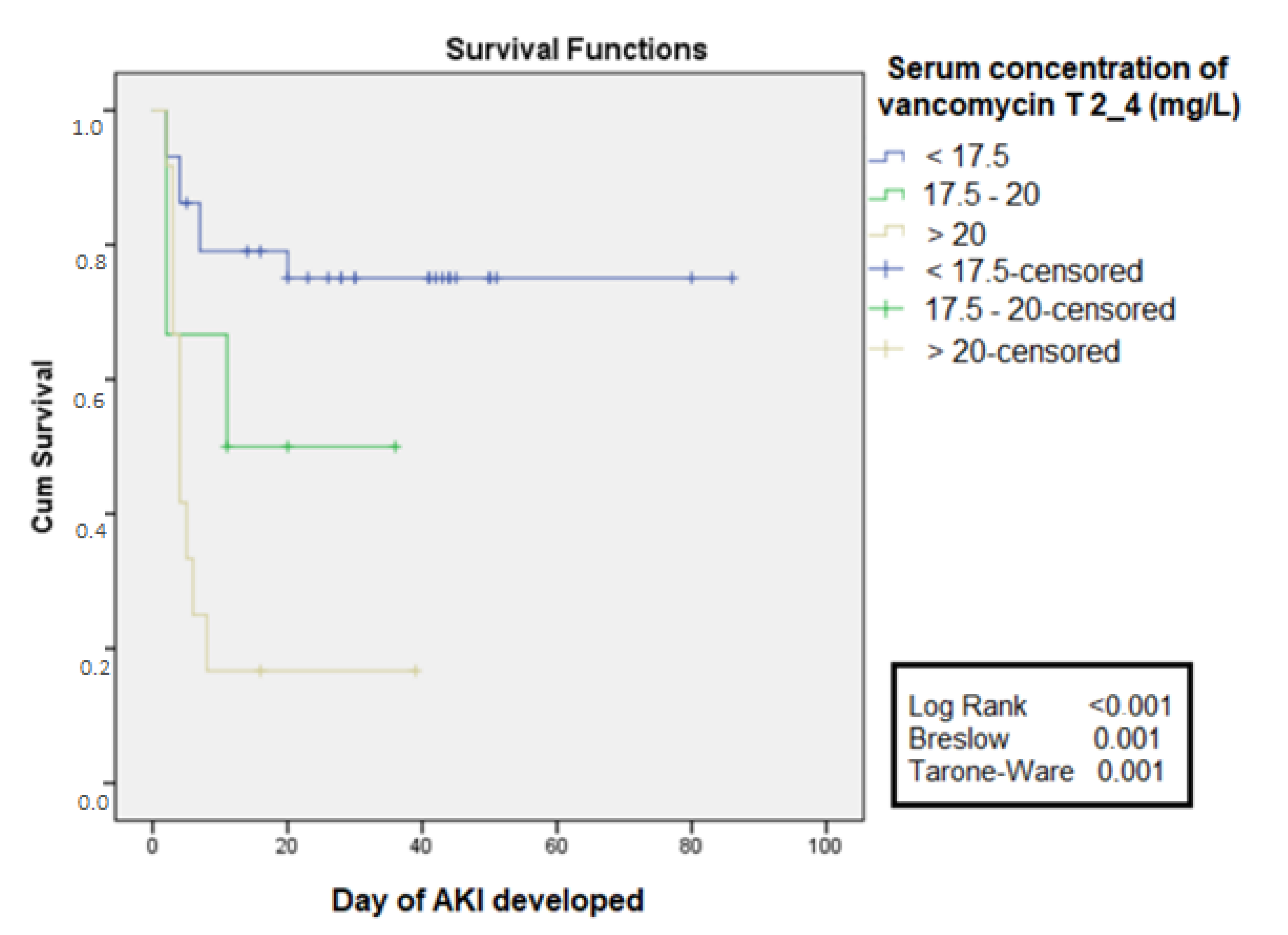
Based on the values of cutoff obtained by the ROC curve at 2 to 4 days, the free time curve for AKI was constructed. It was observed that in the group with serum concentration >20 mg/L the free time for the development of AKI was lower when compared to the group that had serum concentrations between 17.5 and 20 mg/L, which also presented shorter free time compared to the group with a serum concentration <17.5 mg/L, log-rank <0.001 (
Figure 3).
Table 4 shows the clinical and laboratory variables, and
Table 5 shows the characteristics related to vancomycin, distinguishing patients who died or survived.
When the two groups were analyzed using Cox regression, it was observed that the variables age (HR = 1.13,
p= 0.018), glomerular filtration rate estimated by CKD-EPI (HR 1.23,
p = 0.015), levels of serum concentration at the moment 2 to 4 days (HR = 1.60,
p = 0.021) and mean C-protein reactive value (HR 1.26,
p = 0.011) were identified as risk factors for death, as shown in
Table 6.
Based on the values of cutoff obtained by the ROC curve at 2 to 4 days, the free time curve for death was constructed. It was observed that, in the group with serum concentration >20 mg/L, the free time for the development of AKI was lower when compared to the group that had serum concentrations between 17.5 and 20 mg/L, which also presented a lower free time compared to the group with a serum level <17.5 mg/L and log-rank 0.018, as shown in
Figure 4.
4. Discussion
Due to the pharmacokinetic changes of the critical patient related to the drug distribution, elimination, and metabolization, two concerns still permeate vancomycin use, related to its efficacy and safety. There is an increased risk of subtherapeutic concentrations, which may compromise the treatment and induce bacterial resistance. On the other hand, it is a drug whose main side effect is nephrotoxicity, with AKI risk and short- and long-term problems.
This study assessed the impact of therapeutic monitoring of vancomycin on clinical outcomes. It is known that the serum concentration of vancomycin in the trough between 15 and 20 mg/L corresponds to an area under the curve over the minimum inhibitory concentration (AUC/MIC) equal or greater than 400, determining the optimum activity of the antimicrobial [
10,
11]. However, the association between serum vancomycin concentration and clinical outcomes is poorly studied.
Were evaluated 182 critically ill patients using vancomycin, and 63 patients were included in the study. This difficulty of studying vancomycin nephrotoxicity arises from the following problem: high serum levels are a consequence or cause of AKI due to the accumulation of the drug, which is caused by a reduction in its renal whitening due to septic AKI, as approached by Álvarez et al. [
12] and by American guideline [
11]. Therefore, the presence of AKI already installed or started before 48 h of vancomycin use was an exclusion criteria for this study.
Most critically ill patients (92%) had performed the serum vancomycin measurement, and the mean measurements of serum concentrations and dose adjustments were 3.87 and 1.84, respectively. Considering that the average time of use was 11.43 days, and according to the protocol already established in the literature, there is an indication that it is not always serum concentrations determined and adjusted by the ICU team, which can contribute to subtherapeutic concentrations of the antimicrobial. Iwamoto et al. [
13] found an increased risk of AKI and nephrotoxicity in patients who were not submitted to the monitoring of serum concentrations of vancomycin (OR = 0.25 and
p < 0.05).
A study conducted by Davis et al. [
14] assessed adherence to the guidelines established by the American consensus [
11] and showed that only 19% of the institutions questioned used a standard definition to identify nephrotoxicity associated with vancomycin. The most current 2020 guidelines recommend using Bayesian-derived AUC monitoring rather than trough concentrations [
14].
Despite the availability of therapeutic drug monitoring, there is a difficulty in achieving and maintaining adequate serum concentrations, especially in the intensive care environment, due to the collection, the patient, and the pharmacokinetic variation of the drugs [
8]. In our study, this difficulty also occurred, with high rates of toxic and subtherapeutic concentration.
AKI occurred in 44.4% of patients, with a mortality rate of 46%. On average, the development of AKI occurred on the sixth day of vancomycin use, compatible with data from the literature in which nephrotoxic AKI generally occurs from 4 to 8 days after the initiation of treatment [
15,
16]. Such data indicate that it was possible to evaluate the role of the nephrotoxicity of vancomycin as the cause of AKI in septic patients in ICUs. Since the role of sepsis was more critical than that of nephrotoxicity, the incidence of AKI (close to 60%), as well as mortality (higher than 70%), would be higher.
The only variable that showed an association with AKI by Cox regression analysis was the highest level of serum vancomycin between the second and fourth days. It differs from previous studies that identified other variables (use of vasoactive drugs, basal creatinine, and age) as predictors of AKI in ICU patients [
17,
18]. In our study, we evaluated a specific population using vancomycin after ICU admission, and patients with AKI were excluded before introducing the antimicrobial agent, which could justify the different risk factors identified in other studies.
Serum concentrations above 17.53 mg/L between the second and fourth day of use were an excellent predictor of AKI in the critical population, with AUC higher than 0.8 and sensitivity and specificity close to 80%, preceding the diagnosis of AKI in at least 48 h. However, this value is within the range considered therapeutic for severe infections (15–20 mg/L), suggesting that therapeutic concentrations should be less in the critical population due to the presence of other risk factors for AKI: advanced age, previously diminished renal function, dehydration, and the duration of sepsis; the concomitant administration with other nephrotoxic drugs, such as amphotericin B, aminoglycosides, intravenous contrast way, and loop diuretics; and the need for vasopressors due to hemodynamic instability [
19,
20]. A free time curve was built for AKI, stratifying the serum concentration levels in less than 17.5 mg/L, between 17.5 mg/L and 20 mg/L, and higher than 20 mg/L, showing the shorter free time and higher serum levels, with a significant difference between curves.
Bosso et al. [
15] evaluated 288 patients in a prospective multicentric study and found AKI in 29.6% of patients with serum concentrations levels higher than 15 mg/L and in 8.9% of the patients with vancomycin concentrations lower than 15 mg/L. Gupta et al. [
19] identified AKI incidence in 27% of patients, with vancomycin concentrations higher than 15 mg/L as a predictor of nephrotoxicity. Thus, it is questionable whether the ideal therapeutic concentrations aim to prevent AKI.
Age, mean PCR value, the serum concentration of vancomycin between the second and fourth days, and estimated glomerular filtration rate were associated with mortality. Chertow et al. [
20] showed that small increases in serum creatinine were significantly associated with the increase in AKI patients’ mortality. Liangos et al. [
21] found that chronic diseases such as diabetes melittus (DM) were associated with a higher risk of development of AKI, with a consequent increase in mortality. CPR concentration indicating systemic inflammation was shown in the literature associated with mortality, as presented by Villacorta et al. [
22] in patients with heart failure, in which CPR > 3 mg/dL was associated with a higher mortality in comparison to individuals with lower values (
p = 0.018).
This study presents some limitations: the obtained sample was small due to the difficulty of studying nephrotoxicity in critically ill patients, since there are many exclusion variables; the data were obtained in a single center; the agents’ resistance to vancomycin was not studied; and the serum concentration levels were not studied as a prognostic predictor of AKI (severity and need for acute renal support). Despite these limitations, this was the first study of the therapeutic monitoring of vancomycin to present cutoff values to refine the management in the population of septic patients in an intensive care scenario, when AUC cannot be used.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}