
Clinical Validation of the Greek Version of the Acute Cystitis Symptom Score (ACSS)—Part II

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Study Subjects
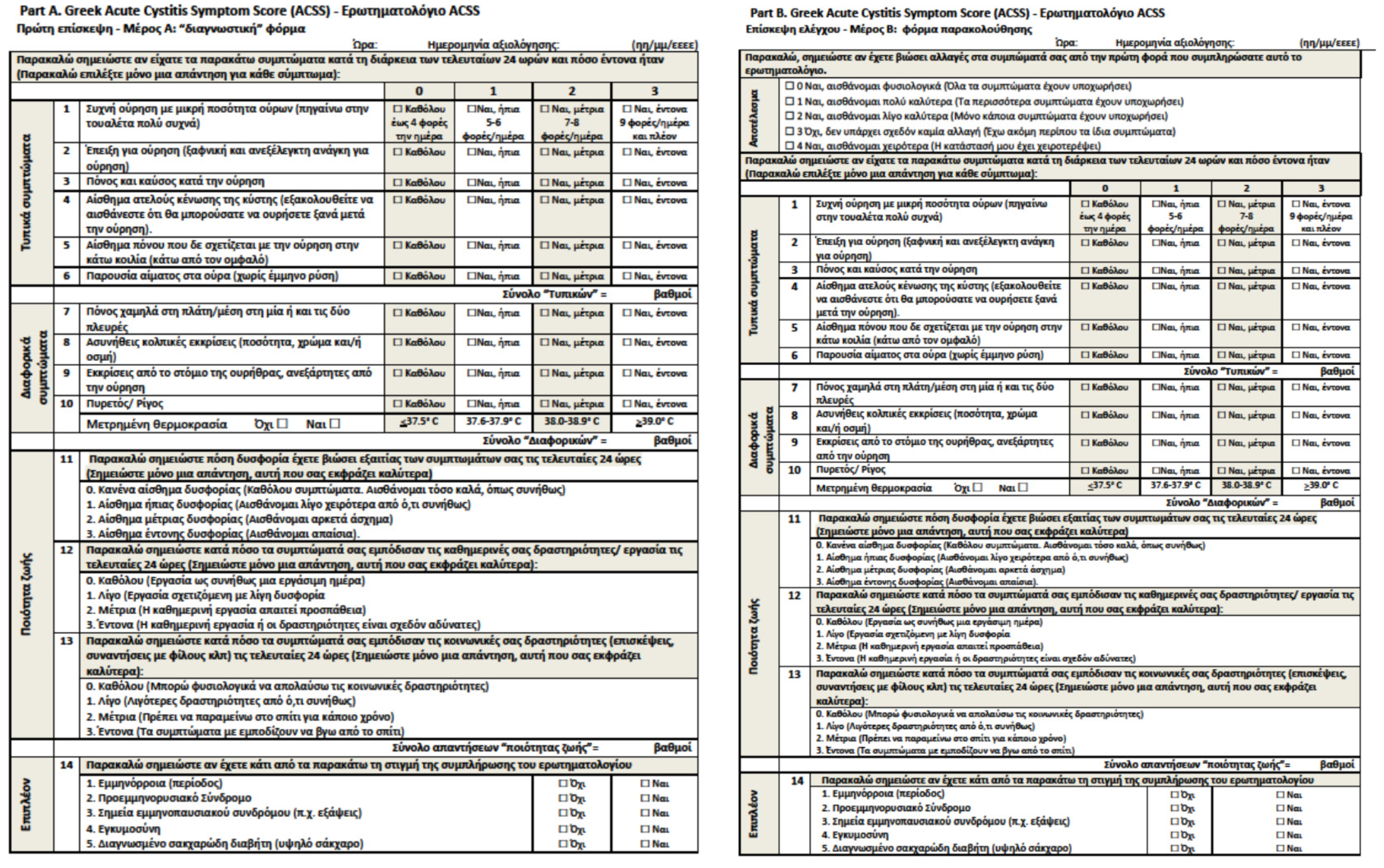
4.3. Study Tool
4.4. Statistical Analysis
4.4.1. Data Processing
4.4.2. Statistical Tests
4.4.3. Sample Size Calculation
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choe, H.S.; Lee, S.J.; Cho, Y.H.; Cek, M.; Tandogdu, Z.; Wagenlehner, F.; Bjerklund-Johansen, T.E.; Naber, K.; GPIU Asian Investigators. Aspects of urinary tract infections and antimicrobial resistance in hospitalized urology patients in Asia: 10-Year results of the Global Prevalence Study of Infections in Urology (GPIU). J. Infect. Chemother. 2018, 24, 278–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colgan, R.; Williams, M. Diagnosis and treatment of acute uncomplicated cystitis. Am. Fam. Physician 2011, 84, 771–776. [Google Scholar] [PubMed]
- Najar, M.S.; Saldanha, C.L.; Banday, K.A. Approach to urinary tract infections. Indian J. Nephrol. 2009, 19, 129–139. [Google Scholar] [CrossRef]
- Anger, J.; Lee, U.; Ackerman, A.L.; Chou, R.; Chughtai, B.; Clemens, J.Q.; Hickling, D.; Kapoor, A.; Kenton, K.S.; Kaufman, M.R.; et al. Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. J. Urol. 2019, 202, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Ternes, B.; Wagenlehner, F.M.E. Guideline-based treatment of urinary tract infections. Urol. A 2020, 59, 550–558. [Google Scholar] [CrossRef]
- Cai, T.; Cocci, A.; Gacci, M.; Verze, P.; Bonkat, G.; Köves, B.; Wagenlehner, F.; Bartoletti, R.; Bjerklund Johansen, T.E. Guidelines in urology: Lights and shadows. Urologia 2020, 87, 125–129. [Google Scholar] [CrossRef]
- Köves, B.; Cai, T.; Veeratterapillay, R.; Pickard, R.; Seisen, T.; Lam, T.B.; Yuan, C.Y.; Bruyere, F.; Wagenlehner, F.; Bartoletti, R.; et al. Benefits and harms of treatment of asymptomatic bacteriuria: A systematic review and meta-analysis by the European Association of Urology Urological Infection Guidelines Panel. Eur. Urol. 2017, 72, 865–868. [Google Scholar] [CrossRef]
- Franz, M.; Horl, W.H. Common errors in diagnosis and management of urinary tract infection. I: Pathophysiology and diagnostic techniques. Nephrol. Dial. Transpl. 1999, 14, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Alidjanov, J.F.; Abdufattaev, U.A.; Makhmudov, D.; Mirkhamidov, D.; Khadzhikhanov, F.A.; Azgamov, A.V.; Pilatz, A.; Naber, K.G.; Wagenlehner, F.M.; Akilov, F.A. Development and clinical testing of the Russian version of the Acute Cystitis Symptom Score—ACSS. Urologiia 2014, 6, 14–22. [Google Scholar]
- Alidjanov, J.F.; Abdufattaev, U.A.; Makhsudov, S.A.; Pilatz, A.; Akilov, F.A.; Naber, K.G.; Wagenlehner, F.M. New self-reporting questionnaire to assess urinary tract infections and differential diagnosis: Acute cystitis symptom score. Urol. Int. 2014, 92, 230–236. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M.E. Reevaluation of the Acute Cystitis Symptom Score, a Self-Reporting Questionnaire. Part I. Development, Diagnosis and Differential Diagnosis. Antibiotics 2018, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M. Reevaluation of the Acute Cystitis Symptom Score, a Self-Reporting Questionnaire. Part II. Patient-Reported Outcome Assessment. Antibiotics 2018, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamatiou, K.; Samara, E.; Alidjanov, J.F.; Naber, K.G.; Pilatz, A.M.E.; Wagenlehner, F.M.E. The impact of education level and age in the linguistic validation of the acute cystitis symptom score questionnaire. Hell. Urol. 2021, in press. [Google Scholar]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Evaluation of the draft guidelines proposed by EMA and FDA for the clinical diagnosis of acute uncomplicated cystitis in women. World J. Urol. 2020, 38, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Additional assessment of Acute Cystitis Symptom Score questionnaire for patient-reported outcome measure in female patients with acute uncomplicated cystitis: Part II. World J. Urol. 2020, 38, 1977–1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magyar, A.; Alidjanov, J.; Adrian, A.; Nagya, K.; Adithyaa Arthanareeswaran, V.K.; Bécsi, A.; Wagenlehner, F.; Naber, K.; Tenke, P.; Köves, B. The role of Acute Cystitis Symptom Score questionnaire for research and antimicrobial stewardship. Validation of the Hungarian version. Cent. Eur. J. Urol. 2018, 71, 134–141. [Google Scholar] [CrossRef]
- Di Vico, T.; Morganti, R.; Cai, T.; Naber, K.G.; Wagenlehner, F.M.E.; Pilatz, A.; Alidjanov, J.; Morelli, G.; Bartoletti, R. Acute Cystitis Symptom Score (ACSS): Clinical validation of the Italian version. Antibiotics 2020, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Wagenlehner, F.M. Validation of the American English Acute Cystitis Symptom Score. Antibiotics 2020, 9, 929. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Khudaybergenov, U.A.; Ayubov, B.A.; Pilatz, A.; Mohr, S.; Munst, J.C.; Ziviello Yuen, O.N.; Pilatz, S.; Christmann, C.; Dittmar, F.; et al. Linguistic and clinical validation of the acute cystitis symptom score in German-speaking Swiss women with acute cystitis. Int. Urogynecol. J. 2021, 1–12. [Google Scholar] [CrossRef]
- Gágyor, I.; Bleidorn, J.; Kochen, M.M.; Schmiemann, G.; Wegscheider, K.; Hummers-Pradier, E. Ibuprofen versus fosfomycin for uncomplicated urinary tract infection in women: Randomised controlled trial. BMJ 2015, 351, h6544. [Google Scholar] [CrossRef] [Green Version]
- Vik, I.; Bollestad, M.; Grude, N.; Bærheim, A.; Damsgaard, E.; Neumark, T.; Bjerrum, L.; Cordoba, G.; Olsen, I.C.; Lindbæk, M. Ibuprofen versus pivmecillinam for uncomplicated urinary tract infection in women-A double-blind, randomized non-inferiority trial. PLoS Med. 2018, 15, e1002569. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, A.; Bütikofer, L.; Odutayo, A.; Mühlemann, K.; da Costa, B.R.; Battaglia, M.; Meli, D.N.; Frey, P.; Limacher, A.; Reichenbach, S.; et al. Symptomatic treatment of uncomplicated lower urinary tract infections in the ambulatory setting: Randomised, double blind trial. BMJ 2017, 359, j4784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenlehner, F.M.; Abramov-Sommariva, D.; Höller, M.; Steindl, H.; Naber, K.G. Non-antibiotic herbal therapy (BNO 1045) versus antibiotic therapy (Fosfomycin Trometamol) for the treatment of acute lower uncomplicated urinary tract infections in women: A double-blind, parallel-group, randomized, multicentre, non-inferiority phase III trial. Urol. Int. 2018, 101, 327–336. [Google Scholar] [PubMed]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M. Reliability of Symptom-Based Diagnosis of Uncomplicated Cystitis. Urol. Int. 2019, 102, 83–95. [Google Scholar] [CrossRef]
- Levene, H. Robust tests for equality of variances. In Contributions to Probability and Statistics Essays in Honor of Harold Hotelling; Olkin, I., Ed.; Stanford University Press: Stanford, CA, USA, 1960. [Google Scholar]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Student. The Probable Error of a Mean. Biometrika 1908, 6, 1–25. [Google Scholar] [CrossRef]
- McNemar, Q. Note on the sampling error of the difference between correlated proportions or percentages. Psychometrika 1947, 12, 153–157. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biom. Bull. 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Pearson, K.; Galton, F. Note on regression and inheritance in the case of two parents. Proc. R. Soc. Lond. 1895, 58, 240–242. [Google Scholar] [CrossRef]
- R Core Team, R. A Language and Environment for Statistical Computing; The Comprehensive R Archive Network (CRAN): Vienna, Austria, 2017; Available online: https://cran.r-project.org/ (accessed on 10 October 2021).
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Yumpu: Diepoldsau, Switzerland, 2020. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An Open-Source Package for R and S+ to Analyze and Compare ROC Curves; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Stevenson, M.; Nunes, T.; Heuer, C.; Marshall, J.; Sanchez, J.; Thornton, R.; Reiczigel, J.; Robison-Cox, J.; Sebastiani, P.; Solymos, P.; et al. epiR: Tools for the Analysis of Epidemiological Data. 2017. Available online: https://cran.r-project.org/web/packages/epiR/epiR.pdf (accessed on 31 August 2021).
- Wickham, H. Tidyverse: Easily Install and Load the ‘Tidyverse’. 2017. Available online: https://tidyverse.tidyverse.org/ (accessed on 10 October 2021).
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, S80–S89. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Cohort | Controls | Patients | p-Value * |
|---|---|---|---|---|
| Number, n (%) | 92 (100.0) | 39 (100.0) | 53 (100.0) | n.a. |
| Age, yr, mean (SD) | 46.7 (16.6) | 49.3 (15.9) | 44.7 (17.0) | 0.189 |
| Employment | ||||
| Full-time, n (%) | 16 (17.4) | n.a. | 16 (30.2) | n.a. |
| Part-time, n (%) | 17 (18.5) | n.a. | 17 (32.1) | n.a. |
| Not working, n (%) | 14 (15.2) | n.a. | 14 (26.4) | n.a. |
| Retired, n (%) | 6 (6.5) | n.a. | 6 (11.3) | n.a. |
| Sexually active, n (%) | 44 (47.8) | n.a. | 44 (83.0) | n.a. |
| Symptomatic episodes of lower UTI within the last year | ||||
| No symptomatic episode, n (%) | 47 (51.1) | n.a. | 47 (88.7) | n.a. |
| One or two symptomatic episodes, n (%) | 6 (6.5) | n.a. | 6 (11.3) | n.a. |
| Received antimicrobial therapy within the last 3 months, n (%) | 9 (9.8) | n.a. | 9 (17.0) | n.a. |
| Urine culture performed, n (%) | 53 (57.6) | 0 (0.0) | 53 (100.0) | n.a. |
| Characteristics following ACSS’s ‘Additional’ domain | ||||
| Cases with menstruation, n (%) | 9 (9.8) | 2 (5.1) | 7 (13.2) | 0.350 |
| Cases with premenstrual symptoms, n (%) | 9 (9.8) | 5 (12.8) | 4 (7.5) | 0.627 |
| Cases with symptoms of menopause, n (%) | 10 (10.9) | 3 (7.7) | 7 (13.2) | 0.616 |
| Cases with pregnancy, n (%) | 1 (1.0) | 0 (0.0) | 1 (1.9) | 1.000 |
| Cases with diabetes mellitus, n (%) | 6 (6.5) | 2 (5.1) | 4 (7.5) | 0.970 |
| Prescribed treatment modality | ||||
| Antimicrobial therapy, n (%) | 44 (47.8) | n.a. | 44 (83.0) | n.a. |
| Non-antimicrobial therapy, n (%) | 4 (4.3) | n.a. | 4 (7.5) | n.a. |
| Combined therapy, n (%) | 5 (5.4) | n.a. | 5 (9.4) | n.a. |
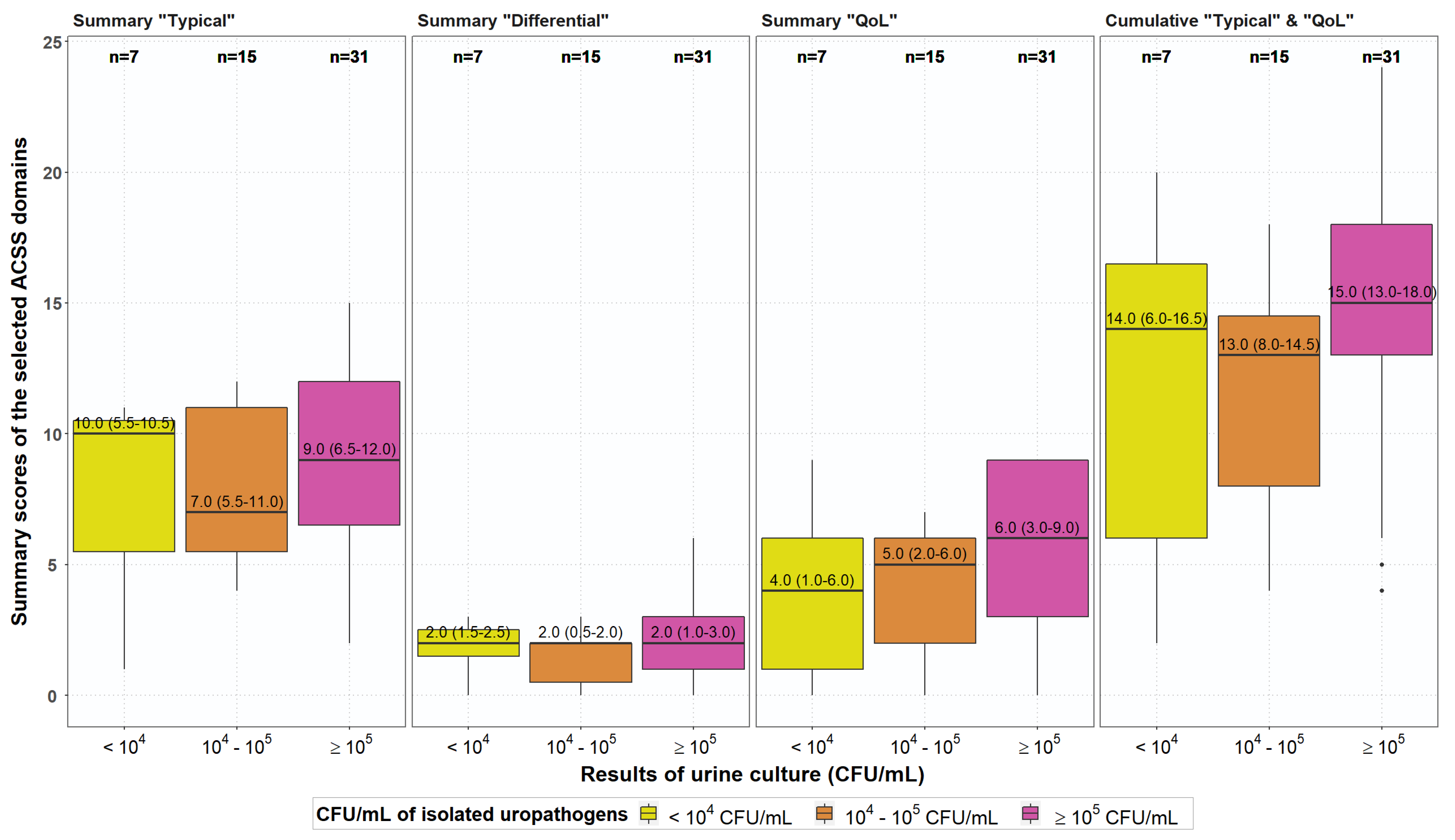
| Pathogens | Bacteriuria (Colony Forming Units (cfu) per mL) | |||
|---|---|---|---|---|
| ≥105/mL | 104/mL | 103/mL | 102/mL | |
| Escherichia coli | 28 | 13 | 1 | 1 |
| Proteus sp. | 2 | |||
| Klebsiella sp. | 2 | |||
| Enterococcus sp. | 1 | |||
| Staphylococcus CoN | 4 | 1 | ||
| Total n (%) | 31 (58.4%) | 15 (28.3%) | 5 (9.4%) | 2 (3.8%) |
| ACSS | Controls (n = 39) | Patients (n = 53) | p-Value | |||
|---|---|---|---|---|---|---|
| Domain | Item | Number | Percent | Number | Percent | |
| Typical Symptoms | 1. Urinary frequency positive | 17 | 43.6 | 49 | 92.4 | <0.001 |
| None | 22 | 56.4 | 4 | 7.6 | <0.001 | |
| Mild | 11 | 28.2 | 17 | 32.1 | 0.694 | |
| Moderate | 6 | 15.4 | 12 | 22.6 | 0.391 | |
| Severe | 0 | 0.0 | 20 | 37.7 | <0.001 | |
| 2. Urinary urgency positive | 7 | 17.9 | 45 | 84.9 | <0.001 | |
| None | 32 | 82.1 | 8 | 15.1 | <0.001 | |
| Mild | 5 | 12.8 | 18 | 34.0 | 0.015 | |
| Moderate | 2 | 5.1 | 13 | 24.6 | 0.007 | |
| Severe | 0 | 0.0 | 14 | 26.4 | <0.001 | |
| 3. Dysuria positive | 0 | 0.0 | 37 | 69.8 | <0.001 | |
| None | 39 | 100.0 | 16 | 30.2 | <0.001 | |
| Mild | 0 | 0.0 | 20 | 37.7 | <0.001 | |
| Moderate | 0 | 0.0 | 11 | 20.8 | <0.001 | |
| Severe | 0 | 0.0 | 6 | 11.3 | <0.001 | |
| 4. Incomplete bladder emptying positive | 4 | 10.3 | 38 | 71.7 | <0.001 | |
| None | 35 | 89.7 | 15 | 28.3 | <0.001 | |
| Mild | 4 | 10.3 | 13 | 24.5 | 0.068 | |
| Moderate | 0 | 0.0 | 5 | 9.4 | 0.024 | |
| Severe | 0 | 0.0 | 20 | 37.7 | <0.001 | |
| 5. Suprapubic pain positive | 5 | 12.8 | 26 | 49.1 | <0.001 | |
| None | 34 | 87.2 | 27 | 50.9 | <0.001 | |
| Mild | 3 | 7.7 | 7 | 13.2 | 0.407 | |
| Moderate | 2 | 5.1 | 16 | 30.2 | <0.001 | |
| Severe | 0 | 0.0 | 3 | 5.7 | 0.083 | |
| 6. Visible blood in urine positive | 0 | 0.0 | 37 | 69.8 | <0.001 | |
| None | 39 | 100.0 | 16 | 30.2 | <0.001 | |
| Mild | 0 | 0.0 | 15 | 28.3 | <0.001 | |
| Moderate | 0 | 0.0 | 13 | 24.5 | <0.001 | |
| Severe | 0 | 0.0 | 9 | 17.0 | <0.001 | |
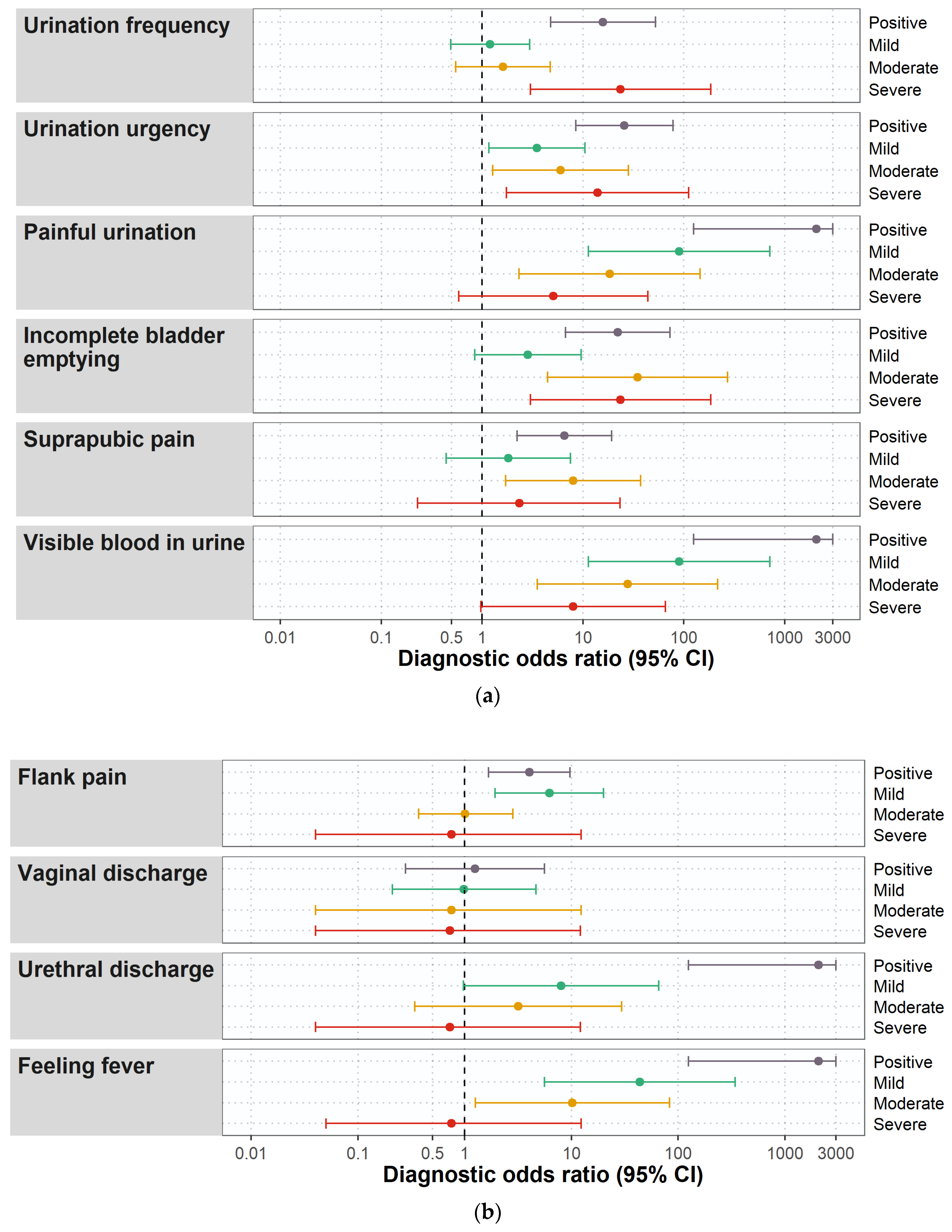
| Differential Symptoms | 7. Flank pain positive | 12 | 30.8 | 34 | 64.2 | 0.001 |
| None | 27 | 69.2 | 19 | 35.8 | 0.001 | |
| Mild | 4 | 10.3 | 22 | 41.5 | <0.001 | |
| Moderate | 8 | 20.5 | 11 | 20.8 | 0.978 | |
| Severe | 0 | 0.0 | 1 | 1.9 | 0.322 | |
| 8. Vaginal discharge positive | 3 | 7.7 | 5 | 9.4 | 0.773 | |
| None | 36 | 92.3 | 48 | 90.6 | 0.773 | |
| Mild | 3 | 7.7 | 4 | 7.6 | 0.980 | |
| Moderate | 0 | 0.0 | 1 | 1.9 | 0.322 | |
| Severe | 0 | 0.0 | 0 | 0.0 | n.a. | |
| 9. Urethral discharge positive | 0 | 0.0 | 9 | 17.0 | 0.002 | |
| None | 39 | 100.0 | 44 | 83.0 | 0.002 | |
| Mild | 0 | 0.0 | 5 | 9.4 | 0.024 | |
| Moderate | 0 | 0.0 | 4 | 7.6 | 0.044 | |
| Severe | 0 | 0.0 | 0 | 0.0 | n.a. | |
| 10. Feeling fever positive | 0 | 0.0 | 28 | 52.8 | <0.001 | |
| None | 39 | 100.0 | 25 | 47.2 | <0.001 | |
| Mild | 0 | 0.0 | 17 | 32.1 | <0.001 | |
| Moderate | 0 | 0.0 | 10 | 18.9 | 0.001 | |
| Severe | 0 | 0.0 | 1 | 1.9 | 0.322 | |
| Quality of Life | 11. General discomfort positive | 2 | 5.1 | 49 | 92.5 | <0.001 |
| None | 37 | 94.8 | 4 | 7.6 | <0.001 | |
| Mild | 1 | 2.6 | 9 | 17.0 | 0.015 | |
| Moderate | 1 | 2.6 | 17 | 32.1 | <0.001 | |
| Severe | 0 | 0 | 23 | 43.1 | <0.001 | |
| 12. Impact on everyday activity positive | 1 | 2.6 | 31 | 58.5 | <0.001 | |
| None | 38 | 97.4 | 22 | 41.5 | <0.001 | |
| Mild | 1 | 2.6 | 5 | 9.4 | 0.024 | |
| Moderate | 0 | 0.0 | 12 | 22.6 | 0.002 | |
| Severe | 0 | 0.0 | 14 | 26.4 | <0.001 | |
| 13. Impact on social life positive | 3 | 7.7 | 38 | 71.7 | <0.001 | |
| None | 36 | 92.3 | 15 | 28.3 | <0.001 | |
| Mild | 2 | 5.1 | 12 | 22.6 | 0.012 | |
| Moderate | 3 | 2.6 | 14 | 26.4 | <0.001 | |
| Severe | 0 | 0.0 | 12 | 22.6 | <0.001 | |
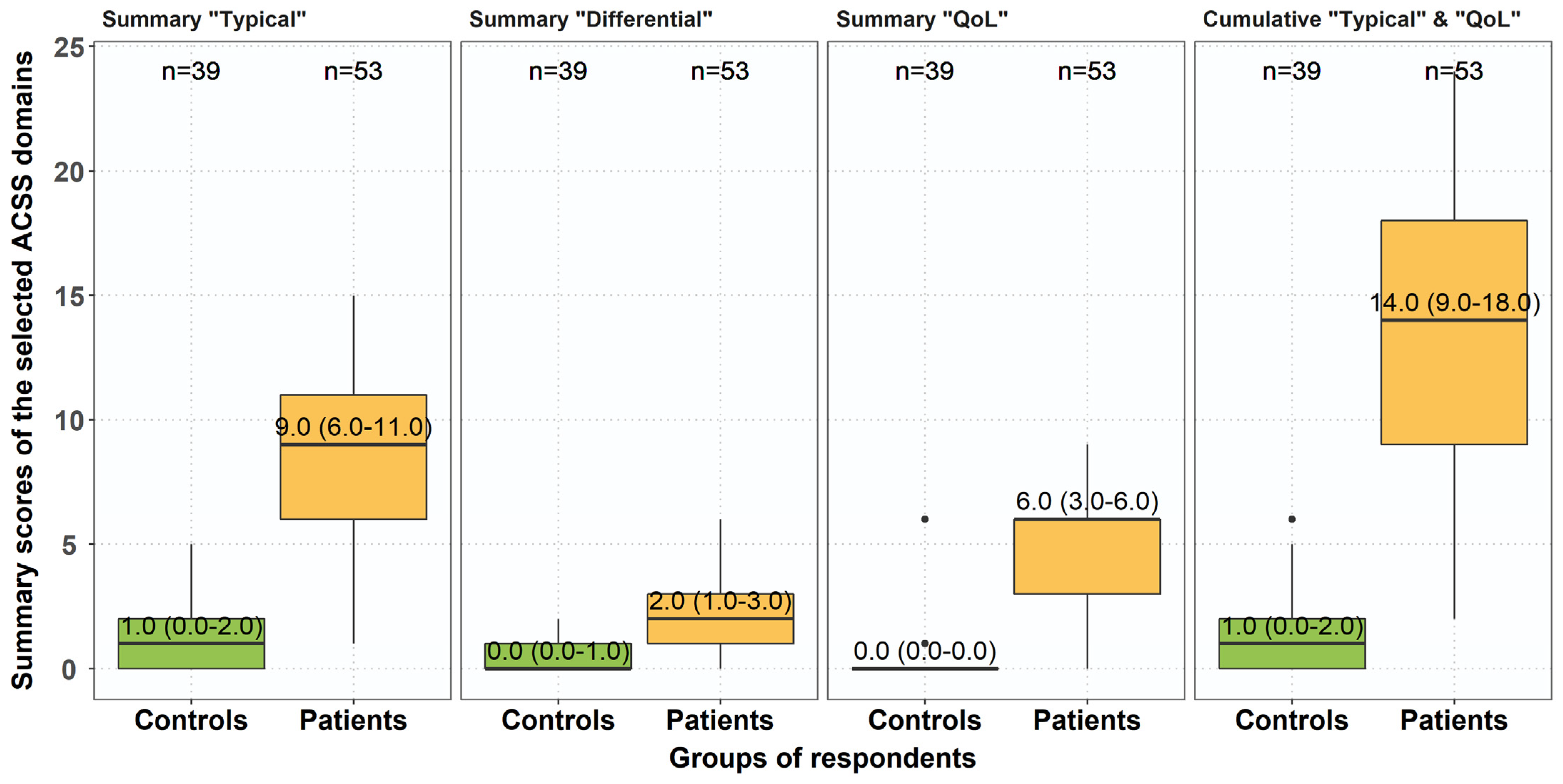
| Summary Scores of the Different ACSS Domains | Total Cohort | Controls | Patients | p-Value * |
|---|---|---|---|---|
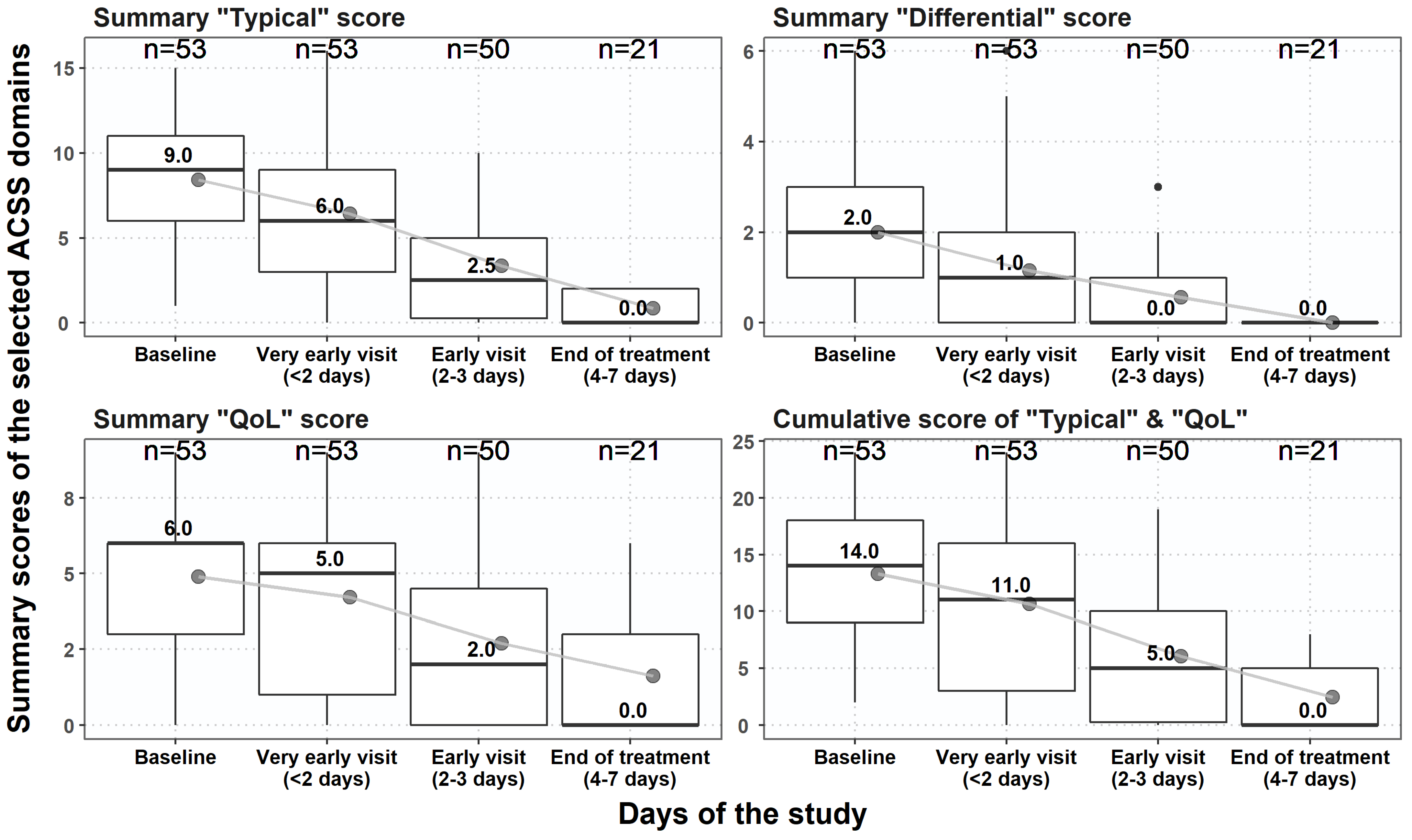
| Summary ‘Typical’ score, median (IQR) | 5.0 (1.0–9.3) | 1.0 (0.0–2.0) | 9.0 (6.0–11.0) | <0.001 |
| Summary ‘Differential’ score, median (IQR) | 1.0 (0.0–2.0) | 0.0 (0.0–1.0) | 2.0 (1.0–3.0) | <0.001 |
| Summary ‘QoL’ score, median (IQR) | 1.0 (0.0–6.0) | 0.0 (0.0–0.0) | 6.0 (3.0–6.0) | <0.001 |
| Cumulative ‘Typical’ and ‘QoL’ score, median (IQR) | 6.0 (1.0–15.0) | 1.0 (0.0–2.0) | 14.0 (9.0–18.0) | <0.001 |
| Cumulative score of the entire ACSS, median (IQR) | 7.5 (2.0–17.0) | 2.0 (0.0–3.0) | 15.0 (12.0–20.0) | <0.001 |
| The ACSS Domain | Patients and Controls | Patients at Baseline and Follow-up Assessments | p-Value * | ||
|---|---|---|---|---|---|
| Cronbach’s Alpha [95%CI] | Split-Half [95%CI] | Cronbach’s Alpha [95%CI] | Split-Half [95%CI] | ||
| Typical | 0.81 [0.75; 0.87] | 0.83 [0.64; 0.90] | 0.81 [0.77; 0.85] | 0.83 [0.63; 0.92] | 0.980 |
| Differential | 0.40 [0.22; 0.58] | 0.33 [0.25; 0.62] | 0.57 [0.48; 0.66] | 0.51 [0.49; 0.69] | 0.061 |
| QoL | 0.91 [0.88; 0.94] | 0.81 [0.80; 0.81] | 0.89 [0.86; 0.92] | 0.77 [0.75; 0.78] | 0.701 |
| Cumulative ‘Typical’ and ‘QoL’ | 0.89 [0.86; 0.93] | 0.89 [0.78; 0.94] | 0.89 [0.86; 0.91] | 0.89 [0.76; 0.95] | 0.798 |
| Entire ACSS | 0.89 [0.86; 0.92] | 0.89 [0.77; 0.94] | 0.88 [0.86; 0.91] | 0.89 [0.76; 0.94] | 0.870 |
| Summary ‘Typical’ Score | 5 and Higher | 6 and Higher | 7 and Higher | 6 and Higher * |
|---|---|---|---|---|
| Sensitivity | 0.74 (0.61; 0.84) | 0.77 (0.64; 0.87) | 0.70 (0.56; 0.82) | 0.77 (0.64; 0.88) |
| Specificity | 0.95 (0.83; 0.99 | 0.98 (0.87; 1.00) | 0.98 (0.87; 1.00) | 0.95 (0.77; 1.00) |
| Positive predictive value | 0.96 (0.85; 0.99) | 0.98 (0.87; 1.00) | 0.97 (0.86; 1.00) | 0.98 (0.87; 1.00) |
| Negative predictive value | 0.70 (0.56; 0.82) | 0.76 (0.63; 0.87) | 0.71 (0.57; 0.82) | 0.64 (0.45; 0.80) |
| Diagnostic odds ratio | 52.0 (11.2; 241.0) | 133.3 (16.5; 1073.6) | 90.2 (11.4; 714.5) | 71.8 (8.7; 589.9) |
| Youden’s index | 0.69 (0.44; 0.84) | 0.75 (0.51; 0.88) | 0.67 (0.42; 0.82) | 0.73 (0.41; 0.88) |
| Correlation with PO | 0.67 (0.55; 0.77) | 0.67 (0.54; 0.76) | 0.61 (0.47; 0.72) | 0.70 (0.56; 0.80) |
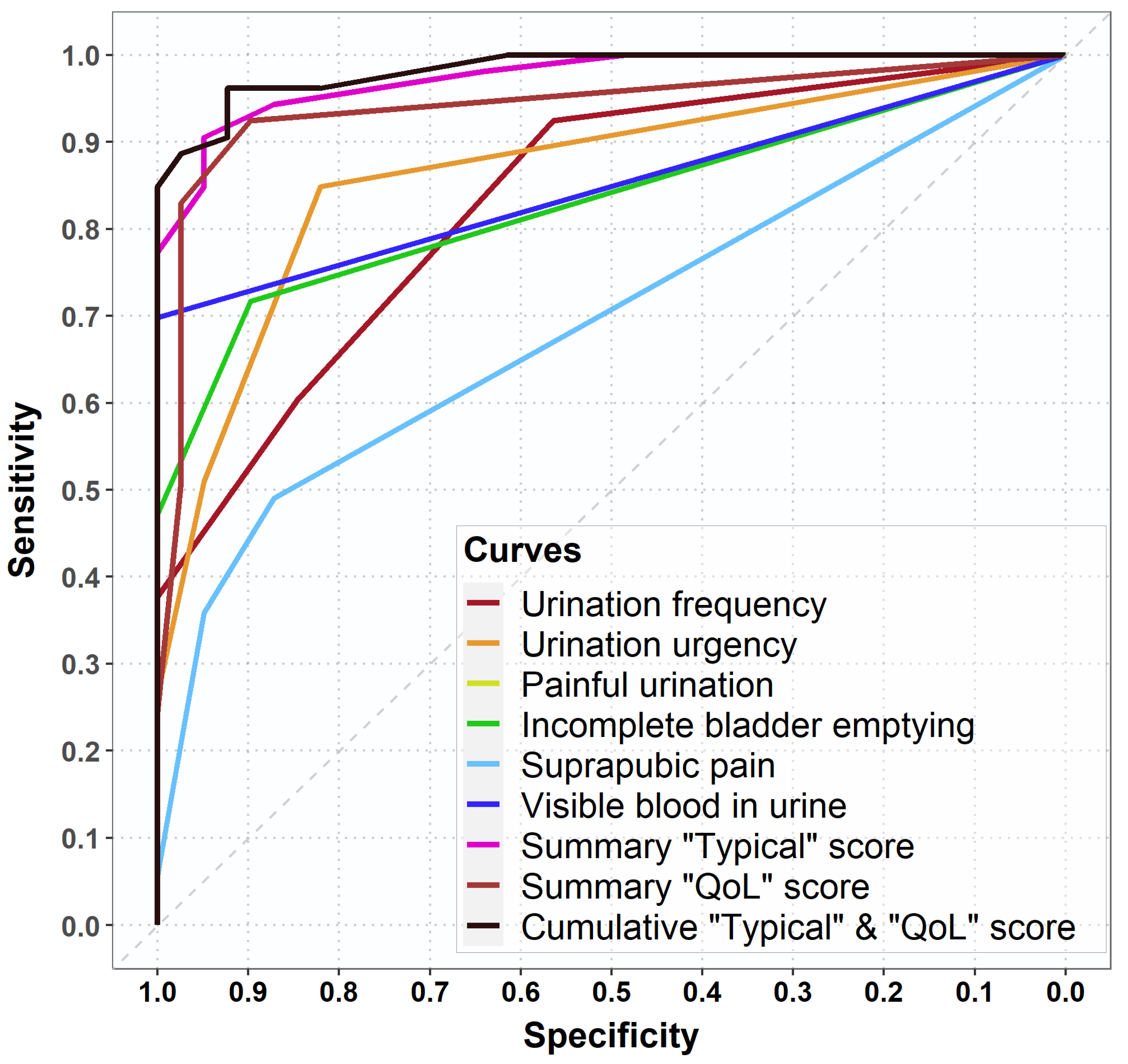
| Area under the ROC-curve | 0.83 (0.76; 0.90) | 0.83 (0.77; 0.89) | 0.81 (0.75; 0.87) | 0.82 (0.73; 0.90) |
| Type | Thresholds for Clinical Success | Success | Non-Success |
|---|---|---|---|
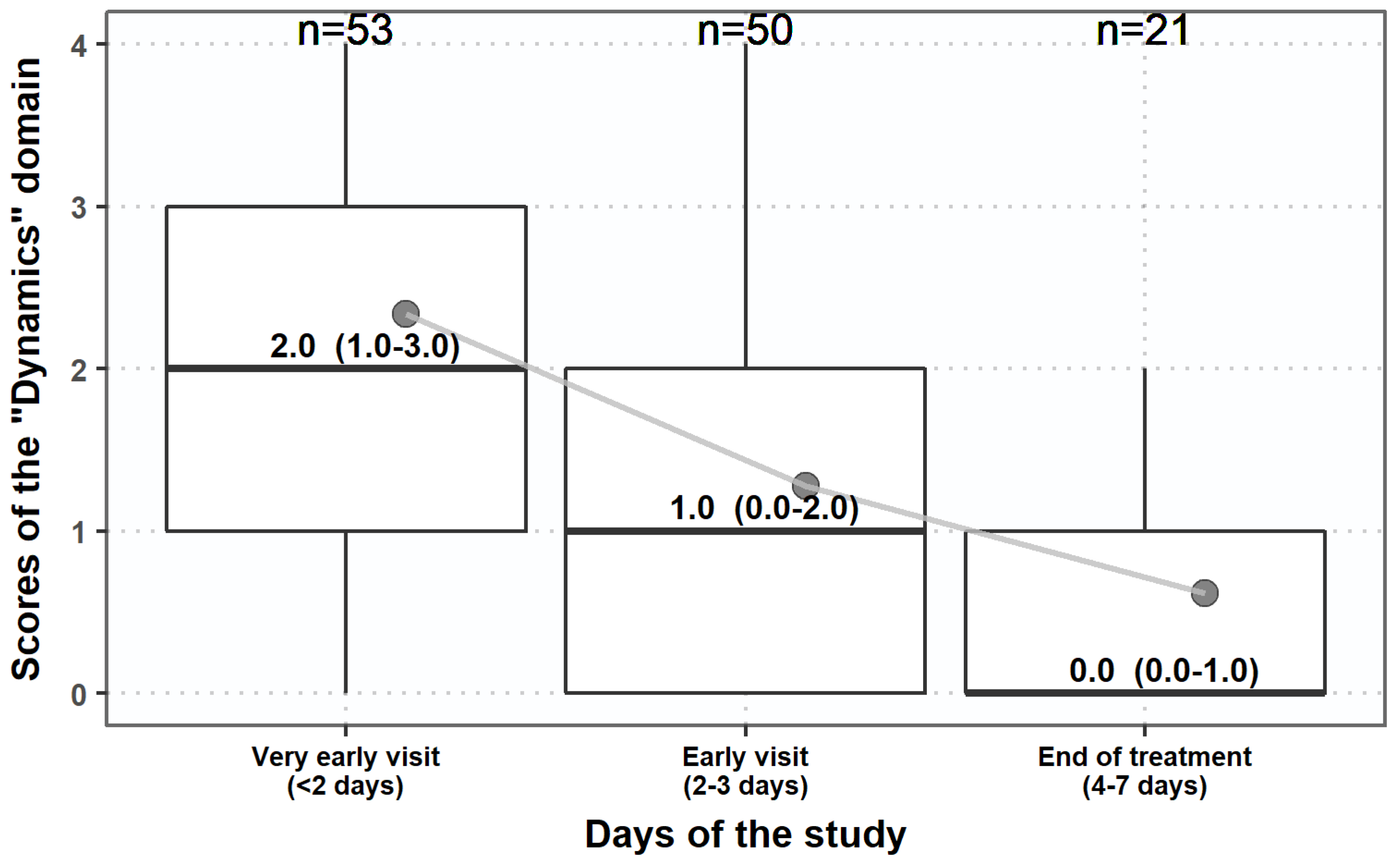
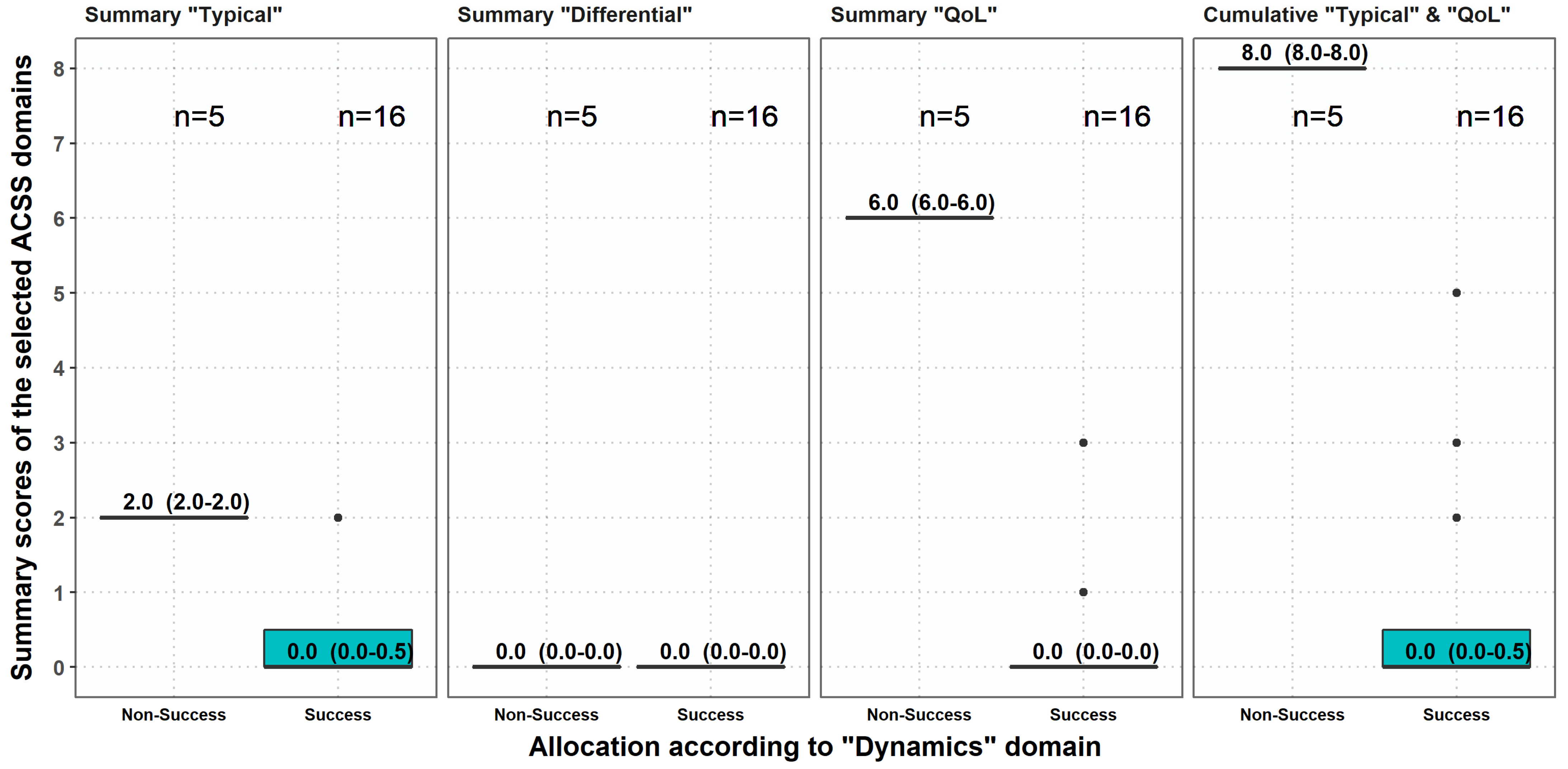
| A | Dynamics, no item >1 | 16 | 5 |
| B | Sum score of typical domain ≤ 5 scores, no item > 1 | 21 | 0 |
| C | Sum score of typical domain < 5 scores, no item > 1 and no item of QoL > 1 | 16 | 5 |
| D | Sum score of the 4 FDA symptoms ≤ 4, no item > 1 | 21 | 0 |
| E | Sum score of the 3 EMA symptoms ≤ 3, no item> 1 | 21 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stamatiou, K.; Samara, E.; Alidjanov, J.F.; Pilatz, A.M.E.; Naber, K.G.; Wagenlehner, F.M.E. Clinical Validation of the Greek Version of the Acute Cystitis Symptom Score (ACSS)—Part II. Antibiotics 2021, 10, 1253. https://doi.org/10.3390/antibiotics10101253
Stamatiou K, Samara E, Alidjanov JF, Pilatz AME, Naber KG, Wagenlehner FME. Clinical Validation of the Greek Version of the Acute Cystitis Symptom Score (ACSS)—Part II. Antibiotics. 2021; 10(10):1253. https://doi.org/10.3390/antibiotics10101253
Chicago/Turabian StyleStamatiou, Konstantinos, Evangelia Samara, Jakhongir F. Alidjanov, Adrian M. E. Pilatz, Kurt G. Naber, and Florian M. E. Wagenlehner. 2021. "Clinical Validation of the Greek Version of the Acute Cystitis Symptom Score (ACSS)—Part II" Antibiotics 10, no. 10: 1253. https://doi.org/10.3390/antibiotics10101253