
How Accurate Are Veterinary Clinicians Employing Flexicult Vet for Identification and Antimicrobial Susceptibility Testing of Urinary Bacteria?

 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
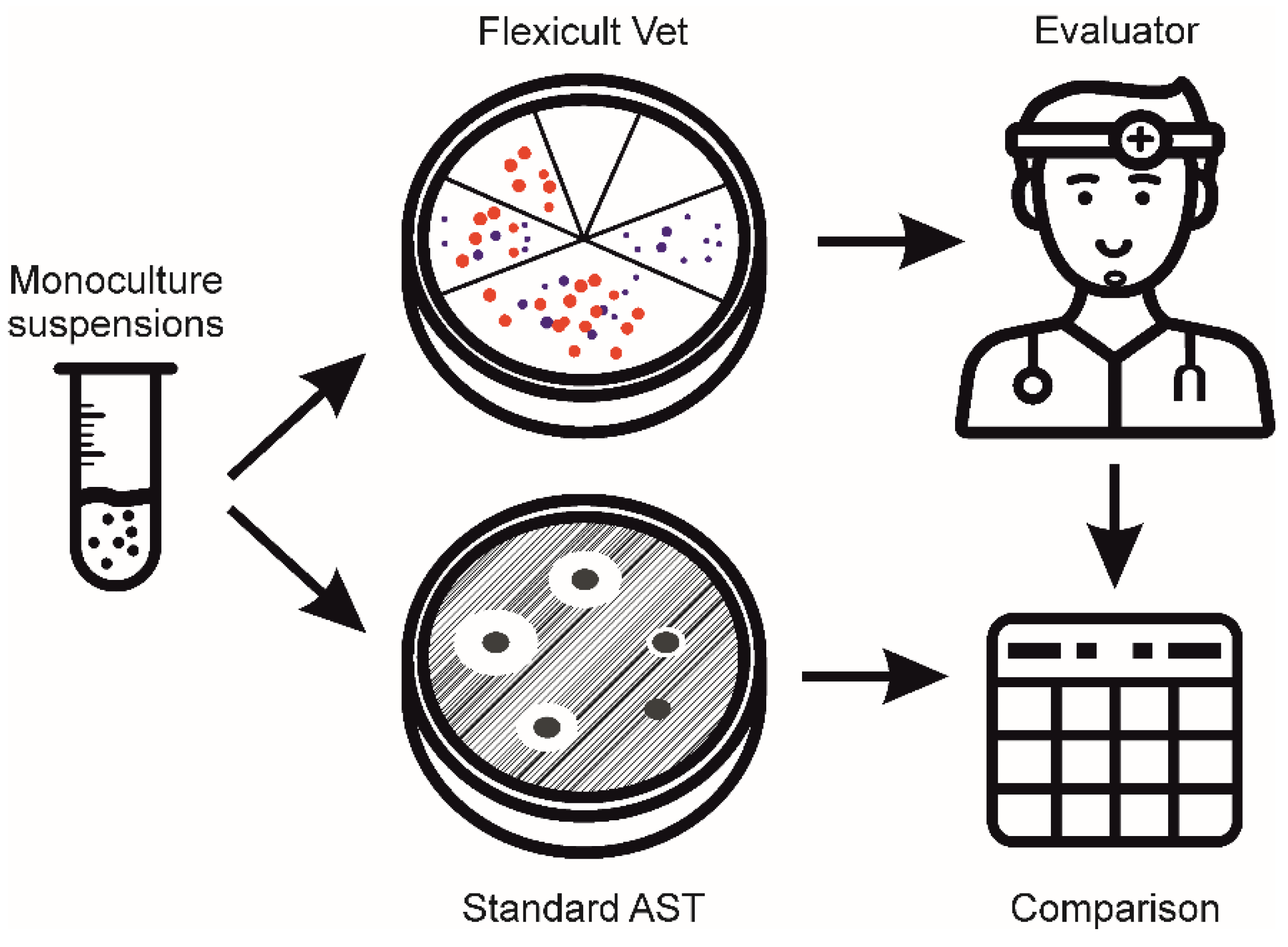
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsch, R.; Teichmann-Knorrn, S.; Sjetne Lund, H. Urinary Tract Infection and Subclinical Bacteriuria in Cats: A Clinical Update. J. Feline Med. Surg. 2019, 21, 1023–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smee, N.; Loyd, K.; Grauer, G. UTIs in Small Animal Patients: Part 1: Etiology and Pathogenesis. J. Am. Anim. Hosp. Assoc. 2013, 49, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Weese, J.S.; Blondeau, J.; Boothe, D.; Guardabassi, L.G.; Gumley, N.; Papich, M.; Jessen, L.R.; Lappin, M.; Rankin, S.; Westropp, J.L.; et al. International Society for Companion Animal Infectious Diseases (ISCAID) Guidelines for the Diagnosis and Management of Bacterial Urinary Tract Infections in Dogs and Cats. Vet. J. 2019, 247, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Guardabassi, L.; Hedberg, S.; Jessen, L.R.; Damborg, P. Optimization and Evaluation of Flexicult® Vet for Detection, Identification and Antimicrobial Susceptibility Testing of Bacterial Uropathogens in Small Animal Veterinary Practice. Acta Vet. Scand. 2015, 57, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, G.V.; Norris, C.R.; Franti, C.E.; Eisele, P.H.; Johnson, D.L.; Ruby, A.L.; Jang, S.S. Interrelations of Organism Prevalence, Specimen Collection Method, and Host Age, Sex, and Breed among 8,354 Canine Urinary Tract Infections (1969–1995). J. Vet. Intern. Med. 2001, 15, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.R.; Rubin, J.E.; Chirino-Trejo, M.; Dowling, P.M. Antimicrobial Resistance and Prevalence of Canine Uropathogens at the Western College of Veterinary Medicine Veterinary Teaching Hospital, 2002–2007. Can. Vet. J. Rev. Vet. Can. 2008, 49, 985–990. [Google Scholar]
- Windahl, U.; Holst, B.S.; Nyman, A.; Grönlund, U.; Bengtsson, B. Characterisation of Bacterial Growth and Antimicrobial Susceptibility Patterns in Canine Urinary Tract Infections. BMC Vet. Res. 2014, 10, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, M.; White, J.; Lam, A. Prevalence of Bacteria and Changes in Trends in Antimicrobial Resistance of Escherichia Coli Isolated from Positive Canine Urinary Samples from an Australian Referral Hospital over a 5-Year Period (2013–2017). Vet. Rec. Open 2019, 6, e000345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Briyne, N.; Atkinson, J.; Borriello, S.P.; Pokludová, L. Antibiotics Used Most Commonly to Treat Animals in Europe. Vet. Rec. 2014, 175, 325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jessen, L.R.; Sørensen, T.M.; Bjornvad, C.R.; Nielsen, S.S.; Guardabassi, L. Effect of Antibiotic Treatment in Canine and Feline Urinary Tract Infections: A Systematic Review. Vet. J. 2015, 203, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Epstein, S.E.; Westropp, J.L. Antimicrobial Susceptibility Patterns in Urinary Tract Infections in Dogs (2010–2013). J. Vet. Intern. Med. 2015, 29, 1045–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.R.; Owens, K.; Gajewski, A.; Clabots, C. Escherichia Coli Colonization Patterns among Human Household Members and Pets, with Attention to Acute Urinary Tract Infection. J. Infect. Dis. 2008, 197, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6, ARBA-0009-2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VET01. Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals, 4th ed.; CLSI Clinical and Laboratory Standards Institute: Annapolis Junction, MD, USA, 2013. [Google Scholar]
- Sørensen, T.M.; Bjørnvad, C.R.; Cordoba, G.; Damborg, P.; Guardabassi, L.; Siersma, V.; Bjerrum, L.; Jessen, L.R. Effects of Diagnostic Work-Up on Medical Decision-Making for Canine Urinary Tract Infection: An Observational Study in Danish Small Animal Practices. J. Vet. Intern. Med. 2018, 32, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Francis, N.A.; Thomas-Jones, E.; Longo, M.; Wootton, M.; Llor, C.; Little, P.; Moore, M.; Bates, J.; Pickles, T.; et al. Point-of-Care Urine Culture for Managing Urinary Tract Infection in Primary Care: A Randomised Controlled Trial of Clinical and Cost-Effectiveness. Br. J. Gen. Pract. 2018, 68, e268. [Google Scholar] [CrossRef] [PubMed]
- Uhl, A.; Hartmann, F.A.; Viviano, K.R. Clinical Performance of a Commercial Point-of-Care Urine Culture System for Identification of Bacteriuria in Dogs. J. Am. Vet. Med. Assoc. 2017, 251, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Olin, S.J.; Bartges, J.W.; Jones, R.D.; Bemis, D.A. Diagnostic Accuracy of a Point-of-Care Urine Bacteriologic Culture Test in Dogs. J. Am. Vet. Med. Assoc. 2013, 243, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Papić, B.; Golob, M.; Zdovc, I.; Kušar, D.; Avberšek, J. Genomic Insights into the Emergence and Spread of Methicillin-Resistant Staphylococcus Pseudintermedius in Veterinary Clinics. Vet. Microbiol. 2021, 258, 109119. [Google Scholar] [CrossRef]
- Brložnik, M.; Šterk, K.; Zdovc, I. Prevalence and Resistance Patterns of Canine Uropathogens in Regard to Concurrent Diseases. Berl. Munch. Tierarztl. Wochenschr. 2016, 129, 340–350. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flexicult Vet | |||||||
|---|---|---|---|---|---|---|---|
| True Species | Investigator | E. coli | S. pseudint. | E. faecium | E. faecalis | Proteus spp. | Other |
| E. coli, n = 13 | E | 98.1 [95.2–100.0] | 1.9 | ||||
| C | 84.6 [72.7–96.6] | 12.8 | 1.3 | 1.3 (Es, Ks) | |||
| All | 90.0 [82.3–98.7] | 8.5 | 0.8 | 0.8 (Ea, Ks) | |||
| S. pseudintermedius, n = 11 | E | 8.3 | 82.6 [68.3–96.9] | 3.4 | 5.7 (Sc, Sa) | ||
| C | 7.6 | 40.3 [22.8–57.7] | 21.6 | 30.6 (Sc, Pa) | |||
| All | 7.9 | 57.2 [44.1–70.3] | 14.3 | 20.6 (Sc, Sa, Pa) | |||
| E. faecium, n = 6 | E | 50.0 | 31.3 [15.2–47.3] | 18.8 (Sc) | |||
| C | 1.6 | 25.0 | 27.6 [18.8–36.3] | 5.1 | 40.8 (Sc, Pa, Ks) | ||
| All | 1.0 | 35.0 | 29.0 [21.7–36.3] | 3.1 | 32.0 (Sc, Pa, Ks) | ||
| E. faecalis, n = 9 | E | 1.4 | 98.6 [95.4–100] | ||||
| C | 0.9 | 97.2 [94.0–100] | 1.9 (Pa) | ||||
| All | 1.1 | 97.8 [95.0–100] | 1.1 (Pa) | ||||
| Proteus spp., n = 4 | E | 93.8 [73.9–100] | 6.3 (Pa) | ||||
| C | 8.3 | 87.5 [62.1–100] | 4.2 (Pa) | ||||
| All | 5.0 | 90.0 [71.6–100] | 5.0 (Pa) | ||||
| Other, n = 4 | E | 8.3 | 3.1 | 88.5 [63.5–100] | |||
| C | 2.1 | 4.9 | 3.5 | 9.7 | 79.9 [52.0–100] | ||
| All | 4.6 | 2.9 | 2.1 | 7.1 | 83.3 [57.6–100] | ||
| All, n = 47 | Experts: 84.6 [77.2–91.9] | Clinicians: 68.7 [59.6–77.8] | All: 75.1 [67.4–82.8] | ||||
| Bacteria | Evaluator | AST | Flexicult Vet | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMP | AMC | OXA | ENR | SXT | ||||||||
| R | S | R | S | R | S | R | S | R | S | |||
| E. coli, n = 13 | E | R | 9 | 1 | 9 | 1 | 6 | 1 | 4 | 1 | ||
| S | – | 3 | – | 3 | – | 6 | – | 8 | ||||
| C | R | 8.83 | 1.17 | 9 | 1 | 6 | 1 | 4 | 1 | |||
| S | 0.17 | 2.83 | – | 3 | – | 6 | 0.17 | 7.83 | ||||
| All | 90.8 [74.1–100] | 92.3 [75.5–100] | 92.3 [75.5–100] | 91.5 [74.8–100] | ||||||||
| S. pseudintermedius, n = 10 | E | R | 6.75 | 2.25 | 2.50 | 6.50 | 3.13 | 5.88 | 8.75 | 0.25 | 9 | – |
| S | – | – | – | 1 | – | 1 | – | 1 | – | 1 | ||
| C | R | 7 | 2 | 2.17 | 6.83 | 3 | 6 | 8.83 | 0.17 | 8.83 | 0.17 | |
| S | – | – | – | 1 | – | 1 | 0.17 | 0.83 | – | 1 | ||
| All | 76.7 * [53.0–100] | 33.0 [2.3–63.7] | 40.5 [11.7–69.3] | 97.0 [92.2–100] | 99.0 [96.7–100] | |||||||
| E. faecium, n = 6 | E | R | 2 | – | 2 | – | 2 | – | 1.50 | 4.50 | ||
| S | – | 4 | – | 4 | – | 4 | – | – | ||||
| C | R | 1.63 | 0.37 | 1.63 | 0.37 | 1.80 | 0.20 | 2 | 4 | |||
| S | 1.27 | 2.73 | – | 4 | 0.93 | 3.07 | – | – | ||||
| All | 83.7 [77.7–89.7] | 96.3 [90.3–100] | 88.7 [80.6–96.7] | 30.0 [7.9–52.1] | ||||||||
| E. faecalis, n = 9 | E | R | – | – | – | – | 5 | – | 8.50 | 0.50 | ||
| S | – | 8 | – | 8 | 1 | 2 | – | – | ||||
| C | R | – | – | – | – | 4.83 | 0.17 | 8.17 | 0.83 | |||
| S | 0.17 | 7.83 | – | 8 | 1 | 2 | – | – | ||||
| All | 98.7 * [95.8–100] | 100 * [100–100] | 86.2 * [57.0–100] | 92.2 [84.4–99.7] | ||||||||
| Proteus spp., n = 4 | E | R | 2.25 | 1.75 | – | 2 | – | 2 | – | 2 | ||
| S | – | – | 0.75 | 1.25 | – | 2 | 0.75 | 1.25 | ||||
| C | R | 1.17 | 2.83 | – | 2 | – | 2 | – | 2 | |||
| S | – | – | – | 2 | – | 2 | 0.33 | 1.67 | ||||
| All | 40.0 [0–100] | 42.5 [0–100] | 50.0 [0–100] | 37.5 [0–100] | ||||||||
| Other, n = 4 | E | R | 2.13 | 0.88 | 1 | 1 | 1 | – | – | – | ||
| S | – | – | – | 1 | – | 3 | 0.13 | 2.88 | ||||
| C | R | 2.08 | 0.92 | 1.22 | 0.78 | 1 | – | – | – | |||
| S | – | – | 0.33 | 0.67 | – | 3 | 0.42 | 2.58 | ||||
| All | 70.0 * [5.4–1] | 64.4 * [0–100] | 100 [100–100] | 90.0 * [77.6–100] | ||||||||
| All samples n = 43 (AMP), 44 (AMC), 10 (OXA), 45 (ENR), 45 (SXT) | All E C | 82.1 [73.3–90.9] 86.3 [76.6–96.1] 79.3 [70.5–88.1] | 74.4 [62.1–86.6] 74.4 [62.0–86.9] 74.3 [61.9–86.7] | 40.6 [11.8–69.4] 41.3 [9.7–72.9] 40.2 [12.0–68.4] | 88.7 [80.1–97.3] 90.6 [81.9–99.2] 87.4 [78.8–96.1] | 80.2 [70.4–90.0] 80.3 [70.0–90.6] 80.2 [70.4–89.9] | ||||||
| All together (n = 187) | All: 79.2 [74.2–84.2] | E: 80.7 [75.5–85.9] | C: 78.2 [73.2–83.2] | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cugmas, B.; Avberšek, M.; Rosa, T.; Godec, L.; Štruc, E.; Golob, M.; Zdovc, I. How Accurate Are Veterinary Clinicians Employing Flexicult Vet for Identification and Antimicrobial Susceptibility Testing of Urinary Bacteria? Antibiotics 2021, 10, 1160. https://doi.org/10.3390/antibiotics10101160
Cugmas B, Avberšek M, Rosa T, Godec L, Štruc E, Golob M, Zdovc I. How Accurate Are Veterinary Clinicians Employing Flexicult Vet for Identification and Antimicrobial Susceptibility Testing of Urinary Bacteria? Antibiotics. 2021; 10(10):1160. https://doi.org/10.3390/antibiotics10101160
Chicago/Turabian StyleCugmas, Blaž, Miha Avberšek, Teja Rosa, Leonida Godec, Eva Štruc, Majda Golob, and Irena Zdovc. 2021. "How Accurate Are Veterinary Clinicians Employing Flexicult Vet for Identification and Antimicrobial Susceptibility Testing of Urinary Bacteria?" Antibiotics 10, no. 10: 1160. https://doi.org/10.3390/antibiotics10101160