EMG-Based Characterization of Walking Asymmetry in Children with Mild Hemiplegic Cerebral Palsy

 ,
,  ,
,  ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Signal Acquisition
2.3. Signal Processing
2.4. Statistical Gait Analysis
2.5. Statistics
3. Results
3.1. Foot-Floor Contact
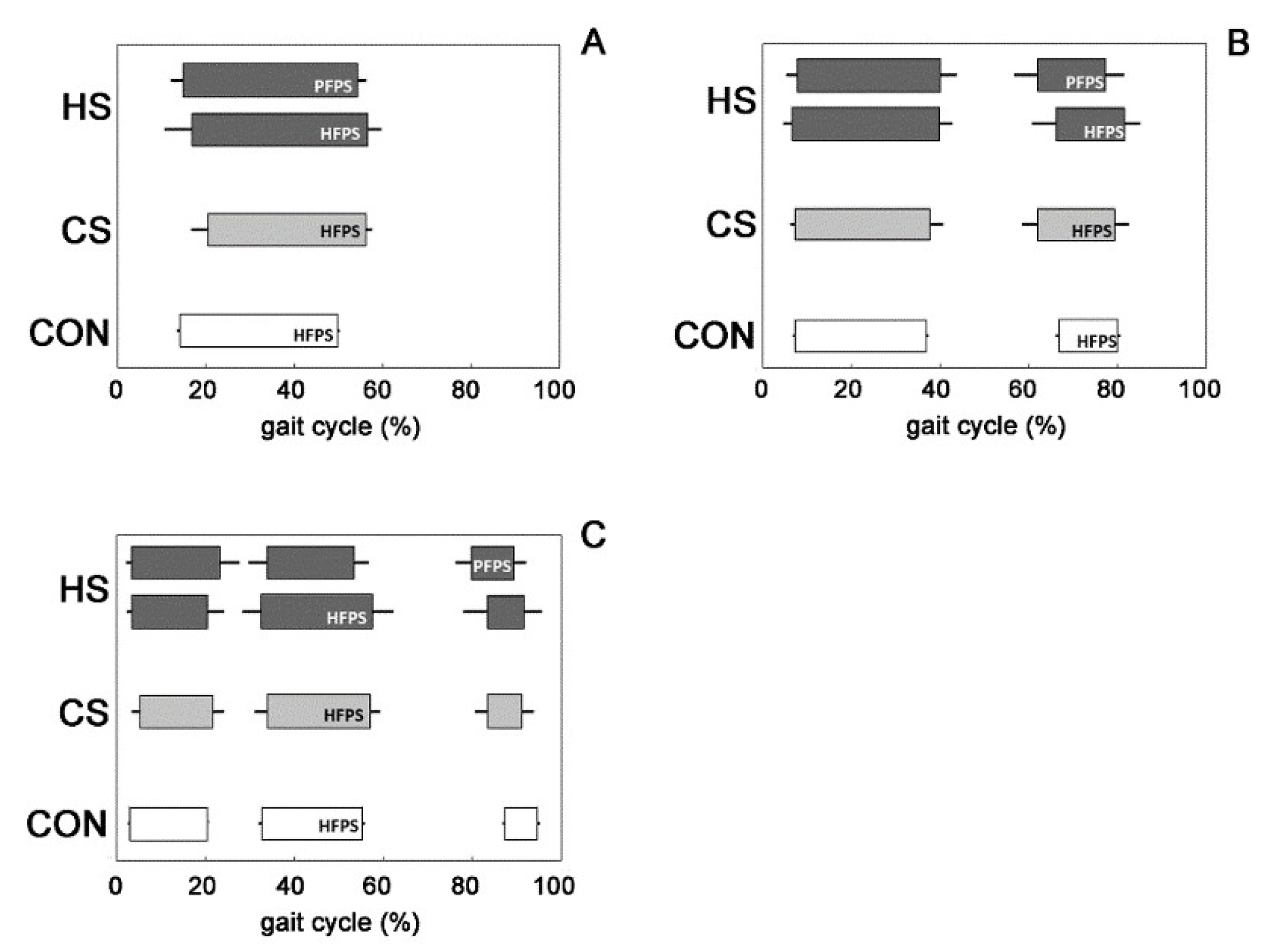
3.2. Muscle Activation Patterns
4. Discussion
4.1. Foot-Floor Contact
4.2. Muscle Activation Patterns
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ostensjø, S.; Carlberg, E.B.; Vøllestad, N.K. Motor impairments in young children with cerebral palsy: Relationship to gross motor function and everyday activities. Dev. Med. Child. Neurol. 2004, 46, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Dobson, F.; Morris, M.E.; Baker, R.; Graham, H.K. Gait classification in children with cerebral palsy: A systematic review. Gait Posture 2007, 25, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Winters, T.F.; Gage, J.R.; Hicks, R. Gait patterns in spastic hemiplegiain children and young adults. J. Bone Jt. Surg. 1987, 69, 437–441. [Google Scholar]
- McDowell, B.C.; Kerr, C.; Kelly, C.; Salazar, J.; Cosgrove, A. The validity of an existing gait classification system when applied to a representative population of children with hemiplegia. Gait Posture 2008, 28, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Knaflitz, M. Multiple gait patterns within the same Winters class in children with hemiplegic cerebral palsy. Clin. Biomech. 2015, 30, 908–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riad, J.; Haglund-Akerlind, Y.; Miller, F. Power generation in children with spastic hemiplegic cerebral palsy. Gait Posture 2008, 27, 641–647. [Google Scholar] [CrossRef]
- Bojanic, D.M.; Petrovacki-Balj, B.D.; Jorgovanovic, N.D.; Ilic, V.R. Quantification of dynamic EMG patterns during gait in children with cerebral palsy. J. Neurosci. Methods 2011, 198, 325–331. [Google Scholar] [CrossRef]
- Galli, M.; Cimolin, V.; Rigoldi, C.; Tenore, N.; Albertini, G. Gait patterns in hemiplegic children with cerebral palsy: Comparison of right and left hemiplegia. Res. Dev. Disabil. 2010, 31, 1340–1345. [Google Scholar] [CrossRef]
- Patikas, D.; Wolf, S.; Döderlein, L. Electromyographic evaluation of the sound and involved side during gait of spastic hemiplegic children with cerebral palsy. Eur. J. Neurol. 2005, 12, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Patikas, D.S.; Wolf, I.; Schuster, W.; Armbrust, P.; Dreher, T.; Döderlein, L. Electromyographic patterns in children with cerebral palsy: Do they change after surgery? Gait Posture 2007, 26, 362–371. [Google Scholar] [CrossRef]
- Cappellini, G.; Sylos-Labini, F.; MacLellan, M.J.; Sacco, A.; Morelli, D.; Lacquaniti, F.; Ivanenko, Y. Backward walking highlights gait asymmetries in children with cerebral palsy. J. Neurophysiol. 2018, 119, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, F.; Mengarelli, A.; Strazza, A.; Malavolta, M.; Verdini, F.; Cardarelli, S.; Burattini, L.; Nascimbeni, A.; Fioretti, S. Gait asymmetry in winters group I hemiplegic children: Role of tibialis anterior. In IFMBE Proceedings; Springer: Berlin, Germany, 2018; Volume 68, pp. 681–684. [Google Scholar]
- Romkes, J.; Brunner, R. An electromyographic analysis of obligatory (hemiplegic cerebral palsy) and voluntary (normal) unilateral toe-walking. Gait Posture 2007, 26, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; Benedetti, M.G.; Knaflitz, M. Normative EMG activation patterns of school-age children during gait. Gait Posture 2010, 32, 285–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, D.A. Biomechanics and Motor Control of Human Movement, 2nd ed.; Wiley: New York, NY, USA, 1990. [Google Scholar]
- Bonato, P.; D′Alessio, T.; Knaflitz, M. A statistical method for the measurement of muscle activation intervals from surface myoelectric signal during gait. IEEE Trans. Biomed. Eng. 1998, 45, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Knaflitz, M. An algorithm for the estimation of the signal-to-noise ratio in surface myoelectric signals generated during cyclic movements. IEEE Trans. Biomed. Eng. 2012, 59, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Balestra, G.; Knaflitz, M. Segmentation and classification of gait cycles. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Mengarelli, A.; Maranesi, E.; Burattini, L.; Fioretti, S.; Di Nardo, F. Co-contraction activity of ankle muscles during walking: A gender comparison. Biomed. Signal. Process. Control. 2017, 33, 1–9. [Google Scholar] [CrossRef]
- Di Nardo, F.; Mengarelli, A.; Ghetti, G.; Fioretti, S. Statistical analysis of EMG signal acquired from tibialis anterior during gait. In IFMBE Proceedings; Springer: Berlin, Germany, 2014; Volume 41, pp. 619–622. [Google Scholar]
- Di Nardo, F.; Mengarelli, A.; Strazza, A.; Agostini, V.; Knaflitz, M.; Burattini, L.; Fioretti, S. A new parameter for quantifying the variability of surface electromyographic signals during gait: The occurrence frequency. J. Electromyogr. Kinesiol. 2017, 36, 25–33. [Google Scholar] [CrossRef]
- Pu, F.; Fan, X.; Yang, Y.; Chen, W.; Li, S.; Li, D.; Fan, Y. Feedback system based on plantar pressure for monitoring toe-walking strides in children with cerebral palsy. Am. J. Phys. Med. Rehabil. 2014, 93, 122–129. [Google Scholar] [CrossRef]
- Desailly, E.; Daniel, Y.; Sardain, P.; Lacouture, P. Foot contact event detection using kinematic data in cerebral palsy children and normal adults gait. Gait Posture 2009, 29, 76–80. [Google Scholar] [CrossRef]
- De Stefano, A.; Burridge, J.H.; Yule, V.T.; Allen, R. Effect of gait cycle selection on EMG analysis during walking in adults and children with gait pathology. Gait Posture 2004, 20, 92–101. [Google Scholar] [CrossRef]
- Perry, J. Gait Analysis—Normal and Pathological Function; Slack Inc.: Thorofare, NJ, USA, 1992. [Google Scholar]
- Di Nardo, F.; Agostini, V.; Strazza, A.; Nascimbeni, A.; Knaflitz, M.; Burattini, L.; Fioretti, S. Gait asymmetry in Winters’ group I hemiplegic children. In IFMBE Proceedings; Springer: Berlin, Germany, 2017; Volume 65, pp. 976–979. [Google Scholar]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Nardo, F.; Strazza, A.; Mengarelli, A.; Cardarelli, S.; Tigrini, A.; Verdini, F.; Nascimbeni, A.; Agostini, V.; Knaflitz, M.; Fioretti, S. EMG-Based Characterization of Walking Asymmetry in Children with Mild Hemiplegic Cerebral Palsy. Biosensors 2019, 9, 82. https://doi.org/10.3390/bios9030082
Di Nardo F, Strazza A, Mengarelli A, Cardarelli S, Tigrini A, Verdini F, Nascimbeni A, Agostini V, Knaflitz M, Fioretti S. EMG-Based Characterization of Walking Asymmetry in Children with Mild Hemiplegic Cerebral Palsy. Biosensors. 2019; 9(3):82. https://doi.org/10.3390/bios9030082
Chicago/Turabian StyleDi Nardo, Francesco, Annachiara Strazza, Alessandro Mengarelli, Stefano Cardarelli, Andrea Tigrini, Federica Verdini, Alberto Nascimbeni, Valentina Agostini, Marco Knaflitz, and Sandro Fioretti. 2019. "EMG-Based Characterization of Walking Asymmetry in Children with Mild Hemiplegic Cerebral Palsy" Biosensors 9, no. 3: 82. https://doi.org/10.3390/bios9030082