Wearable Multisensor Ring-Shaped Probe for Assessing Stress and Blood Oxygenation: Design and Preliminary Measurements

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
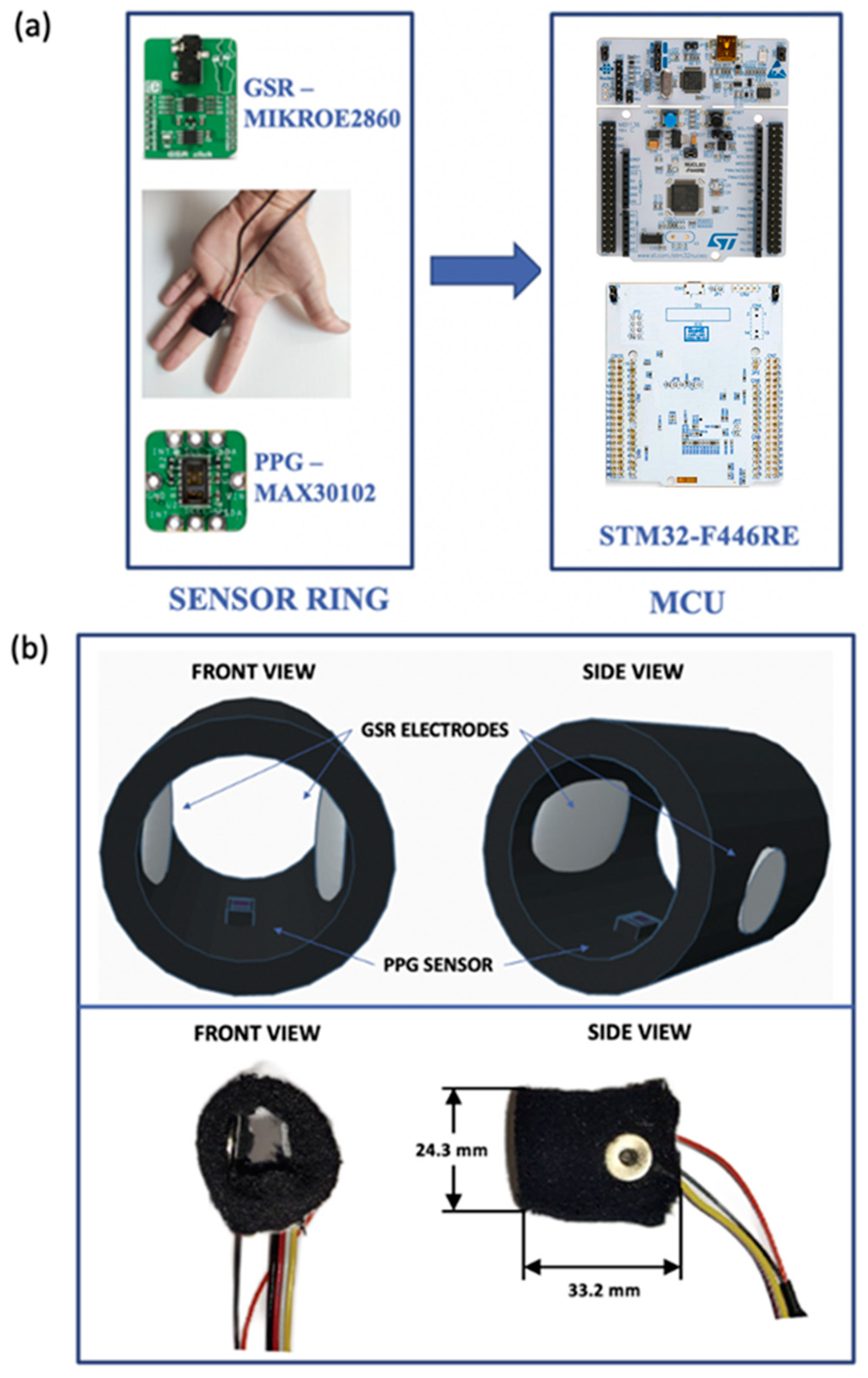
2.1. Description of the Realized Wearable Biosensing System
2.2. Experimental Protocol
- Rest 1 (R1): the subject under test watched relaxing videos (nature, sea, sunset). The duration of this phase was 180 s;
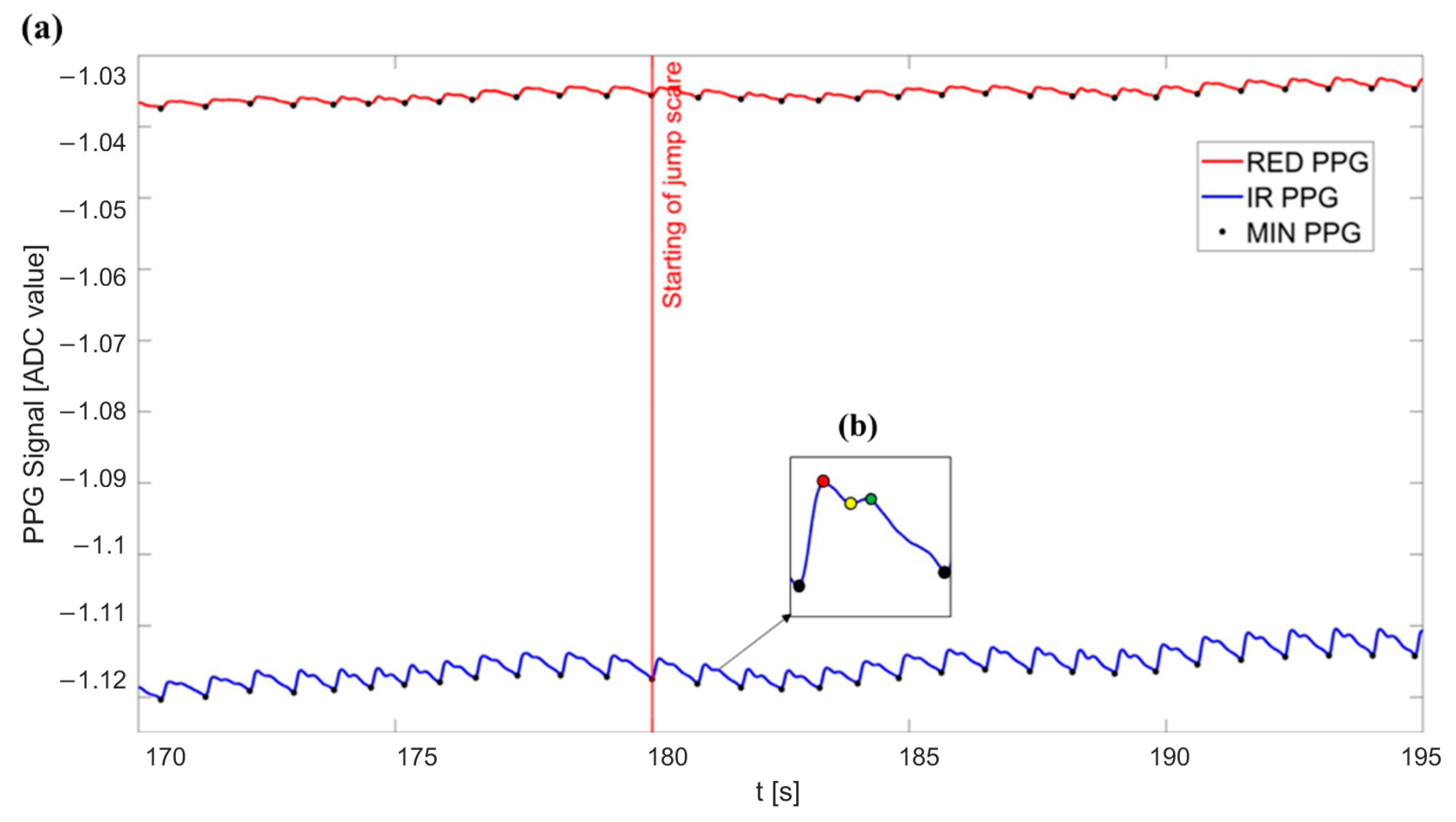
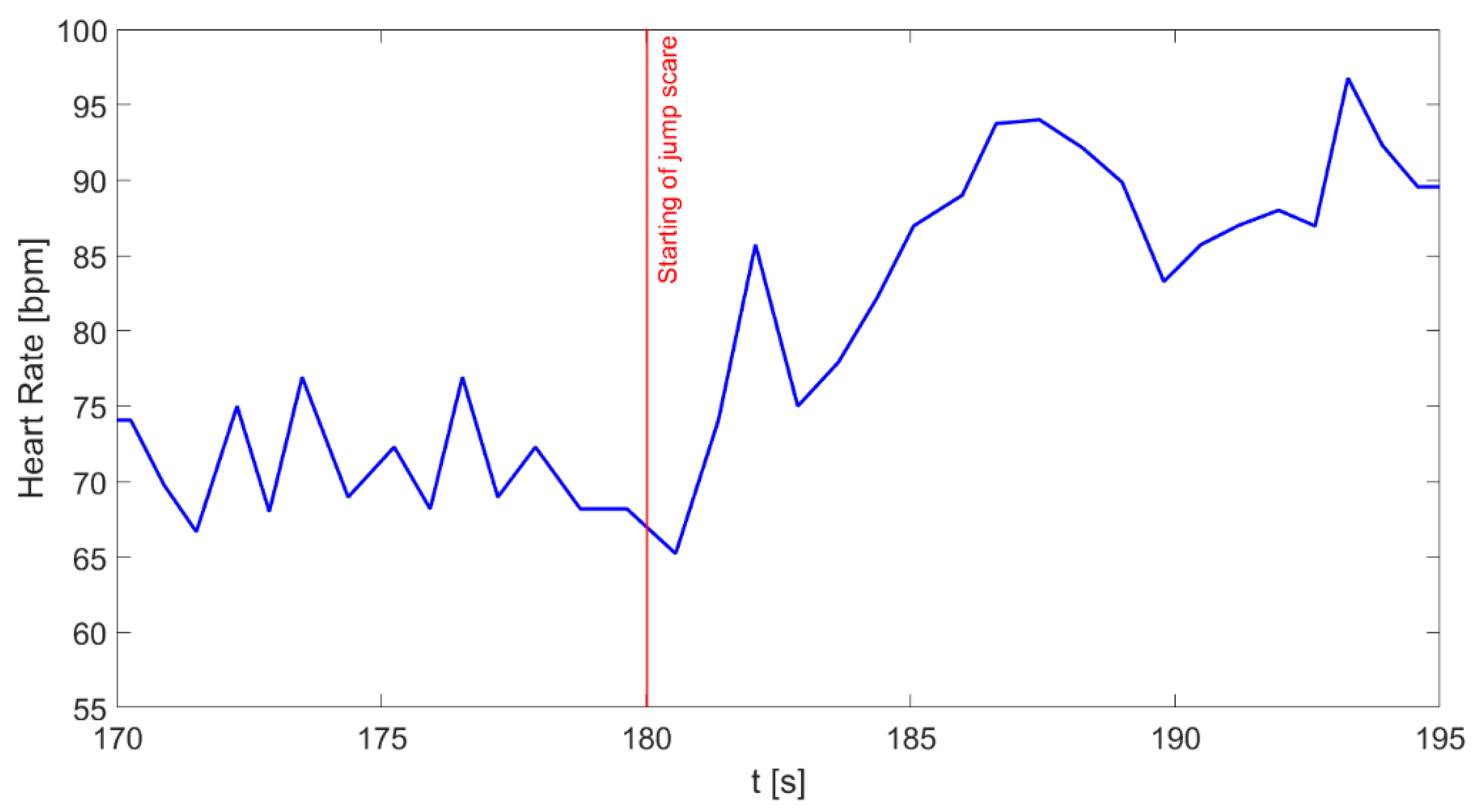
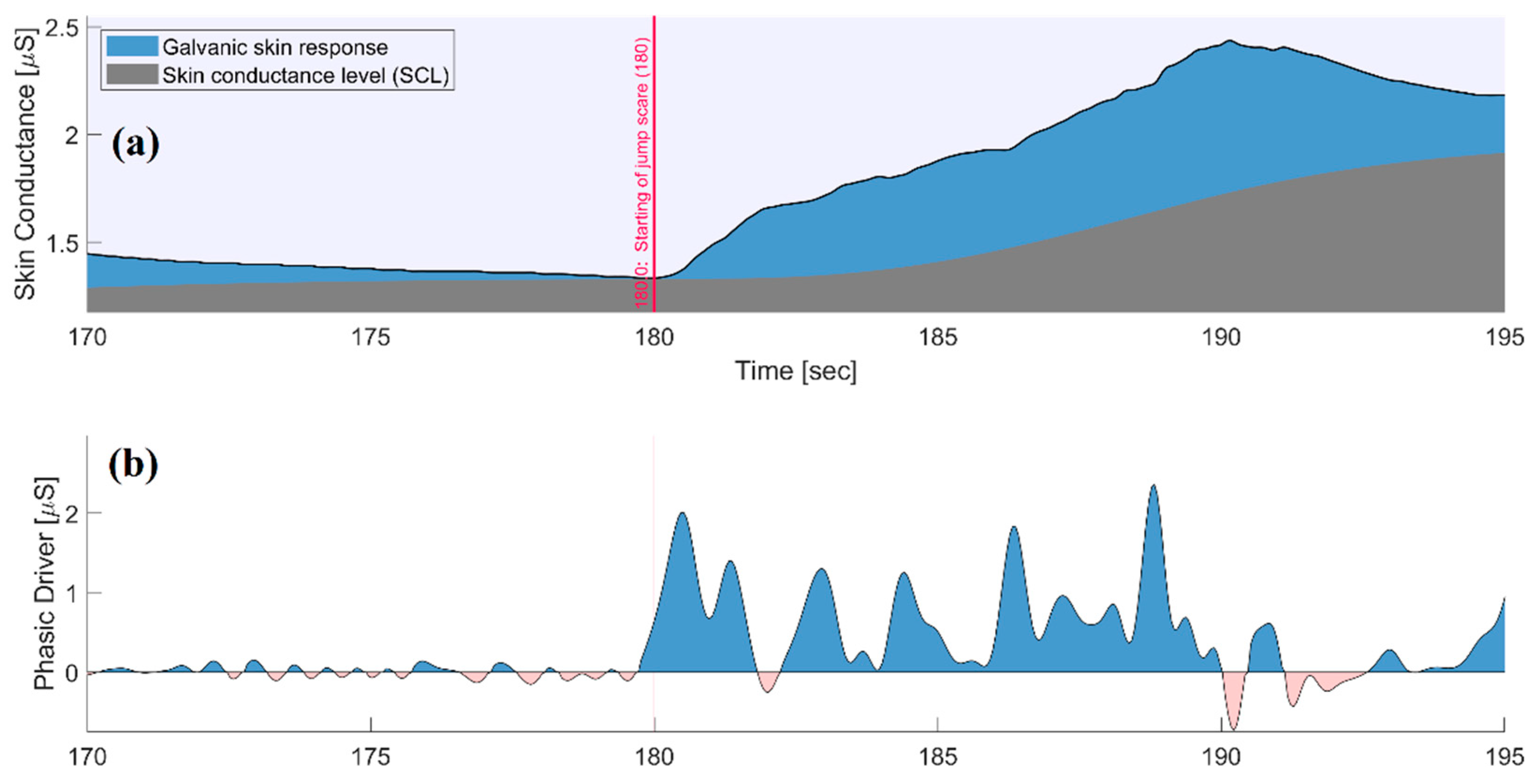
- Sudden fright (SF): the subject experienced a sudden vision of a jump scare video (with the aim of arousing fright). The duration of this phase was 10 s;
- Rest 2 (R2): the subject watched another relaxing video to re-establish a resting condition and allow the complete recovery of the physiological parameters. The duration of this phase was 180 s;
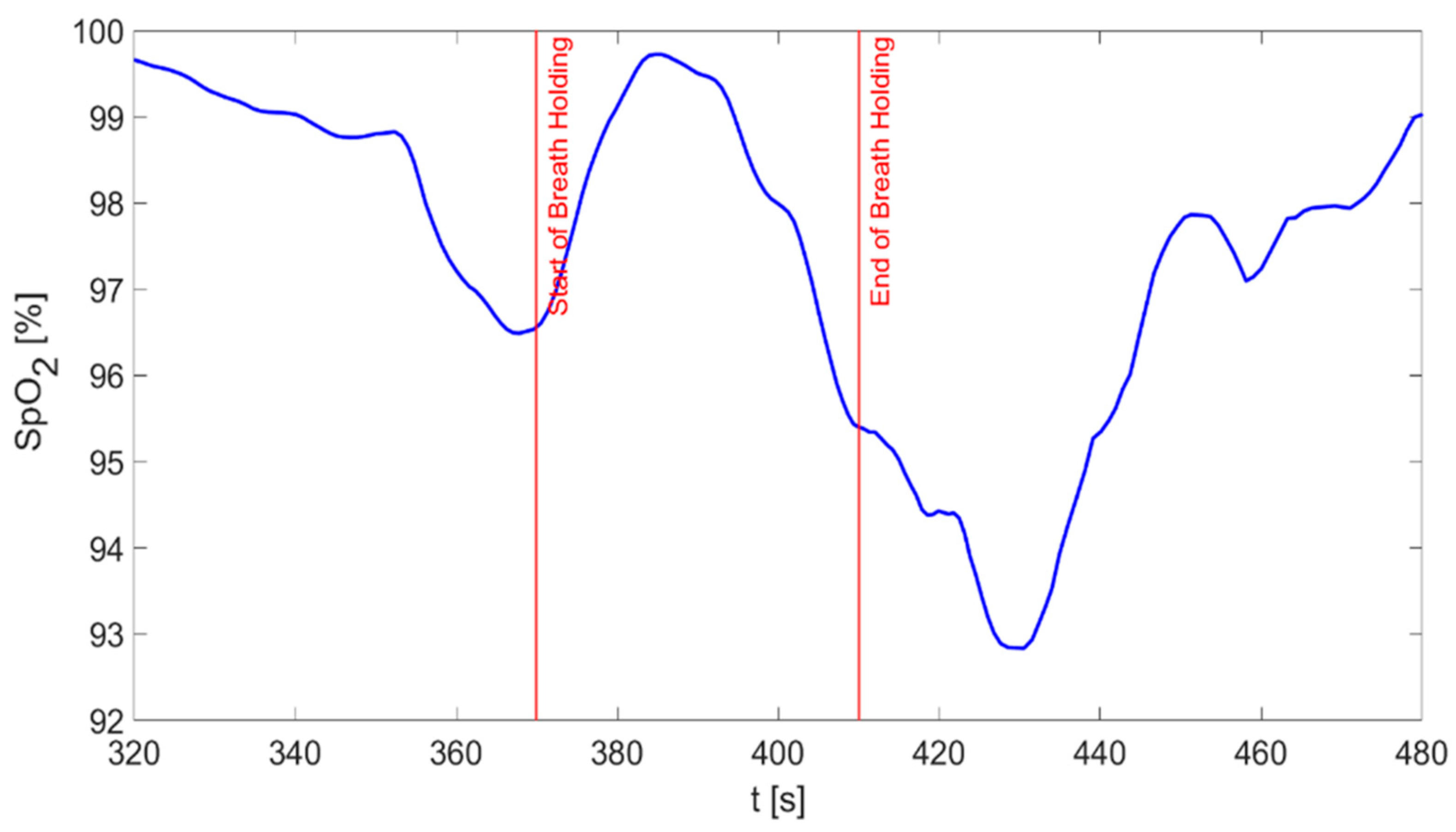
- Breath holding (BH): the subject was asked to hold his breath for 40 s;
- Rest 3 (R3): the subject started to breathe again normally to allow the complete recovery of the physiological parameters. The duration of this phase was 180 s.
2.3. Data Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Inui, T.; Kohno, H.; Kawasaki, Y.; Matsuura, K.; Ueda, H.; Tamura, Y.; Watanabe, M.; Inage, Y.; Yakita, Y.; Wakabayashi, Y.; et al. Use of a Smart Watch for Early Detection of Paroxysmal Atrial Fibrillation: Validation Study. JMIR Cardio 2020, 4, e14857. [Google Scholar] [CrossRef] [PubMed]
- Bellenger, C.R.; Miller, D.J.; Halson, S.L.; Roach, G.D.; Sargent, C. Wrist-Based Photoplethysmography Assessment of Heart Rate and Heart Rate Variability: Validation of Whoop. Sensors 2021, 21, 3571. [Google Scholar] [CrossRef]
- Zhu, P.; Yang, D.; Zhu, J. SpO2 and Heart Rate Measurement with Wearable Watch Based on PPG. In Proceedings of the 2015 IET International Conference on Biomedical Image and Signal Processing (ICBISP 2015), Beijing, China, 19 November 2015; Institution of Engineering and Technology: Stevenage, UK, 2015; p. 5. [Google Scholar]
- Kwon, S.; Hong, J.; Choi, E.-K.; Lee, B.; Baik, C.; Lee, E.; Jeong, E.-R.; Koo, B.-K.; Oh, S.; Yi, Y. Detection of Atrial Fibrillation Using a Ring-Type Wearable Device (CardioTracker) and Deep Learning Analysis of Photoplethysmography Signals: Prospective Observational Proof-of-Concept Study. J. Med. Internet Res. 2020, 22, e16443. [Google Scholar] [CrossRef]
- Agro, D.; Canicatti, R.; Tomasino, A.; Giordano, A.; Adamo, G.; Parisi, A.; Pernice, R.; Stivala, S.; Giaconia, C.; Busacca, A.C.; et al. PPG Embedded System for Blood Pressure Monitoring. In Proceedings of the 2014 AEIT Annual Conference—From Research to Industry: The Need for a More Effective Technology Transfer, AEIT, Trieste, Italy, 18–19 September 2014; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2015. [Google Scholar]
- Maeda, Y.; Sekine, M.; Tamura, T. The Advantages of Wearable Green Reflected Photoplethysmography. J. Med. Syst. 2011, 35, 829–834. [Google Scholar] [CrossRef]
- Dutt, D.N.; Shruthi, S. Digital Processing of ECG and PPG Signals for Study of Arterial Parameters for Cardiovascular Risk Assessment. In Proceedings of the 2015 International Conference on Communication and Signal Processing, ICCSP 2015, Melmaruvathur, India, 2–4 April 2015; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2015; pp. 1506–1510. [Google Scholar]
- Oreggia, D.; Guarino, S.; Parisi, A.; Pernice, R.; Adamo, G.; Mistretta, L.; di Buono, P.; Fallica, G.; Ferla, G.; Cino, A.C.; et al. Physiological Parameters Measurements in a Cardiac Cycle via a Combo PPG-ECG System. In Proceedings of the 2015 AEIT International Annual Conference, AEIT 2015, Naples, Italy, 14–16 October 2015; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2015. [Google Scholar]
- Pernice, R.; Parisi, A.; Adamo, G.; Guarino, S.; Faes, L.; Busacca, A. A Portable System for Multiple Parameters Monitoring: Towards Assessment of Health Conditions and Stress Level in the Automotive Field. In Proceedings of the 2019 AEIT International Conference of Electrical and Electronic Technologies for Automotive, AEIT AUTOMOTIVE, Turin, Italy, 2–4 July 2019; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019. [Google Scholar]
- Allen, J. Photoplethysmography and Its Application in Clinical Physiological Measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [Green Version]
- Gil, E.; Orini, M.; Bailón, R.; Vergara, J.M.; Mainardi, L.; Laguna, P. Photoplethysmography Pulse Rate Variability as a Surrogate Measurement of Heart Rate Variability during Non-Stationary Conditions. Physiol. Meas. 2010, 31, 1271–1290. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pernice, R.; Javorka, M.; Krohova, J.; Czippelova, B.; Turianikova, Z.; Busacca, A.; Faes, L. Comparison of Short-Term Heart Rate Variability Indexes Evaluated through Electrocardiographic and Continuous Blood Pressure Monitoring. Med. Biol. Eng. Comput. 2019, 57, 1247–1263. [Google Scholar] [CrossRef]
- Hamaad, A.; Lip, G.Y.H.; MacFadyen, R.J. Heart Rate Variability Estimates of Autonomic Tone: Relationship to Mapping Pathological and Procedural Stress Responses in Coronary Disease. Ann. Med. 2004, 36, 448–461. [Google Scholar] [CrossRef]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A Healthy Heart Is Not a Metronome: An Integrative Review of the Heart’s Anatomy and Heart Rate Variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalid, S.G.; Ali, S.M.; Liu, H.; Qurashi, A.G.; Ali, U. Photoplethysmography Temporal Marker-Based Machine Learning Classifier for Anesthesia Drug Detection. Med. Biol. Eng. Comput. 2022, 60, 3057–3068. [Google Scholar] [CrossRef] [PubMed]
- Lazazzera, R.; Deviaene, M.; Varon, C.; Buyse, B.; Testelmans, D.; Laguna, P.; Gil, E.; Carrault, G. Detection and Classification of Sleep Apnea and Hypopnea Using PPG and SpO2 Signals. IEEE Trans. Biomed. Eng. 2021, 68, 1496–1506. [Google Scholar] [CrossRef]
- Zhang, X.; Kassem, M.A.M.; Zhou, Y.; Shabsigh, M.; Wang, Q.; Xu, X. A Brief Review of Non-Invasive Monitoring of Respiratory Condition for Extubated Patients with or at Risk for Obstructive Sleep Apnea after Surgery. Front. Med. 2017, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Manta, C.; Jain, S.S.; Coravos, A.; Mendelsohn, D.; Izmailova, E.S. An Evaluation of Biometric Monitoring Technologies for Vital Signs in the Era of COVID-19. Clin. Transl. Sci. 2020, 13, 1034–1044. [Google Scholar] [CrossRef]
- dos Santos, R.R.; da Silva, T.M.; Silva, L.E.V.; Eckeli, A.L.; Salgado, H.C.; Fazan, R. Correlation between Heart Rate Variability and Polysomnography-Derived Scores of Obstructive Sleep Apnea. Front. Netw. Physiol. 2022, 2, 958550. [Google Scholar] [CrossRef]
- Santiago-Fuentes, L.M.; Charleston-Villalobos, S.; González-Camarena, R.; Voss, A.; Mejía-Avila, M.E.; Buendía-Roldan, I.; Reulecke, S.; Aljama-Corrales, T. Effects of Supplemental Oxygen on Cardiovascular and Respiratory Interactions by Extended Partial Directed Coherence in Idiopathic Pulmonary Fibrosis. Front. Netw. Physiol. 2022, 2, 834056. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse Oximetry: Fundamentals and Technology Update. Med. Devices Evid. Res. 2014, 7, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Mannheimer, P.D. The Light–Tissue Interaction of Pulse Oximetry. Anesth. Analg. 2007, 105, S10–S17. [Google Scholar] [CrossRef]
- Selye, H. Forty Years of Stress Research: Principal Remaining Problems and Misconceptions. Can. Med. Assoc. J. 1976, 115, 53–56. [Google Scholar]
- Braithwaite, J.J.; Derrick, D.; Watson, G.; Jones, R.; Rowe, M. A Guide for Analysing Electrodermal Activity (EDA) & Skin Conductance Responses (SCRs) for Psychological Experiments; University of Birmingham: Birmingham, UK, 2015. [Google Scholar]
- Cunanan, A.J.; DeWeese, B.H.; Wagle, J.P.; Carroll, K.M.; Sausaman, R.; Hornsby, W.G.; Haff, G.G.; Triplett, N.T.; Pierce, K.C.; Stone, M.H. The General Adaptation Syndrome: A Foundation for the Concept of Periodization. Sport. Med. 2018, 48, 787–797. [Google Scholar] [CrossRef]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The Relationship of Autonomic Imbalance, Heart Rate Variability and Cardiovascular Disease Risk Factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.A.; Picard, R.W. Detecting Stress during Real-World Driving Tasks Using Physiological Sensors. IEEE Trans. Intell. Transp. Syst. 2005, 6, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, J.; Paredes, P.; Roseway, A.; Czerwinski, M. Under Pressure: Sensing Stress of Computer Users. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, New York, NY, USA, 26 April–1 May 2014; pp. 51–60. [Google Scholar]
- Alberdi, A.; Aztiria, A.; Basarab, A. Towards an Automatic Early Stress Recognition System for Office Environments Based on Multimodal Measurements: A Review. J. Biomed. Inform. 2016, 59, 49–75. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.M.; Zachariae, R. Autonomic Reactivity to Cognitive and Emotional Stress of Low, Medium, and High Hypnotizable Healthy Subjects: Testing Predictions from the High Risk Model of Threat Perception. Int. J. Clin. Exp. Hypn. 2002, 50, 248–275. [Google Scholar] [CrossRef] [PubMed]
- Posada-Quintero, H.F.; Bolkhovsky, J.B. Machine Learning Models for the Identification of Cognitive Tasks Using Autonomic Reactions from Heart Rate Variability and Electrodermal Activity. Behav. Sci. 2019, 9, 45. [Google Scholar] [CrossRef] [Green Version]
- Arya, L.; Sethia, D. HRV and GSR as Viable Physiological Markers for Mental Health Recognition. In Proceedings of the 2022 14th International Conference on Communication Systems & Networks (COMSNETS), Bengaluru, India, 4–8 January 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 37–42. [Google Scholar]
- Volpes, G.; Valenti, S.; Parisi, A.; Busacca, A.; Faes, L.; Pernice, R. Low-Invasive Multisensor Real-Time Acquisition System for the Assessment of Cardiorespiratory and Skin Conductance Parameters. In Proceedings of the MELECON 2022—IEEE Mediterranean Electrotechnical Conference, Palermo, Italy, 14–16 June 2022; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2022; pp. 936–941. [Google Scholar]
- MikroElektronika GSR CLICK. Available online: https://www.mikroe.com/gsr-click (accessed on 24 February 2023).
- Přibil, J.; Přibilová, A.; Frollo, I. Comparative Measurement of the PPG Signal on Different Human Body Positions by Sensors Working in Reflection and Transmission Modes. Eng. Proc. 2020, 2, 69. [Google Scholar]
- Maxim Integrated Products, Inc. MAX30102-High-Sensitivity Pulse Oximeter and Heart-Rate Sensor for Wearable Health, Datasheet. Available online: https://www.analog.com/media/en/technical-documentation/data-sheets/max30102.pdf (accessed on 24 February 2023).
- Béres, S.; Hejjel, L. The Minimal Sampling Frequency of the Photoplethysmogram for Accurate Pulse Rate Variability Parameters in Healthy Volunteers. Biomed. Signal Process. Control. 2021, 68, 102589. [Google Scholar] [CrossRef]
- Mejía-Mejía, E.; Budidha, K.; Abay, T.Y.; May, J.M.; Kyriacou, P.A. Heart Rate Variability (HRV) and Pulse Rate Variability (PRV) for the Assessment of Autonomic Responses. Front. Physiol. 2020, 11, 779. [Google Scholar] [CrossRef] [PubMed]
- Prahl, S. Optical Absorption of Hemoglobin. Available online: https://omlc.org/spectra/hemoglobin/ (accessed on 24 February 2023).
- Hay, O.Y.; Cohen, M.; Nitzan, I.; Kasirer, Y.; Shahroor-Karni, S.; Yitzhaky, Y.; Engelberg, S.; Nitzan, M. Pulse Oximetry with Two Infrared Wavelengths without Calibration in Extracted Arterial Blood. Sensors 2018, 18, 3457. [Google Scholar] [CrossRef] [Green Version]
- Abtahi, M.; Amiri, A.M.; Byrd, D.; Mankodiya, K. Hand Motion Detection in FNIRS Neuroimaging Data. Healthcare 2017, 5, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libelium MySignals SW EHealth and Medical IoT Development Platform Technical Guide. Available online: https://www.generationrobots.com/media/mysignals_technical_guide_sw.pdf (accessed on 24 February 2023).
- Oak, S.-S.; Aroul, P. How to Design Peripheral Oxygen Saturation (SpO2) and Optical Heart Rate Monitoring (OHRM) Systems Using AFE4403; Texas Instruments: Dallas, TX, USA, 2015. [Google Scholar]
- Lopez, S.; Americas, R.T.A.C. Pulse Oximeter—Fundamentals and Design; Freescale Semiconductor: Austin, TX, USA, 2012; p. 23. [Google Scholar]
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse Oximetry: Understanding Its Basic Principles Facilitates Appreciation of Its Limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, K.A.; George, B.; Mohan, N.M.; Kumar, V.J. A Novel Calibration-Free Method of Measurement of Oxygen Saturation in Arterial Blood. In Proceedings of the IEEE Transactions on Instrumentation and Measurement; IEEE: Piscataway, NJ, USA, 2009; Volume 58, pp. 1699–1705. [Google Scholar]
- Operation Manual BM1000 Pulse Oximeter BERRYMED LIMITED. Available online: https://fccid.io/2AG2CBM1000B/User-Manual/UserManual-2882675 (accessed on 24 February 2023).
- Stubán, N.; Masatsugu, N. Non-Invasive Calibration Method for Pulse Oximeters. Period. Polytech. Electr. Eng. 2008, 52, 91–94. [Google Scholar] [CrossRef]
- Benedek, M.; Kaernbach, C. A Continuous Measure of Phasic Electrodermal Activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fruet, D.; Bara, C.; Pernice, R.; Faes, L.; Nollo, G. Assessment of Driving Stress Through SVM And KNN Classifiers on Multi-Domain Physiological Data. In Proceedings of the MELECON 2022—IEEE Mediterranean Electrotechnical Conference, Palermo, Italy, 14–16 June 2022; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2022; pp. 920–925. [Google Scholar]
- Rahma, O.; Putra, A.; Rahmatillah, A.; Putri, Y.; Fajriaty, N.; Ain, K.; Chai, R. Electrodermal Activity for Measuring Cognitive and Emotional Stress Level. J. Med. Signals Sens. 2022, 12, 155–162. [Google Scholar] [CrossRef]
- Shi, P.; Hu, S.; Zhu, Y.; Zheng, J.; Qiu, Y.; Cheang, P.Y.S. Insight into the Dicrotic Notch in Photoplethysmographic Pulses from the Finger Tip of Young Adults. J. Med. Eng. Technol. 2009, 33, 628–633. [Google Scholar] [CrossRef]
- Moscato, S.; Palmerini, L.; Palumbo, P.; Chiari, L. Quality Assessment and Morphological Analysis of Photoplethysmography in Daily Life. Front. Digit. Health 2022, 4, 912353. [Google Scholar] [CrossRef]
- Suma, P.; Suma, K.V. Pulse Rate Variability for Detection of Autonomic Tone of an Individual. In Proceedings of the 2019 4th International Conference on Recent Trends on Electronics, Information, Communication & Technology (RTEICT), Bangalore, India, 17–18 May 2019; pp. 1172–1177. [Google Scholar]
- Goldstein, D.S. Stress-Induced Activation of the Sympathetic Nervous System. Baillieres Clin. Endocrinol. Metab. 1987, 1, 253–278. [Google Scholar] [CrossRef]
- Hirsch, J.A.; Bishop, B. Respiratory Sinus Arrhythmia in Humans: How Breathing Pattern Modulates Heart Rate. Am. J. Physiol. Heart Circ. Physiol. 1981, 241, H620–H629. [Google Scholar] [CrossRef] [Green Version]
- Javorka, M.; Krohova, J.; Czippelova, B.; Turianikova, Z.; Mazgutova, N.; Wiszt, R.; Ciljakova, M.; Cernochova, D.; Pernice, R.; Busacca, A.; et al. Respiratory Sinus Arrhythmia Mechanisms in Young Obese Subjects. Front. Neurosci. 2020, 14, 204. [Google Scholar] [CrossRef] [Green Version]
- Scully, C.G.; Lee, J.; Meyer, J.; Gorbach, A.M.; Granquist-Fraser, D.; Mendelson, Y.; Chon, K.H. Physiological Parameter Monitoring from Optical Recordings with a Mobile Phone. IEEE Trans. Biomed. Eng. 2012, 59, 303–306. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Zhang, J.; Gong, Y.; Xu, L.; Liu, H.; Wei, S.; Wu, Y.; Cha, G.; Wei, H.; Mao, J. Reliable Detection of Myocardial Ischemia Using Machine Learning Based on Temporal-Spatial Characteristics of Electrocardiogram and Vectorcardiogram. Front. Physiol. 2022, 13, 854191. [Google Scholar] [CrossRef] [PubMed]
- Geng, Y.; Wu, X.; Liu, H.; Zheng, D.; Xia, L. Index of Microcirculatory Resistance: State-of-the-Art and Potential Applications in Computational Simulation of Coronary Artery Disease. J. Zhejiang Univ. Sci. B 2022, 23, 123–140. [Google Scholar] [CrossRef]
- Allen, J.; Liu, H.; Iqbal, S.; Zheng, D.; Stansby, G. Deep Learning-Based Photoplethysmography Classification for Peripheral Arterial Disease Detection: A Proof-of-Concept Study. Physiol. Meas. 2021, 42, 054002. [Google Scholar] [CrossRef] [PubMed]
- Bentham, M.; Stansby, G.; Allen, J. Innovative Multi-Site Photoplethysmography Analysis for Quantifying Pulse Amplitude and Timing Variability Characteristics in Peripheral Arterial Disease. Diseases 2018, 6, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zang, Y.; Dai, L.; Zhan, H.; Dou, J.; Xia, L.; Zhang, H. Theoretical Investigation of the Mechanism of Heart Failure Using a Canine Ventricular Cell Model: Especially the Role of up-Regulated CaMKII and SR Ca2+ Leak. J. Mol. Cell Cardiol. 2013, 56, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Chung, H.; Ko, H.; Parisi, A.; Busacca, A.; Faes, L.; Pernice, R.; Lee, J. Adaptive Scheduling of Acceleration and Gyroscope for Motion Artifact Cancelation in Photoplethysmography. Comput. Methods Programs Biomed. 2022, 226, 107126. [Google Scholar] [CrossRef]
- Liu, H.; Allen, J.; Khalid, S.G.; Chen, F.; Zheng, D. Filtering-Induced Time Shifts in Photoplethysmography Pulse Features Measured at Different Body Sites: The Importance of Filter Definition and Standardization. Physiol. Meas. 2021, 42, 074001. [Google Scholar] [CrossRef]
- Xu, W.; Bian, S.; Dong, B.; Shen, Y.; Han, S.; Yu, C.; Zhao, W.; Wang, Y. Unobtrusive Vital Signs and Activity Monitoring Based on Dual Mode Fiber. Opt. Fiber Technol. 2021, 64, 102530. [Google Scholar] [CrossRef]
- Volpes, G.; Sparacino, L.; Valenti, S.; Parisi, A.; Busacca, A.; Faes, L.; Pernice, R. A Portable Multisensor System to Assess Cardiorespiratory Interactions through Photoplethysmography. In Proceedings of the 2022 IEEE International Symposium on Medical Measurements and Applications, MeMeA, Messina, Italy, 22–24 June 2022; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2022. [Google Scholar]
- Volpes, G.; Barà, C.; Busacca, A.; Stivala, S.; Javorka, M.; Faes, L.; Pernice, R. Feasibility of Ultra-Short-Term Analysis of Heart Rate and Systolic Arterial Pressure Variability at Rest and during Stress via Time-Domain and Entropy-Based Measures. Sensors 2022, 22, 9149. [Google Scholar] [CrossRef]
- Goessl, V.C.; Curtiss, J.E.; Hofmann, S.G. The Effect of Heart Rate Variability Biofeedback Training on Stress and Anxiety: A Meta-Analysis. Psychol. Med. 2017, 47, 2578–2586. [Google Scholar] [CrossRef] [PubMed]
- Dolson, C.M.; Harlow, E.R.; Phelan, D.M.; Gabbett, T.J.; Gaal, B.; McMellen, C.; Geletka, B.J.; Calcei, J.G.; Voos, J.E.; Seshadri, D.R. Wearable Sensor Technology to Predict Core Body Temperature: A Systematic Review. Sensors 2022, 22, 7639. [Google Scholar] [CrossRef] [PubMed]
- Awotunde, J.B.; Jimoh, R.G.; AbdulRaheem, M.; Oladipo, I.D.; Folorunso, S.O.; Ajamu, G.J. IoT-Based Wearable Body Sensor Network for COVID-19 Pandemic. In Advances in Data Science and Intelligent Data Communication Technologies for COVID-19: Innovative Solutions against COVID-19; Hassanien, A.-E., Elghamrawy, S.M., Zelinka, I., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 253–275. ISBN 978-3-030-77302-1. [Google Scholar]
- Casson, A.J.; Vazquez Galvez, A.; Jarchi, D. Gyroscope vs. Accelerometer Measurements of Motion from Wrist PPG during Physical Exercise. ICT Express 2016, 2, 175–179. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure/Phase | R1 | SF | R2 | BH | R3 |
|---|---|---|---|---|---|
| PPI mean [ms] PPI SDNN [ms] | 815 ± 61 61 ± 19 | 778 ± 65 65 ± 38 | 806 ± 60 60 ± 16 | 876 ± 104 104 ± 81 | 817 ± 58 58 ± 5 |
| GSR mean [µS] SCL mean [µS] | 0.07 ± 0.05 0.06 ± 0.04 | 0.17 ± 0.09 0.10 ± 0.08 | 0.12 ± 0.10 0.10 ± 0.09 | 0.13 ± 0.10 0.11 ± 0.09 | 0.14 ± 0.11 0.12 ± 0.11 |
| Time Window | W1 (R1 End) | W2 (SF Start) | W3 (R2 Start) | W4 (R2 End) | W5 (BH Start) |
|---|---|---|---|---|---|
| No of SCR peaks | 1.3 | 5.3 | 2.7 | 1.3 | 3.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenti, S.; Volpes, G.; Parisi, A.; Peri, D.; Lee, J.; Faes, L.; Busacca, A.; Pernice, R. Wearable Multisensor Ring-Shaped Probe for Assessing Stress and Blood Oxygenation: Design and Preliminary Measurements. Biosensors 2023, 13, 460. https://doi.org/10.3390/bios13040460
Valenti S, Volpes G, Parisi A, Peri D, Lee J, Faes L, Busacca A, Pernice R. Wearable Multisensor Ring-Shaped Probe for Assessing Stress and Blood Oxygenation: Design and Preliminary Measurements. Biosensors. 2023; 13(4):460. https://doi.org/10.3390/bios13040460
Chicago/Turabian StyleValenti, Simone, Gabriele Volpes, Antonino Parisi, Daniele Peri, Jinseok Lee, Luca Faes, Alessandro Busacca, and Riccardo Pernice. 2023. "Wearable Multisensor Ring-Shaped Probe for Assessing Stress and Blood Oxygenation: Design and Preliminary Measurements" Biosensors 13, no. 4: 460. https://doi.org/10.3390/bios13040460