Patient Stratification for Antibiotic Prescriptions Based on the Bound-Free Phase Detection Immunoassay of C-Reactive Protein in Serum Samples

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Ethics Permission
2.2. Measurements Using the Immunoturbidimetric Assay Kit
2.3. Measurements Using the CE-IVD ELISA Kit
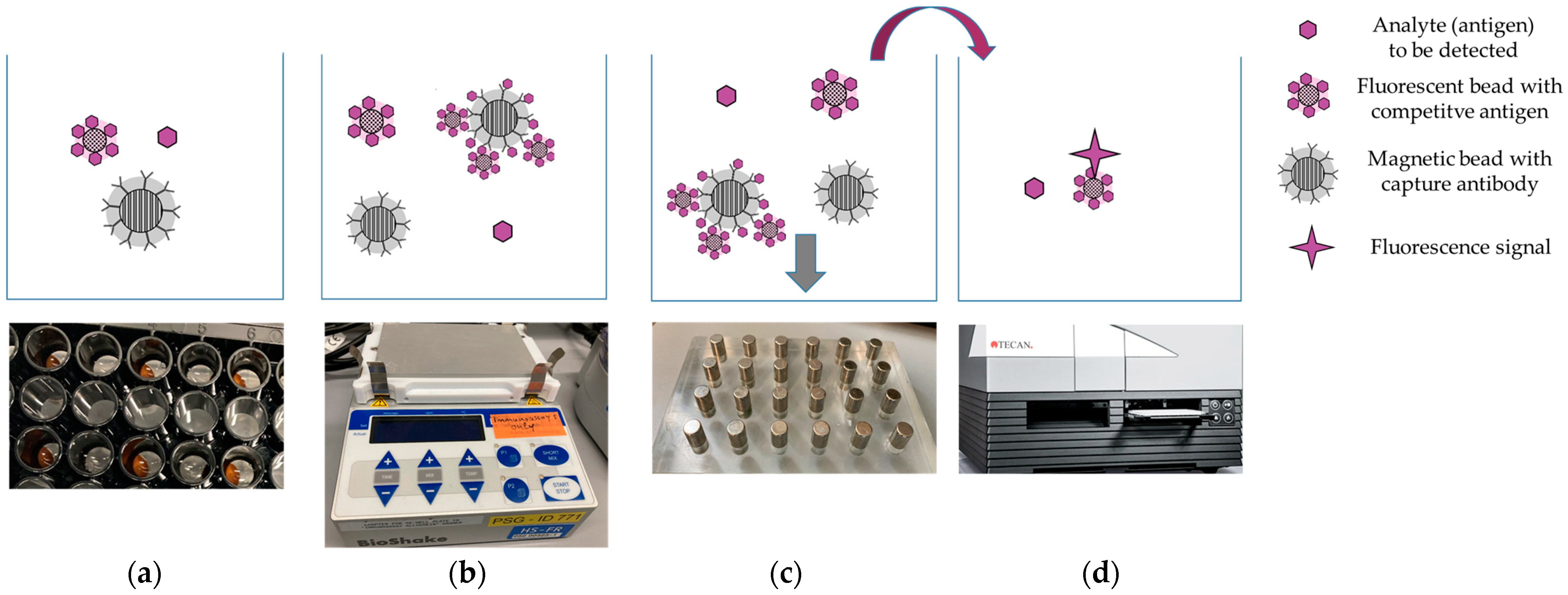
2.4. Measurements Using the BFPD-IA
3. Results and Discussion
3.1. Methods Comparison
3.2. The Clinical Relevance
3.3. The Implementation Perspective and Integration in Clinical Practice
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: A patient level meta-analysis. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef]
- Smedemark, S.A.; Aabenhus, R.; Llor, C.; Fournaise, A.; Olsen, O.; Jørgensen, K.J. Biomarkers as point-of-care tests to guide prescription of antibiotics in people with acute respiratory infections in primary care. Cochrane Database Syst. Rev. 2022, 10, CD010130. [Google Scholar] [CrossRef] [PubMed]
- C-Reactive Protein Point-of-Care Testing (CRP POCT) to Guide Antibiotic Prescribing in Primary Care Settings for Acute Respiratory Tract Infections (RTIs). Rapid Assessment on Other Health Technologies Using the HTA Core Model for Rapid Relative Effectiveness Assessment. EUnetHTA Project ID: OTCA012. 2019. Available online: https://www.eunethta.eu/wp-content/uploads/2019/02/EUnetHTA_OTCA012_CRP-POCT_31012019.pdf (accessed on 3 June 2023).
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Cals, J.W.L.; Butler, C.C.; Hopstaken, R.M.; Hood, K.; Dinant, G.-J. Effect of point of care testing for C reactive protein and training in communication skills on antibiotic use in lower respiratory tract infections: Cluster randomised trial. BMJ 2009, 338, b1374. [Google Scholar] [CrossRef] [PubMed]
- Cals, J.W.L.; Schot, M.J.C.; de Jong, S.A.M.; Dinant, G.-J.; Hopstaken, R.M. Point-of-care C-reactive protein testing and antibiotic prescribing for respiratory tract infections: A randomized controlled trial. Ann. Fam. Med. 2010, 8, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, K.A.; Melbye, H.; Kelly, M.J.; Ceynowa, C.; Mölstad, S.; Hood, K.; Butler, C.C. Influence of CRP testing and clinical findings on antibiotic prescribing in adults presenting with acute cough in primary care. Scand. J. Prim. Health Care 2010, 28, 229–236. [Google Scholar] [CrossRef]
- Cooke, J.; Llor, C.; Hopstaken, R.; Dryden, M.; Butler, C. Respiratory tract infections (RTIs) in primary care: Narrative review of C reactive protein (CRP) point-of-care testing (POCT) and antibacterial use in patients who present with symptoms of RTI. BMJ Open Resp. Res. 2015, 2, e000086. [Google Scholar] [CrossRef]
- Little, P.; Stuart, B.; Francis, N.; Douglas, E.; Tonkin-Crine, S.; Anthierens, S.; Cals, J.W.; Melbye, H.; Santer, M.; Moore, M.; et al. Effects of internet-based training on antibiotic prescribing rates for acute respiratory-tract infections: A multinational, cluster, randomised, factorial, controlled trial. Lancet 2013, 382, 1175–1182. [Google Scholar] [CrossRef]
- Butler, C.C.; Gillespie, D.; White, P.; Bates, J.; Lowe, R.; Thomas-Jones, E.; Wootton, M.; Hood, K.; Phillips, R.; Melbye, H.; et al. C-Reactive Protein Testing to Guide Antibiotic Prescribing for COPD Exacerbations. N. Engl. J. Med. 2019, 381, 111–120. [Google Scholar] [CrossRef]
- Boere, T.M.; van Buul, L.W.; Hopstaken, R.M.; Veenhuizen, R.B.; van Tulder, M.W.; Cals, J.W.L.; Verheij, T.J.M.; Hertogh, C.M.P.M. Using point-of-care C-reactive protein to guide antibiotic prescribing for lower respiratory tract infections in elderly nursing home residents (UPCARE): Study design of a cluster randomized controlled trial. BMC Health Serv. Res. 2020, 20, 149. [Google Scholar] [CrossRef]
- Eccles, S.; Pincus, C.; Higgins, B.; Woodhead, M.; on behalf of the Guideline Development Group. Diagnosis and management of community and hospital acquired pneumonia in adults: Summary of NICE guidance. BMJ 2014, 349, g6722. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S. A short history, principles, and types of ELISA, and our laboratory experience with peptide/protein analyses using ELISA. Peptides 2015, 72, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Tighe, P.J.; Ryder, R.R.; Todd, I.; Fairclough, L.C. ELISA in the multiplex era: Potentials and pitfalls. Proteom. Clin. Appl. 2015, 9, 406–422. [Google Scholar] [CrossRef] [PubMed]
- O’Kennedy, R.; Murphy, C. Immunoassays: Development, Applications and Future Trends; Pan Stanford Publishing: Milton, GA, USA, 2017. [Google Scholar]
- Luong, J.; Vashist, S.K. (Eds.) Handbook of Immunoassay Technologies: Approaches, Performances, and Applications; Academic Press an imprint of Elsevier: London, UK, 2018. [Google Scholar]
- van der Wal, F.J.; Bergervoet, J.H.W.; Achterberg, R.P.; Haasnoot, W. Bead-based immunoassays. In Novel Approaches in Immunoassays; Koistinen, H., Stenman, U.-H., Eds.; Future Medicine Ltd., Unitec House: London, UK, 2014; pp. 52–71. [Google Scholar]
- Vashist, S.K. Trends in Multiplex Immunoassays for In Vitro Diagnostics and Point-of-Care Testing. Diagnostics 2021, 11, 1630. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Shah, S.H.; Salman, M.; Abdullah, M.; Hayat, F.; Akbar, S. Enzyme-Linked Immunosorbent Assay versus Chemiluminescent Immunoassay: A General Overview. Glob. J. Med. Pharm. Biomed. Update 2023, 18, 1. [Google Scholar] [CrossRef]
- Johannsen, B.; Karpíšek, M.; Baumgartner, D.; Klein, V.; Bostanci, N.; Paust, N.; Früh, S.M.; Zengerle, R.; Mitsakakis, K. One-step, wash-free, bead-based immunoassay employing bound-free phase detection. Anal. Chim. Acta 2021, 1153, 338280. [Google Scholar] [CrossRef]
- Johannsen, B.; Baumgartner, D.; Karkossa, L.; Paust, N.; Karpíšek, M.; Bostanci, N.; Zengerle, R.; Mitsakakis, K. ImmunoDisk—A Fully Automated Bead-Based Immunoassay Cartridge with All Reagents Pre-Stored. Biosensors 2022, 12, 413. [Google Scholar] [CrossRef]
- Johannsen, B.; Mark, D.; Boillat-Blanco, N.; Fresco, A.; Baumgartner, D.; Zengerle, R.; Mitsakakis, K. Rapid Diagnosis of Respiratory Tract Infections Using a Point-of-Care Platform Incorporating a Clinical Decision Support Algorithm. Stud. Health Technol. Inform. 2020, 273, 234–239. [Google Scholar]
- Schuijt, T.J.; Boss, D.S.; Musson, R.E.A.; Demir, A.Y. Influence of point-of-care C-reactive protein testing on antibiotic prescription habits in primary care in the Netherlands. Fam. Pract. 2018, 35, 179–185. [Google Scholar] [CrossRef]
- apDia In Vitro Diagnostic Kit—CRP ELISA Manual. Available online: https://apdiagroup.com/wp-content/uploads/2022/07/740001-IFU-CRP-96T-vs06-2022.pdf (accessed on 10 October 2023).
- Diasys CRP FS Immunoturbidimetric Test to Determine C-Reactive Protein (CRP) in Serum and Plasma. Available online: https://www.diasys-diagnostics.com/products/reagents/immunoturbidimetry/reagent-details/7-crp-fs/reagent.show (accessed on 10 October 2023).
- The Thermo Konelab 60I Chemistry Analyzer, Provided by Thermo Fisher Scientific. Available online: https://www.diamonddiagnostics.com/products/Thermo-Konelab-60I-Chemistry-Analyzer_0-TM-KONELAB60I (accessed on 10 October 2023).
- Diasys Calibrators: TruCal CRP: Liquid-Stable Calibrator Set For Use with CRP FS. Available online: https://www.diasys-diagnostics.com/products/calibratorscontrols/calibrators/product-details/24-trucal-crp/product.show (accessed on 10 October 2023).
- Minnaard, M.C.; van de Pol, A.C.; Broekhuizen, B.D.L.; Verheij, T.J.M.; Hopstaken, R.M.; van Delft, S.; Kooijman-Buiting, A.M.J.; de Groot, J.A.H.; de Wit, N.J. Analytical performance, agreement and user-friendliness of five C-reactive protein point-of-care tests. Scand. J. Clin. Lab. Investig. 2013, 73, 627–634. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Landscape of Diagnostics against Antibacterial Resistance, Gaps and Priorities; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Bio-Rad Datasheet, LiquicheckTM Elevated CRP Control Levels 1, 2 and 3. Available online: https://www.bio-rad.com/de-de/product/liquichek-elevated-crp-control?ID=23baeb40-b1f4-41af-b6fc-8006a2f761b3 (accessed on 10 October 2023).
- Luo, Y.; Pehrsson, M.; Langholm, L.; Karsdal, M.; Bay-Jensen, A.-C.; Sun, S. Lot-to-Lot Variance in Immunoassays—Causes, Consequences, and Solutions. Diagnostics 2023, 13, 1835. [Google Scholar] [CrossRef] [PubMed]
- Masetto, T.; Eidizadeh, A.; Peter, C.; Grimmler, M. National external quality assessment and direct method comparison reflect crucial deviations of Procalcitonin measurements in Germany. Clin. Chim. Acta 2022, 529, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Warnken, T.; Huber, K.; Feige, K. Comparison of three different methods for the quantification of equine insulin. BMC Vet. Res. 2016, 12, 196. [Google Scholar] [CrossRef] [PubMed]
- Jukic, T.; Drobne, D.; Pusavec, S.; Ihan, A.; Stubljar, D.; Starc, A. Comparison of 3 Enzyme-Linked Immunoassay Methods to Evaluate Serum Concentrations of Infliximab and Antibodies to Infliximab in 32 Patients with Moderate to Severe Inflammatory Bowel Disease. Med. Sci. Monit. 2023, 29, e939084. [Google Scholar] [CrossRef]
- Liew, M.; Groll, M.C.; Thompson, J.E.; Call, S.L.; Moser, J.E.; Hoopes, J.D. Validating a custom multiplex ELISA against individual commercial immunoassays using clinical samples. BioTechniques 2007, 42, 327–333. [Google Scholar] [CrossRef]
- Technical Note for Maxisop Microtitre Plate (Invitrogen, By Thermo Fisher Scientific). Available online: https://assets.thermofisher.com/TFS-Assets/LSG/manuals/44-2404.pdf (accessed on 10 October 2023).
- Lippi, G.; Blanckaert, N.; Bonini, P.; Green, S.; Kitchen, S.; Palicka, V.; Vassault, A.J.; Plebani, M. Haemolysis: An overview of the leading cause of unsuitable specimens in clinical laboratories. Clin. Chem. Lab. Med. 2008, 46, 764. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Di Somma, S.; Cervellin, G. Hemolyzed specimens: A major challenge for emergency departments and clinical laboratories. Crit. Rev. Clin. Lab. Sci. 2011, 48, 143–153. [Google Scholar] [CrossRef]
- Lippi, G.; Cadamuro, J. Visual assessment of sample quality: Quo usque tandem? Clin. Chem. Lab. Med. 2018, 56, 513–515. [Google Scholar] [CrossRef]
- CRP ELISA, Instructions for Use, Tecan. Available online: https://www.ibl-international.com/media/mageworx/downloads/attachment/file/e/u/eu59131_ifu_eu_en_crp_elisa_2022-06_sym9.pdf (accessed on 10 October 2023).
- Kurian, A.; Neumann, E.J.; Hall, W.F.; Marks, D. Effects of blood sample mishandling on ELISA results for infectious bronchitis virus, avian encephalomyelitis virus and chicken anaemia virus. Vet. J. 2012, 192, 378–381. [Google Scholar] [CrossRef]
- Quality Control Center Switzerland. TECHNISCHES DATENBLATT 31; Hämolysierte, Lipämische, Ikterische Proben. Available online: http://www.cscq.ch/SiteCSCQ/FichierPDF_DE/FT-Haemolysierte-lipaemische-ikterische-Proben.pdf (accessed on 10 October 2023).
- EUR 24922 EN; The Certification of the Mass Concentration of C-Reactive Protein in Human Serum—Certified Reference Material ERM®-DA474/IFCC. Publications Office of the European Union: Luxembourg, 2011.
- Dupuy, A.M.; Bargnoux, A.S.; Larcher, R.; Merindol, A.; Masetto, T.; Badiou, S.; Cristol, J.P. Bioanalytical Performance of a New Particle-Enhanced Method for Measuring Procalcitonin. Diagnostics 2020, 10, 461. [Google Scholar] [CrossRef]
- Lhopitallier, L.; Kronenberg, A.; Meuwly, J.-Y.; Locatelli, I.; Mueller, Y.; Senn, N.; D’Acremont, V.; Boillat-Blanco, N. Procalcitonin and lung ultrasonography point-of-care testing to determine antibiotic prescription in patients with lower respiratory tract infection in primary care: Pragmatic cluster randomised trial. BMJ 2021, 374, n2132. [Google Scholar] [CrossRef] [PubMed]
- Van den Bruel, A.; Thompson, M.J.; Haj-Hassan, T.; Stevens, R.; Moll, H.; Lakhanpaul, M.; Mant, D. Diagnostic value of laboratory tests in identifying serious infections in febrile children: Systematic review. BMJ 2011, 342, d3082. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Schiano Moriello, N.; Hopstaken, R.; Llor, C.; Melbye, H.; Senn, O. The Role of CRP POC Testing in the Fight against Antibiotic Overuse in European Primary Care: Recommendations from a European Expert Panel. Diagnostics 2023, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.; Gelfer, G.; Wang, L.; Myers, J.; Bajema, K.; Johnston, M.; Leggett, J. The potential of molecular diagnostics and serum procalcitonin levels to change the antibiotic management of community-acquired pneumonia. Diagn. Microbiol. Infect. Dis. 2016, 86, 102–107. [Google Scholar] [CrossRef]
- Minnaard, M.C.; de Groot, J.A.H.; Hopstaken, R.M.; Schierenberg, A.; de Wit, N.J.; Reitsma, J.B.; Broekhuizen, B.D.L.; van Vugt, S.F.; Neven, A.K.; Graffelman, A.W.; et al. The added value of C-reactive protein measurement in diagnosing pneumonia in primary care: A meta-analysis of individual patient data. CMAJ 2017, 189, E56–E63. [Google Scholar] [CrossRef]
- Alcoba, G.; Keitel, K.; Maspoli, V.; Lacroix, L.; Manzano, S.; Gehri, M.; Tabin, R.; Gervaix, A.; Galetto-Lacour, A. A three-step diagnosis of pediatric pneumonia at the emergency department using clinical predictors, C-reactive protein, and pneumococcal PCR. Eur. J. Pediatr. 2017, 176, 815–824. [Google Scholar] [CrossRef]
- Nijman, R.G.; Vergouwe, Y.; Moll, H.A.; Smit, F.J.; Weerkamp, F.; Steyerberg, E.W.; van der Lei, J.; de Rijke, Y.B.; Oostenbrink, R. Validation of the Feverkidstool and procalcitonin for detecting serious bacterial infections in febrile children. Pediatr. Res. 2018, 83, 466–476. [Google Scholar] [CrossRef]
- van Houten, C.; van de Maat, J.S.; Naaktgeboren, C.; Bont, L.; Oostenbrink, R. Update of a clinical prediction model for serious bacterial infections in preschool children by adding a host-protein-based assay: A diagnostic study. BMJ Paediatr. Open 2019, 3, e000416. [Google Scholar] [CrossRef]
- Hogendoorn, S.K.L.; Lhopitallier, L.; Richard-Greenblatt, M.; Tenisch, E.; Mbarack, Z.; Samaka, J.; Mlaganile, T.; Mamin, A.; Genton, B.; Kaiser, L.; et al. Clinical sign and biomarker-based algorithm to identify bacterial pneumonia among outpatients with lower respiratory tract infection in Tanzania. BMC Infect. Dis. 2022, 22, 39. [Google Scholar] [CrossRef]
- Pellé, K.G.; Rambaud-Althaus, C.; D’Acremont, V.; Moran, G.; Sampath, R.; Katz, Z.; Moussy, F.G.; Mehl, G.L.; Dittrich, S. Electronic clinical decision support algorithms incorporating point-of-care diagnostic tests in low-resource settings: A target product profile. BMJ Glob. Health 2020, 5, e002067. [Google Scholar] [CrossRef] [PubMed]
- Keitel, K.; Kagoro, F.; Samaka, J.; Masimba, J.; Said, Z.; Temba, H.; Mlaganile, T.; Sangu, W.; Rambaud-Althaus, C.; Gervaix, A. A novel electronic algorithm using host biomarker point-of-care tests for the management of febrile illnesses in Tanzanian children (e-POCT): A randomized, controlled non-inferiority trial. PLoS Med. 2017, 14, e1002411. [Google Scholar] [CrossRef] [PubMed]
- Suttels, V.; Van Singer, M.; Clack, L.C.; Plüss-Suard, C.; Niquille, A.; Mueller, Y.; Boillat Blanco, N. Factors Influencing the Implementation of Antimicrobial Stewardship in Primary Care: A Narrative Review. Antibiotics 2023, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Hays, J.P.; Mitsakakis, K.; Luz, S.; van Belkum, A.; Becker, K.; van den Bruel, A.; Harbarth, S.; Rex, J.H.; Simonsen, G.S.; Werner, G.; et al. The successful uptake and sustainability of rapid infectious disease and antimicrobial resistance point-of-care testing requires a complex ’mix-and-match’ implementation package. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1015–1022. [Google Scholar] [CrossRef]
- Strumann, C.; Steinhaeuser, J.; Emcke, T.; Sonnichsen, A.; Goetz, K. Communication training and the prescribing pattern of antibiotic prescription in primary health care. PLoS ONE 2020, 15, e0233345. [Google Scholar] [CrossRef]
- Rombach, M.; Hin, S.; Specht, M.; Johannsen, B.; Lüddecke, J.; Paust, N.; Zengerle, R.; Roux, L.; Sutcliffe, T.; Peham, J.R.; et al. RespiDisk: A point-of-care platform for fully automated detection of respiratory tract infection pathogens in clinical samples. Analyst 2020, 145, 7040–7047. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Zones between Cutoff Concentrations | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 |
|---|---|---|---|---|
| Zone (A) | ≤20.0 | ≤20.0 | ≤20.0 | ≤20.0 |
| Zone (B) | 20.1–50.0 | 20.1–40.0 | 20.1–60.0 | 20.1–99.9 |
| Zone (C) | 50.1–99.9 | >40.0 | >60.0 | ≥100.0 |
| Zone (D) | ≥100.0 |
| Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | |
|---|---|---|---|---|
| Agreement between ITA and ELISA, considering ITA as the reference of ELISA (average 87.7%) | 46/53 (86.8%) | 49/53 (92.5%) | 45/53 (84.9%) | 46/53 (86.8%) |
| Agreement between BFPD-IA and ELISA, considering ELISA as the reference of BFPD-IA (average 87.3%) | 44/53 (83.0%) | 50/53 (94.3%) | 47/53 (88.7%) | 44/53 (83.0%) |
| Agreement between BFPD-IA and ITA, considering ITA as the reference of BFPD-IA (average 93.9%) | 49/53 (92.5%) | 52/53 (98.1%) | 49/53 (92.5%) | 49/53 (92.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johannsen, B.; Baumgartner, D.; Karpíšek, M.; Stejskal, D.; Boillat-Blanco, N.; Knüsli, J.; Panning, M.; Paust, N.; Zengerle, R.; Mitsakakis, K. Patient Stratification for Antibiotic Prescriptions Based on the Bound-Free Phase Detection Immunoassay of C-Reactive Protein in Serum Samples. Biosensors 2023, 13, 1009. https://doi.org/10.3390/bios13121009
Johannsen B, Baumgartner D, Karpíšek M, Stejskal D, Boillat-Blanco N, Knüsli J, Panning M, Paust N, Zengerle R, Mitsakakis K. Patient Stratification for Antibiotic Prescriptions Based on the Bound-Free Phase Detection Immunoassay of C-Reactive Protein in Serum Samples. Biosensors. 2023; 13(12):1009. https://doi.org/10.3390/bios13121009
Chicago/Turabian StyleJohannsen, Benita, Desirée Baumgartner, Michal Karpíšek, David Stejskal, Noémie Boillat-Blanco, José Knüsli, Marcus Panning, Nils Paust, Roland Zengerle, and Konstantinos Mitsakakis. 2023. "Patient Stratification for Antibiotic Prescriptions Based on the Bound-Free Phase Detection Immunoassay of C-Reactive Protein in Serum Samples" Biosensors 13, no. 12: 1009. https://doi.org/10.3390/bios13121009