Application of a Novel Biosensor for Salivary Conductivity in Detecting Chronic Kidney Disease

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Sensing Device and System
2.1.1. Design of the Biodevice for Measuring Conductivity
2.1.2. The Collection and Analysis of Saliva
2.1.3. Reusability of the Electrode
2.1.4. Selectivity of the Sensor
2.2. Clinical Study Design and Participants
2.3. Procedures of Clinical Study
2.4. Definition of Chronic Kidney Disease
2.5. Statistical Analysis
3. Results
3.1. Reusability of the Sensor
3.2. Selectivity of the Sensor
3.3. Demographic Characteristics of Study Participants
3.4. Association between Salivary Conductivity and Clinical Variables
3.5. The Prevalence of Chronic Kidney Disease (CKD) Increases with Salivary Conductivity
3.6. The Use of Salivary Conductivity to Detect Individuals with CKD
3.7. Characteristics of Low Versus High Salivary Conductivity Population
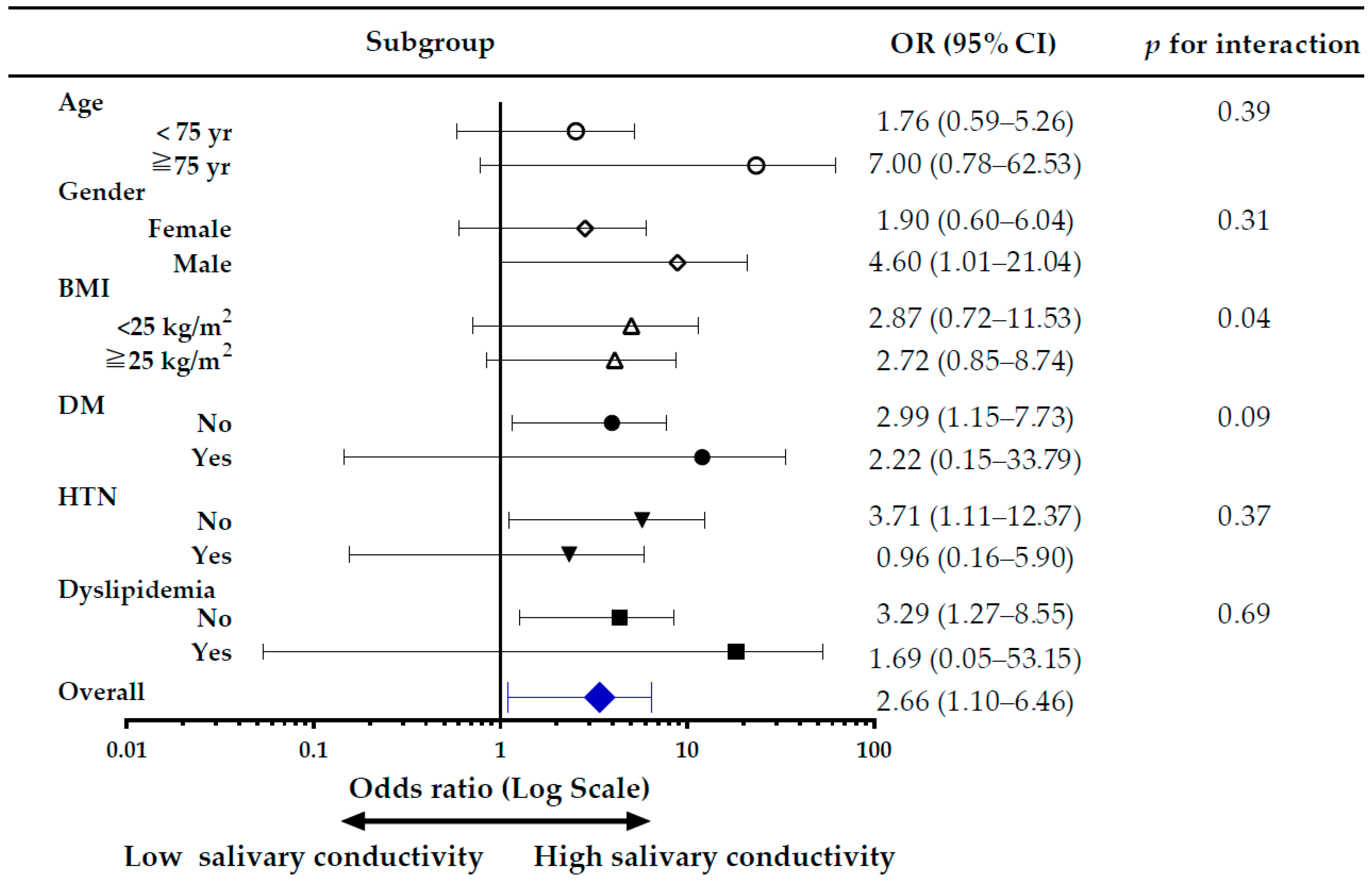
3.8. Subgroup Analysis of the Risk of CKD, Comparing High versus Low Salivary Conductivity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cockwell, P.; Fisher, L.-A. The global burden of chronic kidney disease. Lancet 2020, 395, 662–664. [Google Scholar] [CrossRef] [Green Version]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, C.P.; Cheng, T.Y.D.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462,293 adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar] [CrossRef]
- Chen, T.K.; Knicely, D.H.; Grams, M.E. Chronic Kidney Disease Diagnosis and Management: A Review. JAMA 2019, 322, 1294–1304. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Perlman, R.L.; Finkelstein, F.O.; Liu, L.; Roys, E.; Kiser, M.; Eisele, G.; Burrows-Hudson, S.; Messana, J.M.; Levin, N.; Rajagopalan, S.; et al. Quality of life in chronic kidney disease (CKD): A cross-sectional analysis in the Renal Research Institute-CKD study. Am. J. Kidney Dis. 2005, 45, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Darlington, O.; Dickerson, C.; Evans, M.; McEwan, P.; Sörstadius, E.; Sugrue, D.; van Haalen, H.; Sanchez, J.J.G. Costs and healthcare resource use associated with risk of cardiovascular morbidity in patients with chronic kidney Disease: Evidence from a systematic literature review. Adv. Ther. 2021, 38, 994–1010. [Google Scholar] [CrossRef]
- Plantinga, L.C.; Boulware, L.E.; Coresh, J.; Stevens, L.A.; Miller, E.R., 3rd; Saran, R.; Messer, K.L.; Levey, A.S.; Powe, N.R. Patient awareness of chronic kidney disease: Trends and predictors. Arch. Intern. Med. 2008, 168, 2268–2275. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Kilbride, H.S.; Stevens, P.E.; Eaglestone, G.; Knight, S.; Carter, J.L.; Delaney, M.P.; Farmer, C.K.; Irving, J.; O’Riordan, S.E.; Dalton, R.N.; et al. Accuracy of the MDRD (Modification of Diet in Renal Disease) study and CKD-EPI (CKD Epidemiology Collaboration) equations for estimation of GFR in the elderly. Am. J. Kidney Dis. 2013, 61, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Berns, J.S. Routine screening for CKD should be done in asymptomatic adults… selectively. Clin. J. Am. Soc. Nephrol. 2014, 9, 1988–1992. [Google Scholar] [CrossRef] [PubMed]
- Celec, P.; Tothova, L.; Sebekova, K.; Podracka, L.; Boor, P. Salivary markers of kidney function—Potentials and limitations. Clin. Chim. Acta 2016, 453, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Czumbel, L.M.; Kiss, S.; Farkas, N.; Mandel, I.; Hegyi, A.; Nagy, Á.; Lohinai, Z.; Szakács, Z.; Hegyi, P.; Steward, M.C. Saliva as a candidate for COVID-19 diagnostic testing: A meta-analysis. Front. Med. 2020, 7, 465. [Google Scholar] [CrossRef]
- Gleerup, H.S.; Hasselbalch, S.G.; Simonsen, A.H. Biomarkers for Alzheimer’s disease in saliva: A systematic review. Dis. Markers 2019, 2019, 4761054. [Google Scholar] [CrossRef] [PubMed]
- Hegde, M.N.; Attavar, S.H.; Shetty, N.; Hegde, N.D.; Hegde, N.N. Saliva as a biomarker for dental caries: A systematic review. J. Conserv. Dent. 2019, 22, 2. [Google Scholar]
- Wang, J.; Zhao, Y.; Ren, J.; Xu, Y. Pepsin in saliva as a diagnostic biomarker in laryngopharyngeal reflux: A meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 671–678. [Google Scholar] [CrossRef]
- Chojnowska, S.; Baran, T.; Wilinska, I.; Sienicka, P.; Cabaj-Wiater, I.; Knas, M. Human saliva as a diagnostic material. Adv. Med. Sci. 2018, 63, 185–191. [Google Scholar] [CrossRef]
- Matczuk, J.; Zalewska, A.; Lukaszuk, B.; Knas, M.; Maciejczyk, M.; Garbowska, M.; Ziembicka, D.M.; Waszkiel, D.; Chabowski, A.; Zendzian-Piotrowska, M.; et al. Insulin Resistance and Obesity Affect Lipid Profile in the Salivary Glands. J. Diabetes Res. 2016, 2016, 8163474. [Google Scholar] [CrossRef] [Green Version]
- Kulak-Bejda, A.; Waszkiewicz, N.; Bejda, G.; Zalewska, A.; Maciejczyk, M. Diagnostic Value of Salivary Markers in Neuropsychiatric Disorders. Dis. Markers 2019, 2019, 4360612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Bielas, M.; Zalewska, A.; Gerreth, K. Salivary Biomarkers of Oxidative Stress and Inflammation in Stroke Patients: From Basic Research to Clinical Practice. Oxid. Med. Cell. Longev. 2021, 2021, 5545330. [Google Scholar] [CrossRef]
- Tomas, I.; Marinho, J.S.; Limeres, J.; Santos, M.J.; Araujo, L.; Diz, P. Changes in salivary composition in patients with renal failure. Arch. Oral Biol. 2008, 53, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.D.R.; Hemmila, U.; Mzinganjira, H.; Mtekateka, M.; Banda, E.; Sibale, N.; Kawale, Z.; Phiri, C.; Dreyer, G.; Calice-Silva, V.; et al. Diagnostic performance of a point-of-care saliva urea nitrogen dipstick to screen for kidney disease in low-resource settings where serum creatinine is unavailable. BMJ Glob. Health 2020, 5, e002312. [Google Scholar] [CrossRef] [PubMed]
- Korytowska, N.; Sankowski, B.; Wyczalkowska-Tomasik, A.; Paczek, L.; Wroczynski, P.; Giebultowicz, J. The utility of saliva testing in the estimation of uremic toxin levels in serum. Clin. Chem. Lab. Med. 2018, 57, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; de Andrade Vieira, W.; Siqueira, W.L.; Blumenberg, C.; de Macedo Bernardino, I.; Cardoso, S.V.; Flores-Mir, C.; Paranhos, L.R. Saliva as an alternative to blood in the determination of uremic state in adult patients with chronic kidney disease: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 2203–2217. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Vieira, W.A.; Siqueira, W.L.; Agostini, B.A.; Moffa, E.B.; Paranhos, L.R. Saliva as a tool for monitoring hemodialysis: A systematic review and meta-analysis. Braz. Oral Res. 2020, 35, e016. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.P.; Huang, J.W.; Lee, I.N.; Weng, R.C.; Lin, M.Y.; Yang, J.T.; Lin, C.T. A Portable System to Monitor Saliva Conductivity for Dehydration Diagnosis and Kidney Healthcare. Sci. Rep. 2019, 9, 14771. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Lu, Y.P.; Lee, A.T.; Tung, C.W.; Tsai, Y.H.; Tsay, H.P.; Lin, C.T.; Yang, J.T. A Portable Biodevice to Monitor Salivary Conductivity for the Rapid Assessment of Fluid Status. J. Pers. Med. 2021, 11, 577. [Google Scholar] [CrossRef]
- Lee, A.-T.; Lu, Y.-P.; Chen, C.-H.; Chang, C.-H.; Tsai, Y.-H.; Tung, C.-W.; Yang, J.-T. The Association of Salivary Conductivity with Cardiomegaly in Hemodialysis Patients. Appl. Sci. 2021, 11, 7405. [Google Scholar] [CrossRef]
- Iorgulescu, G. Saliva between normal and pathological. Important factors in determining systemic and oral health. J. Med. Life 2009, 2, 303. [Google Scholar] [PubMed]
- Kuo, Y.-C.; Lee, C.-K.; Lin, C.-T. Improving sensitivity of a miniaturized label-free electrochemical biosensor using zigzag electrodes. Biosens. Bioelectron. 2018, 103, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chang, C. Determination of protein concentration in human saliva. Kaohsiung J. Med. Sci. 1989, 5, 389–397. [Google Scholar]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Manns, B.; Hemmelgarn, B.; Tonelli, M.; Au, F.; So, H.; Weaver, R.; Quinn, A.E.; Klarenbach, S.; Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease. The Cost of Care for People With Chronic Kidney Disease. Can. J. Kidney Health Dis. 2019, 6, 2054358119835521. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.D.; McCulloch, C.E.; Banerjee, T.; Pavkov, M.E.; Burrows, N.R.; Gillespie, B.W.; Saran, R.; Shlipak, M.G.; Powe, N.R.; Tuot, D.S. CKD awareness among US adults by future risk of kidney failure. Am. J. Kidney Dis. 2020, 76, 174–183. [Google Scholar] [CrossRef]
- Xu, F.; Laguna, L.; Sarkar, A. Aging-related changes in quantity and quality of saliva: Where do we stand in our understanding? J. Texture Stud. 2019, 50, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Ashton, N.J.; Ide, M.; Zetterberg, H.; Blennow, K. Salivary Biomarkers for Alzheimer’s Disease and Related Disorders. Neurol. Ther. 2019, 8, 83–94. [Google Scholar] [CrossRef] [Green Version]
- Labat, C.; Thul, S.; Pirault, J.; Temmar, M.; Thornton, S.N.; Benetos, A.; Back, M. Differential Associations for Salivary Sodium, Potassium, Calcium, and Phosphate Levels with Carotid Intima Media Thickness, Heart Rate, and Arterial Stiffness. Dis. Markers 2018, 2018, 3152146. [Google Scholar] [CrossRef]
- Bilancio, G.; Cavallo, P.; Lombardi, C.; Guarino, E.; Cozza, V.; Giordano, F.; Palladino, G.; Cirillo, M. Saliva for assessing creatinine, uric acid, and potassium in nephropathic patients. BMC Nephrol. 2019, 20, 242. [Google Scholar] [CrossRef] [Green Version]
- Jung, D.G.; Jung, D.; Kong, S.H. A Lab-on-a-Chip-Based Non-Invasive Optical Sensor for Measuring Glucose in Saliva. Sensors 2017, 17, 2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 487–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouchi, Y.; Rakugi, H.; Arai, H.; Akishita, M.; Ito, H.; Toba, K.; Kai, I.; Joint Committee of Japan Gerontological Society (JGLS) and Japan Geriatrics Society (JGS) on the Definition and Classification of the Elderly. Redefining the elderly as aged 75 years and older: Proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr. Gerontol. Int. 2017, 17, 1045–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallappallil, M.; Friedman, E.A.; Delano, B.G.; McFarlane, S.I.; Salifu, M.O. Chronic kidney disease in the elderly: Evaluation and management. Clin. Pract. 2014, 11, 525–535. [Google Scholar] [CrossRef] [Green Version]
- Nitta, K.; Okada, K.; Yanai, M.; Takahashi, S. Aging and chronic kidney disease. Kidney Blood Press. Res. 2013, 38, 109–120. [Google Scholar] [CrossRef]
- Anderson, S.; Halter, J.B.; Hazzard, W.R.; Himmelfarb, J.; Horne, F.M.; Kaysen, G.A.; Kusek, J.W.; Nayfield, S.G.; Schmader, K.; Tian, Y.; et al. Prediction, progression, and outcomes of chronic kidney disease in older adults. J. Am. Soc. Nephrol. 2009, 20, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Prakash, S.; O’Hare, A.M. Interaction of aging and chronic kidney disease. Semin. Nephrol. 2009, 29, 497–503. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (N = 214) | Pearson r | p Value for r | |
|---|---|---|---|
| Salivary conductivity, ms/cm | 5.91 ± 1.79 | ||
| Demographics | |||
| Age, years | 63.96 ± 13.53 | 0.362 | <0.01 |
| Gender (male), n (%) | 71 (33.2) | ||
| Body weight, kg | 63.08 ± 10.79 | 0.049 | 0.48 |
| Body height, cm | 158.97 ± 7.67 | 0.037 | 0.59 |
| Body mass index, kg/m2 | 24.90 ± 3.36 | 0.027 | 0.69 |
| Systolic blood pressure, mmHg | 131.26 ± 20.74 | 0.193 | <0.01 |
| Diastolic blood pressure, mmHg | 75.24 ± 11.79 | 0.046 | 0.50 |
| Comorbid conditions, n (%) @ | |||
| Diabetes mellitus | 26 (12.1) | ||
| Hypertension | 62 (29.0) | ||
| Chronic kidney disease | 3 (1.4) | ||
| Ischemic heart disease/stroke | 16 (7.5) | ||
| Dyslipidemia | 30 (14.0) | ||
| Gout | 9 (4.2) | ||
| Chronic liver disease | 24 (11.2) | ||
| Laboratory parameters | |||
| BUN, mg/dL | 15.26 ± 5.28 | 0.178 | <0.01 |
| Creatinine, mg/dL | 0.81 ± 0.26 | 0.251 | <0.01 |
| eGFR, mL/min/1.73 m2 | 86.33 ± 22.81 | −0.323 | <0.01 |
| Serum osmolality, mOsm/kgH2O | 287.69 ± 5.48 | 0.106 | 0.12 |
| Fasting glucose, mg/dL | 103.09 ± 25.31 | 0.153 | 0.03 |
| Hemoglobin A1c, % | 5.89 ± 0.98 | 0.045 | 0.51 |
| ALT, U/L | 22.10 ± 20.91 | 0.027 | 0.70 |
| Triglyceride, mg/dL | 113.19 ± 74.33 | 0.105 | 0.13 |
| Total cholesterol, mg/dL | 198.86 ± 39.48 | −0.056 | 0.41 |
| LDL-C, mg/dL | 120.77 ± 33.63 | −0.066 | 0.33 |
| HDL-C, mg/dL | 55.56 ± 13.22 | −0111 | 0.11 |
| Model 1 | Unstandardized Coefficients β (Standard Error) | Standardized β | p Value |
| Constant | 3.974 (1.062) | <0.001 | |
| Age | 0.035 (0.010) | 0.264 | <0.001 |
| Fasting glucose | 0.009 (0.004) | 0.132 | 0.037 |
| eGFR | −0.015 (0.006) | −0.186 | 0.010 |
| R2 = 0.176 | |||
| Model 2 | Unstandardized Coefficients β (Standard Error) | Standardized β | p Value |
| Constant | 1.452 (0.724) | 0.046 | |
| Age | 0.040 (0.009) | 0.306 | <0.001 |
| Fasting glucose | 0.010 (0.004) | 0.141 | 0.026 |
| Creatinine | 1.043 (0.459) | 0.151 | 0.024 |
| R2 = 0.170 | |||
| Low Salivary Conductivity Group * (N = 140) | High Salivary Conductivity Group (N = 74) | p Value | |
|---|---|---|---|
| Salivary conductivity, ms/cm | 4.84 ± 1.01 | 7.94 ± 1.02 | <0.01 # |
| Demographics | |||
| Age, years | 60.81 ± 13.75 | 69.92 ± 10.93 | <0.01 # |
| Gender (male), n (%) | 42 (30.0) | 29 (39.2) | 0.17 |
| Body weight, kg | 62.94 ± 10.60 | 63.35 ± 11.21 | 0.94 |
| Body height, cm | 159.08 ± 7.39 | 158.76 ± 8.24 | 0.45 |
| Body mass index, kg/m2 | 24.82 ± 3.34 | 25.07 ± 3.40 | 0.61 |
| Systolic blood pressure, mmHg | 128.93 ± 19.78 | 135.68 ± 21.91 | 0.02 # |
| Diastolic blood pressure, mmHg | 74.76 ± 11.60 | 76.14 ± 12.16 | 0.42 |
| Comorbid conditions, n (%) @ | |||
| Diabetes mellitus | 11 (7.9) | 15 (20.5) | <0.01 # |
| Hypertension | 36 (25.7) | 26 (35.6) | 0.13 |
| Chronic kidney disease | 1 (0.7) | 2 (2.7) | 0.27 |
| Ischemic heart disease/Stroke | 7 (5.0) | 9 (12.3) | 0.05 |
| Dyslipidemia | 20 (14.3) | 10 (13.7) | 0.91 |
| Gout | 4 (2.9) | 5 (6.8) | 0.17 |
| Chronic liver disease | 16 (11.4) | 8 (11.0) | 0.92 |
| Laboratory parameters | |||
| BUN, mg/dL | 14.34 ± 4.77 | 16.97 ± 5.78 | <0.01 # |
| Creatinine, mg/dL | 0.76 ± 0.22 | 0.90 ± 0.30 | <0.01 # |
| eGFR, mL/min/1.73 m2 | 91.18 ± 22.17 | 77.17 ± 21.27 | <0.01 # |
| Serum osmolality, mOsm/kgH2O | 287.16 ± 5.04 | 288.69 ± 6.15 | 0.05 # |
| Fasting glucose, mg/dL | 100.41 ± 27.27 | 108.16 ± 20.34 | <0.01 # |
| Hemoglobin A1c, % | 5.85 ± 1.05 | 5.97 ± 0.83 | 0.03 # |
| ALT, U/L | 22.89 ± 24.87 | 20.62 ± 9.74 | 0.69 |
| Triglyceride, mg/dL | 107.50 ± 62.19 | 123.95 ± 92.62 | 0.10 |
| Total cholesterol, mg/dL | 198.18 ± 36.15 | 200.15 ± 45.37 | 0.73 |
| LDL-C, mg/dL | 120.09 ± 30.79 | 122.05 ± 38.65 | 0.69 |
| HDL-C, mg/dL | 56.46 ± 12.81 | 53.84 ± 13.89 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-W.; Tsai, Y.-H.; Lu, Y.-P.; Yang, J.-T.; Chen, M.-Y.; Huang, T.-J.; Weng, R.-C.; Tung, C.-W. Application of a Novel Biosensor for Salivary Conductivity in Detecting Chronic Kidney Disease. Biosensors 2022, 12, 178. https://doi.org/10.3390/bios12030178
Lin C-W, Tsai Y-H, Lu Y-P, Yang J-T, Chen M-Y, Huang T-J, Weng R-C, Tung C-W. Application of a Novel Biosensor for Salivary Conductivity in Detecting Chronic Kidney Disease. Biosensors. 2022; 12(3):178. https://doi.org/10.3390/bios12030178
Chicago/Turabian StyleLin, Chen-Wei, Yuan-Hsiung Tsai, Yen-Pei Lu, Jen-Tsung Yang, Mei-Yen Chen, Tung-Jung Huang, Rui-Cian Weng, and Chun-Wu Tung. 2022. "Application of a Novel Biosensor for Salivary Conductivity in Detecting Chronic Kidney Disease" Biosensors 12, no. 3: 178. https://doi.org/10.3390/bios12030178