Quantification Analysis of Sleep Based on Smartwatch Sensors for Parkinson’s Disease

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
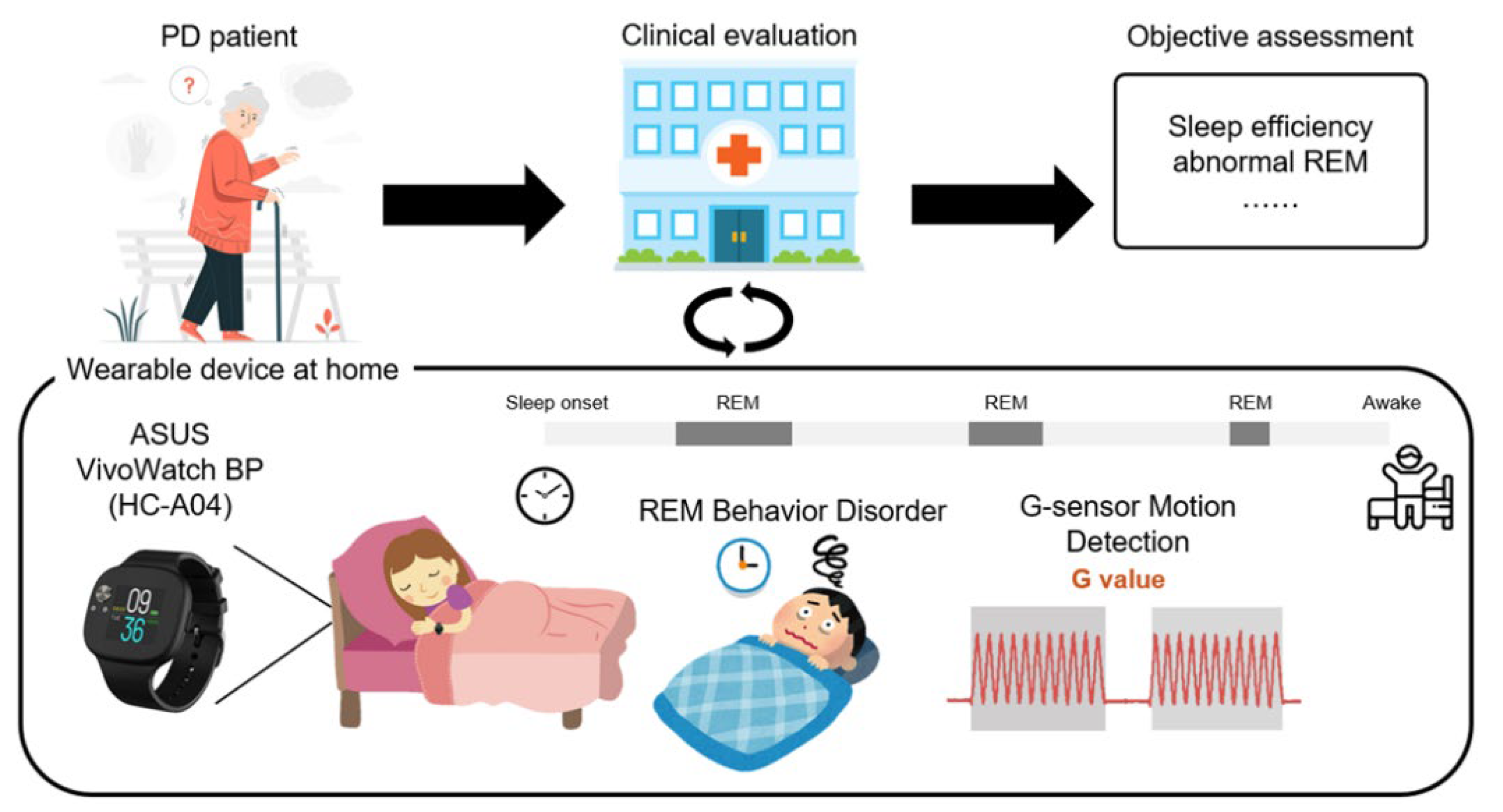
2.1. An Intelligent Wearable Device for Objective Assessment of Sleep in PD Patients
2.2. Data Acquisition and Clinical Trial Design
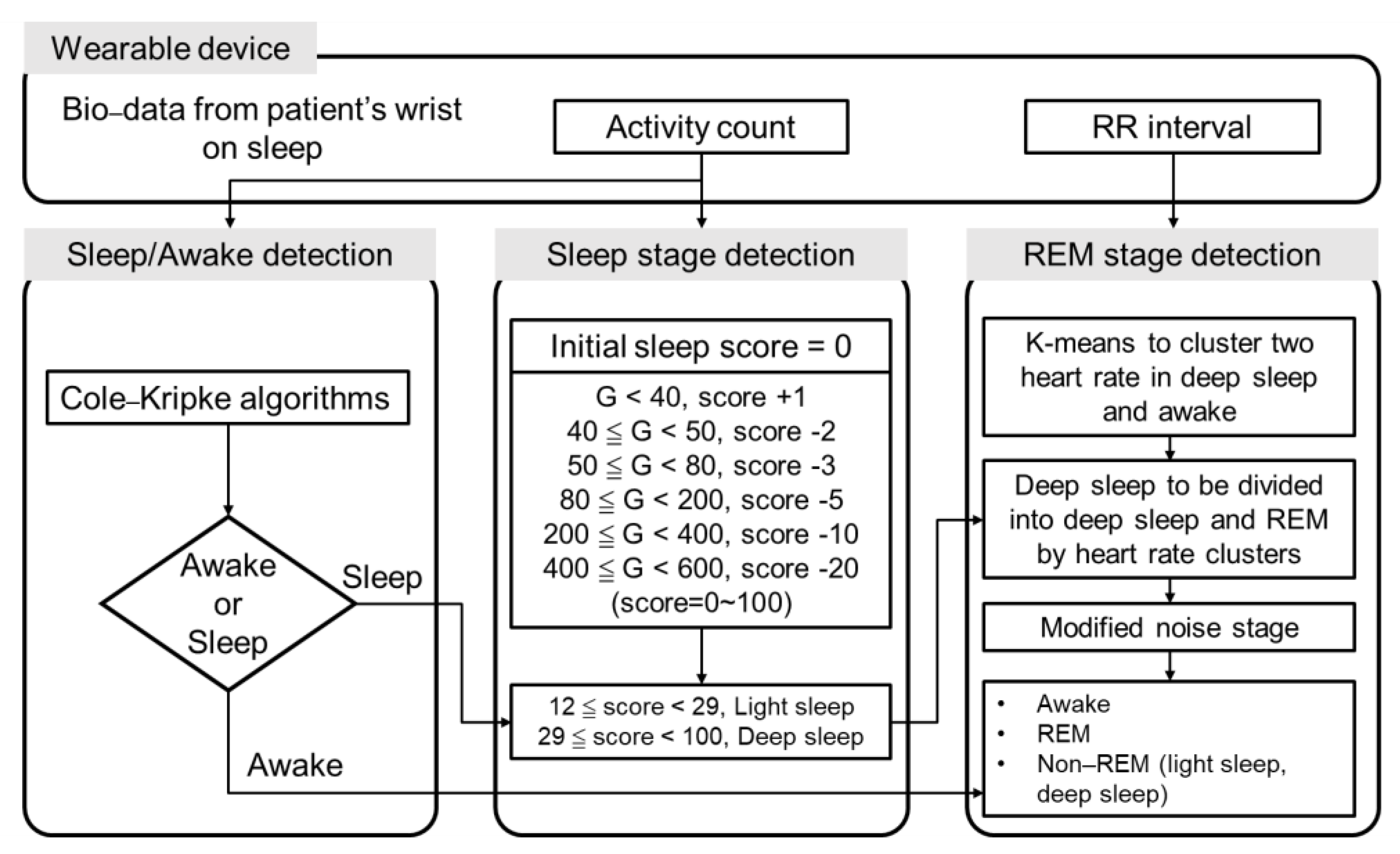
2.3. Design of the Algorithm for Sleep Stage Classification
2.4. Validation Procedure of Sleep-Stage Detection
- (1)
- The first 45 min after sleep onset, as defined by the sleep-stage classification algorithm, was considered a non-REM period;
- (2)
- Separated REM segments of less than 5 min were considered non-REM periods;
- (3)
- Epochs of 3 min or less of non-REM in between two periods of REM stages were considered as REM and could overrule the sleep-stage classification algorithm.
2.5. Statistical Analysis
3. Results
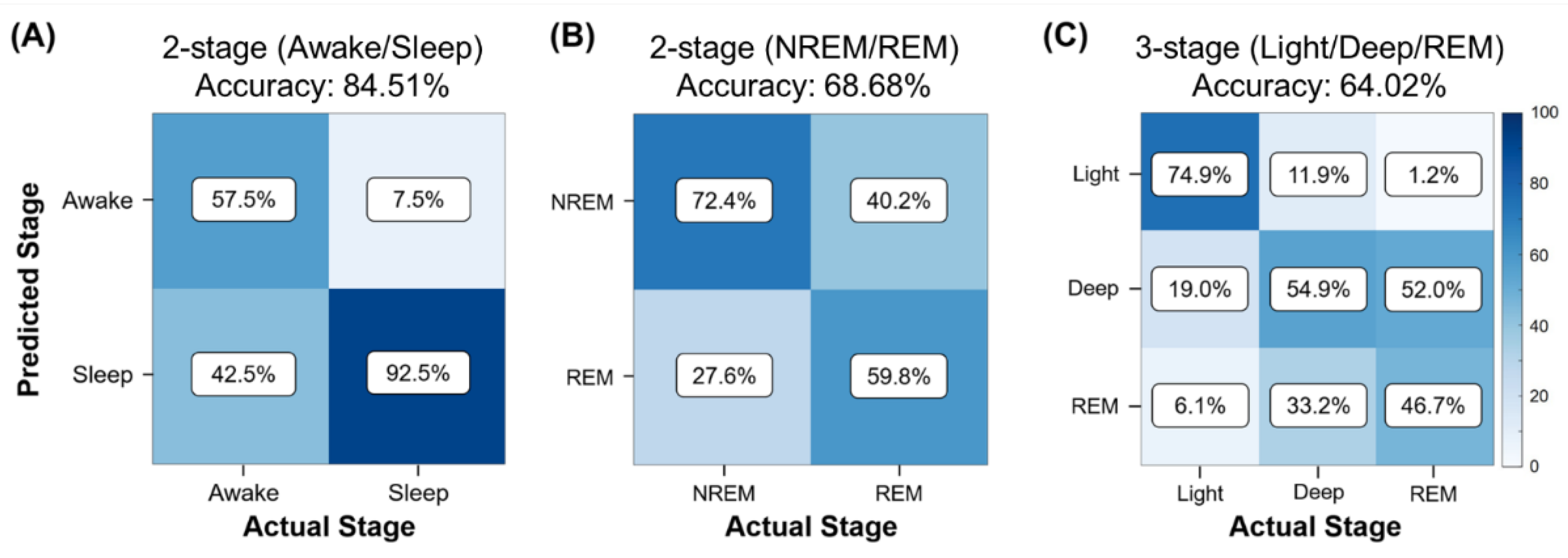
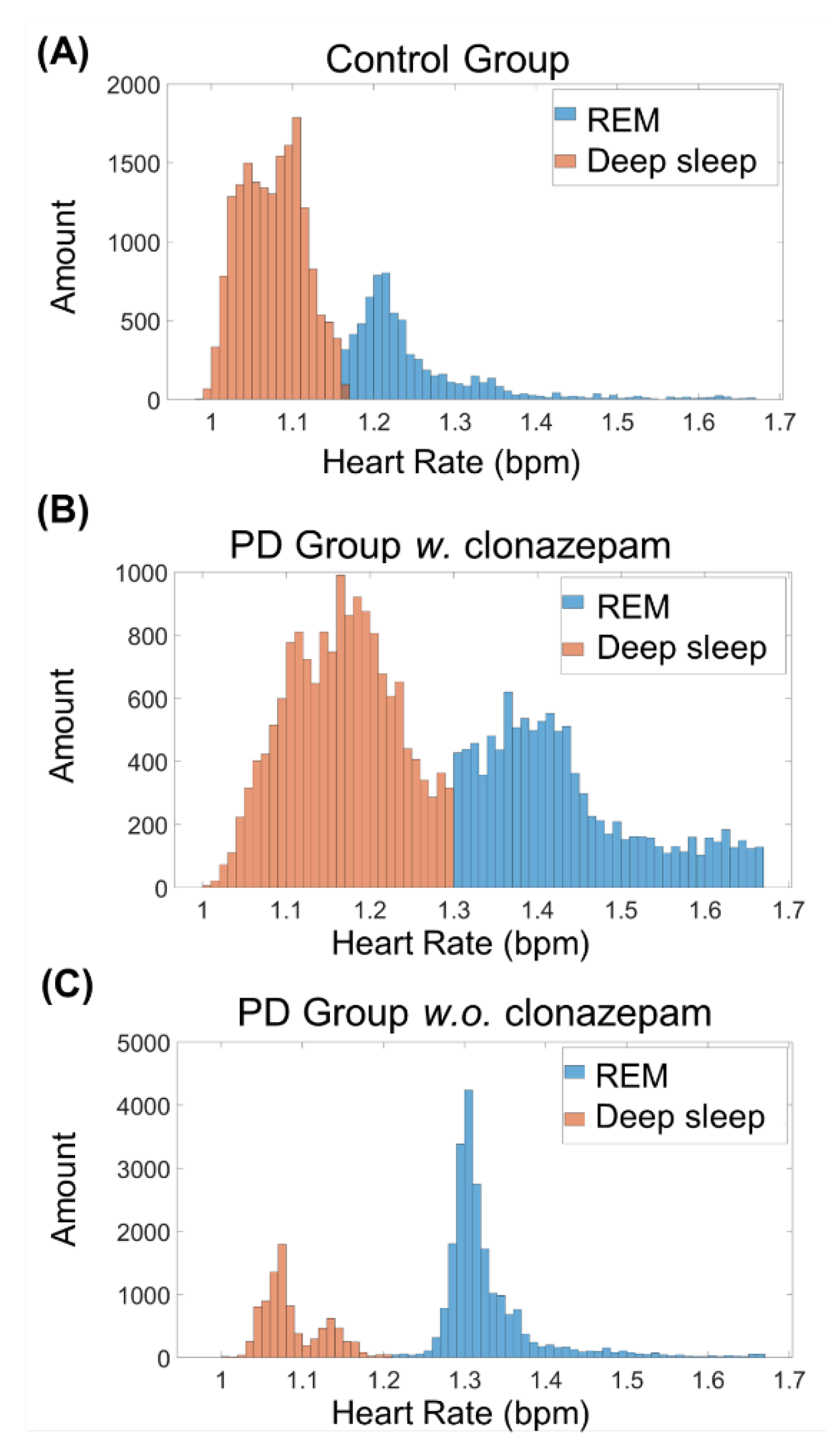
3.1. Personalized Sleep Detection Algorithm for Rapid Eye Movement (REM) Stages
- (1)
- Two-stage sleep–awake detection (awake, sleep);
- (2)
- Two-stage sleep-stage detection (REM sleep, NREM sleep);
- (3)
- Three-stage sleep-stage detection (light sleep, deep sleep, and REM sleep).
3.2. Correlation between Clinical Data and Sleep Algorithm Results
3.3. Statistical Analysis Results
4. Discussion
4.1. Personalized Sleep Detection Algorithm for the REM Stages
4.2. Correlation between Clinical Data and Sleep Algorithm Results
4.3. Statistical Analysis Results
5. Conclusions
6. Limitations of the Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Diaconu, S.; Falup-Pecurariu, O.; Tint, D.; Falup-Pecurariu, C. REM sleep behaviour disorder in Parkinson’s disease (Review). Exp. Med. 2021, 22, 812. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- DeMaagd, G.; Philip, A. Parkinson’s Disease and Its Management: Part 1: Disease Entity, Risk Factors, Pathophysiology, Clinical Presentation, and Diagnosis. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Lubomski, M.; Davis, R.L.; Sue, C.M. Health-Related Quality of Life for Parkinson’s Disease Patients and Their Caregivers. J. Mov. Disord. 2021, 14, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, A.A.; Chakravarthy, S.; Phillips, J.R.; Gupta, A.; Keri, S.; Polner, B.; Frank, M.J.; Jahanshahi, M. Motor symptoms in Parkinson’s disease: A unified framework. Neurosci. Biobehav. Rev. 2016, 68, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Chaudhuri, K.R.; Odin, P.; Antonini, A.; Martinez-Martin, P. Parkinson’s disease: The non-motor issues. Parkinsonism Relat. Disord. 2011, 17, 717–723. [Google Scholar] [CrossRef]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22 (Suppl. S1), S119–S122. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Saricaoglu, M.; Yilmaz, N.H.; Ozer, F.F.; Hanoglu, L. The correlation of non-motor symptoms and sleep on balance in Parkinson’s disease patients with normal cognition and mild cognitive impairment. Ir. J. Med. Sci. 2021, 190, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- El-Manzalawy, Y.; Buxton, O.; Honavar, V. Sleep/wake state prediction and sleep parameter estimation using unsupervised classification via clustering. In Proceedings of the 2017 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Kansas City, MO, USA, 13–16 November 2017; pp. 718–723. [Google Scholar]
- Zahed, H.; Zuzuarregui, J.R.P.; Gilron, R.; Denison, T.; Starr, P.A.; Little, S. The Neurophysiology of Sleep in Parkinson’s Disease. Mov. Disord. 2021, 36, 1526–1542. [Google Scholar] [CrossRef]
- Olanow, C.W.; Schapira, A.H.; Roth, T. Waking up to sleep episodes in Parkinson’s disease. Mov. Disord. 2000, 15, 212–215. [Google Scholar] [CrossRef]
- Xu, Z.; Anderson, K.N.; Saffari, S.E.; Lawson, R.A.; Chaudhuri, K.R.; Brooks, D.; Pavese, N. Progression of sleep disturbances in Parkinson’s disease: A 5-year longitudinal study. J. Neurol. 2021, 268, 312–320. [Google Scholar] [CrossRef]
- Stefani, A.; Hogl, B. Sleep in Parkinson’s disease. Neuropsychopharmacology 2020, 45, 121–128. [Google Scholar] [CrossRef]
- Pacheco, A.D.; Estrella, J.M. Sleep quality, REM sleep behavior disorder and daytime sleepiness in adults with and without Parkinson’s. Arch. De Neurosci. 2021, 26, 20–25. [Google Scholar] [CrossRef]
- Chen, H.; Zhao, E.J.; Zhang, W.; Lu, Y.; Liu, R.; Huang, X.; Ciesielski-Jones, A.J.; Justice, M.A.; Cousins, D.S.; Peddada, S. Meta-analyses on prevalence of selected Parkinson’s nonmotor symptoms before and after diagnosis. Transl. Neurodegener. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Sun, X.; Wang, J.; Tang, L.; Xie, A. Prevalence of rapid eye movement sleep behavior disorder (RBD) in Parkinson’s disease: A meta and meta-regression analysis. Neurol. Sci. 2017, 38, 163–170. [Google Scholar] [CrossRef]
- Sixel-Doring, F.; Trautmann, E.; Mollenhauer, B.; Trenkwalder, C. Associated factors for REM sleep behavior disorder in Parkinson disease. Neurology 2011, 77, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Zoccolella, S.; Savarese, M.; Lamberti, P.; Manni, R.; Pacchetti, C.; Logroscino, G. Sleep disorders and the natural history of Parkinson’s disease: The contribution of epidemiological studies. Sleep Med. Rev. 2011, 15, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Mahale, R.; Yadav, R.; Pal, P.K. Quality of sleep in young onset Parkinson’s disease: Any difference from older onset Parkinson’s disease. Parkinsonism Relat. Disord. 2015, 21, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Chahine, L.M.; Daley, J.; Horn, S.; Colcher, A.; Hurtig, H.; Cantor, C.; Dahodwala, N. Questionnaire-based diagnosis of REM sleep behavior disorder in Parkinson’s disease. Mov. Disord. 2013, 28, 1146–1149. [Google Scholar] [CrossRef]
- Chokroverty, S. Overview of sleep & sleep disorders. Indian J. Med. Res. 2010, 131, 126–140. [Google Scholar]
- Bugalho, P.; Ladeira, F.; Barbosa, R.; Marto, J.P.; Borbinha, C.; da Conceicao, L.; Salavisa, M.; Saraiva, M.; Meira, B.; Fernandes, M. Polysomnographic predictors of sleep, motor and cognitive dysfunction progression in Parkinson’s disease: A longitudinal study. Sleep Med. 2021, 77, 205–208. [Google Scholar] [CrossRef]
- Eisensehr, I.; v Lindeiner, H.; Jager, M.; Noachtar, S. REM sleep behavior disorder in sleep-disordered patients with versus without Parkinson’s disease: Is there a need for polysomnography? J. Neurol. Sci. 2001, 186, 7–11. [Google Scholar] [CrossRef]
- Liu, J.; Zhao, Y.; Lai, B.; Wang, H.; Tsui, K.L. Wearable Device Heart Rate and Activity Data in an Unsupervised Approach to Personalized Sleep Monitoring: Algorithm Validation. JMIR Mhealth Uhealth 2020, 8, e18370. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s disease: Challenges and opportunities. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Ferro, A.; Elshehabi, M.; Godinho, C.; Salkovic, D.; Hobert, M.A.; Domingos, J.; van Uem, J.M.; Ferreira, J.J.; Maetzler, W. New methods for the assessment of Parkinson’s disease (2005 to 2015): A systematic review. Mov. Disord. 2016, 31, 1283–1292. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Baig, F.; Lo, C.; Barber, T.R.; Lawton, M.A.; Zhan, A.; Rolinski, M.; Ruffmann, C.; Klein, J.C.; Rumbold, J.; et al. Smartphone motor testing to distinguish idiopathic REM sleep behavior disorder, controls, and PD. Neurology 2018, 91, e1528–e1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merola, A.; Sturchio, A.; Hacker, S.; Serna, S.; Vizcarra, J.A.; Marsili, L.; Fasano, A.; Espay, A.J. Technology-based assessment of motor and nonmotor phenomena in Parkinson disease. Expert Rev. Neurother. 2018, 18, 825–845. [Google Scholar] [CrossRef] [PubMed]
- Palotti, J.; Mall, R.; Aupetit, M.; Rueschman, M.; Singh, M.; Sathyanarayana, A.; Taheri, S.; Fernandez-Luque, L. Benchmark on a large cohort for sleep-wake classification with machine learning techniques. NPJ Digit. Med. 2019, 2, 50. [Google Scholar] [CrossRef] [Green Version]
- Gunes, S.; Polat, K.; Yosunkaya, S. Efficient sleep stage recognition system based on EEG signal using k-means clustering based feature weighting. Expert Syst. Appl. 2010, 37, 7922–7928. [Google Scholar] [CrossRef]
- Walch, O.; Huang, Y.; Forger, D.; Goldstein, C. Sleep stage prediction with raw acceleration and photoplethysmography heart rate data derived from a consumer wearable device. Sleep 2019, 42, zsz180. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [Green Version]
- Alatriste-Booth, V.; Rodriguez-Violante, M.; Camacho-Ordonez, A.; Cervantes-Arriaga, A. Prevalence and correlates of sleep disorders in Parkinson’s disease: A polysomnographic study. Arq. Neuropsiquiatr. 2015, 73, 241–245. [Google Scholar] [CrossRef]
- Guillodo, E.; Lemey, C.; Simonnet, M.; Walter, M.; Baca-Garcia, E.; Masetti, V.; Moga, S.; Larsen, M.; Network, H.; Ropars, J.; et al. Clinical Applications of Mobile Health Wearable-Based Sleep Monitoring: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e10733. [Google Scholar] [CrossRef]
- Maglione, J.E.; Liu, L.; Neikrug, A.B.; Poon, T.; Natarajan, L.; Calderon, J.; Avanzino, J.A.; Corey-Bloom, J.; Palmer, B.W.; Loredo, J.S.; et al. Actigraphy for the assessment of sleep measures in Parkinson’s disease. Sleep 2013, 36, 1209–1217. [Google Scholar] [CrossRef] [Green Version]
- Busek, P.; Vankova, J.; Opavsky, J.; Salinger, J.; Nevsimalova, S. Spectral analysis of the heart rate variability in sleep. Physiol. Res. 2005, 54, 369–376. [Google Scholar] [PubMed]
- Mendez, M.; Bianchi, A.M.; Villantieri, O.; Cerutti, S. Time-varying analysis of the heart rate variability during REM and non REM sleep stages. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 2006, 3576–3579. [Google Scholar] [CrossRef] [PubMed]
- Berlad, I.I.; Shlitner, A.; Ben-Haim, S.; Lavie, P. Power spectrum analysis and heart rate variability in Stage 4 and REM sleep: Evidence for state-specific changes in autonomic dominance. J. Sleep Res. 1993, 2, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Salsone, M.; Vescio, B.; Fratto, A.; Sturniolo, M.; Arabia, G.; Gambardella, A.; Quattrone, A. Cardiac sympathetic index identifies patients with Parkinson’s disease and REM behavior disorder. Parkinsonism Relat. Disord. 2016, 26, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.L.; Mehlsen, J.; Jennum, P. Reduced sympathetic activity in idiopathic rapid-eye-movement sleep behavior disorder and Parkinson’s disease. Auton Neurosci. 2013, 179, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Arnao, V.; Cinturino, A.; Mastrilli, S.; Butta, C.; Maida, C.; Tuttolomondo, A.; Aridon, P.; D’Amelio, M. Impaired circadian heart rate variability in Parkinson’s disease: A time-domain analysis in ambulatory setting. BMC Neurol. 2020, 20, 152. [Google Scholar] [CrossRef] [PubMed]
- Iakovakis, D.; Mastoras, R.E.; Hadjidimitriou, S.; Charisis, V.; Bostanjopoulou, S.; Katsarou, Z.; Klingelhoefer, L.; Reichmann, H.; Trivedi, D.; Chaudhuri, R.K.; et al. Smartwatch-based Activity Analysis During Sleep for Early Parkinson’s Disease Detection. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 4326–4329. [Google Scholar] [CrossRef]
- Gupta, R.; Goel, D.; Walker, J.; Farney, R.J. REM sleep behavior disorder in Parkinson’s disease: A case from India confirmed with polysomnographic data. J. Neurosci. Rural. Pr. 2013, 4, S91–S94. [Google Scholar] [CrossRef]
- Nomura, T.; Inoue, Y.; Kagimura, T.; Nakashima, K. Clinical significance of REM sleep behavior disorder in Parkinson’s disease. Sleep Med. 2013, 14, 131–135. [Google Scholar] [CrossRef]
- Sauvageot, N.; Vaillant, M.; Diederich, N.J. Reduced sympathetically driven heart rate variability during sleep in Parkinson’s disease: A case-control polysomnography-based study. Mov. Disord. 2011, 26, 234–240. [Google Scholar] [CrossRef]
- Breen, D.P.; Vuono, R.; Nawarathna, U.; Fisher, K.; Shneerson, J.M.; Reddy, A.B.; Barker, R.A. Sleep and circadian rhythm regulation in early Parkinson disease. JAMA Neurol. 2014, 71, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, S.J.; Imbach, L.L.; Valko, P.O.; Maric, A.; Maqkaj, R.; Werth, E.; Baumann, C.R.; Baumann-Vogel, H. Reduced Regional NREM Sleep Slow-Wave Activity Is Associated With Cognitive Impairment in Parkinson Disease. Front. Neurol. 2021, 12, 156. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Y.; Liu, W.Y.; Kang, W.Y.; Yang, Q.; Wang, X.Y.; Ding, J.Q.; Chen, S.D.; Liu, J. Association of rapid eye movement sleep behavior disorder with sleep-disordered breathing in Parkinson’s disease. Sleep Med. 2016, 20, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Niu, L.; Liu, X.; Liu, Y.; Li, S.; Yu, H.; Le, W. Rapid Eye Movement Sleep Behavior Disorder and Neurodegenerative Diseases: An Update. Aging Dis. 2020, 11, 315–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeve, B.F. REM sleep behavior disorder: Updated review of the core features, the REM sleep behavior disorder-neurodegenerative disease association, evolving concepts, controversies, and future directions. Ann. N. Y. Acad. Sci 2010, 1184, 15–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Control Group (n = 30) | PD Group (n = 27) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 61.7 ± 9.2 | 62.3 ± 9.51 | 0.36 |
| Sex (male/female) | 15/15 | 14/13 | |
| PSQI 1 | 6.66 ± 3.6 | 10.6 ± 5.4 | 0.001 ** |
| Start sleep (hh:ss) | 22:50 ±66.8 | 21:52 ± 65.2 | 0.112 |
| End sleep (hh:ss) | 05:36 ± 64.2 | 05:47 ± 91.1 | 0.585 |
| Sleep time (min) | 364.6 ± 66.2 | 373.3 ± 120.6 | 0.371 |
| Bedtime (min) | 434 ± 78.5 | 477.7 ± 82.3 | 0.022 * |
| Sleep efficiency (%) | 85.1 ± 13.4 | 82.25 ± 29.3 | 0.623 |
| Subject | Control Group (n = 30) | PD Group w. Clonazepam (n = 12) | PD Group w.o. Clonazepam (n = 15) | p-Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Age (years) | 61.7 ± 9.2 | 62.5 ± 11.52 | 62.2 ± 8.0 | 0.93 |
| Sex (male/female) | 15/15 | 6/6 | 8/7 | |
| PSQI 1 | 6.66 ± 3.6 | 9.6 ± 5.1 | 11.4 ± 5.7 | 0.006 ** |
| Start sleep (hh:ss) | 22:50 ±66.8 | 21:43 ± 35.5 | 21:53 ± 82.1 | 0.220 |
| End sleep (hh:ss) | 05:36 ± 64.2 | 05:40 ± 70.5 | 05:42 ± 106.7 | 0.792 |
| Sleep time (min) | 364.6 ± 66.2 | 417.5 ± 105.8 | 338 ± 123.4 | 0.090 |
| Bedtime (min) | 434 ± 78.5 | 486.6 ± 65.9 | 470.6 ± 95.2 | 0.120 |
| Sleep efficiency (%) | 85.1 ± 13.4 | 86.5 ± 20.9 | 77 ± 34.8 | 0.445 |
| Equation (6) Method | Equation (7) Method | Equation (8) Method | |
|---|---|---|---|
| G-value range | 0.19–99.51 | 0.26–131.51 | 32.20–300 |
| Accuracy | 68.83% | 74.26% | 90.86% |
| Total Sleep Time (min) | MAE (MAPE) | RMSE | Spearman’s Correlation | p-Value |
| 83.5 (16.49%) | 106 min | 0.70 | 0.001 ** |
| G-Value Threshold | Median (Control/PD) | Mann–Whitney U Statistic | T-Value | p-Value |
|---|---|---|---|---|
| 4500 | 0/0 | 391.5 | 769.5000 | 0.3610 |
| 4200 | 0/0 | 387 | 801.0000 | 0.5682 |
| 3900 | 0/0 | 396 | 774.0000 | 0.8112 |
| 3600 | 0/0 | 350 | 838.0000 | 0.3065 |
| 3300 | 15/30 | 299 | 889.0000 | 0.0744 |
| 3000 | 30/60 | 281 | 907.0000 | 0.0427 |
| 2700 | 60/90 | 302 | 886.0000 | 0.0963 |
| 2400 | 90/15 | 264 | 924.0000 | 0.0240 |
| 2100 | 120/670 | 264.5 | 923.5000 | 0.0248 |
| 1800 | 195/360 | 254.5 | 933.5000 | 0.0162 |
| 1500 | 240/690 | 247 | 941.0000 | 0.0117 * |
| 1200 | 495/1200 | 248.5 | 939.5000 | 0.0126 |
| Subject | Control Group (n = 18) | PD Group (n = 20) | p-Value |
|---|---|---|---|
| Mean ± SD (Minimum–Maximum) | Mean ± SD (Minimum–Maximum) | ||
| Light sleep (N1 + N2) (%) | 25.7 ± 21.3 (3.0–79.4) | 60.0 ± 19.5 (38.6–90.5) | 0.001 * |
| Deep sleep (N3) (%) | 38.1 ± 24.3 (0–76.5) | 22.0 ± 15.0 (1.9–48.6) | 0.011 * |
| REM (%) | 36.1 ± 24.1 (6.9–81.5) | 17.7 ± 11.7 (1.8–38.0) | 0.003 * |
| Abnormal REM (%) | 1.6 ± 1.3 (0–4.0) | 3.8 ± 5.0 (0–25.0) | 0.04 * |
| Subject | Control Group (n = 18) | PD Group w. Clonazepam (n = 10) | PD group w.o. Clonazepam (n = 10) | p-Value |
|---|---|---|---|---|
| Mean ± SD (Minimum–Maximum) | Mean ± SD (Minimum–Maximum) | Mean ± SD (Minimum–Maximum) | ||
| Light sleep (N1 + N2) (%) | 25.7 ± 21.3 (3.0–79.4) | 56.2 ± 19.4 (38.6–90.3) | 64.2 ± 19.7 (40.0–90.5) | 0.001 * |
| Deep sleep (N3) (%) | 38.1 ± 24.3 (0–76.5) | 27.3 ± 15.0 (1.9–43.7) | 16.8 ± 13.8 (1.9–48.6) | 0.031 * |
| REM (%) | 36.1 ± 24.1 (6.9–81.5) | 16.4 ± 11.2 (1.8–31.4) | 18.9 ± 12.7 (4.5–38.0) | 0.017 * |
| Abnormal REM (%) | 1.6 ± 1.3 (0–4.0) | 2.0 ± 1.7 (0–4.8) | 5.7 ± 7.1 (1.3–25.0) | 0.007 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, Y.-F.; Kuo, P.-H.; Wang, C.-F.; Chen, Y.-J.; Chuang, P.-C.; Li, S.-Z.; Chen, B.-W.; Yang, F.-C.; Lo, Y.-C.; Yang, Y.; et al. Quantification Analysis of Sleep Based on Smartwatch Sensors for Parkinson’s Disease. Biosensors 2022, 12, 74. https://doi.org/10.3390/bios12020074
Ko Y-F, Kuo P-H, Wang C-F, Chen Y-J, Chuang P-C, Li S-Z, Chen B-W, Yang F-C, Lo Y-C, Yang Y, et al. Quantification Analysis of Sleep Based on Smartwatch Sensors for Parkinson’s Disease. Biosensors. 2022; 12(2):74. https://doi.org/10.3390/bios12020074
Chicago/Turabian StyleKo, Yi-Feng, Pei-Hsin Kuo, Ching-Fu Wang, Yu-Jen Chen, Pei-Chi Chuang, Shih-Zhang Li, Bo-Wei Chen, Fu-Chi Yang, Yu-Chun Lo, Yi Yang, and et al. 2022. "Quantification Analysis of Sleep Based on Smartwatch Sensors for Parkinson’s Disease" Biosensors 12, no. 2: 74. https://doi.org/10.3390/bios12020074