The Introduction of a New Diagnostic Tool in Forensic Pathology: LiDAR Sensor for 3D Autopsy Documentation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
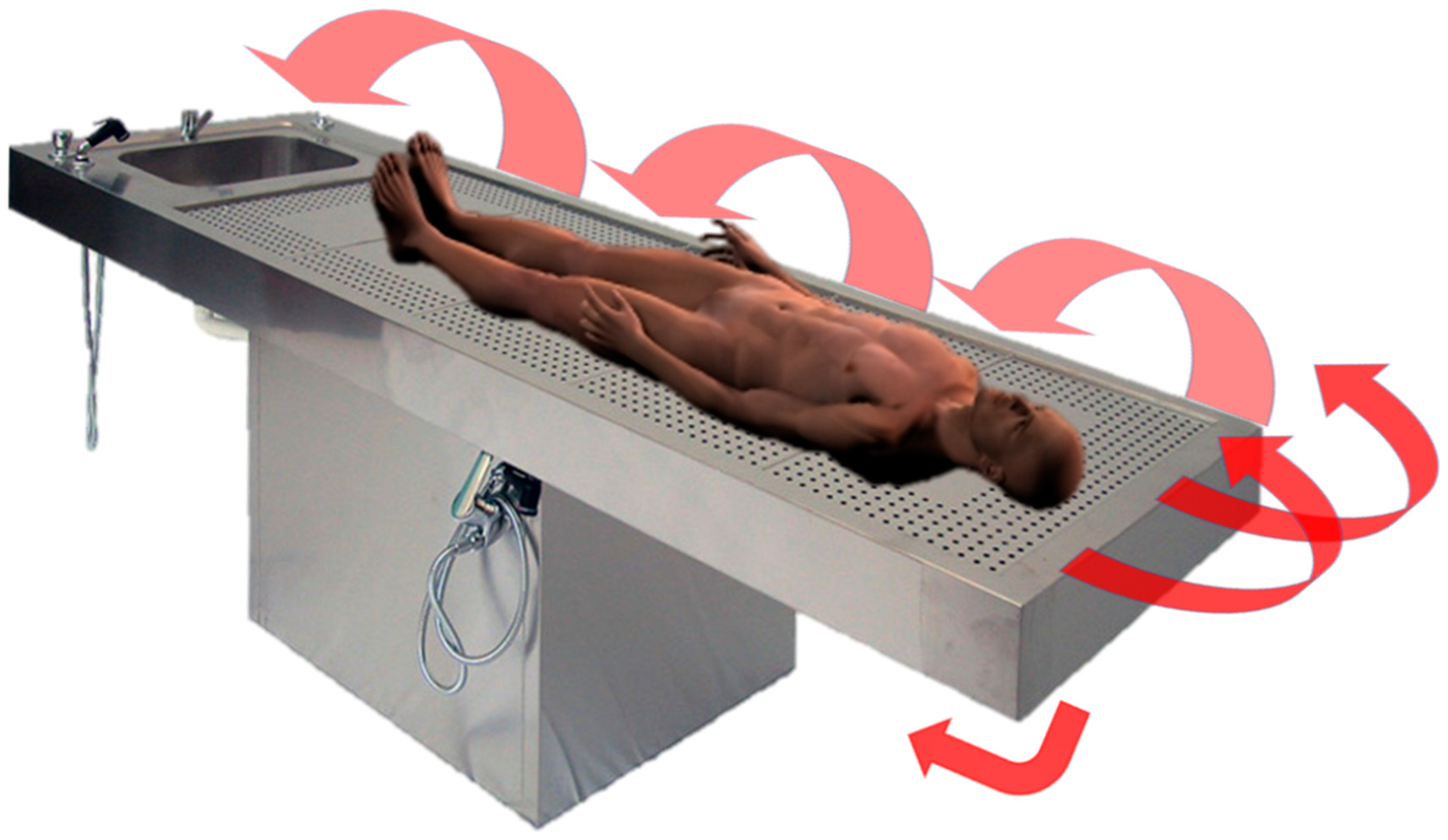
2.2. Equipment, Recording Method, and 3D Model Processing
2.3. Quality and Trustworthiness Evaluation
- −
- Conventional autopsy photographic records vs. 3D reconstruction: qualitative evaluation by consensus.
- −
- Body/lesion measurement attained during the autoptic examination vs. body/lesion measurement attained from the 3D model. When a discrepancy was noticed, re-measurements were obtained.
- −
- Lesion description and autopsy revaluation from conventional autopsy photograph records vs. from 3D image review: qualitative evaluation was performed by two forensic pathologists who did not attend the autopsy and did not have knowledge about the cases.
2.4. 3D Printing
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Thali, M.J.; Braun, M.; Dirnhofer, R. Optical 3D surface digitizing in forensic medicine: 3D documentation of skin and bone injuries. Forensic Sci. Int. 2003, 137, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Gitto, L.; Donato, L.; Di Luca, A.; Bryant, S.M.; Serinelli, S. The Application of Photogrammetry in the Autopsy Room: A Basic, Practical Workflow. J. Forensic Sci. 2020, 65, 2146–2154. [Google Scholar] [CrossRef]
- Schweitzer, W.; Röhrich, E.; Schaepman, M.; Thali, M.J.; Ebert, L. Aspects of 3D surface scanner performance for post-mortem skin documentation in forensic medicine using rigid benchmark objects. J. Forensic Radiol. Imaging 2013, 1, 167–175. [Google Scholar] [CrossRef]
- Thali, M.J.; Braun, M.; Brueschweiler, W.; Dirnhofer, R. ‘Morphological imprint’: Determination of the injury-causing weapon from the wound morphology using forensic 3D/CAD-supported photogrammetry. Forensic Sci. Int. 2003, 132, 177–181. [Google Scholar] [CrossRef]
- Villa, C. Forensic 3D documentation of skin injuries. Int. J. Leg. Med. 2016, 131, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Sansoni, G.; Cattaneo, C.; Trebeschi, M.; Gibelli, D.; Porta, D.; Picozzi, M. Feasibility of contactless 3d optical measureme for the analysis of bone and soft tissue lesions: New technologies and perspectives in forensic sciences. J. Forensic Sci. 2009, 54, 540–545. [Google Scholar] [CrossRef]
- Grassberger, M.; Gehl, A.; Püschel, K.; Turk, E. 3D reconstruction of emergency cranial computed tomography scans as a tool in clinical forensic radiology after survived blunt head trauma—Report of two cases. Forensic Sci. Int. 2011, 207, e19–e23. [Google Scholar] [CrossRef]
- American Geosciences Institute. Available online: https://www.americangeosciences.org/critical-issues/faq/what-lidar-and-what-it-used (accessed on 11 February 2021).
- Cabaleiro, M.; Riveiro, B.; Arias, P.; Caamaño, J.; Vilán, J. Automatic 3D modelling of metal frame connections from LiDAR data for structural engineering purposes. ISPRS J. Photogramm. Remote Sens. 2014, 96, 47–56. [Google Scholar] [CrossRef]
- Bolliger, S.A.; Thali, M.J. Imaging and virtual autopsy: Looking back and forward. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140253. [Google Scholar] [CrossRef]
- Shintaku, H.; Yamaguchi, M.; Toru, S.; Kitagawa, M.; Hirokawa, K.; Yokota, T.; Uchihara, T. Three-dimensional surface models of autopsied human brains constructed from multiple photographs by photogrammetry. PLoS ONE 2019, 14, e0219619. [Google Scholar] [CrossRef] [Green Version]
- Grabherr, S.; Baumann, P.; Minoiu, C.; Fahrni, S.; Mangin, P. Post-mortem imaging in forensic investigations: Current utility, limitations, and ongoing developments. Res. Rep. Forensic Med Sci. 2016, 6, 25–37. [Google Scholar] [CrossRef]
- Kottner, S.; Schaerli, S.; Fürst, M.; Ptacek, W.; Thali, M.; Gascho, D. VirtoScan-on-Rails—An automated 3D imaging system for fast post-mortem whole-body surface documentation at autopsy tables. J. Forensic Med. Pathol. 2019, 15, 198–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kottner, S.; Schulz, M.M.; Berger, F.; Thali, M.; Gascho, D. Beyond the visible spectrum—Applying 3D multispectral full-body imaging to the VirtoScan system. Forensic Sci. Med. Pathol. 2021, 17, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Tóth, D.; Petrus, K.; Heckmann, V.; Simon, G.; Poór, V.S. Application of photogrammetry in forensic pathology education of medical students in response to COVID-19. J. Forensic Sci. 2021, 66, 1533–1537. [Google Scholar] [CrossRef]
- Yoo, S.-S. 3D-printed biological organs: Medical potential and patenting opportunity. Expert Opin. Ther. Patents 2015, 25, 507–511. [Google Scholar] [CrossRef] [Green Version]
- Schubert, C.; Van Langeveld, M.C.; A Donoso, L. Innovations in 3D printing: A 3D overview from optics to organs. Br. J. Ophthalmol. 2014, 98, 159–161. [Google Scholar] [CrossRef]
- iPhone 12 Pro Technical Specifications. Available online: https://support.apple.com/kb/SP831?locale=it_IT&viewlocale=en_US (accessed on 10 February 2022).
- Cignoni, P.; Callieri, M.; Corsini, M.; Dellepiane, M.; Ganovelli, F.; Ranzuglia, G. MeshLab: An open-source mesh processing tool. In Proceedings of the 6th Eurographics Italian Chapter Conference, Salerno, Italy, 2–4 July 2008. [Google Scholar]
- Roberts, I.S.; Benamore, R.E.; Benbow, E.W.; Lee, S.H.; Harris, J.N.; Jackson, A.; Mallett, S.; Patankar, T.; Peebles, C.; Roobottom, C.; et al. Post-mortem imaging as an alternative to autopsy in the diagnosis of adult deaths: A validation study. Lancet 2012, 379, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Henham, A.P.; Lee, K.A.P. Photography in forensic medicine. J. Audiov. Media Med. 1994, 17, 15–20. [Google Scholar] [CrossRef]
- Gouse, S.; Karnam, S.; Girish, H.; Murgod, S. Forensic photography: Prospect through the lens. J. Forensic Dent. Sci. 2018, 10, 2–4. [Google Scholar] [CrossRef]
- Urschler, M.; Bornik, A.; Scheurer, E.; Yen, K.; Bischof, H.; Schmalstieg, D. Forensic-Case Analysis: From 3D Imaging to Interactive Visualization. IEEE Comput. Graph. Appl. 2012, 32, 79–87. [Google Scholar] [CrossRef]
- Maiese, A.; Gitto, L.; dell’Aquila, M.; Bolino, G. When the hidden features become evident: The usefulness of PMCT in a strangulation-related death. Leg. Med. (Tokyo) 2014, 16, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Thali, M.; Dirnhofer, R.; Vock, P. The Virtopsy Approach: 3D Optical and Radiological Scanning and Reconstruction in Forensic Med-icine, 1st ed.; CRC: New York, NY, USA, 2009; pp. 3–10. [Google Scholar]
- Bertozzi, G.; Cafarelli, F.P.; Ferrara, M.; Di Fazio, N.; Guglielmi, G.; Cipolloni, L.; Manetti, F.; La Russa, R.; Fineschi, V. Sudden Cardiac Death and Ex-Situ Post-Mortem Cardiac Magnetic Resonance Imaging: A Morphological Study Based on Diagnostic Correlation Methodology. Diagnostics 2022, 12, 218. [Google Scholar] [CrossRef] [PubMed]
- Buck, U.; Naether, S.; Räss, B.; Jackowski, C.; Thali, M.J. Accident or homicide—Virtual crime scene reconstruction using 3D methods. Forensic Sci. Int. 2013, 225, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Z.; Hu, W.; Shao, Y.; Wang, L.; Wu, R.; Ma, K.; Zou, D.; Chen, Y. Virtual reality and integrated crime scene scanning for immersive and heterogeneous crime scene reconstruction. Forensic Sci. Int. 2019, 303, 109943. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Zheng, H.; Lallie, H. Virtual Reality and 3D Animation in Forensic Visualization. J. Forensic Sci. 2010, 55, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Leipner, A.; Baumeister, R.; Thali, M.J.; Braun, M.; Dobler, E.; Ebert, L.C. Multi-camera system for 3D forensic documentation. Forensic Sci. Int. 2016, 261, 123–128. [Google Scholar] [CrossRef]
- Sieberth, T.; Ebert, L.C.; Gentile, S.; Fliss, B. Clinical forensic height measurements on injured people using a multi camera device for 3D documentation. Forensic Sci. Med. Pathol. 2020, 16, 586–594. [Google Scholar] [CrossRef]
- Brüschweiler, W.; Braun, M.; Dirnhofer, R.; Thali, M. Analysis of patterned injuries and injury-causing instruments with forensic 3D/CAD supported photogrammetry (FPHG): An instruction manual for the documentation process. Forensic Sci. Int. 2003, 132, 130–138. [Google Scholar] [CrossRef]
- Urbanová, P.; Hejna, P.; Jurda, M. Testing photogrammetry-based techniques for three-dimensional surface documentation in forensic pathology. Forensic Sci. Int. 2015, 250, 77–86. [Google Scholar] [CrossRef]
- Flies, M.J.; Larsen, P.K.; Lynnerup, N.; Villa, C. Forensic 3D documentation of skin injuries using photogrammetry: Photographs vs. video and manual vs. automatic measurements. Int. J. Leg. Med. 2018, 133, 963–971. [Google Scholar] [CrossRef]
- Slot, L.; Larsen, P.K.; Lynnerup, N. Photogrammetric Documentation of Regions of Interest at Autopsy-A Pilot Study. J. Forensic Sci. 2013, 59, 226–230. [Google Scholar] [CrossRef] [PubMed]
- The Coroner’s Autopsy: Do We Deserve better? A Report of the National Confidential Enquiry into Patient Outcome and Death, 2006. Available online: https://www.ncepod.org.uk/2006Report/Downloads/Coronial%20Autopsy%20Report%202006.pdf (accessed on 11 February 2021).
- Arunkumar, P.; Maiese, A.; Bolino, G.; Gitto, L. Determined to Die! Ability to Act Following Multiple Self-inflicted Gunshot Wounds to the Head. The Cook County Office of Medical Examiner Experience (2005–2012) and Review of Literature. J. Forensic Sci. 2015, 60, 1373–1379. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Sex | Age (y.o.) |
|---|---|---|
| 1 | M | 71 |
| 2 | M | 54 |
| 3 | F | 45 |
| 4 | M | 63 |
| 5 | F | 81 |
| 6 | M | 35 |
| 7 | F | 22 |
| 8 | F | 55 |
| 9 | M | 58 |
| 10 | M | 74 |
| Case Number | Macroscopic Findings | Microscopic Findings | Cause of Death |
|---|---|---|---|
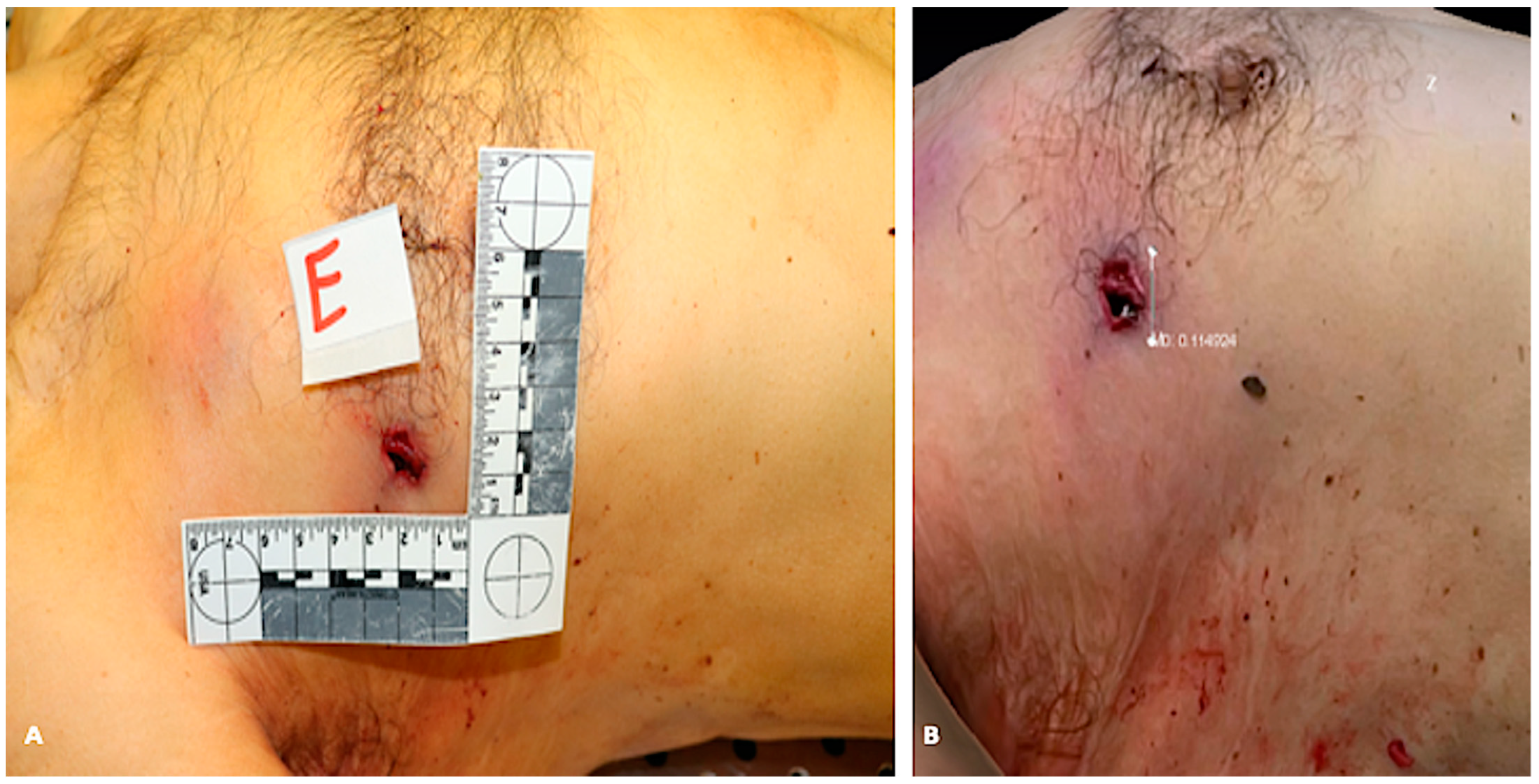
| 1 | Entrance gunshot wound in the right side of the trunk, exit gunshot wound in the left side of the trunk | Hemorrhagic infiltration of soft tissues near the gunshot wounds | Gunshot |
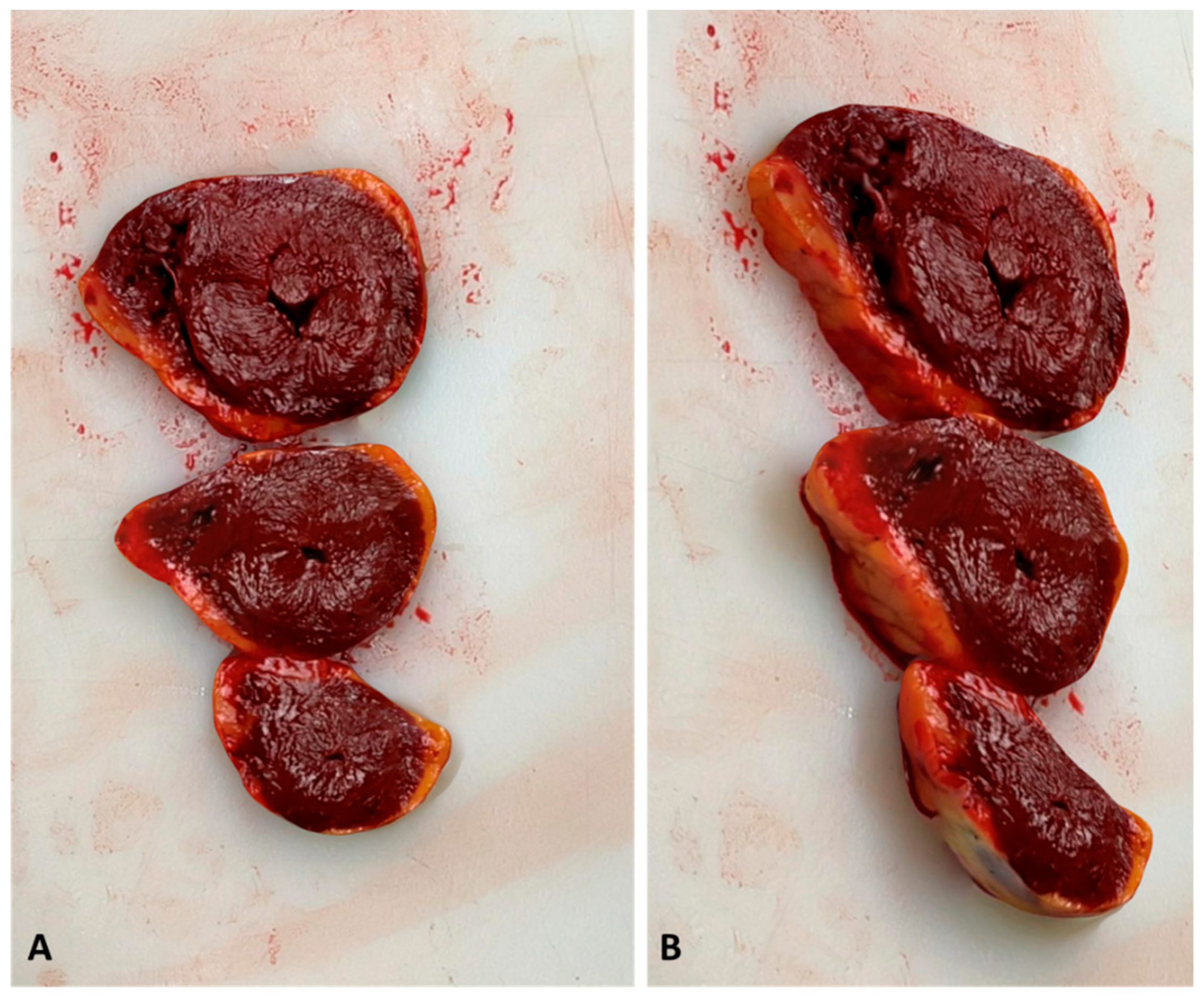
| 2 | Coronary artery disease (atheromatous plaque) | Myocardial ischemia | Cardiovascular disease |
| 3 | Left ventricular hypertrophy | Diffuse myocardial interstitial fibrosis, myocardial hypertrophy | Cardiovascular disease |
| 4 | Diffuse burn lesions in various degrees, soot in the airways | Soot deposition in the medium and small airways’ mucosa, intraepidermal and subepidermal separation alongside coagulation necrosis in the skin | Fire burn > 40% body surface |
| 5 | Entrance gunshot wound in the oral cavity, several skull fracture | Hemorrhagic infiltration of soft tissues near the gunshot wound | Gunshot |
| 6 | Both ventricles dilation | Long and thin myocytes, interstitial fibrosis | Cardiovascular disease |
| 7 | Skull base fractures, lower limbs fractures, intracranial hemorrhage, and cerebral lacerations | Subarachnoid hemorrhage, hemorrhagic infiltration of soft tissues | Traffic accident |
| 8 | Multiple costal fractures, upper limbs fractures, multiple excoriations, heart lacerations, lungs ecchymoses | Hemorrhagic infiltration of soft tissues | Traffic accident |
| 9 | Coronary artery disease (atheromatous plaque) | Myocardial ischemia | Cardiovascular disease |
| 10 | Coronary artery disease (atheromatous plaque) | Myocardial ischemia | Cardiovascular disease |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maiese, A.; Manetti, A.C.; Ciallella, C.; Fineschi, V. The Introduction of a New Diagnostic Tool in Forensic Pathology: LiDAR Sensor for 3D Autopsy Documentation. Biosensors 2022, 12, 132. https://doi.org/10.3390/bios12020132
Maiese A, Manetti AC, Ciallella C, Fineschi V. The Introduction of a New Diagnostic Tool in Forensic Pathology: LiDAR Sensor for 3D Autopsy Documentation. Biosensors. 2022; 12(2):132. https://doi.org/10.3390/bios12020132
Chicago/Turabian StyleMaiese, Aniello, Alice Chiara Manetti, Costantino Ciallella, and Vittorio Fineschi. 2022. "The Introduction of a New Diagnostic Tool in Forensic Pathology: LiDAR Sensor for 3D Autopsy Documentation" Biosensors 12, no. 2: 132. https://doi.org/10.3390/bios12020132