Detection and Quantification of Tp53 and p53-Anti-p53 Autoantibody Immune Complex: Promising Biomarkers in Early Stage Lung Cancer Diagnosis


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Clinical Samples
2.3. Preparation of Bio-Conjugates
2.3.1. Synthesis of p53-cAb-DNA Conjugate
2.3.2. Synthesis of Anti-Mouse IgG-Cy5 and Anti-Human IgG-Cy5
2.3.3. Synthesis of p53-dAb-FB and Anti-Human-IgG-FB Conjugates
2.3.4. Synthesis of FB-DNA Conjugate
2.4. Preparation of Lateral Flow Strip Membranes (LFSM) for the Detection of PIC and Tp53
2.5. Quantification of PIC in the Lung Cancer Sample Using 9G DNAChip and DAGON Method
2.5.1. Obtaining a Standard Curve for PIC Quantification
2.5.2. Quantification of PIC in Lung Cancer Sample and its Quantification
2.6. General Procedure for the Detection of PIC and Tp53 Using LFSM
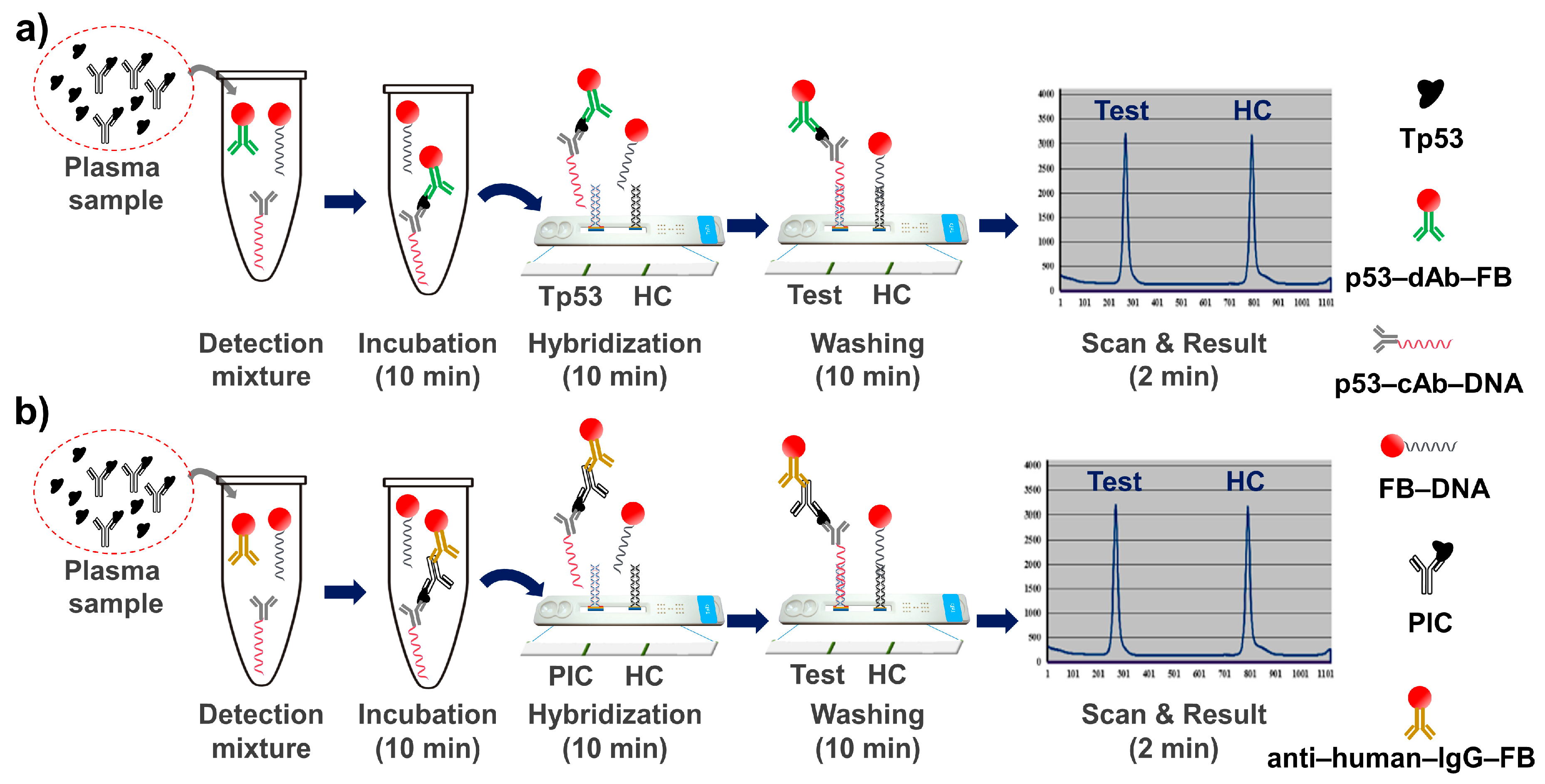
2.6.1. Detection of Tp53 Using LFSM
2.6.2. Detection of PIC Using LFSM
2.7. Optimization of Incubation Time, Hybridization Time, and Washing Time for Tp53 and PIC Detection
2.8. Interference Study
2.9. Linearity Study Using Clinical Samples, Standard Curves for Tp53 and PIC
2.10. Statistical Analysis
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Caini, S.; Del Riccio, M.; Vettori, V.; Scotti, V.; Martinoli, C.; Raimondi, S.; Cammarata, G.; Palli, D.; Banini, M.; Masala, G.; et al. Quitting Smoking At or Around Diagnosis Improves the Overall Survival of Lung Cancer Patients: A Systematic Review and Meta-Analysis. J. Thorac. Oncol. 2022. [Google Scholar] [CrossRef]
- Emmerick, I.C.M.; Singh, A.; Powers, M.; Lou, F.; Lin, P.; Maxfield, M.; Uy, K. Factors associated with diagnosis of stages I and II lung cancer: A multivariate analysis. Rev. Saude. Publica 2021, 55, 112. [Google Scholar] [CrossRef]
- Babar, L.; Modi, P.; Anjum, F. Lung Cancer Screening. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.; Jemal, A. Cancer Statistics 2021. CA Cancer J. Clin. 2021, 1, 7–33. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 962–970. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]
- Sozzi, G.; Boeri, M. Potential biomarkers for lung cancer screening. Transl. Lung Cancer Res. 2014, 3, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Schlichtholz, B.; Tredaniel, J.; Lubin, R.; Zalcman, G.; Hirsch, A.; Soussi, T. Analyses of p53 antibodies in sera of patients with lung carcinoma define immunodominant regions in the p53 protein. Br. J. Cancer 1994, 69, 809–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laudanski, J.; Niklinska, W.; Burzykowski, T.; Chyczewski, L.; Niklinski, J. Prognostic significance of p53 and bcl-2 abnormalities in operable nonsmall cell lung cancer. Eur. Respir. J. 2001, 17, 660–666. [Google Scholar] [CrossRef] [Green Version]
- Choe, W.; Chae, J.D.; Lee, B.H.; Kim, S.H.; Park, S.Y.; Nimse, S.B.; Kim, J.; Warkad, S.D.; Song, K.S.; Oh, A.C.; et al. 9G Test(TM) Cancer/Lung: A Desirable Companion to LDCT for Lung Cancer Screening. Cancers (Basel) 2020, 12, 3192. [Google Scholar] [CrossRef] [PubMed]
- Soussi, T. p53 Antibodies in the sera of patients with various types of cancer: A review. Cancer Res. 2000, 60, 1777–1788. [Google Scholar] [PubMed]
- Giaccia, A.J.; Kastan, M.B. The complexity of p53 modulation: Emerging patterns from divergent signals. Genes. Dev. 1998, 12, 2973–2983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, S.E.; Kim, R.; Wang, P.C.; Bhat, U.G.; Kusumoto, H.; Lu, T.; Beck, W.T. Differences in mutant p53 protein stability and functional activity in teniposide-sensitive and -resistant human leukemic CEM cells. Oncogene 2000, 19, 5010–5019. [Google Scholar] [CrossRef] [Green Version]
- Yan, W.; Liu, S.; Xu, E.; Zhang, J.; Zhang, Y.; Chen, X.; Chen, X. Histone deacetylase inhibitors suppress mutant p53 transcription via histone deacetylase 8. Oncogene 2013, 32, 599–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollstein, M.; Sidransky, D.; Vogelstein, B.; Harris, C.C. p53 mutations in human cancers. Science 1991, 253, 49–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubin, R.; Zalcman, G.; Bouchet, L.; Tredanel, J.; Legros, Y.; Cazals, D.; Hirsch, A.; Soussi, T. Serum p53 antibodies as early markers of lung cancer. Nat. Med. 1995, 1, 701–702. [Google Scholar] [CrossRef] [PubMed]
- Rurańska, B.; Stawicka, M.; Godlewski, D. The role of p53 gene in lung cancer with special emphasis on hereditary types. Rep. Pract. Oncol. 1997, 2, 56. [Google Scholar] [CrossRef]
- Li, Y.; Karjalainen, A.; Koskinen, H.; Hemminki, K.; Vainio, H.; Shnaidman, M.; Ying, Z.; Pukkala, E.; Brandt-Rauf, P.W. p53 autoantibodies predict subsequent development of cancer. Int. J. Cancer 2005, 114, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Solassol, J.; Maudelonde, T.; Mange, A.; Pujol, J.-L. Clinical Relevance of Autoantibody Detection in Lung Cancer. J. Thorac. Oncol. 2011, 6, 955–962. [Google Scholar] [CrossRef]
- Desmetz, C.; Mange, A.; Maudelonde, T.; Solassol, J. Autoantibody signatures: Progress and perspectives for early cancer detection. J. Cell. Mol. Med. 2011, 15, 2013–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, L.; Tsay, J.-C.J.; Li, J.; Yie, T.-A.; Munger, J.S.; Pass, H.; Rom, W.N.; Zhang, Y.; Tan, E.M.; Zhang, J.-Y. Autoantibodies against tumor-associated antigens in the early detection of lung cancer. Lung Cancer 2016, 99, 172–179. [Google Scholar] [CrossRef]
- Song, K.-S.; Nimse, S.B.; Sonawane, M.D.; Lin, Y.; Zhou, Z.; Kim, T. A glass fibre membrane platform for ultra-sensitive detection of cardiac troponin T. Analyst 2017, 142, 3816–3821. [Google Scholar] [CrossRef] [PubMed]
- Sonawane, M.D.; Nimse, S.B.; Song, K.-S.; Kim, T. Multiplex detection of cardiac biomarkers. Anal. Methods 2017, 9, 3773–3776. [Google Scholar] [CrossRef]
- Jung, Y.; Lee, J.M.; Jung, H.; Chung, B.H. Self-Directed and Self-Oriented Immobilization of Antibody by Protein G−DNA Conjugate. Anal. Chem. 2007, 79, 6534–6541. [Google Scholar] [CrossRef] [PubMed]
- Song, S.Y.; Han, Y.D.; Kim, K.; Yang, S.S.; Yoon, H.C. A fluoro-microbead guiding chip for simple and quantifiable immunoassay of cardiac troponin I (cTnI). Biosens. Bioelectron. 2011, 26, 3818–3824. [Google Scholar] [CrossRef] [PubMed]
- Sayyed, D.R.; Song, K.-S.; Nimse, S.B.; An, H.; Kim, J.; Kim, T. HPV Genotyping 9G Membrane Test. Viruses 2013, 5, 2840–2855. [Google Scholar] [CrossRef]
- Song, K.; Nimse, S.B.; An, H.; Kim, T. HPV Genotyping 9G Membrane Test: A Point-of-Care Diagnostic Platform. Sensors 2014, 14, 19162–19175. [Google Scholar] [CrossRef] [Green Version]
- Song, K.-S.; Nimse, S.B.; Cho, N.H.; Sung, N.; Kim, H.-j.; Yang, J.; Kim, T. MTB-DR-RIF 9G test: Detection and discrimination of tuberculosis and multi-drug resistant tuberculosis strains. Tuberculosis 2015, 95, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Chantratita, W.; Song, K.-S.; Nimse, S.B.; Pongthanapisith, V.; Thongbaiphet, N.; Wongtabtim, G.; Pasomsub, E.; Angkanavin, K.; Sonawane, M.D.; Warkad, S.D.; et al. 6 HCV Genotyping 9G test for HCV 1a, 1b, 2, 3, 4 and 6 (6a, 6f, 6i and 6n) with high accuracy. J. Virol. Methods 2017, 246, 95–99. [Google Scholar] [CrossRef] [PubMed]
- May, P.; May, E. Twenty years of p53 research: Structural and functional aspects of the p53 protein. Oncogene 1999, 18, 7621–7636. [Google Scholar] [CrossRef] [Green Version]
- el-Deiry, W.S.; Kern, S.E.; Pietenpol, J.A.; Kinzler, K.W.; Vogelstein, B. Definition of a consensus binding site for p53. Nat. Genet. 1992, 1, 45–49. [Google Scholar] [CrossRef]
- Donehower, L.A.; Soussi, T.; Korkut, A.; Liu, Y.; Schultz, A.; Cardenas, M.; Li, X.; Babur, O.; Hsu, T.-K.; Lichtarge, O.; et al. Integrated Analysis of TP53 Gene and Pathway Alterations in The Cancer Genome Atlas. Cell Rep. 2019, 28, 1370–1384.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, K.S.; Nimse, S.B.; Kim, J.; Kim, J.; Nguyen, V.T.; Ta, V.T.; Kim, T. 9G DNAChip: Microarray based on the multiple interactions of 9 consecutive guanines. Chem Commun. (Camb) 2011, 47, 7101–7103. [Google Scholar] [CrossRef] [Green Version]
- Song, K.-S.; Nimse, S.B.; Kim, J.; Kim, J.; Ta, V.-T.; Nguyen, V.-T.; Kim, T. 9G DNAChip: A platform for the efficient detection of proteins. Chem. Commun. 2011, 47, 7716–7718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimse, S.B.; Song, K.-S.; Kim, J.; Sayyed, D.R.; Kim, T. 9G DNAChip Technology: Self-Assembled Monolayer (SAM) of ssDNA for Ultra-Sensitive Detection of Biomarkers. Int. J. Mol. Sci. 2013, 14, 5723–5733. [Google Scholar] [CrossRef] [PubMed]
- Pierson-Perry, J.F.; Vaks, J.E.; Durham, A.P.; Fischer, C.; Gutenbrunner, C.; Hillyard, D.; Kondratovich, M.V.; Ladwig, P.; Middleberg, R.A. Evaluation of Detection Capability for Clinical Laboratory Measurement Procedures; Approved Guideline-Second Edition; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012; pp. 8–10. [Google Scholar]
- Oostendorp, M.; Lentjes, E.G. Utility of dilution tests in investigating interference in the free thyroxine assay. Clin. Chem. Lab. Med. 2017, 55, e4–e6. [Google Scholar] [CrossRef]
- Szkandera, J.; Stotz, M.; Absenger, G.; Stojakovic, T.; Samonigg, H.; Kornprat, P.; Schaberl-Moser, R.; Alzoughbi, W.; Lackner, C.; Ress, A.L.; et al. Validation of C-reactive protein levels as a prognostic indicator for survival in a large cohort of pancreatic cancer patients. Br. J. Cancer 2014, 110, 183–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, K.-S.; Nimse, S.B.; Warkad, S.D.; Oh, A.-C.; Kim, T.; Hong, Y.J. Quantification of CYFRA 21-1 and a CYFRA 21-1–anti-CYFRA 21-1 autoantibody immune complex for detection of early stage lung cancer. Chem. Commun. 2019, 55, 10060–10063. [Google Scholar] [CrossRef] [Green Version]
- Vassilakopoulos, T.; Troupis, T.; Sotiropoulou, C.; Zacharatos, P.; Katsaounou, P.; Parthenis, D.; Noussia, O.; Troupis, G.; Papiris, S.; Kittas, C.; et al. Diagnostic and prognostic significance of squamous cell carcinoma antigen in non-small cell lung cancer. Lung Cancer 2001, 32, 137–144. [Google Scholar] [CrossRef]
- Lee, J.S.; Song, I.H.; Warkad, S.D.; Yeom, G.S.; Nimse, S.B. An abiotic fluorescent probe for the detection and quantification of carcinoembryonic antigen. Bioorg. Chem. 2022, 119, 105490. [Google Scholar] [CrossRef] [PubMed]
- Sanchez De Cos, J.; Masa, F.; de la Cruz, J.L.; Disdier, C.; Vergara, C. Squamous cell carcinoma antigen (SCC Ag) in the diagnosis and prognosis of lung cancer. Chest 1994, 105, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Zhang, L.; Wang, B. The Value of Combination Analysis of Tumor Biomarkers for Early Differentiating Diagnosis of Lung Cancer and Pulmonary Tuberculosis. Ann. Clin. Lab. Sci. 2019, 49, 645–649. [Google Scholar] [PubMed]
- Chu, X.Y.; Hou, X.B.; Song, W.A.; Xue, Z.Q.; Wang, B.; Zhang, L.B. Diagnostic values of SCC, CEA, Cyfra21-1 and NSE for lung cancer in patients with suspicious pulmonary masses: A single center analysis. Cancer Biol. Ther. 2011, 11, 995–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Body, J.J.; Sculier, J.P.; Raymakers, N.; Paesmans, M.; Ravez, P.; Libert, P.; Richez, M.; Dabouis, G.; Lacroix, H.; Bureau, G.; et al. Evaluation of squamous cell carcinoma antigen as a new marker for lung cancer. Cancer 1990, 65, 1552–1556. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Healthy Population (n = 15) | Lung Cancer Patients (n = 30) |
|---|---|---|
| Age, years (SD) | 60 (58–68) | 61.5 (47–81) |
| Male gender, n (%) | 55 (64.5%) | 17 (65.7%) |
| PIC, pg/mL (IQR) | 2497.5 (350.4~5676.3) | 2871.5 (310.3~7500.0) |
| Tp53, pg/mL (IQR) | 2026.8 (271.0~4887.2) | 1282.6 (111.10~4530.6) |
| PIC/Tp53 ratio (IQR) | 1.23 (0.706~1.920) | 2.22 (1.164~3.384) |
| CIC, pg/mL (IQR) | 3.11 (0.411~8.146) | 3.15 (0.499~8.038) |
| CYFRA 21-1, pg/mL (IQR) | 2.13 (0.408~5.168) | 1.35 (0.186~4.271) |
| CIC/CYFRA 21-1 ratio (IQR) | 1.46 (0.411~8.146) | 2.51 (1.632~4.244) |
| Cancer Index [(CS1/CS2) × (LS1/LS2)] | 1.79 (0.759~2.766) | 5.41 (3.615~9.401) |
| Biomarkers | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|
| PIC | 16.7 (5.64~34.7) | 93.3 (68.1~99.8) | 83.3 (39.0~97.5) | 35.9 (31.2~40.9) |
| Tp53 | 23.3 (9.93~42.3) | 66.7 (38.4~88.2) | 58.33 (34.8~78.6) | 30.3 (22.42~39.6) |
| PIC/Tp53 ratio | 78.7 (69.2~96.2) | 93.3 (68.1~99.8) | 96.3 (79.6~99.4) | 77.8 (58.2~89.8) |
| CIC | 13.3 (3.8~30.7) | 86.7 (59.5~98.3) | 66.6 (29.2~90.7) | 33.3 (28.2~38.9) |
| CYFRA 21-1 | 10.0 (44.9~92.2) | 73.3 (44.9~92.2) | 42.9 (16.1~74.5) | 28.9 (22.7~36.1) |
| CIC/CYFRA 21-1 | 73.3 (54.1~87.7) | 93.3 (78.2~98.5) | 76.7 (59.4–87.1) | 65.2 (50.9~77.2) |
| Cancer Index [(CS1/CS2) × (LS1/LS2)] | 81.6 (88.4~98.1) | 93.3 (78.2~99.4) | 86.7 (67.2–92.5) | 71.2 (68.4–95.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, K.-S.; Nimse, S.B.; Warkad, S.D.; Kim, J.-H.; Kim, H.-J.; Kim, T. Detection and Quantification of Tp53 and p53-Anti-p53 Autoantibody Immune Complex: Promising Biomarkers in Early Stage Lung Cancer Diagnosis. Biosensors 2022, 12, 127. https://doi.org/10.3390/bios12020127
Song K-S, Nimse SB, Warkad SD, Kim J-H, Kim H-J, Kim T. Detection and Quantification of Tp53 and p53-Anti-p53 Autoantibody Immune Complex: Promising Biomarkers in Early Stage Lung Cancer Diagnosis. Biosensors. 2022; 12(2):127. https://doi.org/10.3390/bios12020127
Chicago/Turabian StyleSong, Keum-Soo, Satish Balasaheb Nimse, Shrikant Dashrath Warkad, Jung-Hoon Kim, Hey-Jin Kim, and Taisun Kim. 2022. "Detection and Quantification of Tp53 and p53-Anti-p53 Autoantibody Immune Complex: Promising Biomarkers in Early Stage Lung Cancer Diagnosis" Biosensors 12, no. 2: 127. https://doi.org/10.3390/bios12020127