A Useful Combination of Quantitative Ultrashort Echo Time MR Imaging and a Probing Device for Biomechanical Evaluation of Articular Cartilage

 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lyyra, T.; Jurvelin, J.; Pitkänen, P.; Väätäinen, U.; Kiviranta, I. Indentation instrument for the measurement of cartilage stiffness under arthroscopic control. Med. Eng. Phys. 1995, 17, 395–399. [Google Scholar] [CrossRef]
- Kiviranta, P.; Lammentausta, E.; Töyräs, J.; Kiviranta, I.; Jurvelin, J.S. Indentation diagnostics of cartilage degeneration. Osteoarthri. Tis. Cartil. 2008, 16, 796–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steadman, J.R.; Rodkey, W.G.; Rodrigo, J.J. Microfracture: Surgical technique and rehabilitation to treat chondral defects. Clin. Orthop. Relat. Res. 2001, 391, S362–S369. [Google Scholar] [CrossRef] [PubMed]
- Matsusue, Y.; Yamamuro, T.; Hama, H. Arthroscopic multiple osteochondral transplantation to the chondral defect in the knee asso ciated with anterior cruciate ligament disruption. Arthroscopy 1993, 9, 318–321. [Google Scholar] [CrossRef]
- Wakitani, S.; Goto, T.; Pineda, S.J.; Young, R.G.; Mansour, J.M.; Caplan, A.I.; Goldberg, V.M. Mesenchymal cell-based repair of large, full-thickness defects of articular cartilage. J. Bone Jt. Surg. Am. 1994, 76, 579–592. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Uchio, Y.; Kawasaki, K.; Wakitani, S.; Iwasa, J. Transplantation of cartilage-like tissue made by tissue engineering in the treat ment of cartilage defects of the knee. J. Bone Jt. Surg. Br. 2002, 84, 571–578. [Google Scholar] [CrossRef]
- Nieminen, M.T.; Töyräs, J.; Laasanen, M.S.; Silvennoinen, J.; Helminen, H.J.; Jurvelin, J.S. Prediction of biomechanical properties of articular cartilage with quantitative magnetic resonance imaging. J. Biomech. 2004, 37, 321–328. [Google Scholar] [CrossRef]
- Nykänen, O.; Sarin, J.K.; Ketola, J.H.; Leskinen, H.; Te Moller, N.C.R.; Tiitu, V.; Mancini, I.A.D.; Visser, J.; Brommer, H.; van Weeren, P.R.; et al. T2* and quantitative susceptibility mapping in an equine model of post-traumatic osteoarthritis: Assessment of mechanical and structural properties of articular cartilage. Osteoarthr. Cartil. 2019, 27, 1481–1490. [Google Scholar] [CrossRef] [Green Version]
- Chan, D.D.; Neu, C.P. Probing articular cartilage damage and disease by quantitative magnetic resonance imaging. J. R. Soc. Interface 2013, 10, 20120608. [Google Scholar] [CrossRef] [PubMed]
- Bittersohl, B.; Hosalkar, H.S.; Miese, F.R.; Schibensky, J.; König, D.P.; Herten, M.; Antoch, G.; Krauspe, R.; Zilkens, C. Zonal T2* and T1 Gd assessment of knee joint cartilage in various histological grades of cartilage degeneration: An Observational in Vitro Study. BMJ Open 2015, 5, e006895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binks, D.A.; Hodgson, R.J.; Ries, M.E.; Foster, R.J.; Smye, S.W.; McGonagle, D.; Radjenovic, A. Quantitative parametric MRI of articular cartilage: A review of progress and open challenges. Br. J. Radiol. 2013, 86, 20120163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Shao, H.; Ma, Y.; Wan, L.; Zhang, Y.; Jiang, J.; Du, J.; Tang, G. Quantitative ultrashort echo time magnetization transfer (UTE-MT) for diagnosis of early cartilage degeneration: Comparison with UTE-T2* and T2 mapping. Quant. Imaging Med. Surg. 2020, 10, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.R.; Williams, A.A.; West, R.V.; Qian, Y.; Fu, F.H.; Do, B.H.; Bruno, S. Quantitative magnetic resonance imaging UTE-T2* mapping of cartilage and meniscus healing after anatomic anterior cruciate ligament reconstruction. Am. J. Sports Med. 2014, 42, 1847–1856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.; Qian, Y.; Bear, D.; Chu, C.R. Assessing degeneration of human articular cartilage with ultra-short echo time (UTE) T2* mapping. Osteoarthr. Cartil. 2010, 18, 539–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titchenal, M.R.; Williams, A.A.; Chehab, E.F.; Asay, J.L.; Dragoo, J.L.; Gold, G.E.; McAdams, T.R.; Andriacchi, T.P.; Chu, C.R. Cartilage sub surface changes to magnetic resonance imaging UTE-T2* 2 years after anterior cruciate ligament reconstruction correlate with walking mechanics associated with knee osteoarthritis. Am. J. Sports Med. 2018, 46, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.A.; Gold, G.E. MR imaging of articular cartilage physiology. Magn. Reson. Imaging Clin. N. Am. 2011, 19, 249–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederauer, G.G.; Niederauer, G.M.; Cullen, L.C., Jr.; Athanasiou, K.A.; Thomas, J.B.; Niederauer, M.Q. Correlation of cartilage stiffness to thickness and level of degeneration using a handheld indentation probe. Ann. Biomed. Eng. 2004, 32, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Appleyard, R.C.; Swain, M.V.; Khanna, S.; Murrel, G.A.C. The accuracy and reliability of a novel handheld dynamic indentation probe for analyzing articular cartilage. Phys. Med. Biol. 2001, 46, 541–550. [Google Scholar] [CrossRef]
- Sim, S.; Chevrier, A.; Garon, M.; Quenneville, E.; Yaroshinsky, A.; Hoemann, C.D.; Buschmann, M.D. Non-destructive electromechan ical assessment (Arthro-BST) of human articular cartilage correlates with histological scores and biomechanical properties. Osteoarthr. Cartil. 2014, 22, 1926–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickevicius, T.; Maciulaitis, J.; Usas, A.; Gudas, R. Quantitative Arthroscopic Assessment of Articular Cartilage Quality by Means of Cartilage Electromechanical Properties. Arthrosc. Tech. 2018, 7, e763–e766. [Google Scholar] [CrossRef] [PubMed]
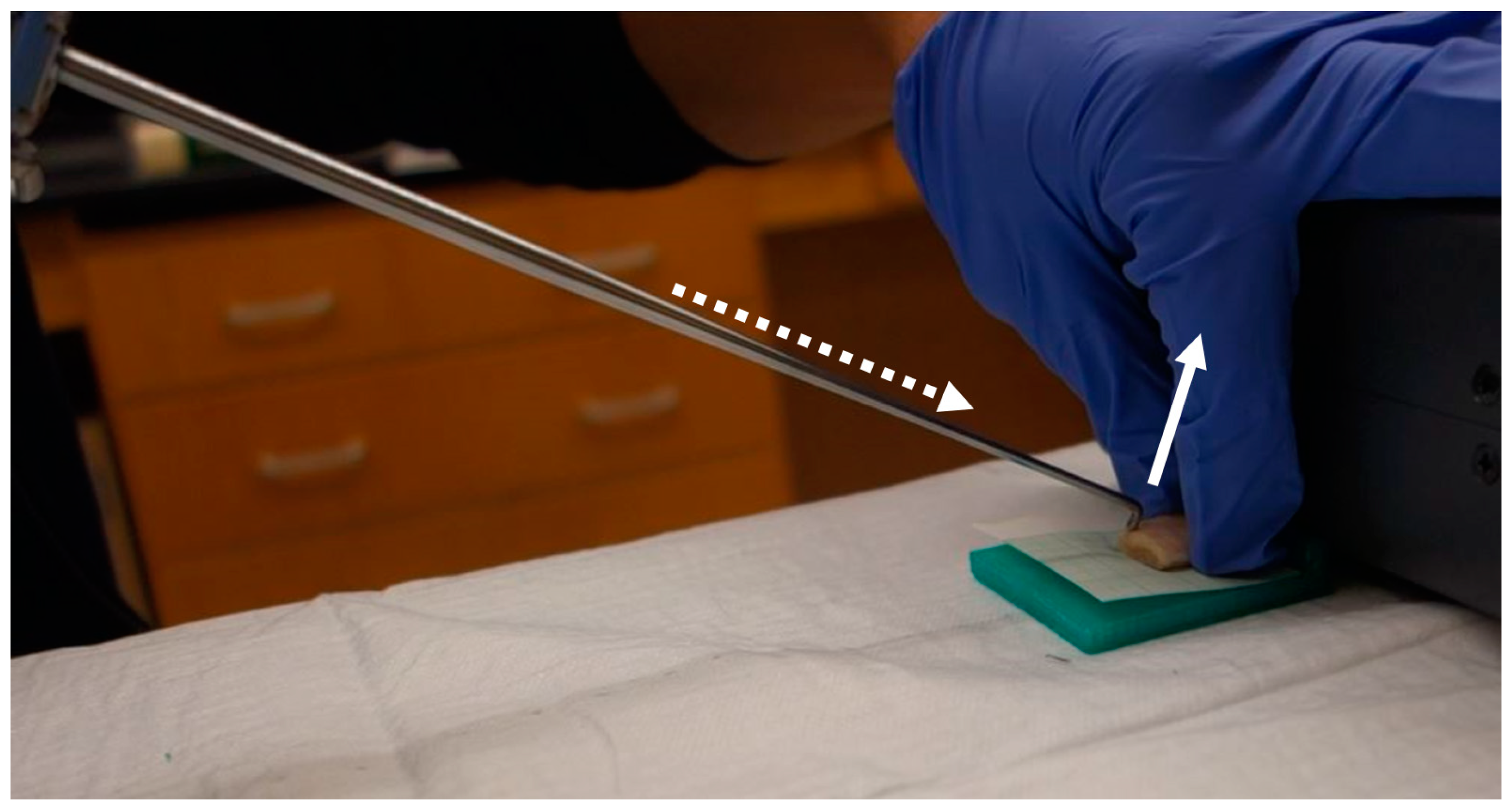
- Hananouchi, T. A probing device for quantitatively measuring the mechanical properties of soft tissues during arthroscopy. J. Vis. Exp. 2020, 159, e60722. [Google Scholar] [CrossRef] [PubMed]
- Hananouchi, T.; Aoki, S.K. Quantitative evaluation of capsular and labral resistances in the hip joint using a instrumented ar throscopic probe. Biomed. Mater. Eng. 2019, 30, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, W.C.; Keer, L.M.; Herrmann, G.; Mockros, L.F. A mathematical analysis for indentation tests of articular cartilage. J. Biomech. 1972, 5, 541–551. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Jerban, S.; Ma, Y.; Dorthe, E.W.; Kakos, L.; Le, N.; Alenezi, S.; Sah, R.L.; Chang, E.Y.; D’Lima, D.; Du, J. Assessing cortical bone mechanical properties using collagen proton fraction from ultrashort echo time magnetization transfer (UTE-MT) MRI modeling. Bone Rep. 2019, 11, 100220. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.Y.; Bae, W.C.; Shao, H.; Biswas, R.; Li, S.; Chen, J.; Patil, S.; Healey, R.; D’Lima, D.D.; Chung, C.B.; et al. Ultrashort echo time magnetization transfer (UTE-MT) imaging of cortical bone. NMR Biomed. 2015, 28, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Cheng, X.; Dorthe, E.W.; Zhao, Y.; D’Lima, D.; Bydder, G.M.; Liu, S.; Du, J.; Ma, Y.J. Evaluation of normal cadaveric Achilles tendon and enthesis with ultrashort echo time (UTE) magnetic resonance imaging and indentation testing. NMR Biomed. 2019, 32, e4034. [Google Scholar] [CrossRef]
- Zhu, Y.; Cheng, X.; Ma, Y.; Wong, J.H.; Xie, Y.; Du, J.; Chang, E.Y. Rotator cuff tendon assessment using magic-angle insensitive 3D ultrashort echo time cones magnetization transfer (UTE-Cones-MT) imaging and modeling with histological correlation. J. Magn. Reson. Imaging 2018, 48, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Jerban, S.; Ma, Y.; Namiranian, B.; Ashir, A.; Shirazian, H.; Wei, Z.; Le, N.; Wu, M.; Cai, Z.; Du, J.; et al. Age-related decrease in collagen proton fraction in tibial tendons estimated by magnetization transfer modeling of ultrashort echo time magnetic resonance imaging (UTE-MRI). Sci. Rep. 2019, 9, 17974. [Google Scholar] [CrossRef] [PubMed]
- Waldschmidt, J.G.; Rilling, R.J.; Kajdacsy-Balla, A.A.; Boynton, M.D.; Erickson, S.J. In vitro and in vivo MR imaging of hyaline cartilage: Zonal anatomy, imaging pitfalls, and pathologic conditions. Radiographics 1997, 17, 1387–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, W.C.; Temple, M.M.; Amiel, D.; Coutts, R.D.; Niederauer, G.G.; Sah, R.L. Indentation testing of human cartilage: Sensitivity to articular surface degeneration. Arthritis Rheum. 2003, 48, 3382–3394. [Google Scholar] [CrossRef] [PubMed]
- Knecht, S.; Vanwanseele, B.; Stüssi, E. A review on the mechanical quality of articular cartilage—Implications for the diagnosis of osteoarthritis. Clin. Biomech. 2006, 21, 999–1012. [Google Scholar] [CrossRef] [PubMed]
- Aroganam, G.; Manivannan, N.; Harrison, D. Review on wearable technology sensors used in consumer sport applications. Sensors 2019, 19, 1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papi, E.; Bo, Y.N.; McGregor, A.H. A flexible wearable sensor for knee flexion assessment during gait. Gait Posture. 2018, 62, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Boddy, K.J.; Marsh, J.A.; Caravan, A.; Lindley, K.E.; Scheffey, J.O.; O’Connell, M.E. Exploring wearable sensors as an alternative to marker-based motion capture in the pitching delivery. PeerJ 2019, 7, e6365. [Google Scholar] [CrossRef] [PubMed]
- Anseth, K.S.; Bowman, C.N.; Brannon-Peppas, L. Mechanical properties of hydrogels and their experimental determination. Biomaterials 1996, 17, 1647–1657. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) |
|---|---|
| Stiffness (N/mm) | 0.30 (0.15) |
| Elastic modulus (MPa) | 0.30 (0.16) |
| UTE-T2* (ms) | 23.18 (7.70) |
| UTE-MTR (%) | 26.76 (3.80) |
| Probing device force (N) | 1.06 (0.30) |
| Variable | Stiffness | Elastic Modulus | UTE-T2* | UTE-MTR | Probing Device Force |
|---|---|---|---|---|---|
| Stiffness | 1.000 | - | - | - | - |
| Elastic modulus | 0.997 | 1.000 | - | - | - |
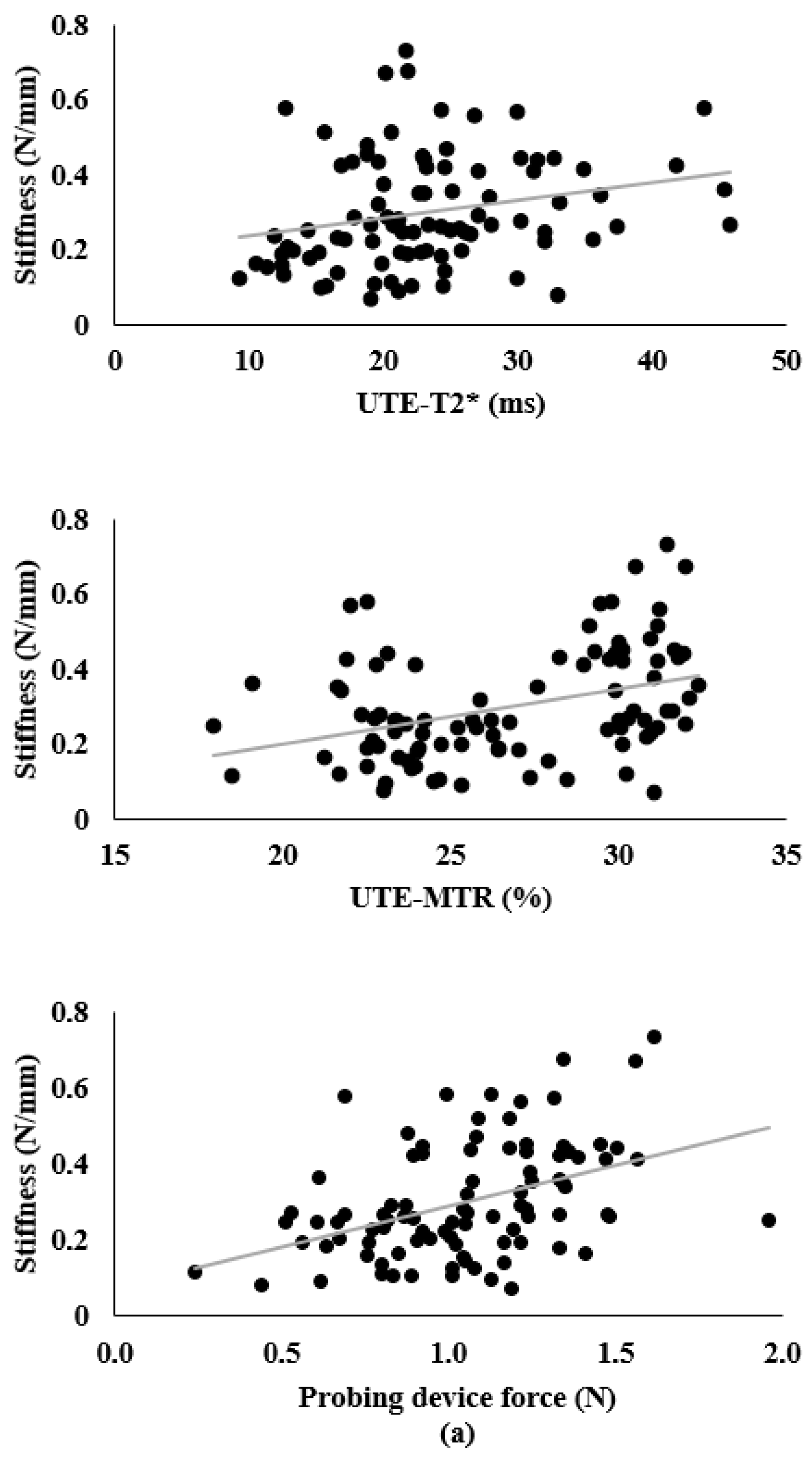
| UTE-T2* | 0.240 | 0.255 | 1.000 | - | - |
| UTE-MTR | 0.378 | 0.379 | −0.174 | 1.000 | - |
| Probing device force | 0.426 | 0.423 | −0.063 | 0.356 | 1.000 |
| Outcome Variable | Predictor | B | 95% CI | p | sr | sr2 |
|---|---|---|---|---|---|---|
| Stiffness a | UTE-T2* | 0.006 | 0.003–0.010 | 0.001 | 0.311 | 0.097 |
| UTE-MTR | 0.012 | 0.005–0.020 | 0.001 | 0.289 | 0.084 | |
| Probing device force | 0.168 | 0.076–0.260 | 0.001 | 0.312 | 0.097 | |
| Intercept | −0.351 | −0.567, −0.135 | 0.002 | - | - | |
| Elastic modulus b | UTE-T2* | 0.007 | 0.003–0.010 | <0.001 | 0.326 | 0.106 |
| UTE-MTR | 0.013 | 0.005–0.021 | 0.001 | 0.294 | 0.086 | |
| Probing device force | 0.173 | 0.077–0.268 | 0.001 | 0.309 | 0.096 | |
| Intercept | −0.387 | −0.610, −0.165 | 0.001 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hananouchi, T.; Chen, Y.; Jerban, S.; Teramoto, M.; Ma, Y.; Dorthe, E.W.; Chang, E.Y.; Du, J.; D’Lima, D.D. A Useful Combination of Quantitative Ultrashort Echo Time MR Imaging and a Probing Device for Biomechanical Evaluation of Articular Cartilage. Biosensors 2021, 11, 52. https://doi.org/10.3390/bios11020052
Hananouchi T, Chen Y, Jerban S, Teramoto M, Ma Y, Dorthe EW, Chang EY, Du J, D’Lima DD. A Useful Combination of Quantitative Ultrashort Echo Time MR Imaging and a Probing Device for Biomechanical Evaluation of Articular Cartilage. Biosensors. 2021; 11(2):52. https://doi.org/10.3390/bios11020052
Chicago/Turabian StyleHananouchi, Takehito, Yanjun Chen, Saeed Jerban, Masaru Teramoto, Yajun Ma, Erik W. Dorthe, Eric Y. Chang, Jiang Du, and Darryl D. D’Lima. 2021. "A Useful Combination of Quantitative Ultrashort Echo Time MR Imaging and a Probing Device for Biomechanical Evaluation of Articular Cartilage" Biosensors 11, no. 2: 52. https://doi.org/10.3390/bios11020052