On Demand Biosensors for Early Diagnosis of Cancer and Immune Checkpoints Blockade Therapy Monitoring from Liquid Biopsy


Abstract
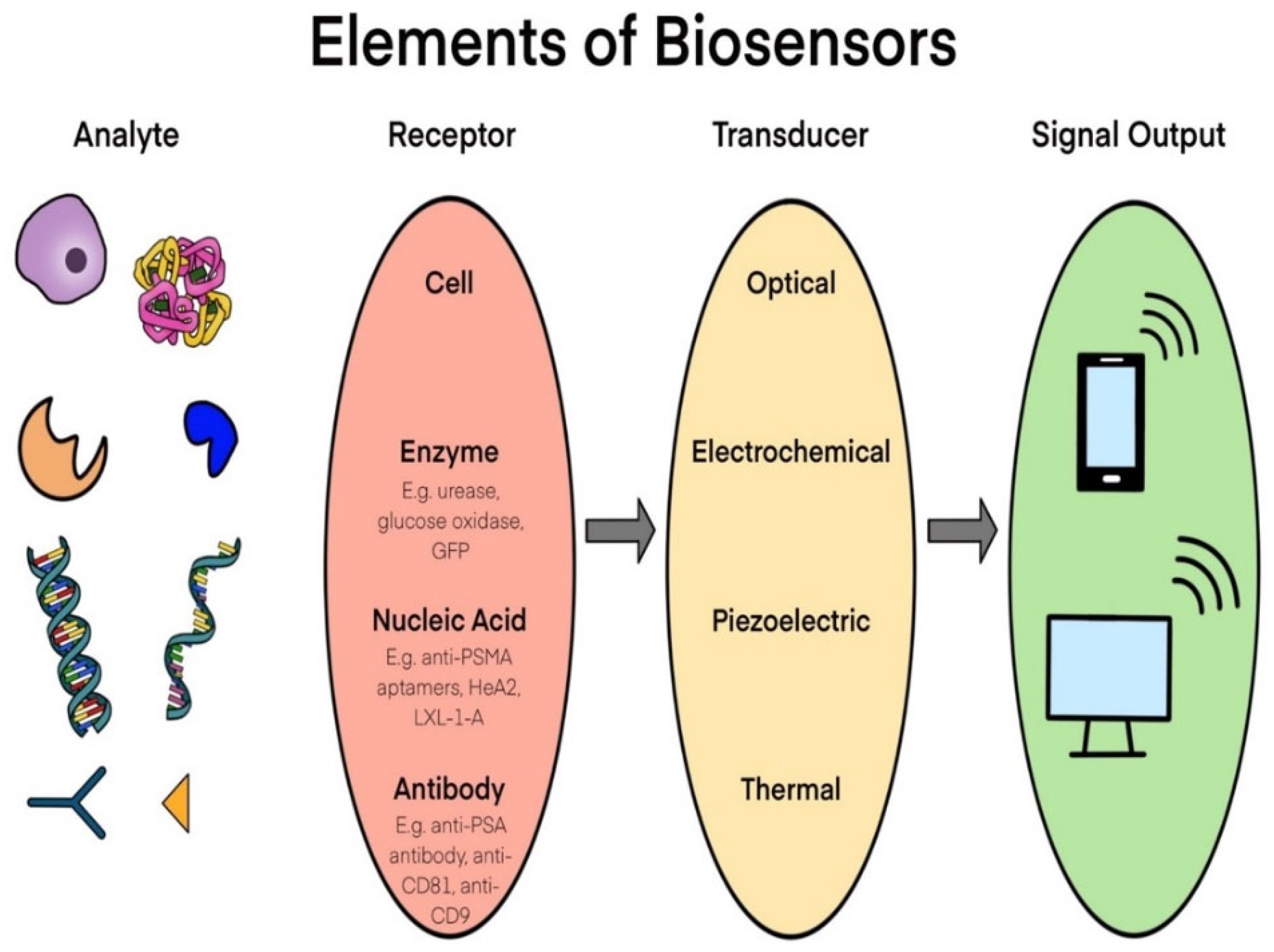
:1. Introduction
2. Key Methods for the Detection of Cancer Biomarkers from Liquid Biopsy
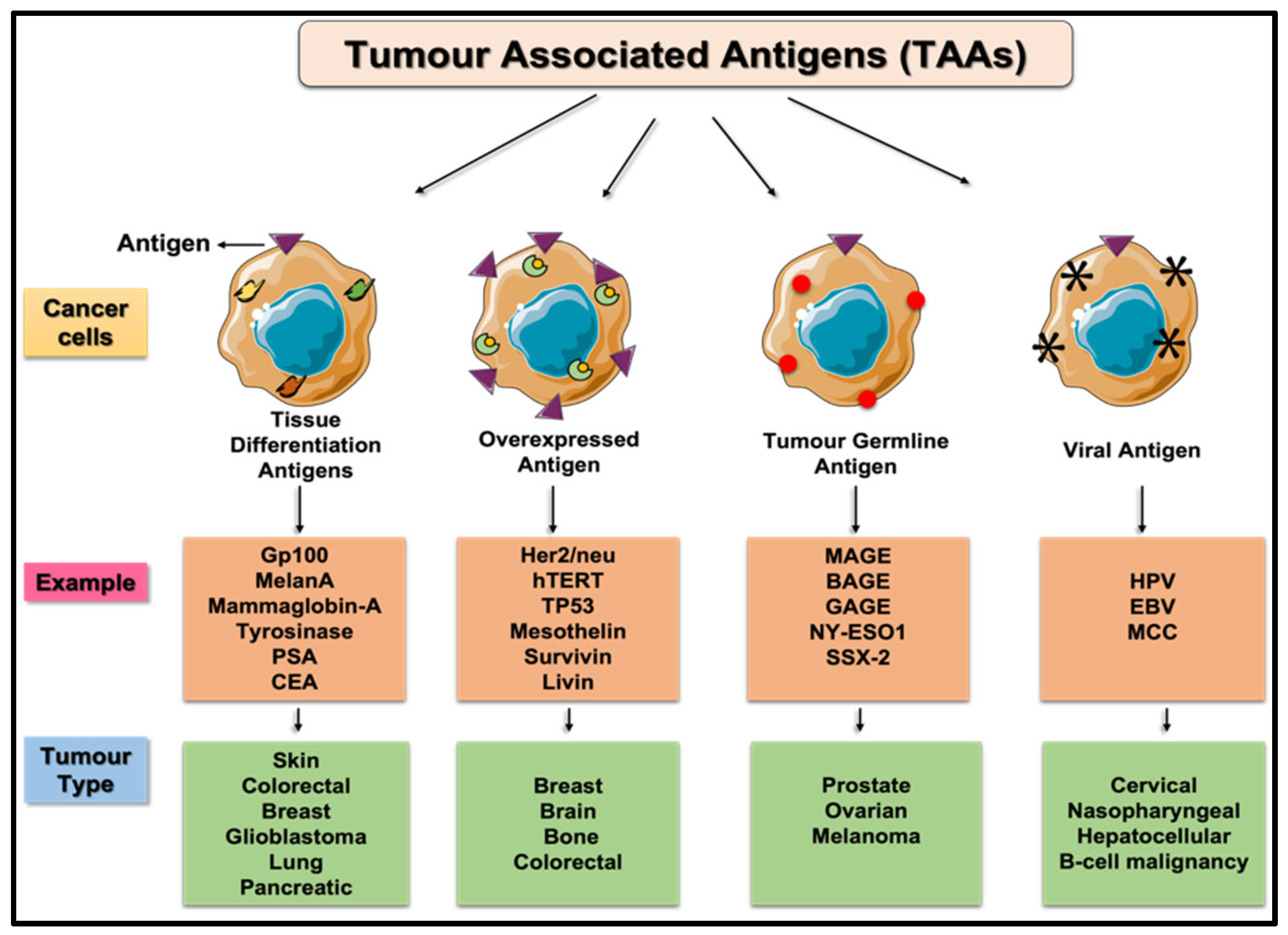
2.1. Tumor-Associated Antigens (TAAs)
2.2. Overexpressing Cancer Biomarkers
2.3. Differentiation Antigens
2.4. Cancer Testis Antigens
2.5. Prostate Specific Antigen (PSA) Based Biosensor
3. Immune Checkpoints as a Marker for Cancer Diagnosis
3.1. T-Cell Immunoglobulin and Mucin Domain-3 (TIM-3)
3.2. B- and T-Lymphocyte Attenuator (BTLA)
3.3. Immune Markers in Serum
3.4. Lymphocyte-Activation Gene 3 (LAG-3)
3.5. PD-1
3.6. PD-L1
4. Biosensors for Cancer Markers and Immune Checkpoint Detection
4.1. Biosensors for Detection of Multiple Cancer/IC Markers
4.2. Exosome Biosensor
4.3. Biosensors for Overall Cancer Immunotherapy
4.4. Biosensors for CRISPR
4.5. Biosensors for ICB: Advantages and Limitations
5. Conclusions and Future Potential of Biosensors for ICB Detection
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AbC | Capture antibody |
| Abs | Second antibody |
| ADAM | A disintegrin and metalloprotease |
| ALP | Alkaline phosphatase |
| BTLA | B- and T- lymphocyte attenuator |
| CEA | Carcinoembryonic antigen |
| CLL | Chronic lymphocytic leukemia |
| CRC | Colorectal cancer |
| CT scan | Computed tomography scan |
| CTC | Circulating tumor cells |
| ctDNA | Circulating tumor DNA |
| CTL | Cytotoxic T lymphocytes |
| CTLA-4 | Cytotoxic T-lymphocyte–associated antigen 4 |
| DLBCL | Diffuse large B-cell lymphoma |
| EC | Electrochemical biosensors |
| EGFR | Epidermal growth factor receptor |
| ELISA | Enzyme-linked immunoassay |
| FRET | Fluorescence resonance energy transfer |
| GSPE-MFD | Gold screen-printed electrode-based microfluidic devices |
| HCC | Hepatocellular carcinoma |
| HER2 | Human epidermal growth factor receptor 2 |
| Hq | Hydroquinone |
| HRP | Horse radish peroxide |
| IC | Immune checkpoints |
| ICB | Immue checkpoint blockade |
| IFN-γ | Interferon gamma |
| IgG | Immunoglobulin G |
| IHC | Immunohistochemistry |
| IL-2 | Interleukin-2 |
| LAG-3 | Lymphocyte activation gene 3 |
| LOD | Limit-of-detection |
| MAGE-A | Melanoma-associated antigen-A |
| MICB | Multiplexed immune checkpoint biosensor |
| MNP | Magnetic nanoparticles |
| MUC1 | Mucin 1 |
| NPC | Nasopharyngeal carcinoma |
| NTME | Non-tumor microenvironment |
| PD-1 | Programmed death 1 |
| PD-L1 | Programmed death-1 ligand |
| PSA | Prostate specific antigen |
| PTC | Papillary thyroid cancer |
| ScFv | Single-chain variable fragment |
| sLAG-3 | Serum lymphocyte activation gene-3 |
| sPD-1 | Serum programmed death-1 |
| sPD-L1 | Serum programmed death-1 ligand |
| SPR | Surface plasmon resonance |
| sTIM-3 | Serum T cell immunoglobulin and mucin-domain containing-3 |
| TAA | Tumor-associated antigen |
| TIM-3 | T cell immunoglobulin and mucin-domain containing-3 |
| TME | Tumor microenvironment |
| TNF-α | Tumor necrosis factor alpha |
| TSA | Tumor-specific antigen |
References
- Tothill, I.E. Biosensors for cancer markers diagnosis. Semin. Cell Dev. Biol. 2009, 20, 55–62. [Google Scholar] [CrossRef]
- Cheng, N.; Du, D.; Wang, X.; Liu, D.; Xu, W.; Luo, Y. Recent Advances in Biosensors for Detecting Cancer-Derived Exosomes. Trends Biotechnol. 2019, 37, 1236–1254. [Google Scholar] [CrossRef]
- Naresh, V.; Lee, N. A Review on Biosensors and Recent Development of Nanostructured Materials-Enabled Biosensors. Sensors 2021, 21, 1109. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra Biosensors and their applications—A review. J. Oral. Biol. Craniofac. Res. 2016, 6, 153–159. [CrossRef] [Green Version]
- Soler, M.; Lechuga, L.M. Principles, technologies, and applications of plasmonic biosensors. J. Appl. Physics 2021, 129, 111102. [Google Scholar] [CrossRef]
- Chen, Y.T.; Lee, Y.C.; Lai, Y.H.; Lim, J.C.; Huang, N.T.; Lin, C.T.; Huang, N.T. Review of Integrated Optical Biosensors for Point-Of-Care Applications. Biosensors 2020, 10, 209. [Google Scholar] [CrossRef]
- Liu, D.; Wang, J.; Wu, L.; Huang, Y.; Zhang, Y.; Zhu, M.; Wang, Y.; Zhu, Z.; Yang, C. Trends in miniaturized biosensors for point-of-care testing. TrAC Trends Anal. Chem. 2020, 122, 115701. [Google Scholar] [CrossRef]
- Dey, D.; Goswami, T. Optical biosensors: A revolution towards quantum nanoscale electronics device fabrication. J. Biomed. Biotechnol. 2011, 2011, 348218. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Xiao, W.; Li, G.; Wu, P.; He, Y.; Chen, C.; He, Y.; Ding, P.; Kai, T. The research of aptamer biosensor technologies for detection of microorganism. Appl. MicroBiol. Biotechnol. 2020, 104, 9877–9890. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Chou, W.; Liu, L.; Cui, Y.; Xue, P.; Jia, M. Electrochemical Sensors Fabricated by Electrospinning Technology: An Overview. Sensors 2019, 19, 3676. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Boo, H.; Chung, T.D. Electrochemical non-enzymatic glucose sensors. Anal. Chim. Acta 2006, 556, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Kilgour, E.; Rothwell, D.G.; Brady, G.; Dive, C. Liquid Biopsy-Based Biomarkers of Treatment Response and Resistance. Cancer Cell 2020, 37, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Hollingsworth, R.E.; Jansen, K. Turning the corner on therapeutic cancer vaccines. NPJ Vaccines 2019, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Briones, J.; Espulgar, W.; Koyama, S.; Takamatsu, H.; Tamiya, E.; Saito, M. The future of microfluidics in immune checkpoint blockade. Cancer Gene Ther. 2021, 28, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Theobald, M.; Biggs, J.; Dittmer, D.; Levine, A.J.; Sherman, L.A. Targeting p53 as a general tumor antigen. Proc. Natl. Acad. Sci. USA 1995, 92, 11993–11997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casiano, C.A.; Mediavilla-Varela, M.; Tan, E.M. Tumor-associated antigen arrays for the serological diagnosis of cancer. Mol. Cell Proteomics 2006, 5, 1745–1759. [Google Scholar] [CrossRef] [Green Version]
- Rangel, M.G.H.; Silva, M.L.S. Detection of the cancer-associated T antigen using an Arachis hypogea agglutinin biosensor. Biosens Bioelectron. 2019, 141, 111401. [Google Scholar] [CrossRef]
- Kufe, D.W. MUC1-C oncoprotein as a target in breast cancer: Activation of signaling pathways and therapeutic approaches. Oncogene 2013, 32, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, N.; Iqbal, N. Human Epidermal Growth Factor Receptor 2 (HER2) in Cancers: Overexpression and Therapeutic Implications. Mol. Biol. Int. 2014, 2014, 1–9. [Google Scholar] [CrossRef]
- Gutierrez, C.; Schiff, R. HER2: Biology, detection, and clinical implications. Arch. Pathol. Lab. Med. 2011, 135, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Kallioniemi, O.P.; Kallioniemi, A.; Kurisu, W.; Thor, A.; Chen, L.C.; Smith, H.S.; Waldman, F.M.; Pinkel, D.; Gray, J.W. ERBB2 amplification in breast cancer analyzed by fluorescence in situ hybridization. Proc. Natl. Acad. Sci. USA 1992, 89, 5321–5325. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Schreurs, M.W.; de Boer, A.J.; Kawakami, Y.; Rosenberg, S.A.; Adema, G.J.; Figdor, C.G. Melanocyte lineage-specific antigen gp100 is recognized by melanoma-derived tumor-infiltrating lymphocytes. J. Exp. Med. 1994, 179, 1005–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, W.K.; Choi, D.H.; Park, H.C.; Park, W.; Yu, J.I.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Kim, H.C.; Cho, Y.B.; et al. Elevated CEA is associated with worse survival in recurrent rectal cancer. Oncotarget 2017, 8, 105936–105941. [Google Scholar] [CrossRef] [Green Version]
- Tsikitis, V.L.; Malireddy, K.; Green, E.A.; Christensen, B.; Whelan, R.; Hyder, J.; Marcello, P.; Larach, S.; Lauter, D.; Sargent, D.J.; et al. Postoperative surveillance recommendations for early stage colon cancer based on results from the clinical outcomes of surgical therapy trial. J. Clin. Oncol. 2009, 27, 3671–3676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, R.H.Z.; Liu, N.; Gao, F.; Luo, X. Electrochemical biosensors for the detection of carcinoembryonic antigenwith low fouling and high sensitivity based on copolymerized polydopamineand zwitterionic polymer. Sens. Actuators B Chem. 2020, 319, 128253. [Google Scholar] [CrossRef]
- Gjerstorff, M.F.; Andersen, M.H.; Ditzel, H.J. Oncogenic cancer/testis antigens: Prime candidates for immunotherapy. Oncotarget 2015, 6, 15772–15787. [Google Scholar] [CrossRef] [Green Version]
- Park, T.S.; Groh, E.M.; Patel, K.; Kerkar, S.P.; Lee, C.C.; Rosenberg, S.A. Expression of MAGE-A and NY-ESO-1 in Primary and Metastatic Cancers. J. Immunother. 2016, 39, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Salimi, A.; Kavosi, B.; Fathi, F.; Hallaj, R. Highly sensitive immunosensing of prostate-specific antigen based on ionic liquid-carbon nanotubes modified electrode: Application as cancer biomarker for prostate biopsies. Biosens. Bioelectron. 2013, 42, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Kavosi, B.; Salimi, A.; Hallaj, R.; Amani, K. A highly sensitive prostate-specific antigen immunosensor based on gold nanoparticles/PAMAM dendrimer loaded on MWCNTS/chitosan/ionic liquid nanocomposite. Biosens. Bioelectron. 2014, 52, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Damborska, D.; Bertok, T.; Dosekova, E.; Holazova, A.; Lorencova, L.; Kasak, P.; Tkac, J. Nanomaterial-based biosensors for detection of prostate specific antigen. Mikrochim. Acta 2017, 184, 3049–3067. [Google Scholar] [CrossRef] [PubMed]
- Luo, B.; Wang, Y.; Lu, H.; Wu, S.; Lu, Y.; Shi, S.; Li, L.; Jiang, S.; Zhao, M. Label-free and specific detection of soluble programmed death ligand-1 using a localized surface plasmon resonance biosensor based on excessively tilted fiber gratings. Biomed. Opt. Express 2019, 10, 5136–5148. [Google Scholar] [CrossRef]
- Helmerhorst, D.J.C.E.; Nussio, M.; Mamotte, C.D. Real-time and Label-free Bio-sensing of Molecular Interactions by Surface Plasmon Resonance: A Laboratory Medicine Perspective. Clin. Biochem. Rev. 2012, 33, 161–173. [Google Scholar]
- Luo, B.; Wang, Y.; Lu, H.; Wu, S.; Lu, Y.; Shi, S.; Li, L.; Jiang, S.; Zhao, M. Localized surface plasmon resonance based nanobiosensor for biomarker detection of invasive cancer cells. J. Biomed. Opt. 2014, 19, 51202. [Google Scholar]
- Chen, J.S.; Chen, P.F.; Lin, H.T.; Huang, N.T. A Localized surface plasmon resonance (LSPR) sensor integrated automated microfluidic system for multiplex inflammatory biomarker detection. Analyst 2020, 145, 7654–7661. [Google Scholar] [CrossRef]
- Khanmohammadi, A.; Aghaie, A.; Vahedi, E.; Qazvini, A.; Ghanei, M.; Afkhami, A.; Hajian, A.; Bagheri, H. Electrochemical biosensors for the detection of lung cancer biomarkers: A review. Talanta 2020, 206, 120251. [Google Scholar] [CrossRef]
- Jalil, O.; Pandey, C.M.; Kumar, D. Electrochemical biosensor for the epithelial cancer biomarker EpCAM based on reduced graphene oxide modified with nanostructured titanium dioxide. Mikrochim. Acta 2020, 187, 275. [Google Scholar] [CrossRef] [PubMed]
- El Aamri, M.; Yammouri, G.; Mohammadi, H.; Amine, A.; Korri-Youssoufi, H. Electrochemical Biosensors for Detection of MicroRNA as a Cancer Biomarker: Pros and Cons. Biosensors 2020, 10, 186. [Google Scholar] [CrossRef]
- Gajdosova, V.; Lorencova, L.; Kasak, P.; Tkac, J. Electrochemical Nanobiosensors for Detection of Breast Cancer Biomarkers. Sensors 2020, 20, 4022. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Zhu, A.; Xu, Q.; Chen, Y.; Xu, J.; Weng, J. Colorimetric Biosensor for Detection of Cancer Biomarker by Au Nanoparticle-Decorated Bi2Se3 Nanosheets. ACS Appl. Mater. Interfaces 2017, 9, 6931–6940. [Google Scholar] [CrossRef]
- Cai, J.; Ding, L.; Gong, P.; Huang, J. A colorimetric detection of microRNA-148a in gastric cancer by gold nanoparticle-RNA conjugates. Nanotechnology 2020, 31, 95501. [Google Scholar] [CrossRef] [PubMed]
- Mollasalehi, H.; Shajari, E. A colorimetric nano-biosensor for simultaneous detection of prevalent cancers using unamplified cell-free ribonucleic acid biomarkers. Bioorg. Chem. 2021, 107, 104605. [Google Scholar] [CrossRef]
- Wuethrich, A.; Rajkumar, A.R.; Shanmugasundaram, K.B.; Reza, K.K.; Dey, S.; Howard, C.B.; Sina, A.A.; Trau, M. Single droplet detection of immune checkpoints on a multiplexed electrohydrodynamic biosensor. Analyst 2019, 144, 6914–6921. [Google Scholar] [CrossRef]
- Cho, S.; Yang, H.C.; Rhee, W.J. Simultaneous multiplexed detection of exosomal microRNAs and surface proteins for prostate cancer diagnosis. Biosens. Bioelectron. 2019, 146, 111749. [Google Scholar] [CrossRef]
- Wei, X.; Bian, F.; Cai, X.; Wang, Y.; Cai, L.; Yang, J.; Zhu, Y.; Zhao, Y. Multiplexed Detection Strategy for Bladder Cancer MicroRNAs Based on Photonic Crystal Barcodes. Anal. Chem. 2020, 92, 6121–6127. [Google Scholar] [CrossRef]
- Traynor, S.M. Recent Advances in Electrochemical Detection of Prostate Specific Antigen (PSA) in Clinically-Relevant Samples. J. Electrochem. Soc. 2020, 167, 037551. [Google Scholar] [CrossRef]
- Li, H.; Li, S.; Xia, F. Biosensors Based on Sandwich Assays; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Neupane, D.; Stine, K.J. Electrochemical Sandwich Assays for Biomarkers Incorporating Aptamers, Antibodies and Nanomaterials for Detection of Specific Protein Biomarkers. Appl. Sci. 2021, 11, 7087. [Google Scholar] [CrossRef]
- Chen, S.; Wang, Z.; Cui, X.; Jiang, L.; Zhi, Y.; Ding, X.; Nie, Z.; Zhou, P.; Cui, D. Microfluidic Device Directly Fabricated on Screen-Printed Electrodes for Ultrasensitive Electrochemical Sensing of PSA. Nanoscale Res. Lett. 2019, 14, 71. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Laschi, S.; Mascini, M.; Marrazza, G. A New Electrochemical Multiplexed Assay for PSA Cancer Marker Detection. Electroanalysis 2011, 23, 91. [Google Scholar] [CrossRef]
- Niu, X.; Cheng, N.; Ruan, X.; Du, D.; Lin, Y. Nanozyme-Based Immunosensors and Immunoassays: Recent Developments and Future Trends. J. Electrochem. Soc. 2020, 167, 37508. [Google Scholar] [CrossRef]
- Robert, C. A decade of immune-checkpoint inhibitors in cancer therapy. Nat. Commun. 2020, 11, 3801. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable Complete Response After Discontinuation of Pembrolizumab in Patients with Metastatic Melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of Indications of FDA-Approved Immune Checkpoint Inhibitors per NCCN Guidelines with the Level of Evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef] [Green Version]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef]
- Shibru, B.; Fey, K.; Fricke, S.; Blaudszun, A.R.; Furst, F.; Weise, M.; Seiffert, S.; Weyh, M.K.; Kohl, U.; Sack, U.; et al. Detection of Immune Checkpoint Receptors—A Current Challenge in Clinical Flow Cytometry. Front. Immunol. 2021, 12, 694055. [Google Scholar] [CrossRef]
- Wolf, Y.; Anderson, A.C.; Kuchroo, V.K. TIM3 comes of age as an inhibitory receptor. Nat. Rev. Immunol. 2020, 20, 173–185. [Google Scholar] [CrossRef]
- Acharya, N.; Sabatos-Peyton, C.; Anderson, A.C. Tim-3 finds its place in the cancer immunotherapy landscape. J. Immunother. Cancer 2020, 8, e000911. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, H.; Kane, L.P. Immune regulation by Tim-3. F1000 Res. 2018, 7, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Liu, C.; Qian, S.; Hou, H. The expression of Tim-3 in peripheral blood of ovarian cancer. DNA Cell Biol. 2013, 32, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhi, L.; Duan, N.; Su, P. Abnormal expression of Tim-3 antigen on peripheral blood T cells is associated with progressive disease in osteosarcoma patients. FEBS Open Biol. 2016, 6, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Zhang, X.H.; Hu, X.D.; Liu, P.D.; Zhang, H.Q. The effects of combined selenium nanoparticles and radiation therapy on breast cancer cells in vitro. Artif. Cells Nanomed. Biotechnol. 2018, 46, 937–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Zheng, Y.; Mao, R.; Su, Z.; Zhang, J. BTLA/HVEM Signaling: Milestones in Research and Role in Chronic Hepatitis B Virus Infection. Front. Immunol. 2019, 10, 617. [Google Scholar] [CrossRef]
- Deng, Z.; Zheng, Y.; Cai, P.; Zheng, Z. The Role of B and T Lymphocyte Attenuator in Respiratory System Diseases. Front. Immunol. 2021, 12, 635623. [Google Scholar] [CrossRef]
- Lan, X.; Li, S.; Gao, H.; Nanding, A.; Quan, L.; Yang, C.; Ding, S.; Xue, Y. Increased BTLA and HVEM in gastric cancer are associated with progression and poor prognosis. Onco Targets Ther. 2017, 10, 919–926. [Google Scholar] [CrossRef] [Green Version]
- König, B.; Grätzel, M. An immunosensor for the detection of human B-lymphocytes. Bioorg. Med. Chem. Lett. 1994, 4, 2429–2434. [Google Scholar] [CrossRef]
- Carinelli, S.; Ballesteros, C.X.; Marti, M.; Alegret, S.; Pividori, M.I. Electrochemical magneto-actuated biosensor for CD4 count in AIDS diagnosis and monitoring. Biosens. Bioelectron. 2015, 74, 974–980. [Google Scholar] [CrossRef]
- Kim, J.; Park, G.; Lee, S.; Hwang, S.W.; Min, N.; Lee, K.M. Single wall carbon nanotube electrode system capable of quantitative detection of CD4(+) T cells. Biosens. Bioelectron. 2017, 90, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cai, H.H.; Zhang, L.; Cai, J.; Yang, P.H.; Chen, Z.W. A novel gold nanoparticle-doped polyaniline nanofibers-based cytosensor confers simple and efficient evaluation of T-cell activation. Biosens. Bioelectron. 2013, 50, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Andrews, L.P.; Marciscano, A.E.; Drake, C.G.; Vignali, D.A. LAG3 (CD223) as a cancer immunotherapy target. Immunol. Rev. 2017, 276, 80–96. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Wang, Y.; Zhao, S.; Zhao, C.; Zhou, C.; Hirsch, F.R. sLAG-3 in non-small-cell lung cancer patients’ serum. Oncol. Targets Ther. 2018, 11, 4781–4784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Jilisihan, B.; Wang, W.; Tang, Y.; Keyoumu, S. Soluble LAG3 acts as a potential prognostic marker of gastric cancer and its positive correlation with CD8+T cell frequency and secretion of IL-12 and INF-gamma in peripheral blood. Cancer Biomark 2018, 23, 341–351. [Google Scholar] [CrossRef]
- Triebel, F.; Hacene, K.; Pichon, M.F. A soluble lymphocyte activation gene-3 (sLAG-3) protein as a prognostic factor in human breast cancer expressing estrogen or progesterone receptors. Cancer Lett. 2006, 235, 147–153. [Google Scholar] [CrossRef]
- Ugurel, S.; Schadendorf, D.; Horny, K.; Sucker, A.; Schramm, S.; Utikal, J.; Pfohler, C.; Herbst, R.; Schilling, B.; Blank, C.; et al. Elevated baseline serum PD-1 or PD-L1 predicts poor outcome of PD-1 inhibition therapy in metastatic melanoma. Ann. Oncol. 2020, 31, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.; Zhao, Z.; Arooj, S.; Fu, Y.; Liao, G. Soluble PD-1: Predictive, Prognostic, and Therapeutic Value for Cancer Immunotherapy. Front. Immunol. 2020, 11, 587460. [Google Scholar] [CrossRef]
- Li, Y.; Cui, X.; Yang, Y.J.; Chen, Q.Q.; Zhong, L.; Zhang, T.; Cai, R.L.; Miao, J.Y.; Yu, S.C.; Zhang, F. Serum sPD-1 and sPD-L1 as Biomarkers for Evaluating the Efficacy of Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients. Clin. Breast Cancer 2019, 19, 326–332.e1. [Google Scholar] [CrossRef]
- Romero, Y.; Wise, R.; Zolkiewska, A. Proteolytic processing of PD-L1 by ADAM proteases in breast cancer cells. Cancer Immunol. Immunother. 2020, 69, 43–55. [Google Scholar] [CrossRef]
- Aghajani, M.J.; Roberts, T.L.; Yang, T.; McCafferty, C.E.; Caixeiro, N.J.; De Souza, P.; Niles, N. Elevated levels of soluble PD-L1 are associated with reduced recurrence in papillary thyroid cancer. Endocr. Connect. 2019, 8, 1040–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, I.; Lee, H.; Yoon, S.E.; Ryu, K.J.; Ko, Y.H.; Kim, W.S.; Kim, S.J. Serum levels of soluble programmed death-ligand 1 (sPD-L1) in patients with primary central nervous system diffuse large B-cell lymphoma. BMC Cancer 2020, 20, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller-Hackbarth, K.; Dewitz, C.; Schweigert, O.; Trad, A.; Garbers, C.; Rose-John, S.; Scheller, J. A disintegrin and metalloprotease (ADAM) 10 and ADAM17 are major sheddases of T cell immunoglobulin and mucin domain 3 (Tim-3). J. Biol. Chem. 2013, 288, 34529–34544. [Google Scholar] [CrossRef] [Green Version]
- Ge, W.; Li, J.; Fan, W.; Xu, D.; Sun, S. Tim-3 as a diagnostic and prognostic biomarker of osteosarcoma. Tumour Biol. 2017, 39, 1010428317715643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Li, N.; Sang, J.; Fan, X.; Deng, H.; Zhang, X.; Han, Q.; Lv, Y.; Liu, Z. Highly elevated soluble Tim-3 levels correlate with increased hepatocellular carcinoma risk and poor survival of hepatocellular carcinoma patients in chronic hepatitis B virus infection. Cancer Manag Res. 2018, 10, 941–951. [Google Scholar] [CrossRef] [Green Version]
- Kangas, M.J.; Burks, R.M.; Atwater, J.; Lukowicz, R.M.; Williams, P.; Holmes, A.E. Colorimetric Sensor Arrays for the Detection and Identification of Chemical Weapons and Explosives. Crit. Rev. Anal. Chem. 2017, 47, 138–153. [Google Scholar] [CrossRef] [Green Version]
- Menon, S.; Mathew, M.R.; Sam, S.; Keerthi, K.; Kumar, K.G. Recent advances and challenges in electrochemical biosensors for emerging and re-emerging infectious diseases. J. Electroana.l Chem. 2020, 878, 114596. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 Checkpoint Signaling Inhibition for Cancer Immunotherapy: Mechanism, Combinations, and Clinical Outcome. Front. Pharmacol. 2017, 8, 561. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in cancer immunotherapy: Clinical implications and future considerations. Hum. Vaccin. Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef]
- Kruger, S.; Legenstein, M.L.; Rosgen, V.; Haas, M.; Modest, D.P.; Westphalen, C.B.; Ormanns, S.; Kirchner, T.; Heinemann, V.; Holdenrieder, S.; et al. Serum levels of soluble programmed death protein 1 (sPD-1) and soluble programmed death ligand 1 (sPD-L1) in advanced pancreatic cancer. Oncoimmunology 2017, 6, e1310358. [Google Scholar] [CrossRef]
- Cunningham, R.A.; Holland, M.; McWilliams, E.; Hodi, F.S.; Severgnini, M. Detection of clinically relevant immune checkpoint markers by multicolor flow cytometry. J. Biol. Methods 2019, 6, e114. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Ye, X.; Cui, T. Recent Progress of Biomarker Detection Sensors. Research 2020, 2020, 7949037. [Google Scholar] [CrossRef] [PubMed]
- Azmi, A.S.; Bao, B.; Sarkar, F.H. Exosomes in cancer development, metastasis, and drug resistance: A comprehensive review. Cancer Metastasis Rev. 2013, 32, 623–642. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Zeng, X.; An, Z.; Yang, Y.; Eisenbaum, M.; Gu, X.; Jornet, J.M.; Dy, G.K.; Reid, M.E.; Gan, Q.; et al. Sensitive Detection of Exosomal Proteins via a Compact Surface Plasmon Resonance Biosensor for Cancer Diagnosis. ACS Sens. 2018, 3, 1471–1479. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, M.; Nardin, C.; Chanteloup, G.; Derangere, V.; Algros, M.P.; Arnould, L.; Garrido, C.; Aubin, F.; Gobbo, J. Tracking the evolution of circulating exosomal-PD-L1 to monitor melanoma patients. J. Extracell Vesicles 2020, 9, 1710899. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Soler, M.; Szydzik, C.; Khoshmanesh, K.; Schmidt, J.; Coukos, G.; Mitchell, A.; Altug, H. Label-Free Optofluidic Nanobiosensor Enables Real-Time Analysis of Single-Cell Cytokine Secretion. Small 2018, 14, e1800698. [Google Scholar] [CrossRef]
- Dutta, N.; Lillehoj, P.B.; Estrela, P.; Dutta, G. Electrochemical Biosensors for Cytokine Profiling: Recent Advancements and Possibilities in the Near Future. Biosensors 2021, 11, 94. [Google Scholar] [CrossRef]
- Oh, B.R.; Huang, N.T.; Chen, W.; Seo, J.H.; Chen, P.; Cornell, T.T.; Shanley, T.P.; Fu, J.; Kurabayashi, K. Integrated nanoplasmonic sensing for cellular functional immunoanalysis using human blood. ACS Nano 2014, 8, 2667–2676. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Wang, J.; Liu, G. CRISPR/Cas Systems towards Next-Generation Biosensing. Trends Biotechnol. 2019, 37, 730–743. [Google Scholar] [CrossRef]
- Mukama, O.; Wu, J.; Li, Z.; Liang, Q.; Yi, Z.; Lu, X.; Liu, Y.; Liu, Y.; Hussain, M.; Makafe, G.G.; et al. An ultrasensitive and specific point-of-care CRISPR/Cas12 based lateral flow biosensor for the rapid detection of nucleic acids. Biosens. Bioelectron. 2020, 159, 112143. [Google Scholar] [CrossRef]
- Bruch, R.; Baaske, J.; Chatelle, C.; Meirich, M.; Madlener, S.; Weber, W.; Dincer, C.; Urban, G.A. CRISPR/Cas13a-Powered Electrochemical Microfluidic Biosensor for Nucleic Acid Amplification-Free miRNA Diagnostics. Adv. Mater. 2019, 31, e1905311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadana, A. Market Size and Economics for Biosensors. In Fractal Binding and Dissociation Kinetics for Different Biosensor Applications; Elsevier: Amsterdam, The Netherlands, 2005; pp. 265–299. [Google Scholar]
- Tchou, J.; Lam, L.; Li, Y.R.; Edwards, C.; Ky, B.; Zhang, H. Monitoring serum HER2 levels in breast cancer patients. Springerplus 2015, 4, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Jung, S.Y.; Kang, S.H.; Song, E.J.; Park, I.H.; Kong, S.Y.; Kwon, Y.M.; Lee, K.S.; Kang, H.S.; Lee, E.S. The Significance of Serum HER2 Levels at Diagnosis on Intrinsic Subtype-Specific Outcome of Operable Breast Cancer Patients. PLoS ONE 2016, 11, e0163370. [Google Scholar] [CrossRef]
- Leyland-Jones, B.; Smith, B.R. Serum HER2 testing in patients with HER2-positive breast cancer: The death knell tolls. Lancet Oncol. 2011, 12, 286–295. [Google Scholar] [CrossRef]
- Lee, J.S.; Park, S.; Park, J.M.; Cho, J.H.; Kim, S.I.; Park, B.W. Elevated levels of serum tumor markers CA 15-3 and CEA are prognostic factors for diagnosis of metastatic breast cancers. Breast Cancer Res. Treat. 2013, 141, 477–484. [Google Scholar] [CrossRef]
- Fakhari, A.; Gharepapagh, E.; Dabiri, S.; Gilani, N. Correlation of cancer antigen 15-3 (CA15-3) serum level and bony metastases in breast cancer patients. Med. J. Islam Repub. Iran 2019, 33, 142. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Sun, X.; He, Y.; Liu, C.; Liu, H. Elevated Levels of Serum Tumor Markers CEA and CA15-3 Are Prognostic Parameters for Different Molecular Subtypes of Breast Cancer. PLoS ONE 2015, 10, e0133830. [Google Scholar] [CrossRef] [PubMed]
- Loo, L.; Capobianco, J.A.; Wu, W.; Gao, X.; Shih, W.Y.; Shih, W.H.; Pourrezaei, K.; Robinson, M.K.; Adams, G.P. Highly sensitive detection of HER2 extracellular domain in the serum of breast cancer patients by piezoelectric microcantilevers. Anal. Chem. 2011, 83, 3392–3397. [Google Scholar] [CrossRef] [Green Version]
- Scambia, G.; Panici, P.B.; Baiocchi, G.; Perrone, L.; Greggi, S.; di Roberto, P.; Mancuso, S. CA 15-3 serum levels in ovarian cancer. Oncology 1988, 45, 263–267. [Google Scholar] [CrossRef]
- Scambia, G.; Panici, P.B.; Baiocchi, G.; Perrone, L.; Greggi, S.; Mancuso, S. CA 15-3 as a tumor marker in gynecological malignancies. Gynecol. Oncol. 1988, 30, 265–273. [Google Scholar] [CrossRef]
- Charkhchi, P.; Cybulski, C.; Gronwald, J.; Wong, F.O.; Narod, S.A.; Akbari, M.R. CA125 and Ovarian Cancer: A Comprehensive Review. Cancers 2020, 12, 3730. [Google Scholar] [CrossRef]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and algorithms for diagnosis of ovarian cancer: CA125, HE4, RMI and ROMA, a review. J. Ovarian Res. 2019, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nan, J.; Li, J.; Li, X.; Guo, G.; Wen, X.; Tian, Y. Preoperative Serum Carcinoembryonic Antigen as a Marker for Predicting the Outcome of Three Cancers. Biomark. Cancer 2017, 9, 1–7. [Google Scholar] [CrossRef]
- Meng, Q.; Shi, S.; Liang, C.; Liang, D.; Xu, W.; Ji, S.; Zhang, B.; Ni, Q.; Xu, J.; Yu, X. Diagnostic and prognostic value of carcinoembryonic antigen in pancreatic cancer: A systematic review and meta-analysis. Oncol. Targets Ther. 2017, 10, 4591–4598. [Google Scholar] [CrossRef] [Green Version]
- Ballehaninna, U.K.; Chamberlain, R.S. Serum CA 19-9 as a Biomarker for Pancreatic Cancer-A Comprehensive Review. Indian J. Surg. Oncol. 2011, 2, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Poruk, K.E.; Gay, D.Z.; Brown, K.; Mulvihill, J.D.; Boucher, K.M.; Scaife, C.L.; Firpo, M.A.; Mulvihill, S.J. The clinical utility of CA 19-9 in pancreatic adenocarcinoma: Diagnostic and prognostic updates. Curr. Mol. Med. 2013, 13, 340–351. [Google Scholar]
- Haglund, C. Tumour marker antigen CA125 in pancreatic cancer: A comparison with CA19-9 and CEA. Br. J. Cancer 1986, 54, 897–901. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Xu, H.X.; Wang, W.Q.; Wu, C.T.; Xiang, J.F.; Liu, C.; Long, J.; Xu, J.; Fu, L.; Ni, Q.X. Serum CA125 is a novel predictive marker for pancreatic cancer metastasis and correlates with the metastasis-associated burden. Oncotarget 2016, 7, 5943–5956. [Google Scholar] [CrossRef] [Green Version]
- Penney, D.G.; Weeks, T.A. Age dependence of cardiac growth in the normal and carbon monoxide-exposed rat. Dev. Biol. 1979, 71, 153–162. [Google Scholar] [CrossRef]
- Shi, H.Z.; Wang, Y.N.; Huang, X.H.; Zhang, K.C.; Xi, H.Q.; Cui, J.X.; Liu, G.X.; Liang, W.T.; Wei, B.; Chen, L. Serum HER2 as a predictive biomarker for tissue HER2 status and prognosis in patients with gastric cancer. World J. Gastroenterol. 2017, 23, 1836–1842. [Google Scholar] [CrossRef]
- Cainap, C.; Nagy, V.; Gherman, A.; Cetean, S.; Laszlo, I.; Constantin, A.M.; Cainap, S. Classic tumor markers in gastric cancer. Current standards and limitations. Clujul Med. 2015, 88, 111–115. [Google Scholar]
- Arrieta, O.; Villarreal-Garza, C.; Martinez-Barrera, L.; Morales, M.; Dorantes-Gallareta, Y.; Pena-Curiel, O.; Contreras-Reyes, S.; Macedo-Perez, E.O.; Alatorre-Alexander, J. Usefulness of serum carcinoembryonic antigen (CEA) in evaluating response to chemotherapy in patients with advanced non-small-cell lung cancer: A prospective cohort study. BMC Cancer 2013, 13, 254. [Google Scholar] [CrossRef] [Green Version]
- Grunnet, M.; Sorensen, J.B. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer 2012, 76, 138–143. [Google Scholar] [CrossRef]
- Nithin, K.U.; Sridhar, M.G.; Srilatha, K.; Habebullah, S. CA 125 is a better marker to differentiate endometrial cancer and abnormal uterine bleeding. Afr. Health Sci. 2018, 18, 972–978. [Google Scholar]
- Duk, J.M.; Aalders, J.G.; Fleuren, G.J.; de Bruijn, H.W.A. CA 125: A useful marker in endometrial carcinoma. Am. J. Obst. Gynecol. 1986, 155, 1097–1102. [Google Scholar] [CrossRef]
- Goldstein, M.J.; Mitchell, E.P. Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Invest. 2005, 23, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Su, B.B.; Shi, H.; Wan, J. Role of serum carcinoembryonic antigen in the detection of colorectal cancer before and after surgical resection. World J. Gastroenterol. 2012, 18, 2121–2126. [Google Scholar] [CrossRef] [PubMed]
- Catalona, W.J.; Smith, D.S.; Ornstein, D.K. Prostate cancer detection in men with serum PSA concentrations of 2.6 to 4.0 ng/mL and benign prostate examination. Enhancement of specificity with free PSA measurements. JAMA 1997, 277, 1452–1455. [Google Scholar] [CrossRef]
- Catalona, W.J.; Loeb, S. Prostate cancer screening and determining the appropriate prostate-specific antigen cutoff values. J. Natl. Compr. Cancer Netw. 2010, 8, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Benvenuto, M.; Focaccetti, C.; Izzi, V.; Masuelli, L.; Modesti, A.; Bei, R. Tumor antigens heterogeneity and immune response-targeting neoantigens in breast cancer. Semin Cancer Biol. 2021, 72, 65–75. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Types of Antigens | Antigen | Cancer Type | Strengths for Early Detection | Limitations for Early Detection |
|---|---|---|---|---|
| Overexpressed Antigen | MUC1 | Breast | Expressed in over 90% of breast tumors | Most prevalent in metastasized breast cancers |
| HER2 | Breast/Esophageal Gastric/Ovarian Endometrial | Nearly 2 million receptors expressed on tumor cell surface | Can cause toxicity to healthy cells given low expression of antigen | |
| Differentiation Antigen | gp100 | Melanoma | High expression in malignant glioma cells | Expression in normal brain tissues |
| CEA | Colorectal cancer | Greater sensitivity than other diagnostic methods | Limited sensitivity Most effective in detection of recurrent cancers | |
| CT Antigen | MAGE-A | Melanoma Squamous cell carcinomas | Very specific to cancer cells | Higher prevalence in metastatic cancers |
| Biosensor Types | Advantages | Disadvantages | Examples of Biomarkers Detected | References |
|---|---|---|---|---|
| Localized and Compact Surface Plasmon Resonance Biosensor (LSPR and CSPR) | Highly sensitive and specific Label-free system Real-time measurement and detection Usage of gold nanomaterials Small sample size required to run | Complex mechanism of action Cost-effectiveness Non-target binding Immobilization on surface causing configurational changes | PD-L1 MT1-MMP IFN-γ PSA IgG TNF-α CRP | [31,32,33,34] |
| Electrochemical Biosensor | Cost and time- effective Small sample size required to run Very easy to use system for consumers Really good detection limits | Reproducibility issues (either one or few time usage) Not as sensitive as the other biosensors and conventional methods Very low shelf life | CEA NSE MUC1 EpCAM Multiple Types of miRNAs BRCA1 HER2 | [35,36,37,38] |
| Colorimetric Biosensor | Cost and time-effective Very easy-to use Small sample size required Portable and easy to maintain | Low sensitivity and specificity Reproducibility issues Low shelf life Limited multiplexing and quantification capabilities | CEA AFP PSA miRNA-148a miR-21 miR-155 | [39,40,41] |
| Multiplexed Nanobiosensors | Cost-effective High sensitivity and specificity compared to conventional methods Parallel detection of checkpoint markers (gives more insight in checkpoint interactions) Very small sample size needed | Still need to find effective ways for the target to get to the surface rapidly Non-target binding on the surface Non-specific interferences | PD-1 PD-L1 LAG-3 miR-21 miR-574-3p EpCAM Bladder Cancer MicroRNAs | [42,43,44] |
| Cancer Type | Biomarker | Diagnostic (D) Prognostic (P) | LOD/mL | References {LOD References} |
|---|---|---|---|---|
| Tumor-Associated Antigens | ||||
| Breast | HER-2 ECD, CEA CA15-3 | D/P | 2 ng, 5 ng, 21.8U | [99,100,101,102] {[103,104,105]} |
| Ovarian | CA125, CA15-3 | D | 35 U, 12U | [21,106,107,108,109], {[106,108]} |
| Pancreatic | CEA | P | 5 ng | [110] {[111]} |
| CA19-9 | D | 37U | [112] {[113]} | |
| CA125 | D/P | 35U | [114,115] {[116]} | |
| Gastric | CEA, HER-2 ECD | P | 5 ng, 24.75 ng | [110,117] {[117,118]} |
| NSCLC | CEA | P | 3–5ng | [119,120] {[120]} |
| Endometrial | CA 125 | D/P | 17.8U | [121,122] {[121]} |
| Colorectal | CEA | D/P | 5ng | [123] {[124]} |
| Prostate | PSA | D | 2.5–4 ng # | [125] {[126]}[127] |
| Immune Checkpoint Markers | ||||
| Primary central nervous system lymphoma (PCNSL) | PD-L1 | D/P | 0.43 ng | [78] {[79]} |
| NSCLC, DLBCL, CLL, NPC, HCC, ADR, PAC, HCC, Melanoma | PD-1 | P | ND, 500 pg 1 | [73,74] {[73]} |
| Breast, Gastric | LAG-3 | P | 120 pg, 378.3 ng | [70,71] {[71,73]} |
| PAC, Osteosarcoma, Ovarian | TIM-3 | P, D/P, ND | 3 ng, 14.4 ng | [59,60,81,82] {[81,82]} |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mummareddy, S.; Pradhan, S.; Narasimhan, A.K.; Natarajan, A. On Demand Biosensors for Early Diagnosis of Cancer and Immune Checkpoints Blockade Therapy Monitoring from Liquid Biopsy. Biosensors 2021, 11, 500. https://doi.org/10.3390/bios11120500
Mummareddy S, Pradhan S, Narasimhan AK, Natarajan A. On Demand Biosensors for Early Diagnosis of Cancer and Immune Checkpoints Blockade Therapy Monitoring from Liquid Biopsy. Biosensors. 2021; 11(12):500. https://doi.org/10.3390/bios11120500
Chicago/Turabian StyleMummareddy, Sai, Stuti Pradhan, Ashwin Kumar Narasimhan, and Arutselvan Natarajan. 2021. "On Demand Biosensors for Early Diagnosis of Cancer and Immune Checkpoints Blockade Therapy Monitoring from Liquid Biopsy" Biosensors 11, no. 12: 500. https://doi.org/10.3390/bios11120500