
Decellularized Porcine Conjunctiva in Treating Severe Symblepharon
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patients
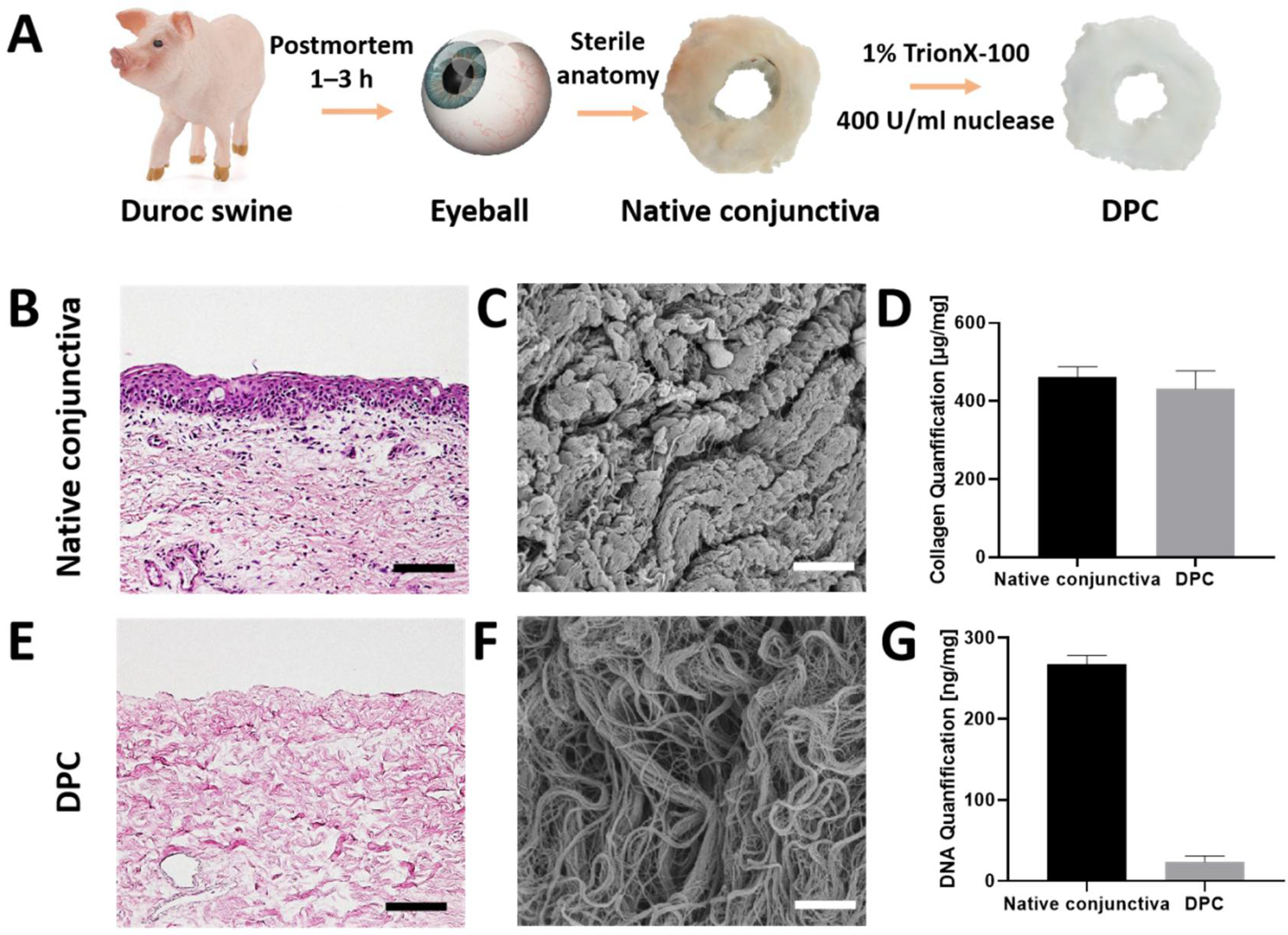
2.3. Preparation and Assessment of the Biomaterial
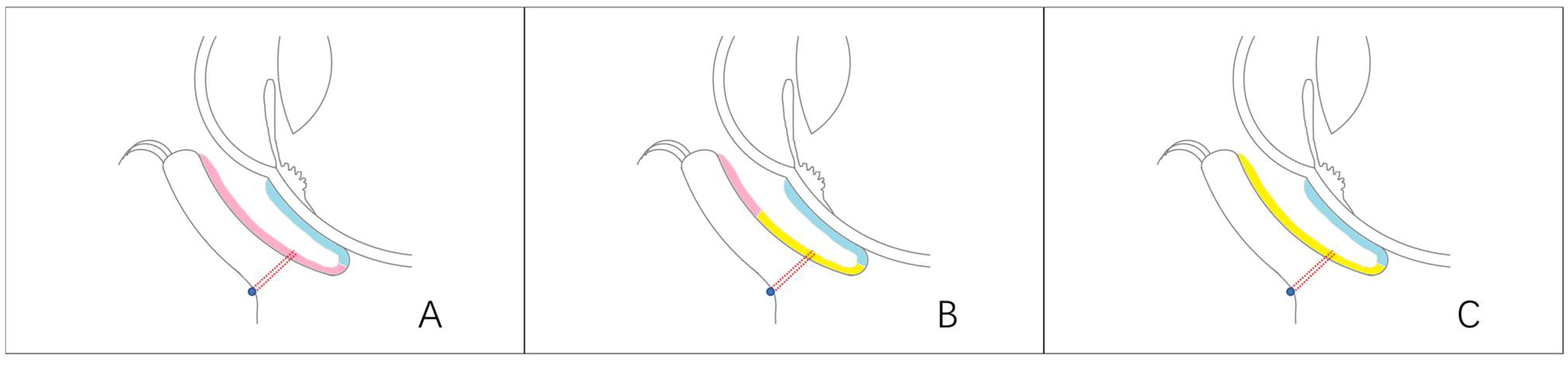
2.4. Surgical Techniques
2.5. Postoperative Treatment
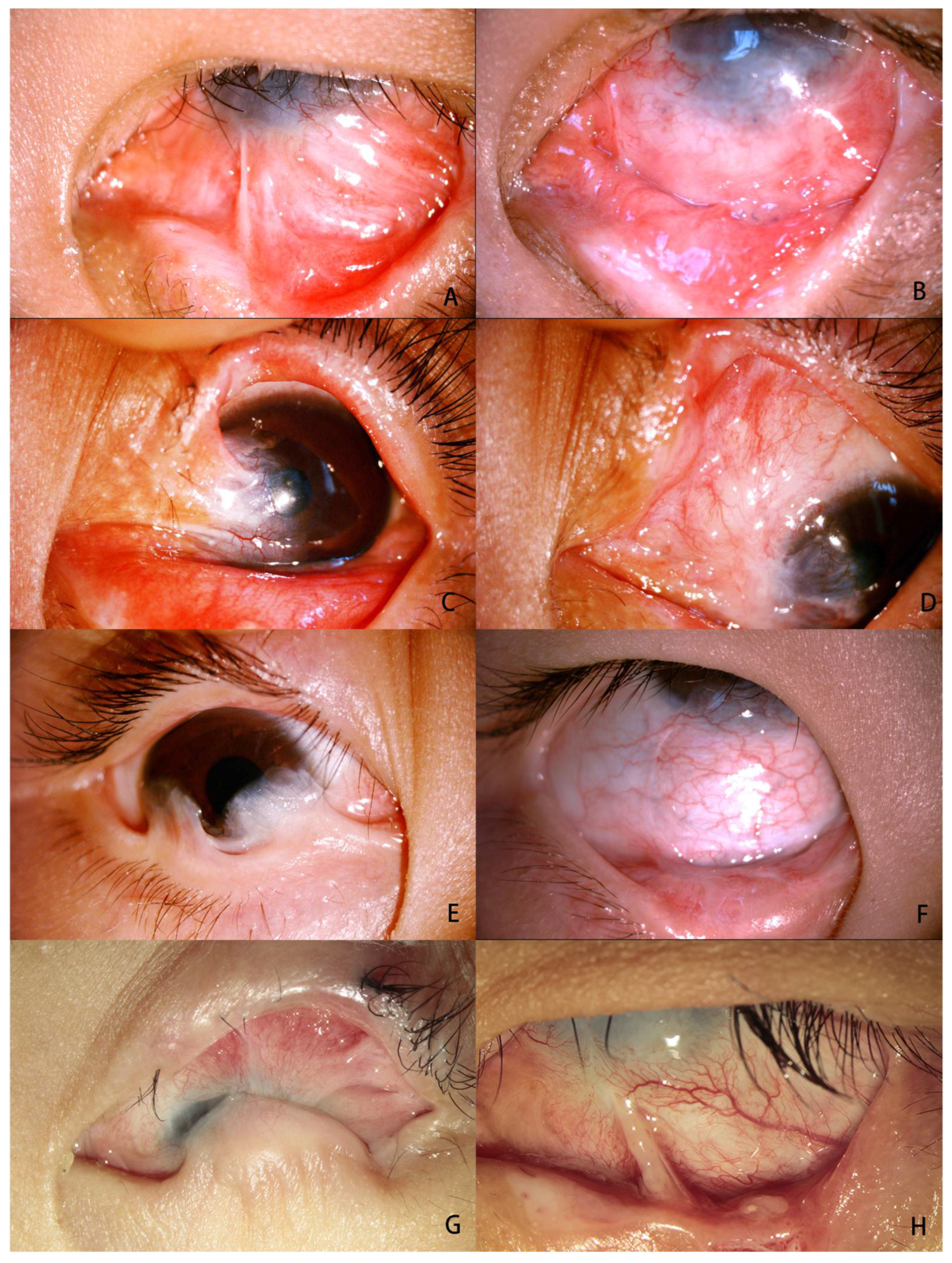
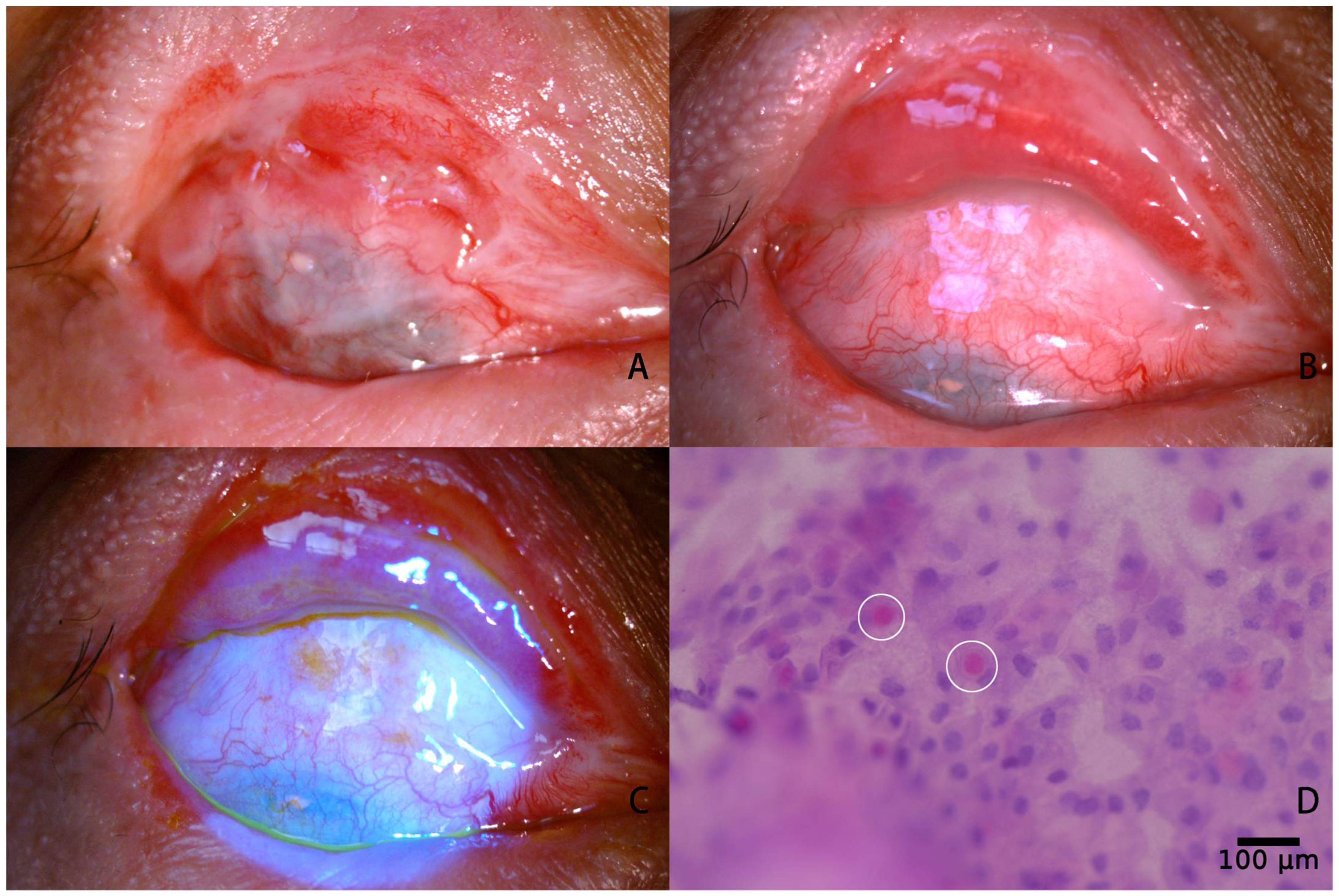
2.6. Evaluation of Clinical Outcomes
2.6.1. Fornix Depth Measurement
2.6.2. Schirmer II Test
2.6.3. Measurement of the Amplitude of Eye Movement
3. Results
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sant’ Anna, A.E.; Hazarbassanov, R.M.; de Freitas, D.; Gomes, J.Á. Minor salivary glands and labial mucous membrane graft in the treatment of severe symblepharon and dry eye in patients with Stevens-Johnson syndrome. Br. J. Ophthalmol. 2012, 96, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Senger, B.; Memar, S.A.; Ahmann, A.; Houser, J.J.; Doughty-McDonald, L. Dermatologic and ophthalmologic treatment of erythema multiforme major: A case report. Cureus 2021, 13, e20854. [Google Scholar] [CrossRef] [PubMed]
- Aslan Katırcıoğlu, Y.; Kaderli, A.; Şingar Özdemir, E.; Örnek, F. Clinical Results of the Use of Amniotic Membrane Transplantation Alone or in Combination with Adjuvant Therapies in Conjunctival Fornix Reconstruction. Turk. J. Ophthalmol. 2022, 52, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Kheirkhah, A.; Ghaffari, R.; Kaghazkanani, R.; Hashemi, H.; Behrouz, M.J.; Raju, V.K. A combined approach of amniotic membrane and oral mucosa transplantation for fornix reconstruction in severe symblepharon. Cornea 2013, 32, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kuckelkorn, R.; Schrage, N.; Redbrake, C.; Kottek, A.; Reim, M. Autologous transplantation of nasal mucosa after severe chemical and thermal eye burns. Acta Ophthalmol. Scand. 1996, 74, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.S.; Klefter, O.N.; Julian, H.O.; Lynge Pedersen, A.M.; Heegaard, S. Management of patients with ocular manifestations in vesiculobullous disorders affecting the mouth. Oral Dis. 2017, 23, 849–853. [Google Scholar] [CrossRef]
- Jovanovic, N.; Russell, W.W.; Heisel, C.J.; Hood, C.T.; Kahana, A. Direct Injection of 5-Fluorouracil Improves Outcomes in Cicatrizing Conjunctival Disorders Secondary to Systemic Disease. Ophthalmic Plast. Reconstr. Surg. 2021, 37, 145–153. [Google Scholar] [CrossRef]
- Muraine, M.; Gueudry, J.; Toubeau, D.; Gardea, E.; Verspyck, E.; Menguy, E.; Brasseur, G. Intérêt des greffes de membranes amniotiques dans les pathologies oculaires de surface [Advantages of amniotic membrane transplantation in eye surface diseases]. J. Fr. D’ophtalmologie 2006, 29, 1070–1083. [Google Scholar] [CrossRef]
- Kruse, F.E.; Meller, D. Die Amnionmembrantransplantation zur Rekonstruktion der Augenoberfläche [Amniotic membrane transplantation for reconstruction of the ocular surface]. Der Ophthalmol. Z. Der Dtsch. Ophthalmol. Ges. 2001, 98, 801–810. [Google Scholar]
- Hopkinson, A.; McIntosh, R.S.; Tighe, P.J.; James, D.K.; Dua, H.S. Amniotic membrane for ocular surface reconstruction: Donor variations and the effect of handling on TGF-beta content. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4316–4322. [Google Scholar] [CrossRef]
- Rahman, I.; Said, D.G.; Maharajan, V.S.; Dua, H.S. Amniotic membrane in ophthalmology: Indications and limitations. Eye 2009, 23, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Borrelli, M.; Reichl, S.; Schrader, S.; Geerling, G. Review of alternative carrier materials for ocular surface reconstruction. Curr. Eye Res. 2014, 39, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Henderson, H.W.A.; Collin, J.R.O. Mucous membrane grafting. Dev. Ophthalmol. 2008, 41, 230–242. [Google Scholar] [PubMed]
- Mai, C.; Bertelmann, E. Oral mucosal grafts: Old technique in new light. Ophthalmic Res. 2013, 50, 91–98. [Google Scholar] [CrossRef]
- Kim, J.H.; Chun, Y.S.; Lee, S.H.; Mun, S.K.; Jung, H.S.; Lee, S.H.; Son, Y.; Kim, J.C. Ocular surface reconstruction with autologous nasal mucosa in cicatricial ocular surface disease. Am. J. Ophthalmol. 2010, 149, 45–53. [Google Scholar] [CrossRef]
- Schrader, S.; Notara, M.; Beaconsfield, M.; Tuft, S.J.; Daniels, J.T.; Geerling, G. Tissue engineering for conjunctival reconstruction: Established methods and future outlooks. Curr. Eye Res. 2009, 34, 913–924. [Google Scholar] [CrossRef]
- Porzionato, A.; Stocco, E.; Barbon, S.; Grandi, F.; Macchi, V.; De Caro, R. Tissue-Engineered Grafts from Human Decellularized Extracellular Matrices: A Systematic Review and Future Perspectives. Int. J. Mol. Sci. 2018, 19, 4117. [Google Scholar] [CrossRef]
- Zhao, L.; Jia, Y.; Zhao, C.; Li, H.; Wang, F.; Dong, M.; Liu, T.; Zhang, S.; Zhou, Q.; Shi, W. Ocular surface repair using decellularized porcine conjunctiva. Acta Biomater. 2020, 101, 344–356. [Google Scholar] [CrossRef]
- Kheirkhah, A.; Blanco, G.; Casas, V.; Hayashida, Y.; Raju, V.K.; Tseng, S.C. Surgical strategies for fornix reconstruction based on symblepharon severity. Am. J. Ophthalmol. 2008, 146, 266–275. [Google Scholar] [CrossRef]
- Shi, W.; Wang, T.; Gao, H.; Xie, L. Management of severe ocular burns with symblepharon. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 101–106. [Google Scholar] [CrossRef]
- McGinnigle, S.; Naroo, S.A.; Eperjesi, F. Evaluation of dry eye. Surv. Ophthalmol. 2012, 57, 293–316. [Google Scholar] [CrossRef] [PubMed]
- Jutley, G.; Carpenter, D.; Hau, S.; Booth, D.; Jasim, H.A.; Tay, E.; Daniel, C.; Saw, V. Upper and lower conjunctival fornix depth in healthy white caucasian eyes: A method of objective assessment. Eye 2016, 30, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.; Espana, E.M.; Tseng, S.C. Amniotic membrane transplantation for reconstruction of the conjunctival fornices. Ophthalmology 2003, 110, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Witt, J.; Mertsch, S.; Borrelli, M.; Dietrich, J.; Geerling, G.; Schrader, S.; Spaniol, K. Decellularised conjunctiva for ocular surface reconstruction. Acta Biomater. 2018, 67, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Witt, J.; Dietrich, J.; Mertsch, S.; Schrader, S.; Spaniol, K.; Geerling, G. Decellularized porcine conjunctiva as an alternative substrate for tissue-engineered epithelialized conjunctiva. Ocul. Surf. 2020, 18, 901–911. [Google Scholar] [CrossRef]
- Zhao, D.; Yin, H.Y.; Cheng, A.; Chen, R.; Sheha, H.; Tseng, S.C. Sealing of the gap between the conjunctiva and tenon capsule to improve symblepharon surgery. Am. J. Ophthalmol. 2015, 160, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, I. Pre- and intraoperative mitomycin C for recurrent pterygium associated with symblepharon. Clin. Ophthalmol. 2013, 7, 199–202. [Google Scholar] [CrossRef]
- Rockwood, E.J.; Parrish, R.K., 2nd; Heuer, D.K.; Skuta, G.L.; Hodapp, E.; Palmberg, P.F.; Gressel, M.G.; Feuer, W. Glaucoma filtering surgery with 5-fluorouracil. Ophthalmology 1987, 94, 1071–1078. [Google Scholar] [CrossRef]
- Wang, T.; Shan, F.; Zhou, Q.; Shi, W.; Xie, L. Allogeneic Cultivated Limbal Epithelial Sheet Transplantation in Reconstruction of Conjunctival Sac After Chemical and Thermal Burns. Front. Med. 2021, 8, 697264. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Symblepharon | Conjunctival Substitute | Number of Eyes | Clinical Outcomes | The Average of FD (mm) | The Average of Schirmer II Test (mm) | The Average of EMD (mm) | Goblet Cells (n) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Complete Success, n (%) | Partial Success, n (%) | Failure, n (%) | Preoperative | Postoperative | Preoperative | Postoperative | Preoperative | Postoperative | ||||
| grade III | AC+DPC | 3 | 7 (100) | 0 (0) | 0 (0) | 1.36 | 8 | 12.5 | 14 | 4.86 | 6.93 | 7 |
| AC+AOM+DPC | 4 | |||||||||||
| grade IV | DPC+DPC | 2 | 5 (55.56) | 3 (33.33) | 1 (11.11) | 0 | 7.17 | none | 10.56 | 2.89 | 6.28 | 8 |
| AOM+DPC | 7 | |||||||||||
| Total | 16 | 12 (75) | 3 (18.75) | 1 (6.25) | 0.59 | 7.53 | 12.5 | 12.06 | 3.75 | 6.56 | 15 | |
| Number | Trauma Causes | Grading and Width of Symblepharon | Conjunctival Substitute (Palpebral + Bulbar Conjunctiva) | Clinical Outcomes | Preoperative FD (mm) | Postoperative FD (mm) | Preoperative Schirmer II Test (mm) | Postoperative Schirmer II Test (mm) | Preoperative EMD (mm) | Postoperative EMD (mm) | Goblet Cells |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Alkali burn | IVb | DPC+DPC | partial success | 0 | 8 | Not examined | 11 | 3 | 6.5 | exist |
| 2 | thermal burn | IVb | DPC+DPC | partial success | 0 | 9 | Not examined | 10 | 3 | 5 | exist |
| 3 | thermal burn | IVa | AOM+DPC | complete success | 0 | 7.5 | Not examined | 8 | 3.5 | 6 | exist |
| 4 | Alkali burn | IIIc | AC+AOM+DPC | complete success | 2 | 8 | 10 | 13 | 4 | 6 | exist |
| 5 | Alkali burn | IIIa | AC+DPC | complete success | 2 | 8 | 16 | 15 | 5 | 6.5 | exist |
| 6 | thermal burn | IIIc | AC+AOM+DPC | complete success | 1.5 | 8 | 13 | 15 | 3 | 5.5 | exist |
| 7 | thermal burn | IIIa | AC+DPC | complete success | 1 | 9 | 11 | 13 | 7 | 8 | exist |
| 8 | thermal burn | IIIc | AC+AOM+DPC | complete success | 1 | 6 | Not examined | 12 | 6 | 7 | exist |
| 9 | thermal burn | IVa | AOM+DPC | complete success | 0 | 5 | Not examined | 13 | 3.5 | 8 | exist |
| 10 | Alkali burn | IVc | AOM+DPC | failure | 0 | 3 | Not examined | 6 | 2.5 | 4 | none |
| 11 | thermal burn | IVb | AOM+DPC | complete success | 0 | 9 | Not examined | 10 | 2 | 7 | exist |
| 12 | thermal burn | IVb | AOM+DPC | complete success | 0 | 7.5 | Not examined | 13 | 3 | 7 | exist |
| 13 | thermal burn | IVb | AOM+DPC | complete success | 0 | 8.5 | Not examined | 15 | 3.5 | 8 | exist |
| 14 | Alkali burn | IIIa | AC+DPC | complete success | 1 | 9 | 14 | 17 | 4 | 7.5 | exist |
| 15 | Alkali burn | IVc | AOM+DPC | partial success | 0 | 7 | Not examined | 9 | 2 | 5 | exist |
| 16 | thermal burn | IIIb | AC+AOM+DPC | complete success | 1 | 8 | 11 | 13 | 5 | 8 | exist |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shan, F.; Feng, X.; Li, J.; Yang, S.; Wang, F.; Shi, W.; Zhao, L.; Zhou, Q. Decellularized Porcine Conjunctiva in Treating Severe Symblepharon. J. Funct. Biomater. 2023, 14, 318. https://doi.org/10.3390/jfb14060318
Shan F, Feng X, Li J, Yang S, Wang F, Shi W, Zhao L, Zhou Q. Decellularized Porcine Conjunctiva in Treating Severe Symblepharon. Journal of Functional Biomaterials. 2023; 14(6):318. https://doi.org/10.3390/jfb14060318
Chicago/Turabian StyleShan, Fengmei, Xueying Feng, Jie Li, Sha Yang, Fuhua Wang, Weiyun Shi, Long Zhao, and Qingjun Zhou. 2023. "Decellularized Porcine Conjunctiva in Treating Severe Symblepharon" Journal of Functional Biomaterials 14, no. 6: 318. https://doi.org/10.3390/jfb14060318