
A Framework for User-Focused Electronic Health Record System Leveraging Hyperledger Fabric



Abstract
:1. Introduction
2. Literature Review
2.1. Electronic Health Records
2.2. Blockchain
2.3. The Adoption of Blockchain Technologies in the Healthcare Sector
2.4. User-Focused EMR Systems Using Blockchain
3. Materials and Methods
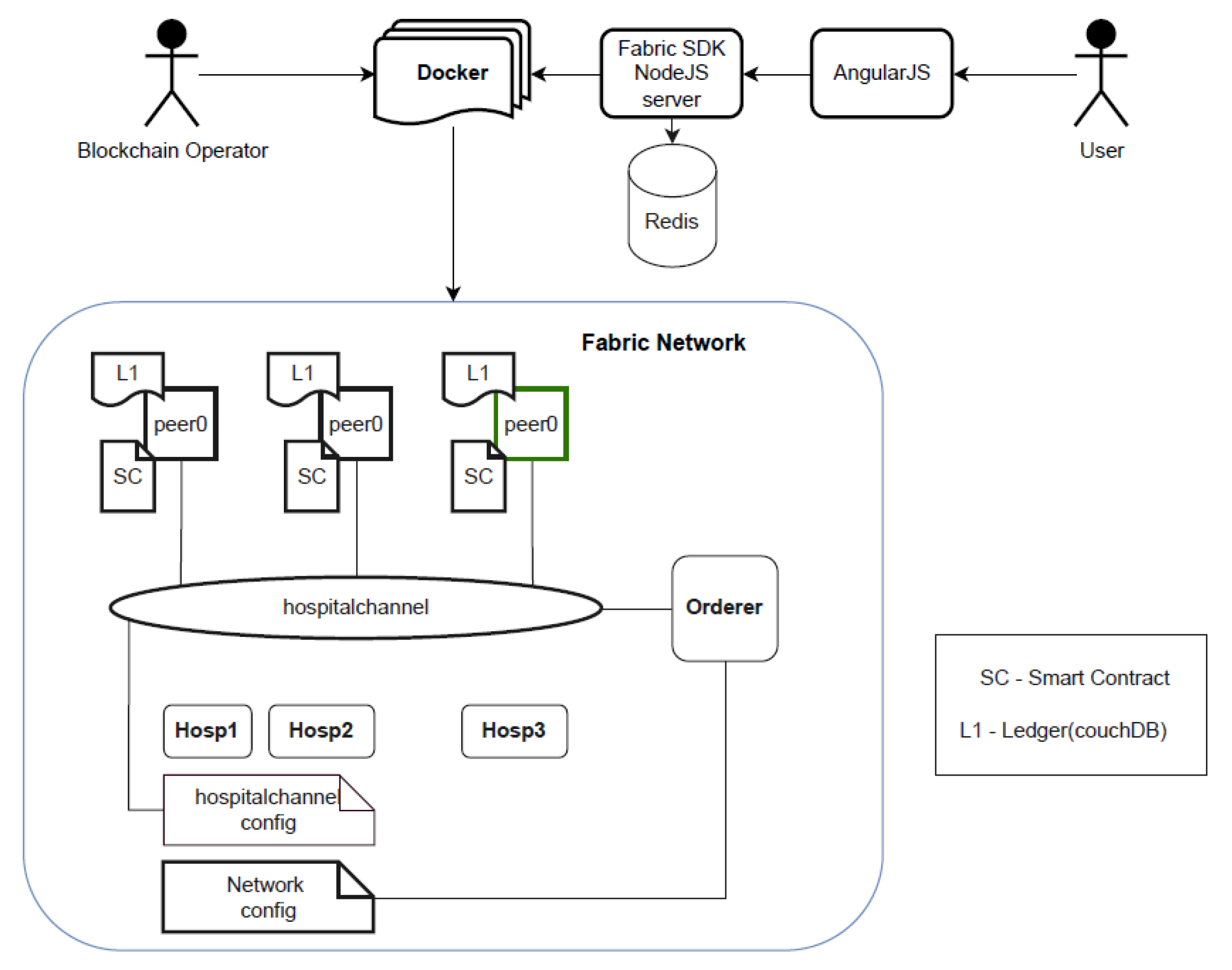
3.1. Overview of System Architecture
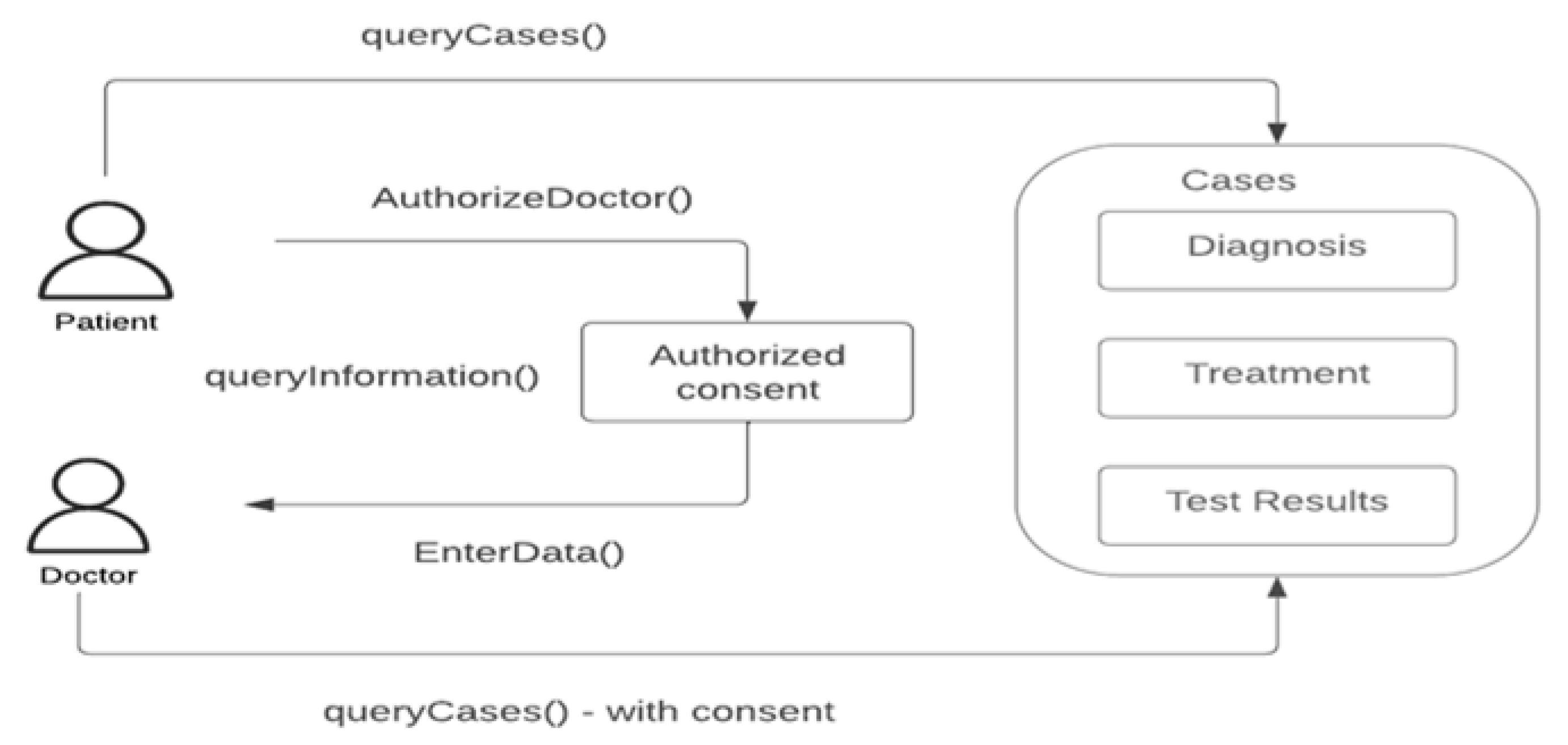
3.2. Workflow
3.3. Implementation of the Hyperledger Fabric in the Healthcare Sector
3.3.1. Technology Stack
- Hyperledger Fabric: These are smart contracts built inside this blockchain [12].
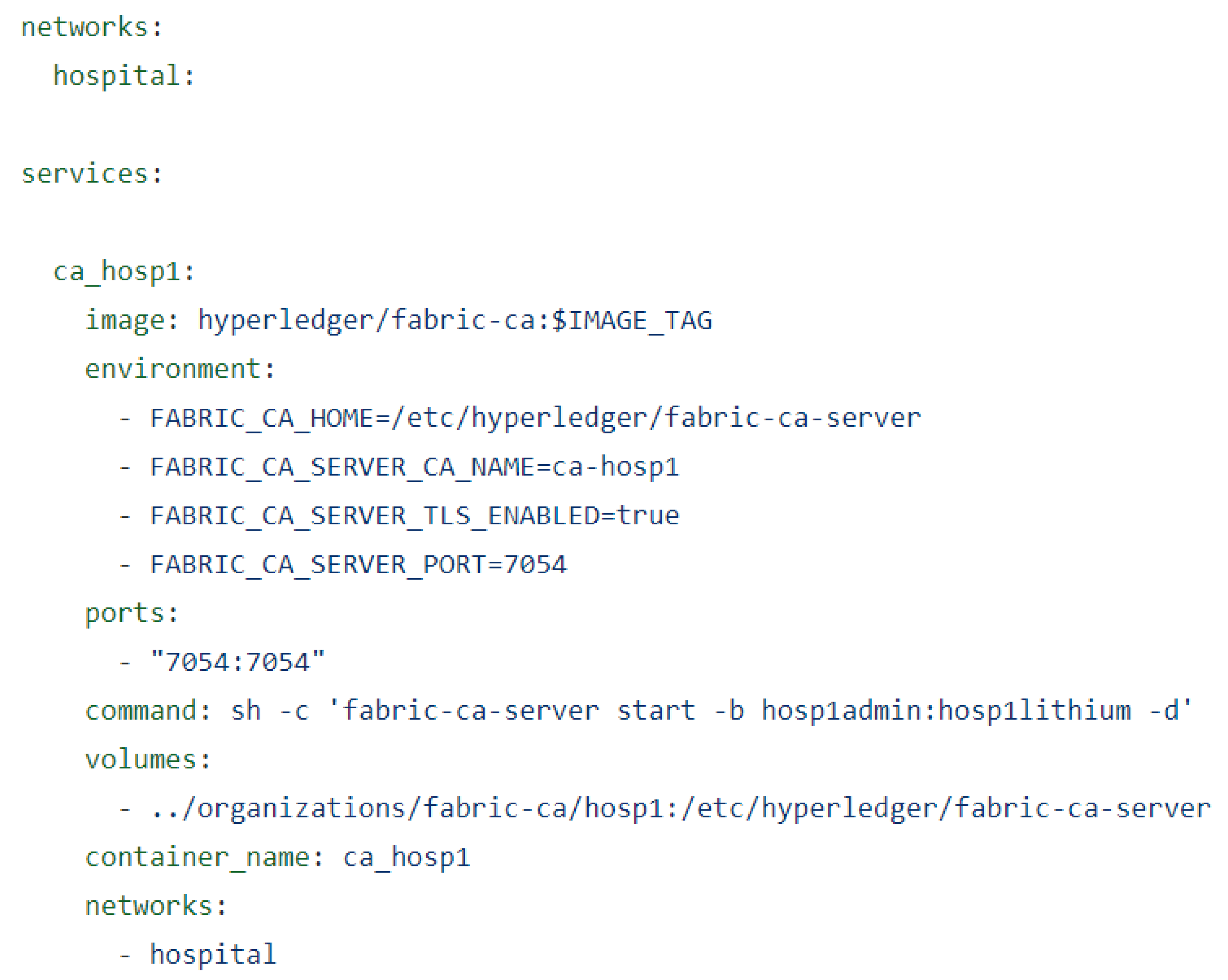
- Docker Compose: Used to deliver software packages called containers (docker-compose-ca.yaml, docker-compose-couch.yaml, docker-compose-net.yaml) [12].
- Couch DB: Open-source database, which allows the storage of data in JSON format and is used as an external state of a database for Hyperledger fabric [12].
- Node JS: This is an open-source cross-platform backend where the script runs in the terminal and executes JavaScript code outside of the browser. In this project, Node JS is used to provide API to react with Hyperledger Fabric blockchain (which performs the first level of user authentication and acts as the gateway to the Fabric smart contracts) [12].
- Angular JavaScript: This framework has been used to build the client application web interface.
- Interplanetary file system (IPFS): This is a peer-to-peer file storage network for storing and sharing data in a distributed file system. Content is accessible through peers located anywhere in the world [12].
3.3.2. Healthcare Network
3.3.3. State of Distributed Database
3.3.4. Deployment of Chaincode to the Network
3.3.5. Use of Software Development Kit (sdk)
Fabric-Ca-Client
Fabric-Network
Fabric-Common
Wallet
Use of the API
Implementation of JSON Web Tokens
3.3.6. Client/Front-End Development
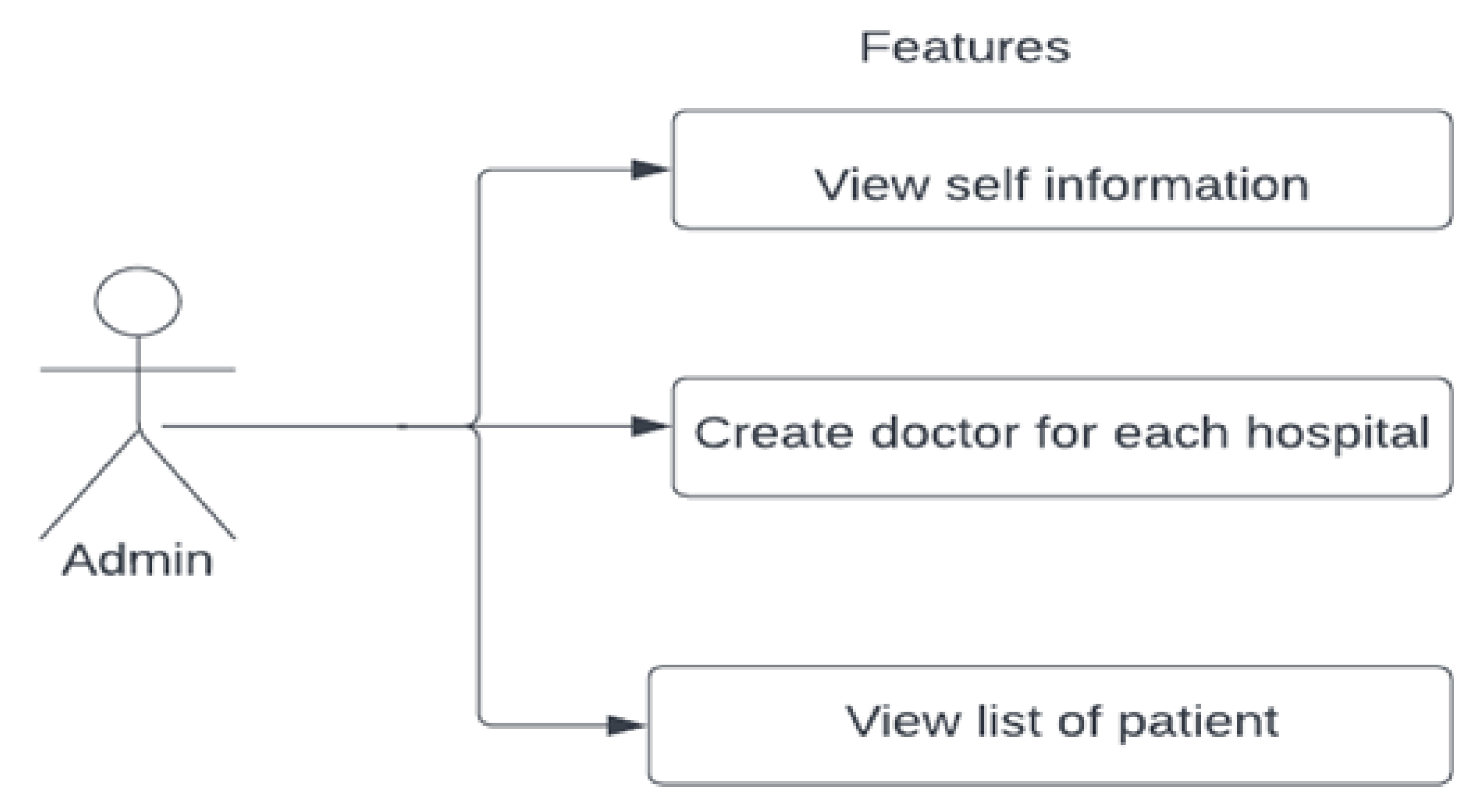
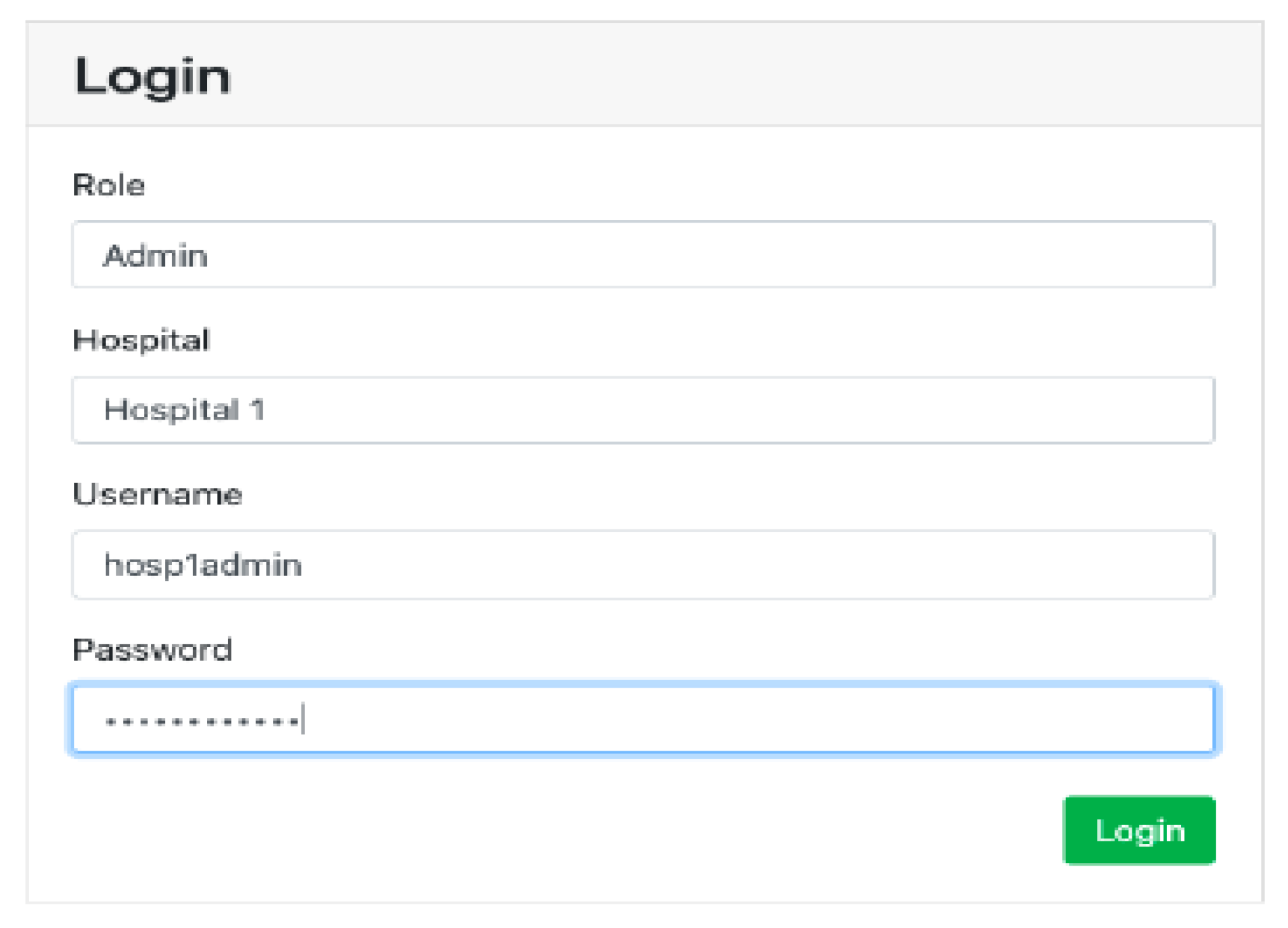
Login Screen for Admin
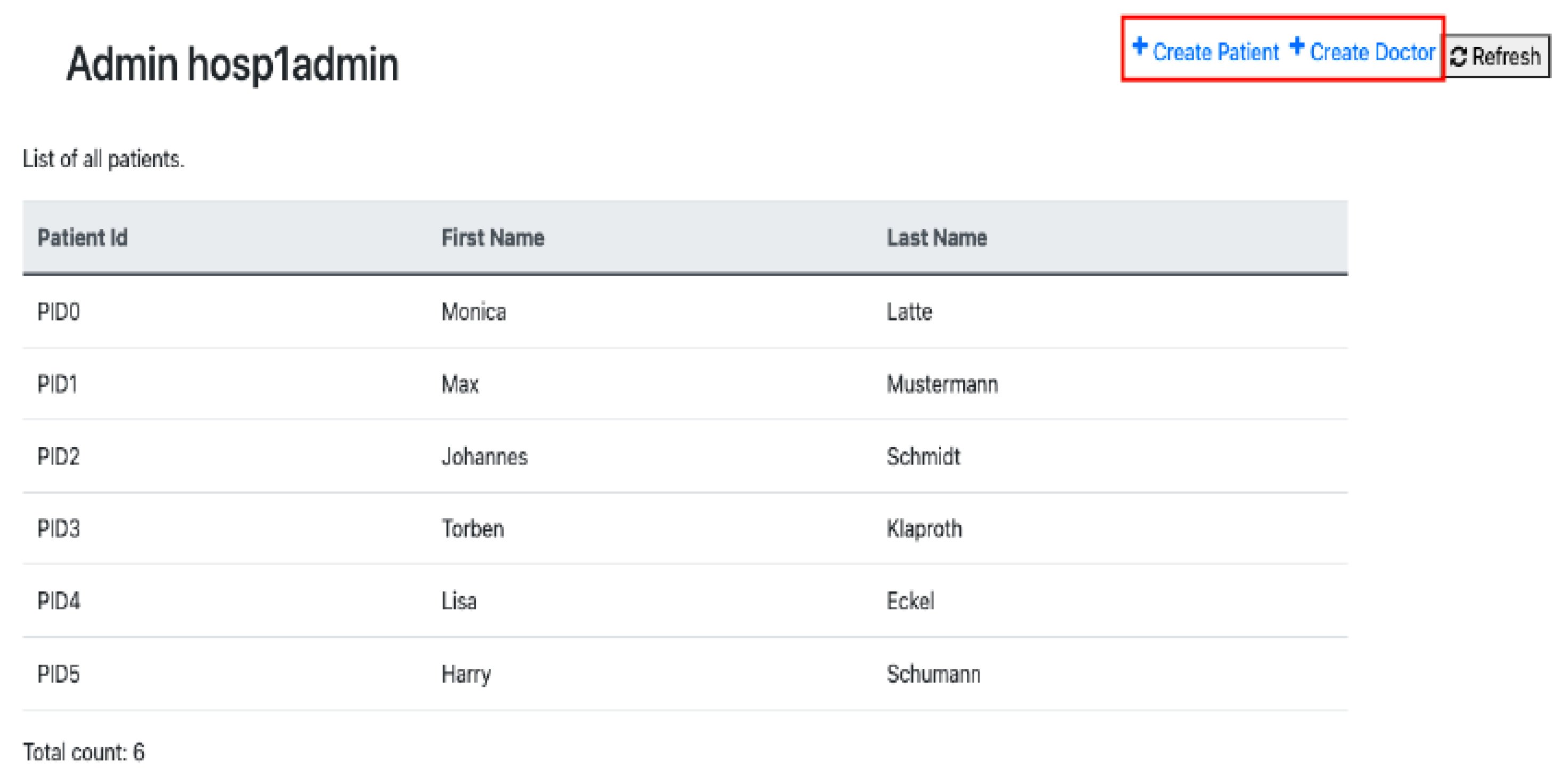
Admin Dashboard Screen
Asset-Create-Patient
Asset-Create-Doctor
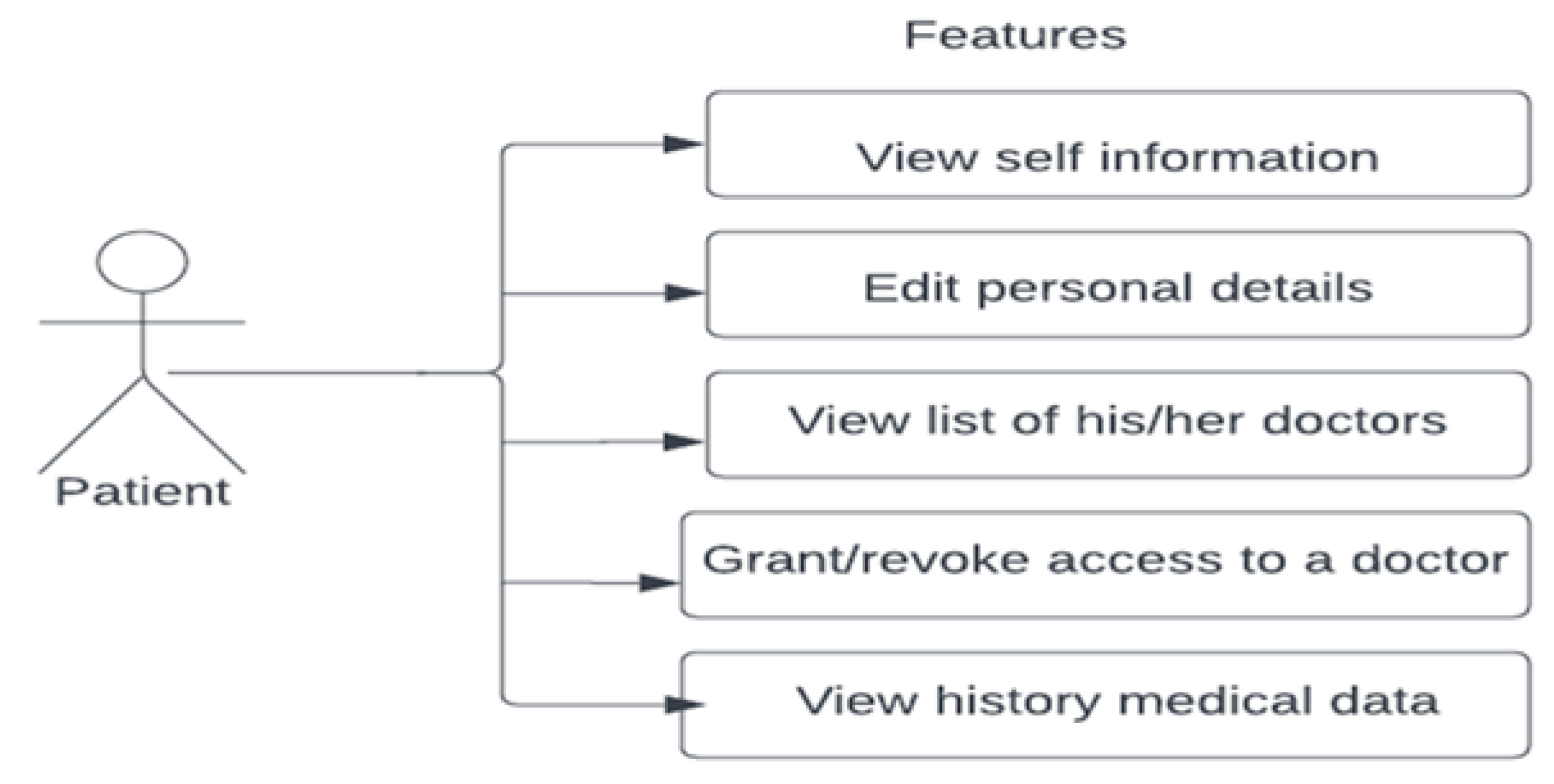
Patient Login
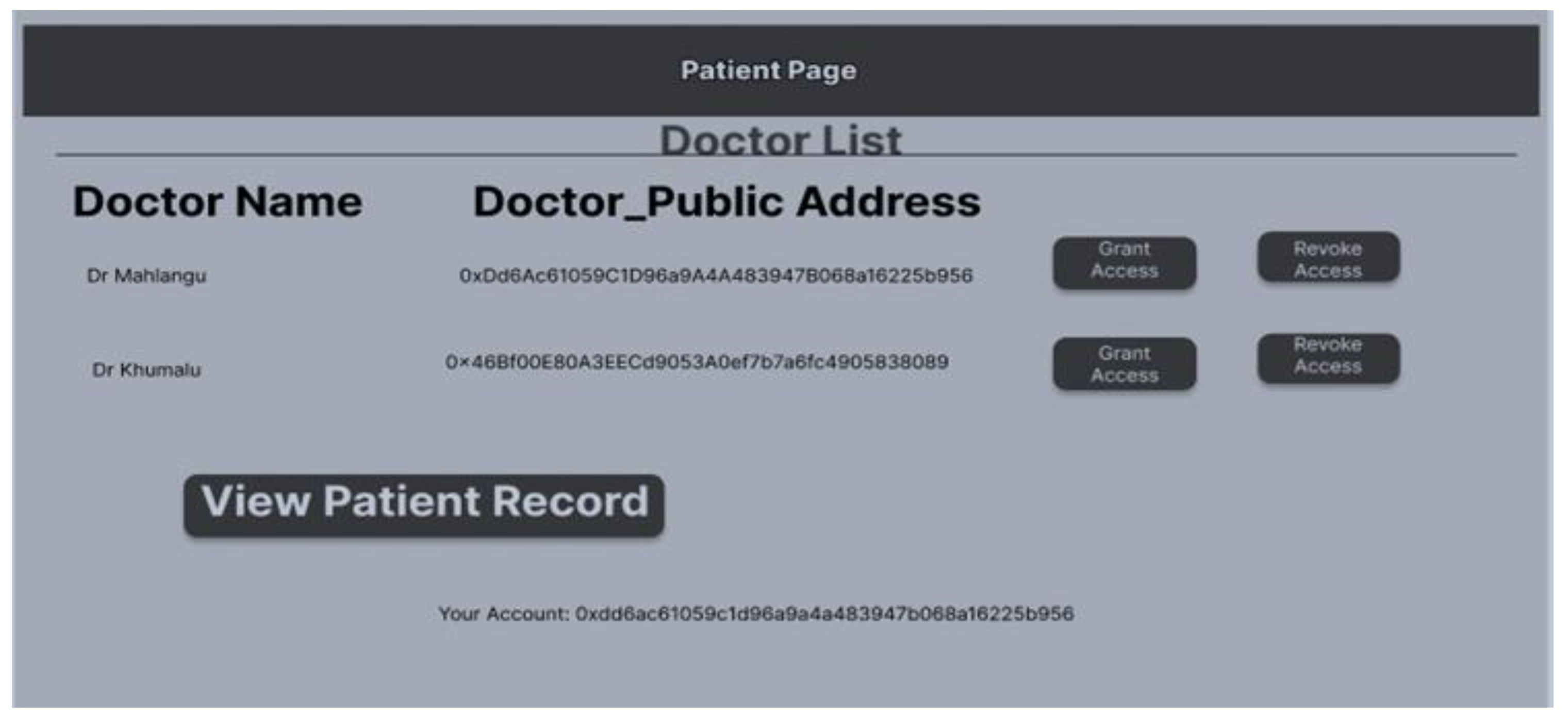
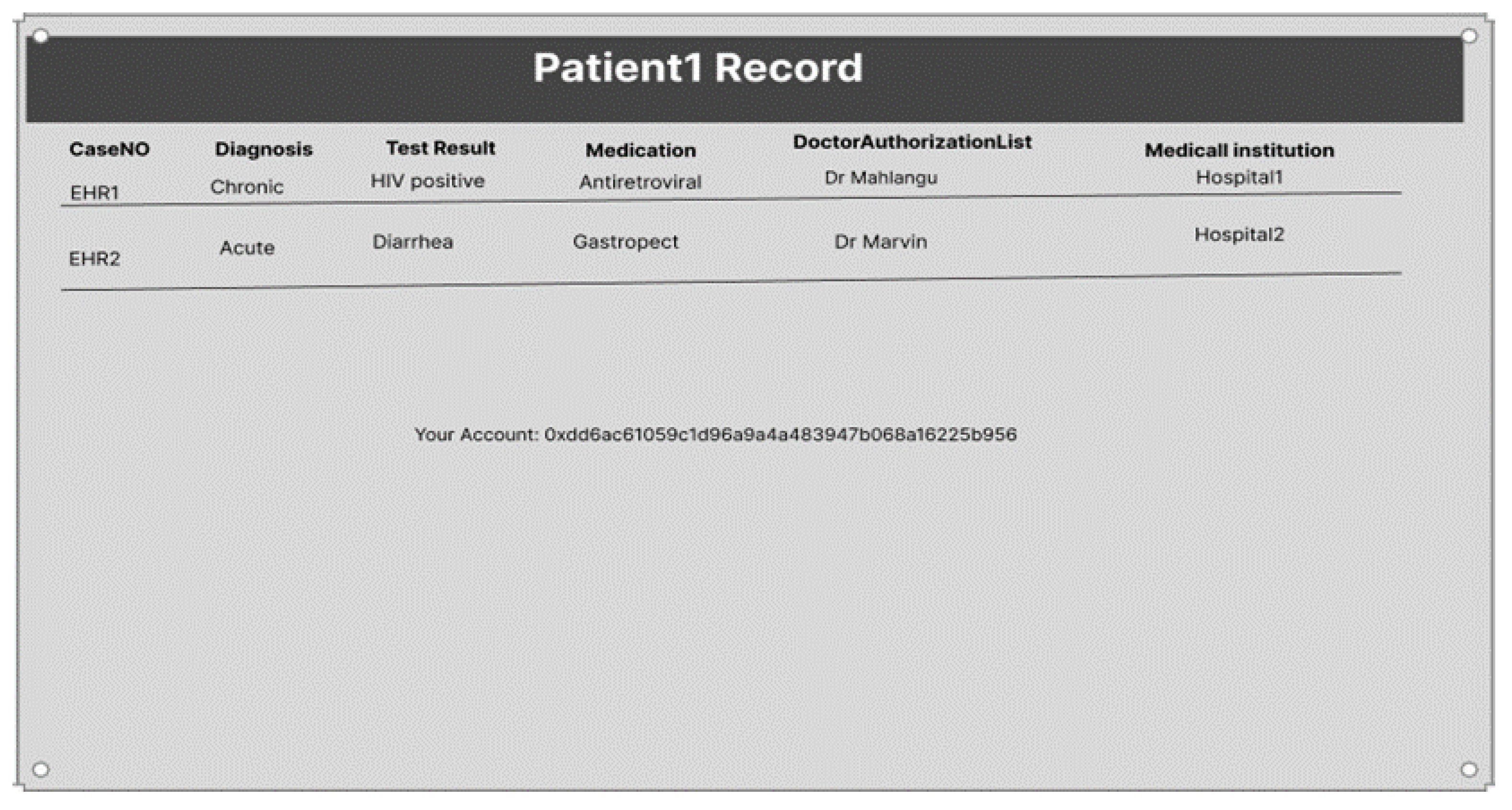
View Patient Information
Feature Grant/Revoke Access
Update Personal Details
View History
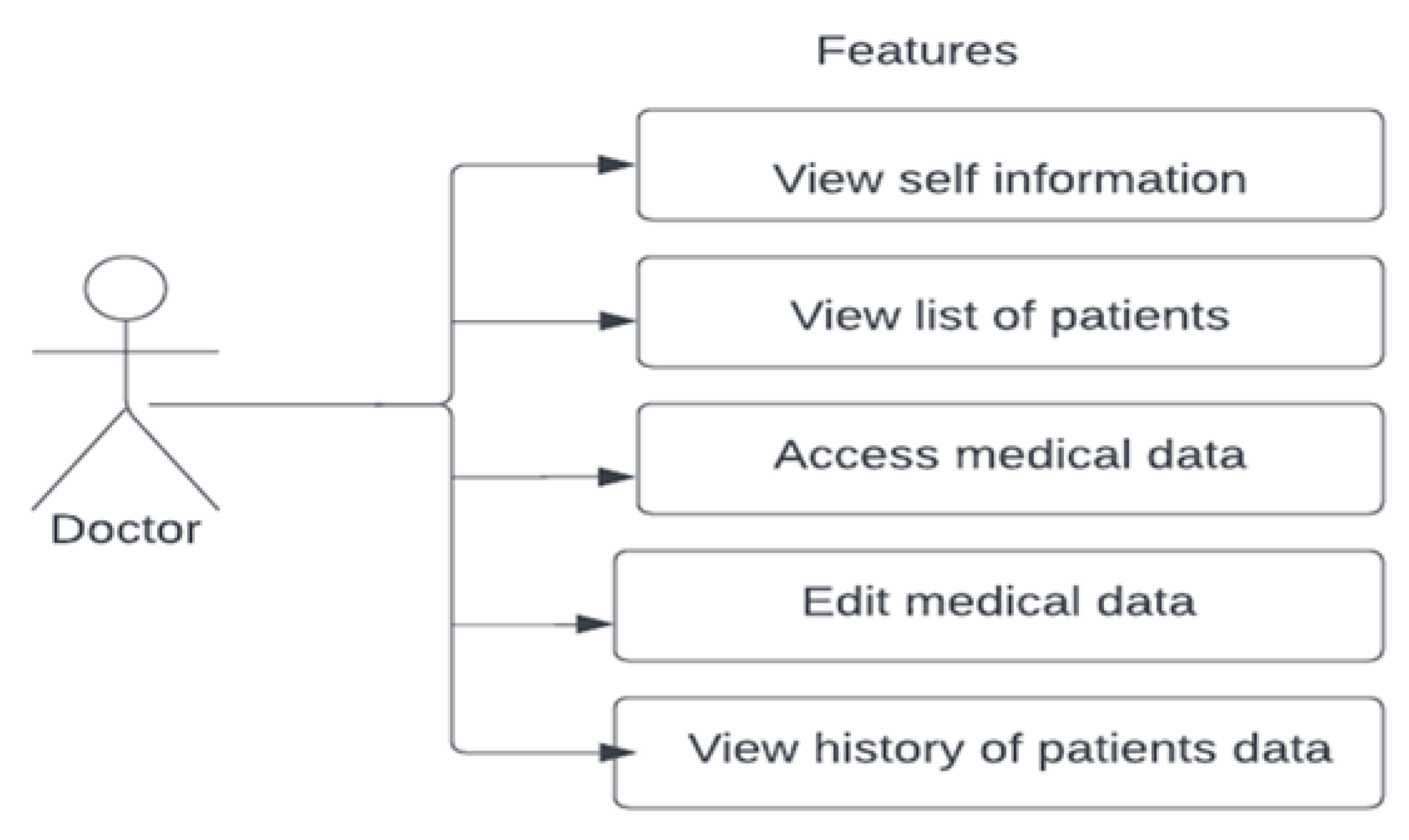
Doctor Login Screen
Feature to View Patients
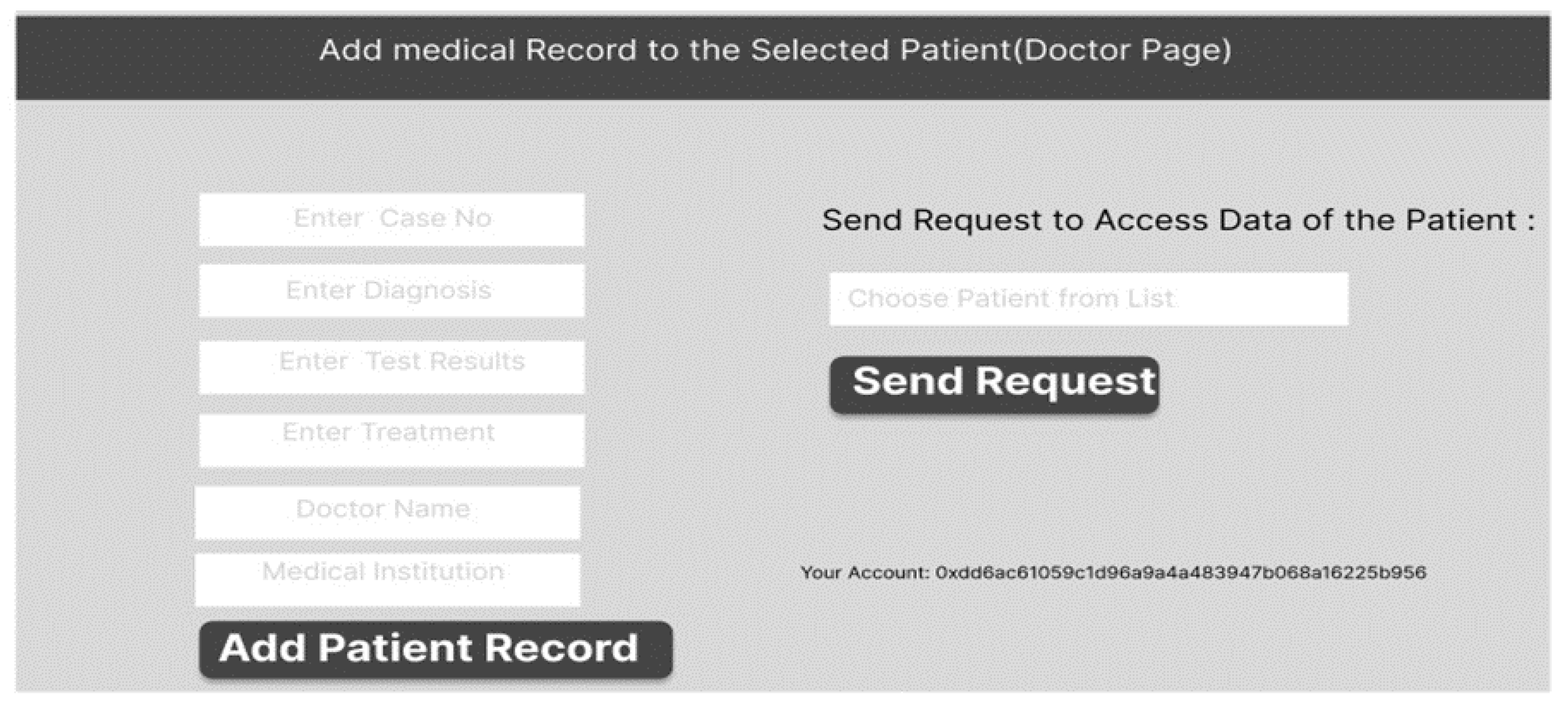
Update Medical Information
Medical History
4. Results
4.1. Pros and Cons Analysis of the Fabric Network
4.1.1. Pros
4.1.2. Cons
4.2. Challenges
4.3. Hyperledger Drawbacks
4.4. Application Scalability
4.5. Comparison of Database Systems
5. Conclusions
6. Future Work
- Currently, the metadata concept keeps the actual patient data on the blockchain network as developed. If such a system is to be used as a national or global solution, this may become impossible because the blockchain would become huge. Conversely, it may be preferable to merely keep the metadata for health records and accesses on the blockchain, with the actual data remaining in a conventional database. This hybrid method may make it possible to take advantage of some of the features of both traditional database systems and decentralized systems. Therefore, development work is required in this area.
- Although the project developed a prototype, the system was designed with scalability in mind. It is envisaged that many hospitals and other medical facilities will join the blockchain network for the implementation of this system. One organization may have multiple peers, and there may be different sub-channels and endorsement policies. Further studies are required to address this feature of the system.
- To protect the security of EHRs in the future, a workaround for private data collection utilizing a modified data structure needs to be developed. Additionally, retrieving transaction history from private data may prove to be a practical solution to the problem of acquiring transaction history if it is supported by the next version of Hyperledger Fabric.
- Multiple orderer systems are used in Hyperledger Fabric v2.x to develop a fail-safe system that is crash tolerant. For example, if there are three ordering nodes in a system and one node fails, the ordering service will continue to function using the other two ordering nodes and by electing a new leader. Raft is the initial step toward Fabric’s creation of a byzantine fault tolerant (BFT) ordering service, according to official Hyperledger Fabric documentation. Consequently, further development work is required to enhance this functionality of the system.
- The system manages medical information and, normally, healthcare processes are incorporated with consultation. Therefore, a consultation feature needs to be developed to improve the standard of the app and make the process easier for both the doctor and patient.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Network—Organization Setup

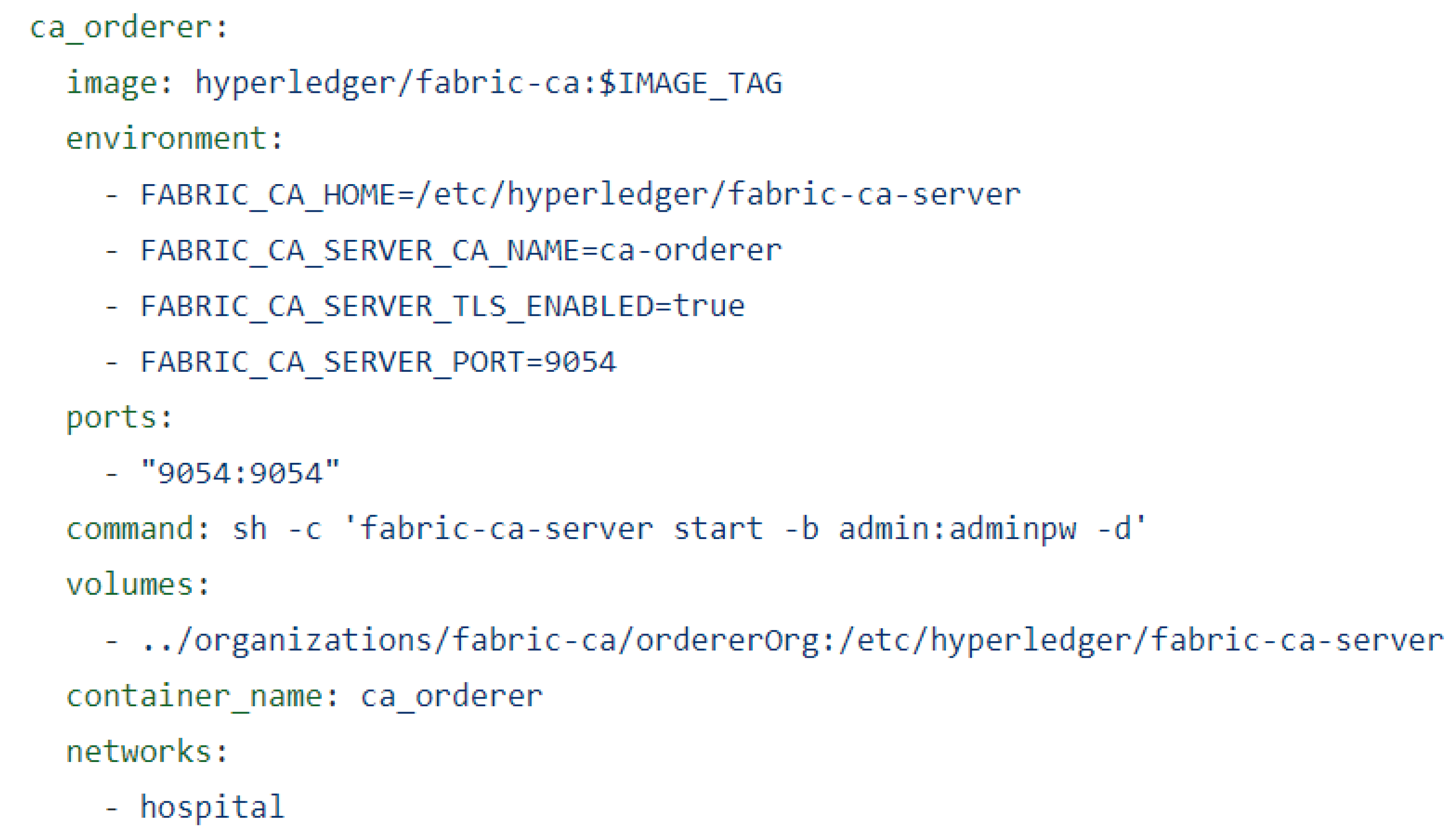
Appendix B. Orderer Setup

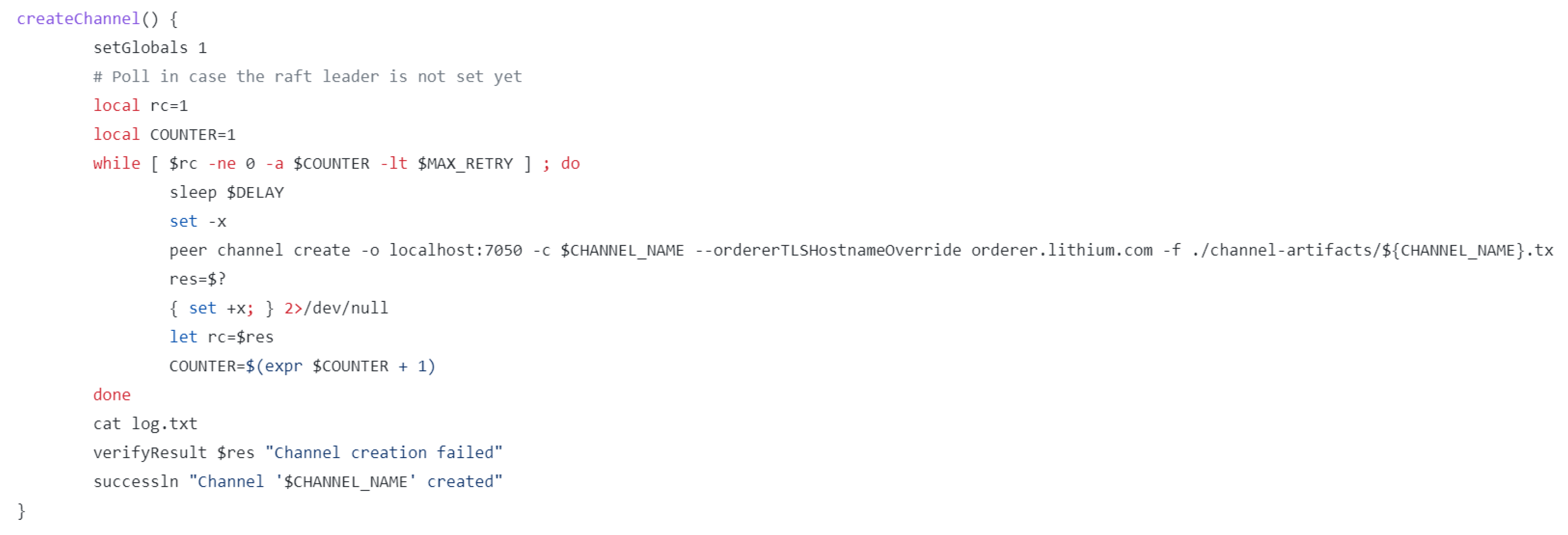
Appendix C. Create Channel

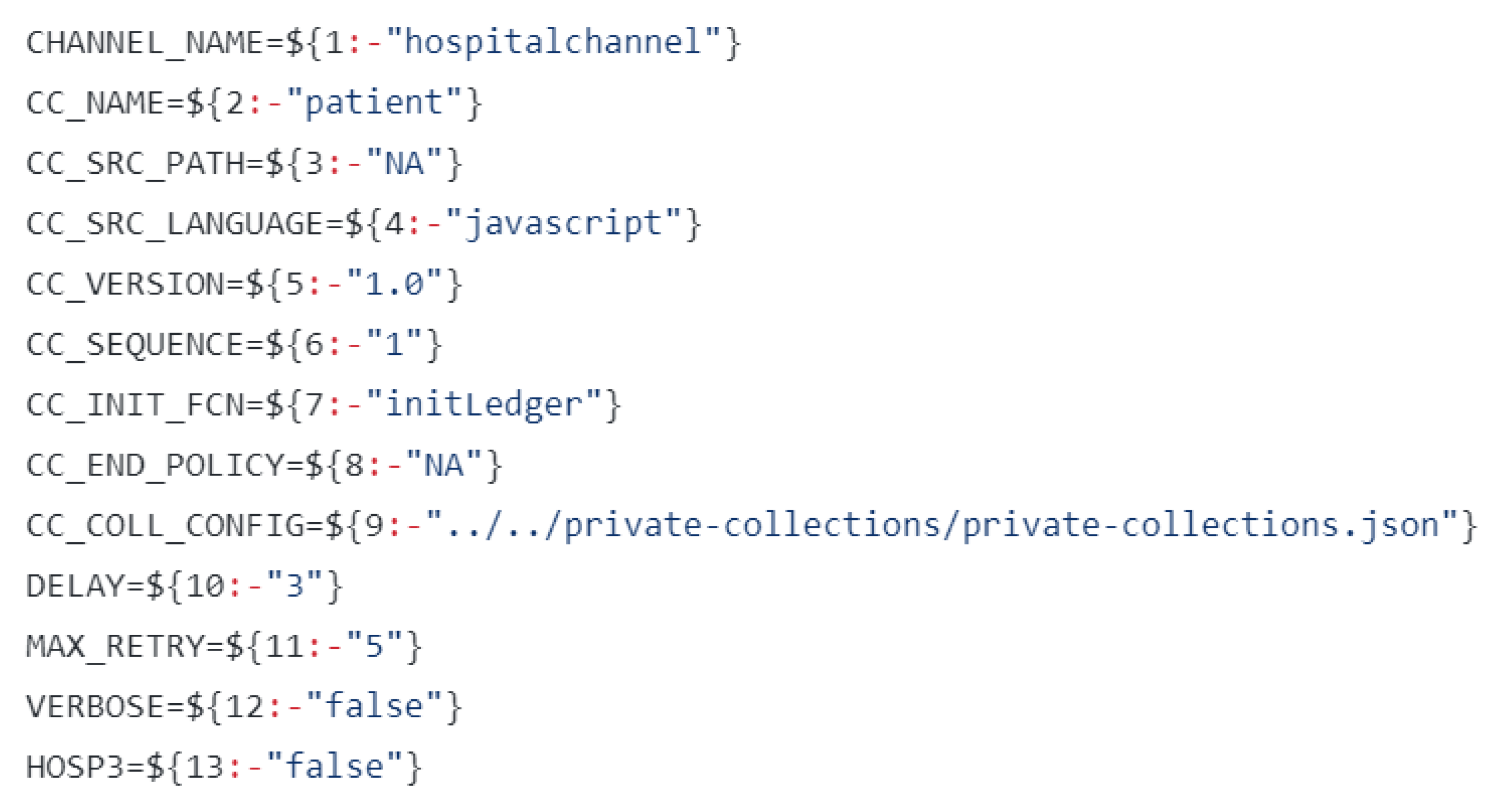
Appendix D. Deploy Chaincode

Appendix E. Enroll Server

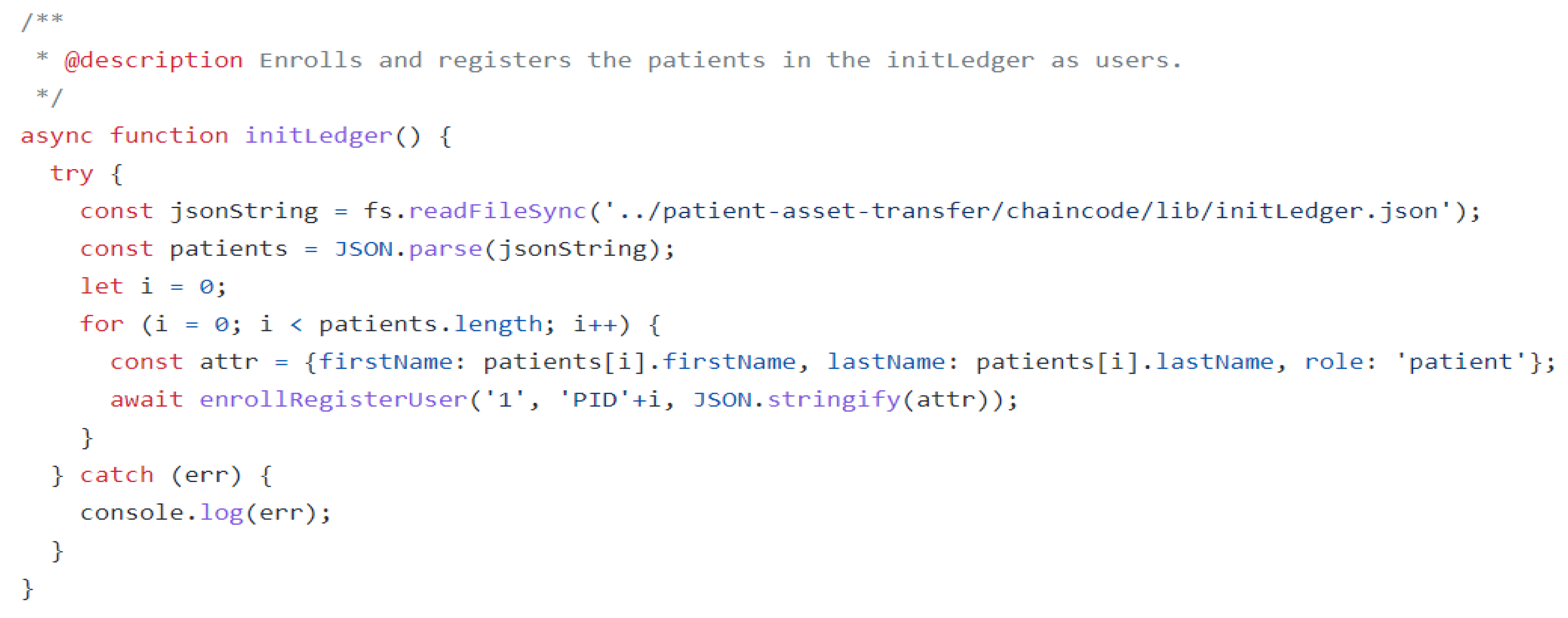
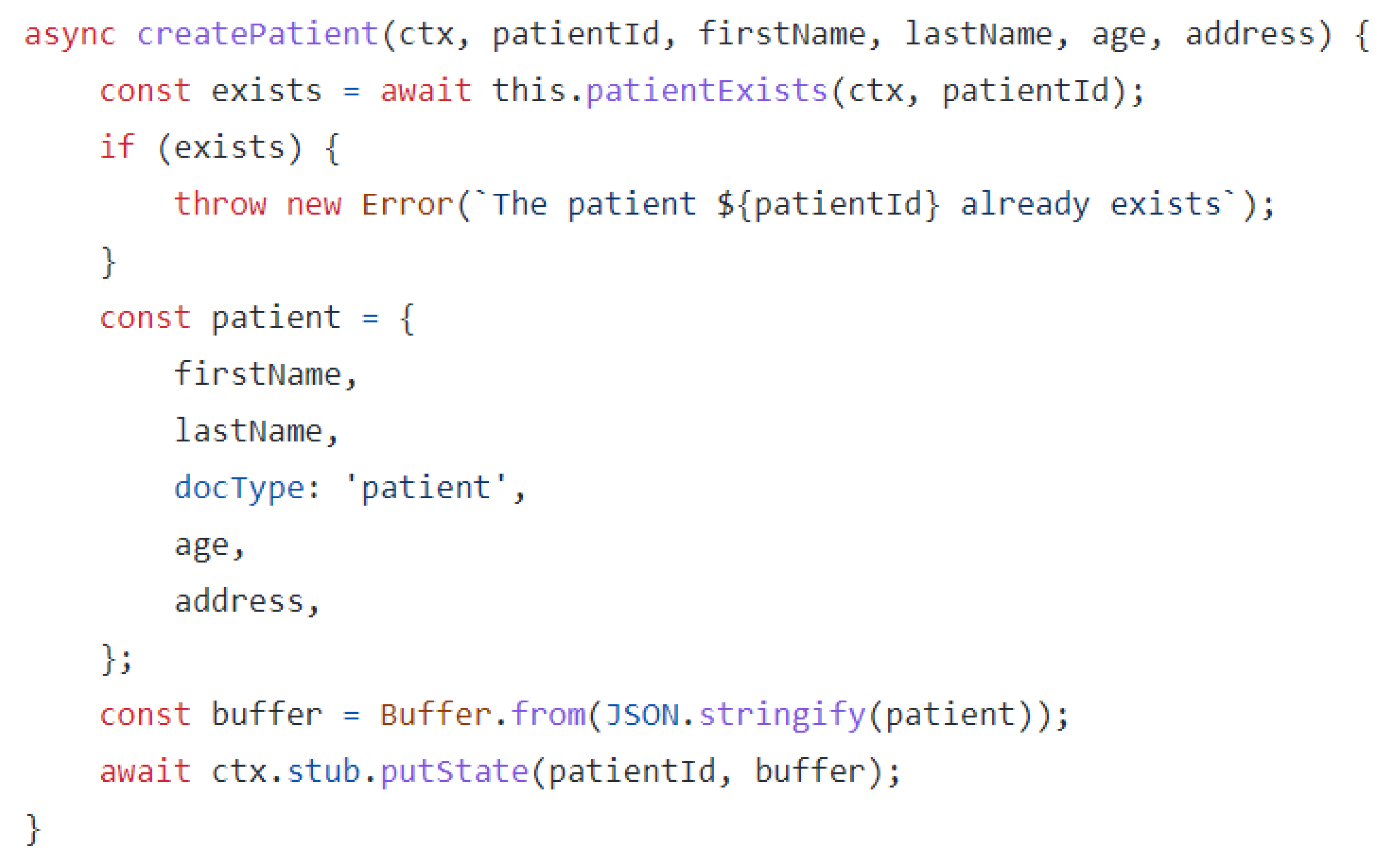
Appendix F. Create Patient in a Server

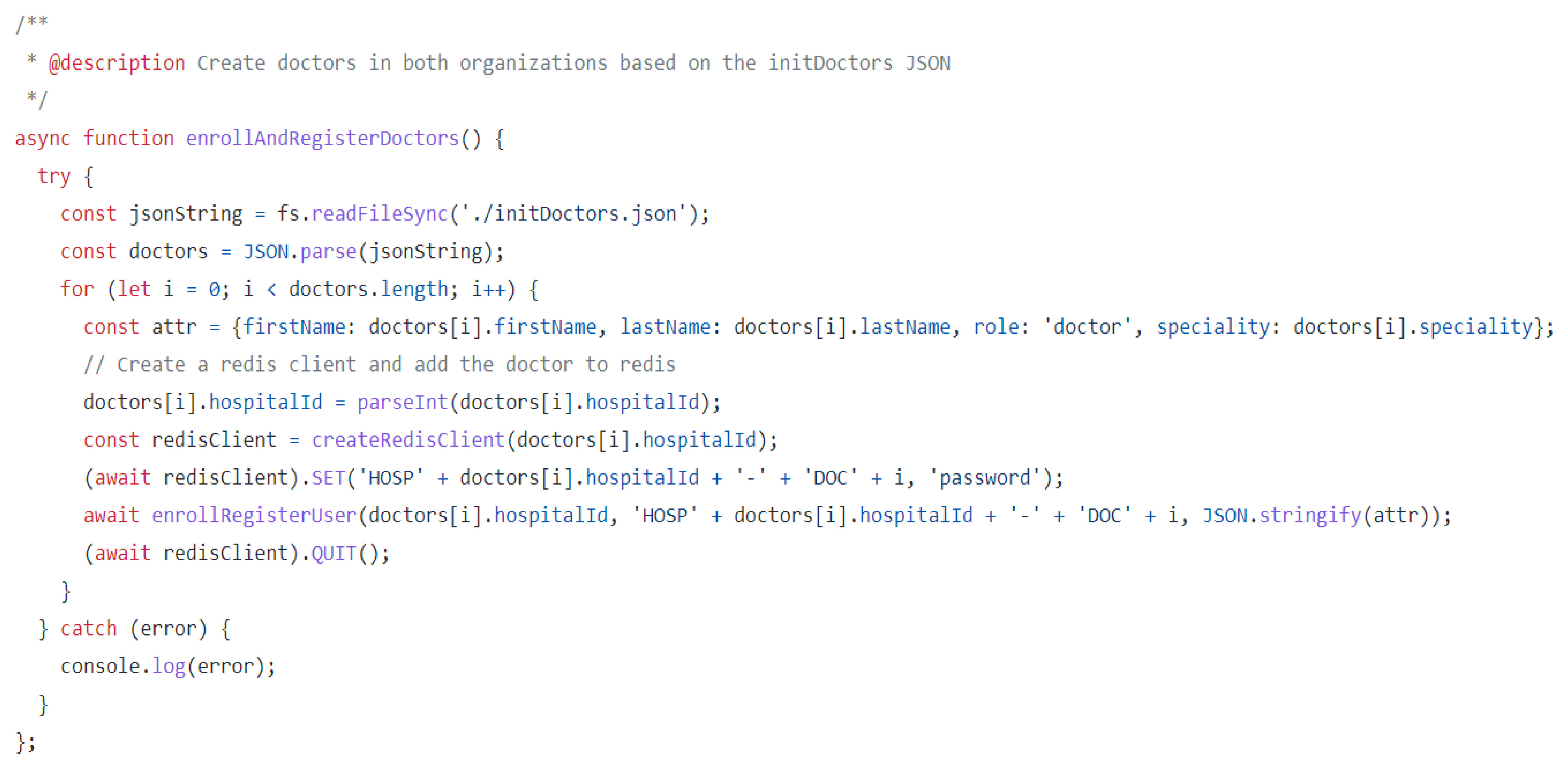
Appendix G. Create Doctor

References
- Universal Health Coverage Advocacy Guide. Available online: www.UHC2030.org (accessed on 4 August 2022).
- Katurura, M.C.; Cilliers, L. Electronic health record system in the public health care sector of South Africa: A systematic literature review. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hing, E.F.; Yang, N.F.; Jamoon, E.W. Adoption of Certified Electronic Health Record Systems and Electronic Information Sharing in Physician Offices: United States, 2013 and 2014. NCHS Data Brief 2016, 236, 1–8. [Google Scholar]
- Mandal, A.; Dumaru, P.; Bhandari, S.; Shrestha, S.; Shakya, S. Decentralized Electronic Health Record System. J. Inst. Eng. 2020, 15, 77–80. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.H.; Sim, I. Physicians’ Use of Electronic Medical Records: Barriers and Solutions. Health Aff. 2004, 23, 116–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, P.; Steinbach, M.; Kumar, V.; Simon, G. Mining Electronic Health Records (EHRs). ACM Comput. Surv. 2018, 50, 1–40. [Google Scholar] [CrossRef]
- Li, L.; Yue, Z.; Wu, G. Electronic Medical Record Sharing System Based on Hyperledger Fabric and InterPlanetary File System. In Proceedings of the ACM International Conference Proceeding Series, New York, NY, USA, 13 February 2021; pp. 149–154. [Google Scholar] [CrossRef]
- Ajami, S.; ArabChadegani, R. Barriers to implement Electronic Health Records (EHRs). Mater. Socio Medica 2013, 25, 213–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apathy, N.C.; Holmgren, A.J.; Adler-Milstein, J. A decade post-HITECH: Critical access hospitals have electronic health records but struggle to keep up with other advanced functions. J. Am. Med. Informatics Assoc. 2021, 28, 1947–1954. [Google Scholar] [CrossRef]
- Seh, A.H.; Zarour, M.; Alenezi, M.; Sarkar, A.K.; Agrawal, A.; Kumar, R.; Ahmad Khan, R. Healthcare Data Breaches: Insights and Implications. Healthcare 2020, 8, 133. [Google Scholar] [CrossRef]
- Chelladurai, U.; Pandian, S. A novel blockchain based electronic health record automation system for healthcare. J. Ambient. Intell. Humaniz. Comput. 2022, 13, 693–703. [Google Scholar] [CrossRef]
- Uddin, M.; Memon, M.S.; Memon, I.; Ali, I.; Memon, J.; Abdelhaq, M.; Alsaqour, R. Hyperledger Fabric Blockchain: Secure and Efficient Solution for Electronic Health Records. Comput. Mater. Contin. 2021, 68, 2377–2397. [Google Scholar] [CrossRef]
- Katuu, S. Transforming South Africa’s health sector: The eHealth Strategy, the implementation of electronic document and records management systems (EDRMS) and the utility of maturity models. J. Sci. Technol. Policy Manag. 2016, 7, 330–345. [Google Scholar] [CrossRef]
- Jardim, S.V. The Electronic Health Record and its Contribution to Healthcare Information Systems Interoperability. Procedia Technol. 2013, 9, 940–948. [Google Scholar] [CrossRef] [Green Version]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inform. 2016, 25, S48–S61. [Google Scholar] [CrossRef]
- Onuiri, E.E.; Idowu, S.A.; Komolafe, O. Electronic Health Record Systems and Cyber-Security Challenges. In Proceedings of the International Conference on African Development Issues, Ota, Nigeria, 11–13 May 2015. [Google Scholar]
- Lasi, H.; Fettke, P.; Kemper, H.G.; Feld, T.; Hoffmann, M. Industry 4.0. Bus. Inf. Syst. Eng. 2014, 6, 239–242. [Google Scholar] [CrossRef]
- Clauson, K.A.; Breeden, E.A.; Davidson, C.; Mackey, T.K. Leveraging Blockchain Technology to Enhance Supply Chain Management in Healthcare: An Exploration of Challenges and Opportunities in the Health Supply Chain. Blockchain Healthc Today 2018, 1, 1–12. [Google Scholar] [CrossRef]
- Beck, R. Beyond Bitcoin: The Rise of Blockchain World. Computer 2018, 51, 54–58. [Google Scholar] [CrossRef] [Green Version]
- Sunyaev, A. Distributed Ledger Technology. In Internet Computing; Springer: Cham, Switzerland, 2020; pp. 265–299. [Google Scholar]
- Paul, P.K. Blockchain Technology and its Types—A Short Review. Int. J. Appl. Sci. Eng. 2021, 9, 189–200. [Google Scholar] [CrossRef]
- Kuo, T.-T.; Kim, H.-E.; Ohno-Machado, L. Blockchain distributed ledger technologies for biomedical and health care applications. J. Am. Med. Inform. Assoc. 2017, 24, 1211–1220. [Google Scholar] [CrossRef] [Green Version]
- Khan, D.; Jung, L.T.; Hashmani, M.A. Systematic Literature Review of Challenges in Blockchain Scalability. Appl. Sci. 2021, 11, 9372. [Google Scholar] [CrossRef]
- Dharani, J.; Sundarakantham, K.; Kunwar, S.; Mercy Shalinie, S. A Privacy-Preserving Framework for Endorsement Process in Hyperledger Fabric. Comput. Secur. 2022, 116, 102637. [Google Scholar] [CrossRef]
- Sun, J.; Yao, X.; Wang, S.; Wu, Y. Blockchain-Based Secure Storage and Access Scheme for Electronic Medical Records in IPFS. IEEE Access 2020, 8, 59389–59401. [Google Scholar] [CrossRef]
- Castaldo, L.; Cinque, V. Blockchain-Based Logging for the Cross-Border Exchange of eHealth Data in Europe. In Communications in Computer and Information Science; Springer: Cham, Switzerland, 2018; Volume 821. [Google Scholar]
- Yue, X.; Wang, H.; Jin, D.; Li, M.; Jiang, W. Healthcare Data Gateways: Found Healthcare Intelligence on Blockchain with Novel Privacy Risk Control. J. Med. Syst. 2016, 40, 218. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.F.; ArunKumar, N.; Ramirez-Gonzalez, G.; Abdulhay, E.; Tavares, J.M.R.S.; de Albuquerque, V.H.C. A medical records managing and securing blockchain based system supported by a Genetic Algorithm and Discrete Wavelet Transform. Cogn. Syst. Res. 2018, 52, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.; Lin, X. Towards Secure and Privacy-Preserving Data Sharing in e-Health Systems via Consortium Blockchain. J. Med. Syst. 2018, 42, 140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G.; Rosenbloom, S.T. FHIRChain: Applying Blockchain to Securely and Scalably Share Clinical Data. Comput. Struct. Biotechnol. J. 2018, 16, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Cao, J.; Wu, H.; Yang, Y.; Ma, M.D.; He, J. BlocHIE: A BLOCkchain-Based Platform for Healthcare Information Exchange. In Proceedings of the 2018 IEEE International Conference on Smart Computing (SMARTCOMP), Taormina, Italy, 18–20 June 2018; pp. 49–56. [Google Scholar] [CrossRef]
- Al Omar, A.; Alam Bhuiyan, Z.; Basu, A.; Kiyomoto, S.; Rahman, M.S. Privacy-friendly platform for healthcare data in cloud based on blockchain environment. Futur. Gener. Comput. Syst. 2019, 95, 511–521. [Google Scholar] [CrossRef]
- Gutierrez, O.; Saavedra, J.J.; Zurbaran, M.; Salazar, A.; Wightman, P.M. User-Centered Differential Privacy Mechanisms for Electronic Medical Records. In Proceedings of the International Carnahan Conference on Security Technology, Montreal, QC, Canada, 22–25 October 2018. [Google Scholar] [CrossRef]
- Mandl, K.D.; Simons, W.W.; Crawford, W.C.R.; Abbett, J.M. Indivo: A personally controlled health record for health in-for-mation exchange and communication. BMC Med. Inform. Decis. Mak. 2007, 7, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, S.; He, D.; Li, L.; Kumar, N.; Khan, M.K.; Choo, K.-K.R. Applications of blockchain in ensuring the security and privacy of electronic health record systems: A survey. Comput. Secur. 2020, 97, 101966. [Google Scholar] [CrossRef]
- Zhu, L.; Wu, Y.; Gai, K.; Choo, K.-K.R. Controllable and trustworthy blockchain-based cloud data management. Futur. Gener. Comput. Syst. 2019, 91, 527–535. [Google Scholar] [CrossRef]
- Smart Contracts and Chaincode—Hyperledger-Fabricdocs Main Documentation. Available online: https://hyperledger-fabric.readthedocs.io/en/latest/smartcontract/smartcontract.html (accessed on 24 October 2022).
- Hyperledger Fabric SDK for Node.js Module: Fabric-Network. Available online: https://hyperledger.github.io/fabric-sdk-node/release-2.2/module-fabric-network.html (accessed on 24 October 2022).
- Wallet—Hyperledger-Fabricdocs Main Documentation. Available online: https://hyperledger-fabric.readthedocs.io/en/release-2.2/developapps/wallet.html (accessed on 24 October 2022).
- Proxy-Re-Encryption GitHub Topics. Available online: https://github.com/topics/proxy-re-encryption?l=javascript (accessed on 24 October 2022).
- Fernandes, A.; Rocha, V.; da Conceicao, A.F.; Horita, F. Scalable Architecture for sharing EHR using the Hyperledger Blockchain. In Proceedings of the 2020 IEEE International Conference on Software Architecture Companion, ICSA-C.2020, Salvador, Brazil, 16–20 March 2020. [Google Scholar] [CrossRef]
- Hyperledger JIRA. Available online: https://jira.hyperledger.org/browse/FABC-5094 (accessed on 24 October 2022).
- Tripathi, A.K.; Tripathi, M. A Framework of Distributed Database Management Systems in the Modern Organization and the Uncertainties removal. Int. J. Adv. Res. Comput. Sci. 2011, 2, 550–555. [Google Scholar]
- Abdullah, N.; Håkansson, A.; Moradian, E. Blockchain-based approach to enhance big data authentication in a distributed environment. In Proceedings of the Ninth International Conference on Ubiquitous and Future Networks (ICUFN), Milan, Italy, 4–7 July 2017; IEEE Computer Society: Washington, DC, USA, 2017; pp. 887–892. [Google Scholar]
- McHugh, J.; Abiteboul, S.; Goldman, R.; Quass, D.; Widom, J. Lore: A database management system for semistructured data. ACM Sigmod Rec. 1997, 26, 54–66. [Google Scholar] [CrossRef]
- Stephen, R.; Alex, A. A review on blockchain security. In IOP Conference Series: Materials Science and Engineering; IOP Publishing: Bristol, UK, 2018; p. 012030. Volume 396, No. 1. [Google Scholar]
- Muqorobin, M.; Rais, N.A.R. Comparison of PHP Programming Language with Codeigniter Framework in Project CRUD. Int. J. Comput. Inf. Syst. IJCIS 2022, 3, 94–98. [Google Scholar] [CrossRef]
- Knutsen, K.E.; Liang, Q.; Karandikar, N.; Ibrahim, I.H.B.; Tong, X.G.T.; Tam, J.J.H. Containerized immutable maritime data sharing utilizing Distributed Ledger Technologies. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2022; p. 012006. Volume 2311, No. 1. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Public Blockchain (Ethereum) | Private Blockchain (HLF) | |
|---|---|---|
| Smart contracts | Written in Solidity, Migration | Java, JavaScript, Golang |
| Consensus | proof-of-stake (PoS), proof-of-work (PoW) | Different approaches |
| Scalability | Low | Higher |
| Privacy | Transactions are private | Transactions are private |
| Cost | High | Low |
| Crypto | Mining Ethers | None |
| Transaction speed | 20 tps | Greater than 2000 tps |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndzimakhwe, M.; Telukdarie, A.; Munien, I.; Vermeulen, A.; Chude-Okonkwo, U.K.; Philbin, S.P. A Framework for User-Focused Electronic Health Record System Leveraging Hyperledger Fabric. Information 2023, 14, 51. https://doi.org/10.3390/info14010051
Ndzimakhwe M, Telukdarie A, Munien I, Vermeulen A, Chude-Okonkwo UK, Philbin SP. A Framework for User-Focused Electronic Health Record System Leveraging Hyperledger Fabric. Information. 2023; 14(1):51. https://doi.org/10.3390/info14010051
Chicago/Turabian StyleNdzimakhwe, Mandla, Arnesh Telukdarie, Inderasan Munien, Andre Vermeulen, Uche K. Chude-Okonkwo, and Simon P. Philbin. 2023. "A Framework for User-Focused Electronic Health Record System Leveraging Hyperledger Fabric" Information 14, no. 1: 51. https://doi.org/10.3390/info14010051