Cloud Based Virtual Reality Exposure Therapy Service for Public Speaking Anxiety †

Abstract
:1. Introduction
2. Related Works
3. System Development
3.1. Hardware Selection
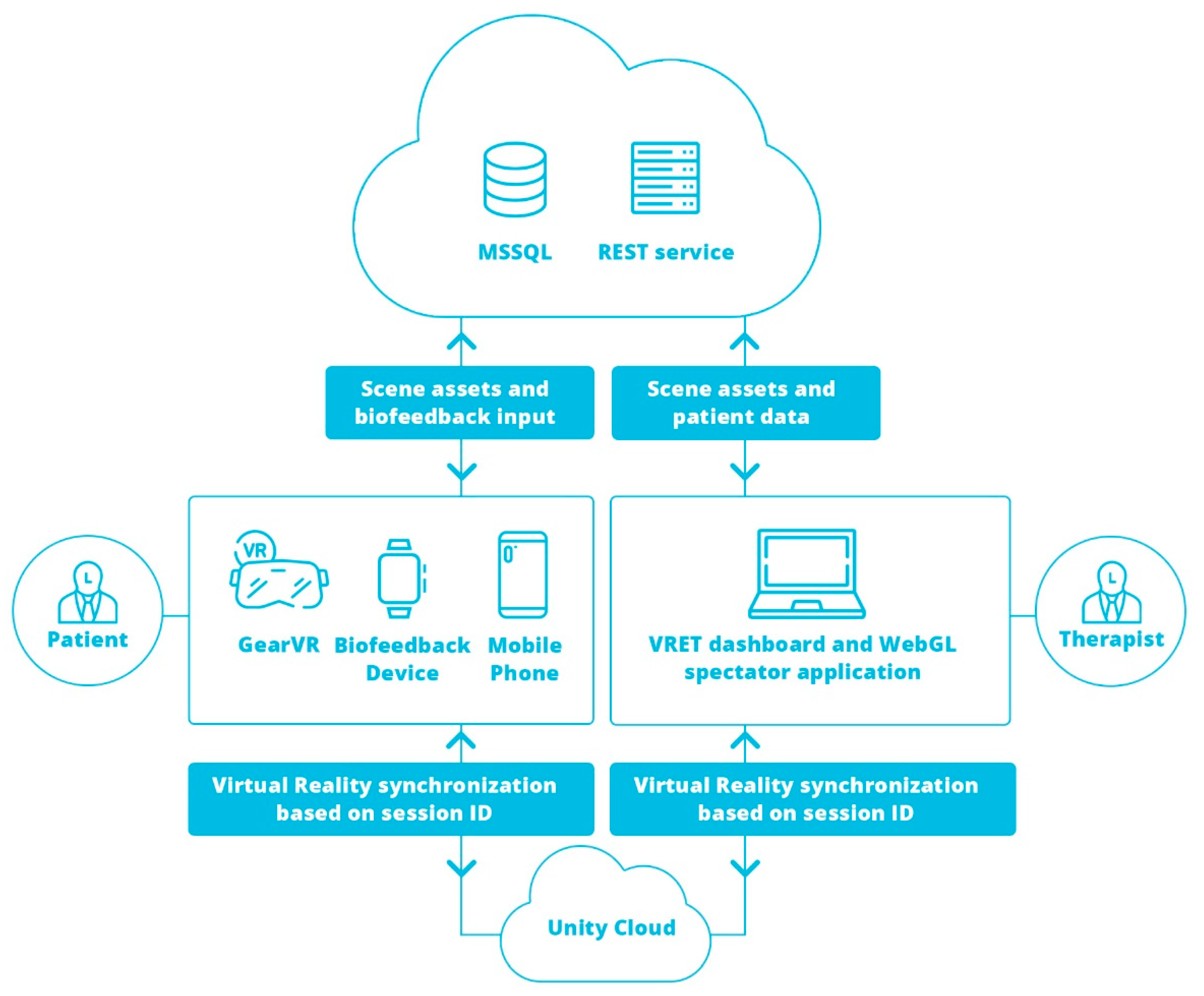
3.2. System Architecture
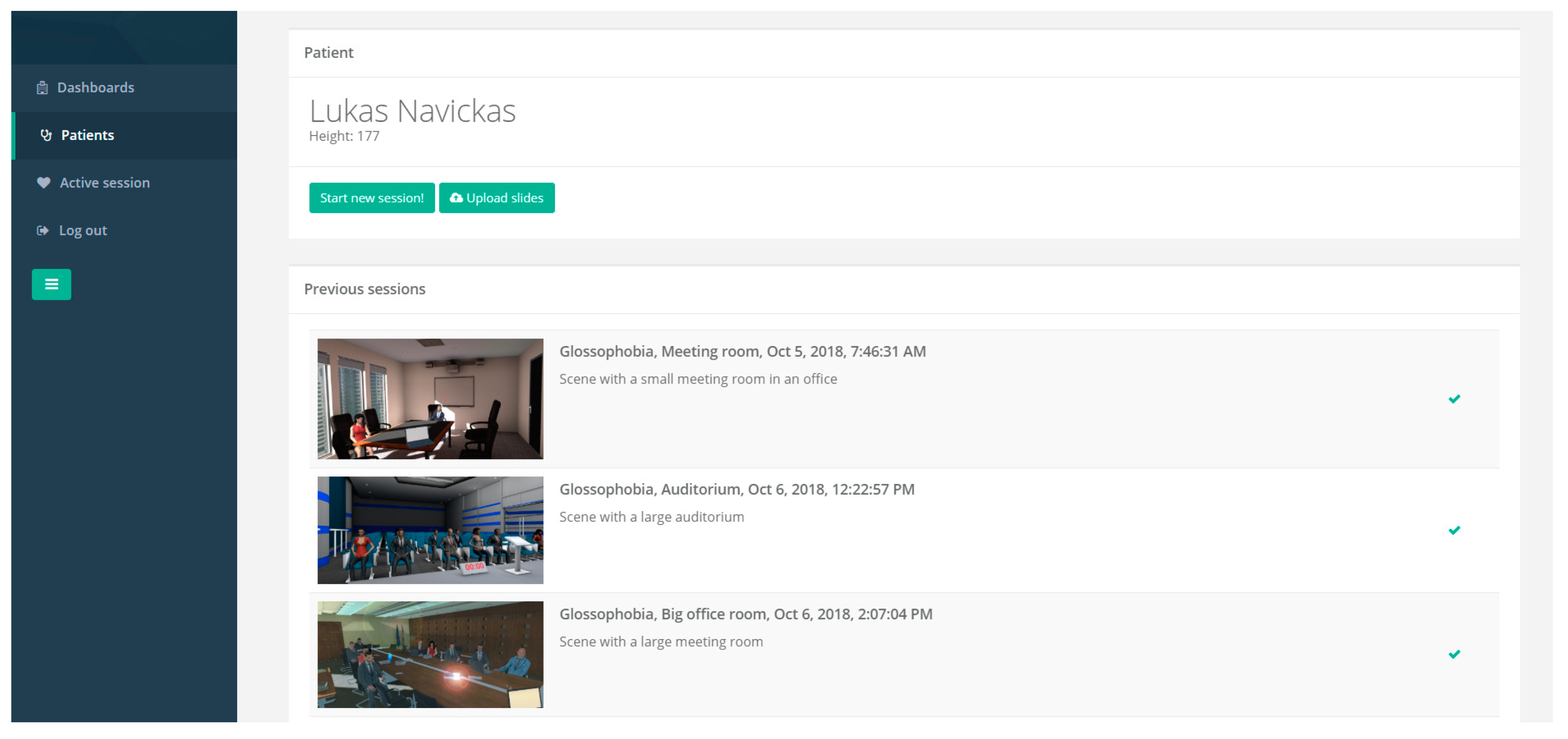
3.3. Therapist Dashboard
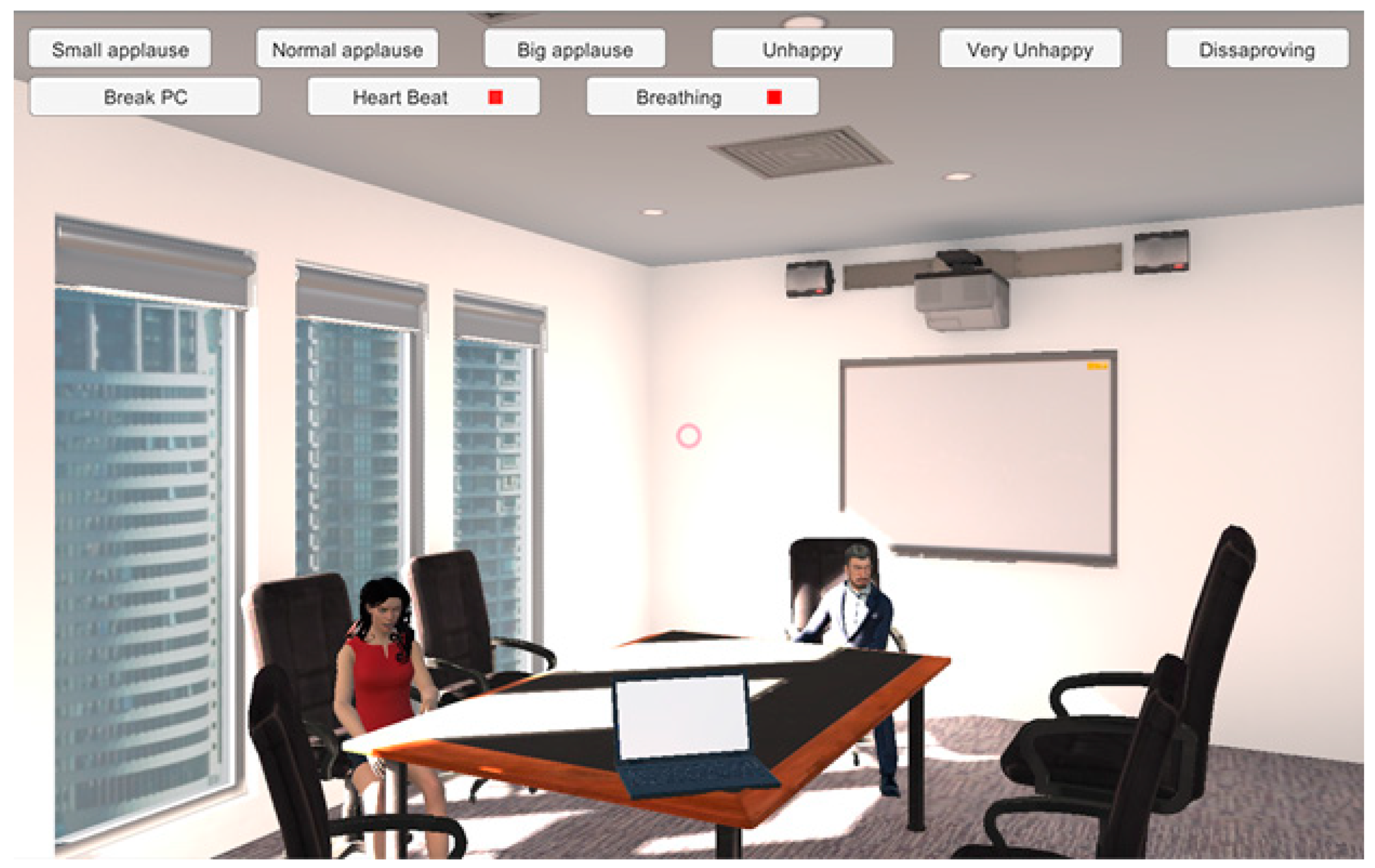
3.4. VRET Spectator Application
3.5. Virtual Reality Application
3.6. System Usage Workflow
4. VRET Module for Public Speaking Anxiety
4.1. Interaction and Session Settings
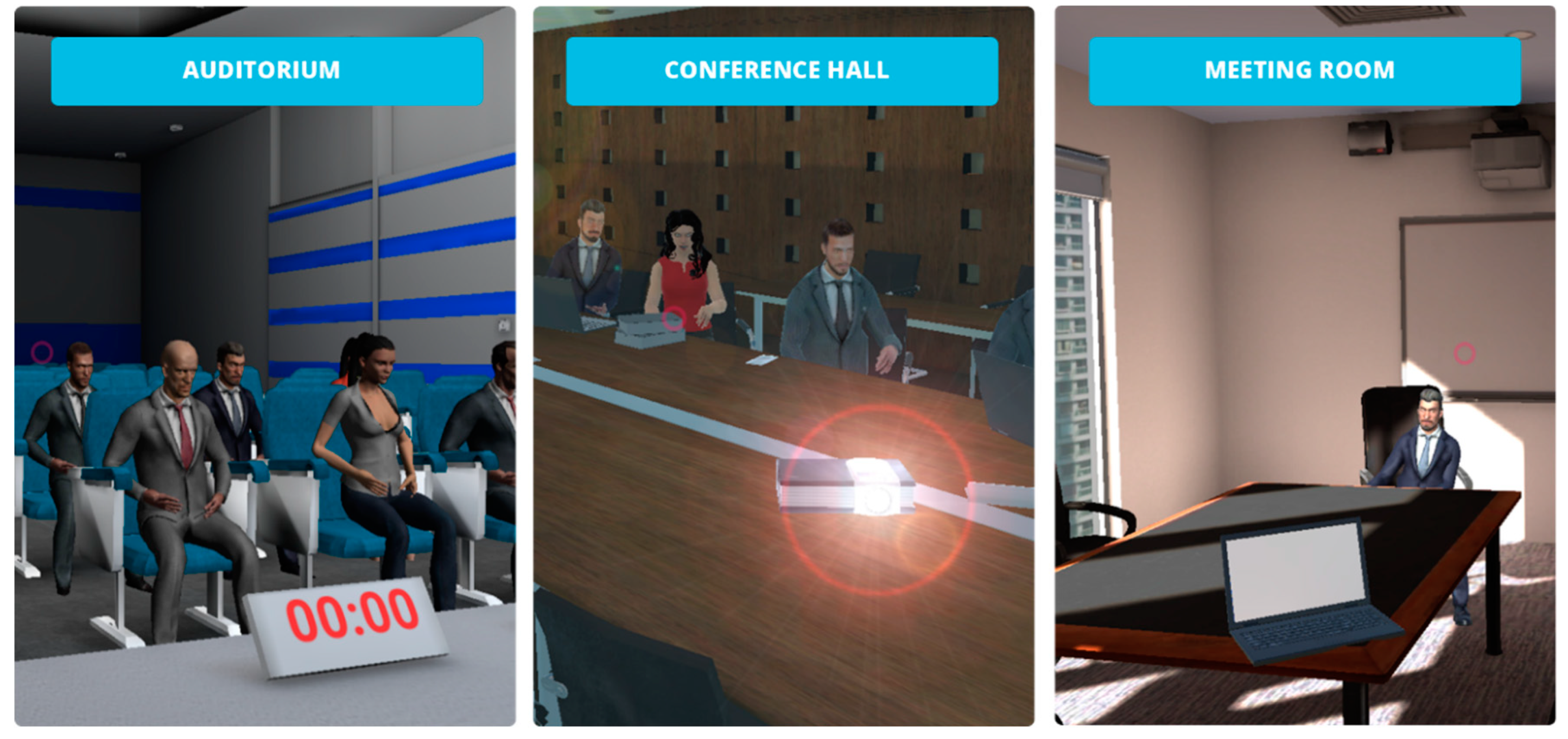
4.2. VR Environments for Treatment of Public Speaking Anxiety
4.2.1. Meeting Room
4.2.2. Conference Room
4.2.3. Auditorium
4.3. Biofeedback Tracking
5. Experiment
5.1. Participants Demographics
5.2. Flow of the Experiment
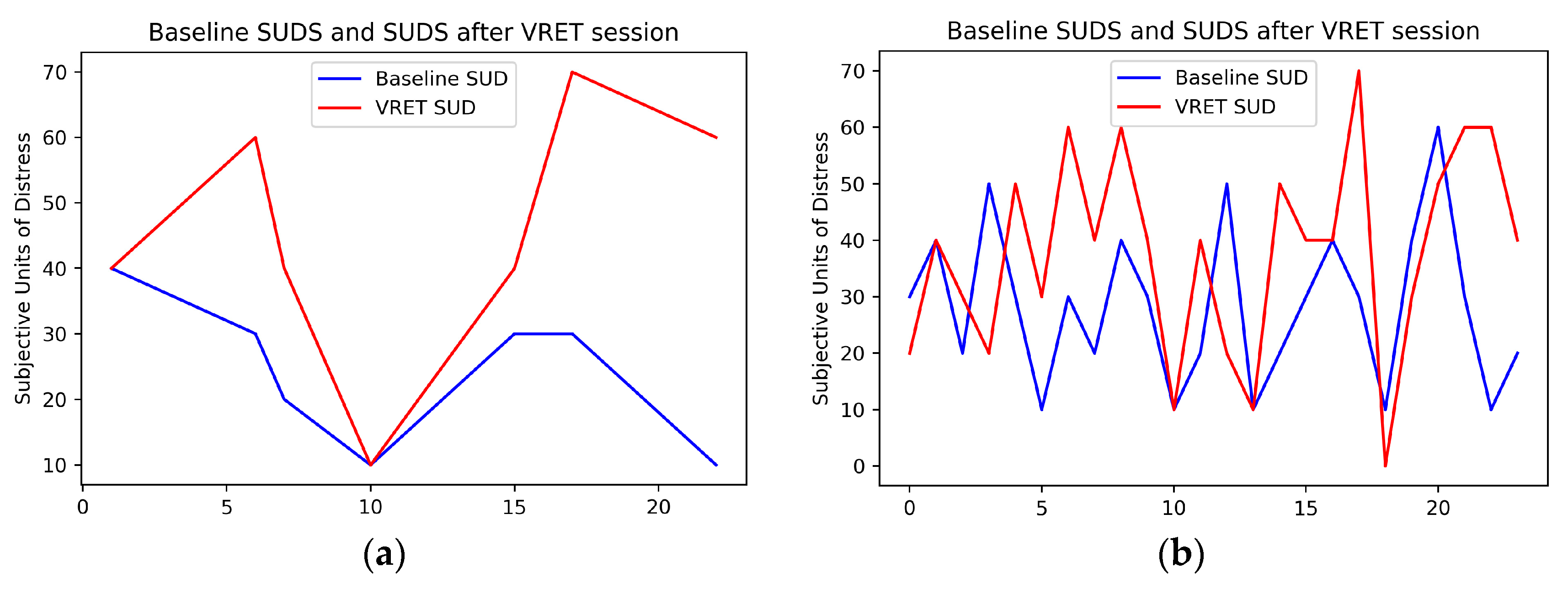
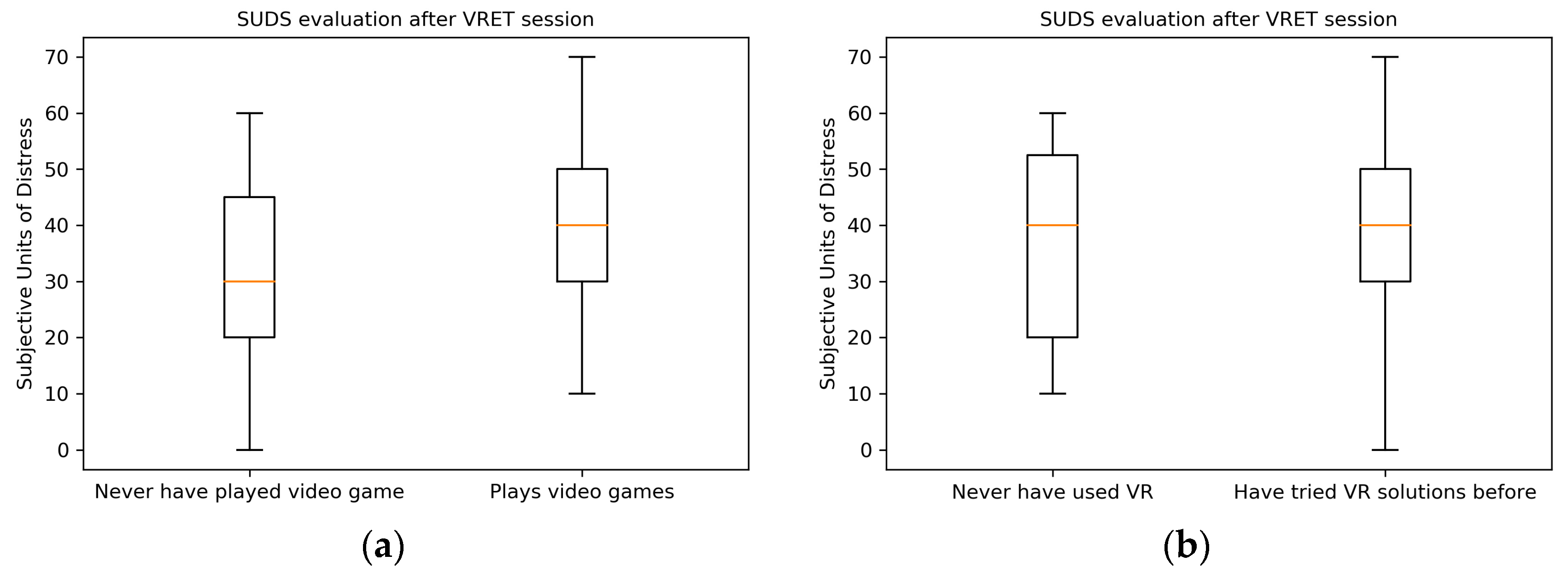
5.3. Subjective Units of Distress Scale (SUDS) and Subjective Symptoms of Discomfort
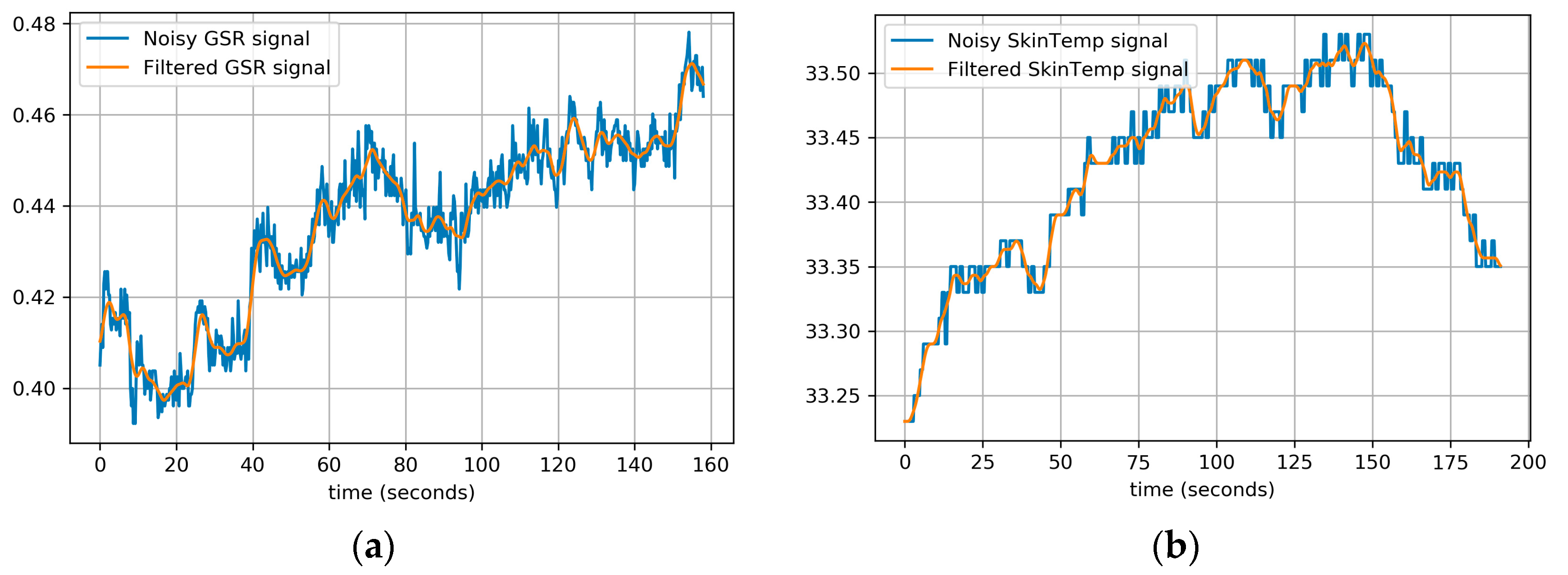
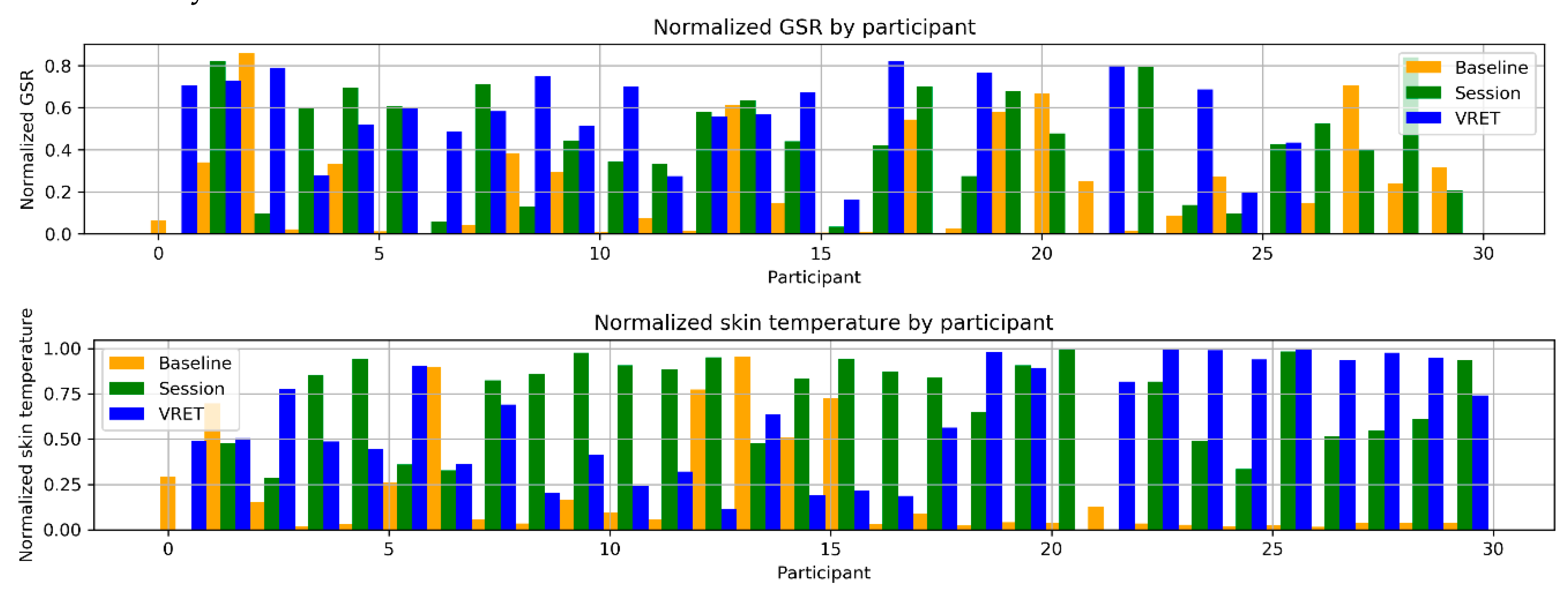
5.4. Biofeedback Data Collection
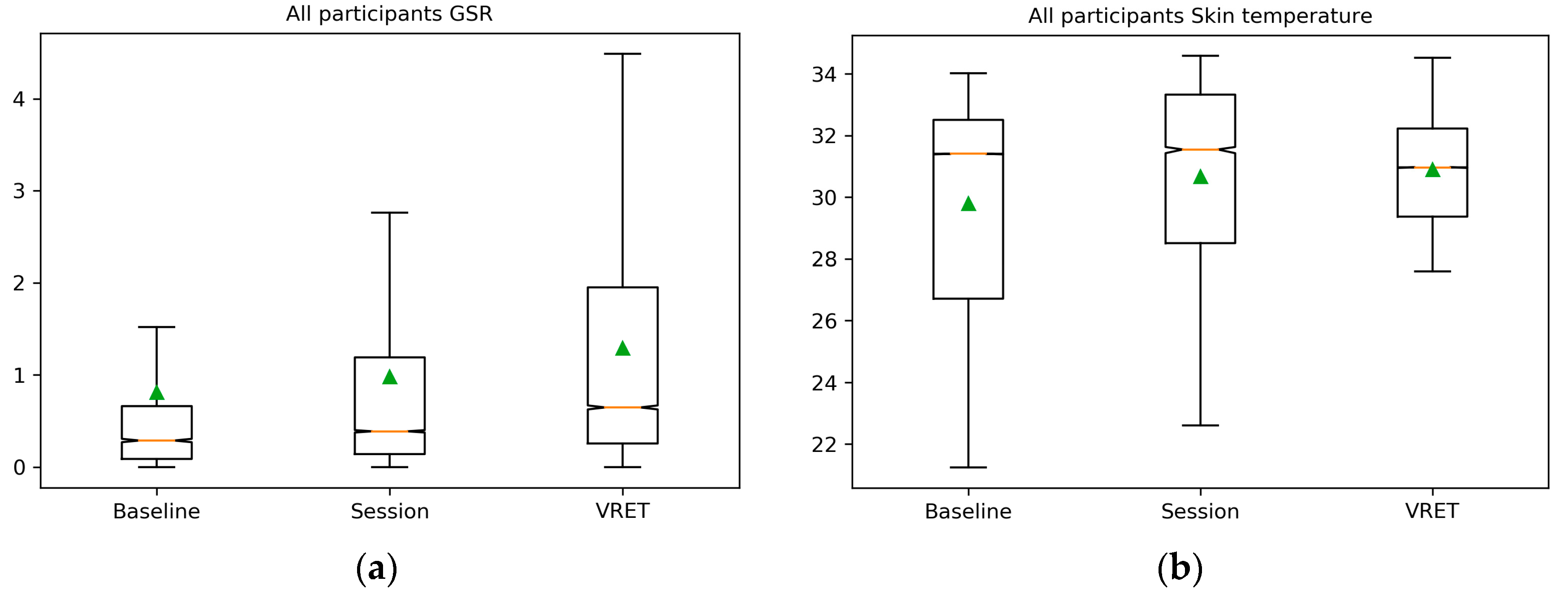
5.5. Galvanic Skin Response and Skin Temperature Feature Analysis
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593. [Google Scholar] [CrossRef] [PubMed]
- McCann, R.A.; Armstrong, C.M.; Skopp, N.A.; Edwards-Stewart, A.; Smolenski, D.J.; June, J.D.; Metzger-Abamukong, M.; Reger, G.M. Virtual reality exposure therapy for the treatment of anxiety disorders: An evaluation of research quality. J. Anxiety Disord. 2014, 28, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Owens, M.E.; Beidel, D.C. Can Virtual Reality Effectively Elicit Distress Associated with Social Anxiety Disorder? J. Psychopathol. Behav. Assess. 2015, 37, 296–305. [Google Scholar] [CrossRef]
- Valmaggia, L.R.; Latif, L.; Kempton, M.J.; Rus-Calafell, M. Virtual reality in the psychological treatment for mental health problems: A systematic review of recent evidence. Psychiatry Res. 2016, 236, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Diemer, J.; Alpers, G.W.; Peperkorn, H.M.; Shiban, Y.; hlberger, A.M. The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 2015, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Raghav, K.; Wijk, A.J.V.; Abdullah, F.; Islam, M.N.; Bernatchez, M.; Jongh, A.D. Efficacy of virtual reality exposure therapy for treatment of dental phobia: A randomized control trial. BMC Oral Health 2016, 16, 25. [Google Scholar] [CrossRef] [PubMed]
- Tudor, A.D.; Poeschl, S.; Doering, N. Virtual audience customization for public speaking training procedures. In Proceedings of the 2013 IEEE Virtual Reality (VR), Lake Buena Vista, FL, USA, 18–20 March 2013; pp. 61–62. [Google Scholar]
- Botella, C.; Fernández-Álvarez, J.; Guillén, V.; García-Palacios, A.; Baños, R. Recent Progress in Virtual Reality Exposure Therapy for Phobias: A Systematic Review. Curr. Psychiatry Rep. 2017, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Carl, E.; Stein, A.T.; Levihn-Coon, A.; Pogue, J.R.; Rothbaum, B.; Emmelkamp, P.; Asmundson, G.J.; Carlbring, P.; Powers, M.B. Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials. J. Anxiety Disord. 2019, 61, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Levy, F.; Leboucher, P.; Rautureau, G.; Jouvent, R. E-virtual reality exposure therapy in acrophobia: A pilot study. J. Telemed. Telecare 2016, 22, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Lindner, P.; Miloff, A.; Fagernäs, S.; Andersen, J.; Sigeman, M.; Andersson, G.; Furmark, T.; Carlbring, P. Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: A randomized controlled trial. J. Anxiety Disord. 2019, 61, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Wiederhold, B.K.; Miller, I.T.; Wiederhold, M.D. Using Virtual Reality to Mobilize Health Care: Mobile Virtual Reality Technology for Attenuation of Anxiety and Pain. IEEE Consum. Electron. Mag. 2018, 7, 106–109. [Google Scholar] [CrossRef]
- Freeman, D.; Haselton, P.; Freeman, J.; Spanlang, B.; Kishore, S.; Albery, E.; Denne, M.; Brown, P.; Slater, M.; Nickless, A. Automated psychological therapy using immersive virtual reality for treatment of fear of heights: A single-blind, parallel-group, randomised controlled trial. Lancet Psychiatry 2018, 5, 625–632. [Google Scholar] [CrossRef]
- Manju, T.; Padmavathi, S.; Tamilselvi, D. A Rehabilitation Therapy for Autism Spectrum Disorder Using Virtual Reality. In Proceedings of the International Conference on Intelligent Information Technologies, Chennai, India, 20–22 December 2017. [Google Scholar]
- Miloff, A.; Lindner, P.; Hamilton, W.; Reuterskiöld, L.; Andersson, G.; Carlbring, P. Single-session gamified virtual reality exposure therapy for spider phobia vs. traditional exposure therapy: Study protocol for a randomized controlled non-inferiority trial. Trials 2016, 17, 60. [Google Scholar] [CrossRef] [PubMed]
- Shiban, Y.; Diemer, J.; Müller, J.; Brütting-Schick, J.; Pauli, P.; Mühlberger, A. Diaphragmatic breathing during virtual reality exposure therapy for aviophobia: Functional coping strategy or avoidance behavior? A pilot study. BMC Psychiatry 2017, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Skulimowski, S.; Badurowicz, M. Wearable sensors as feedback method in virtual reality anti-stress therapy. In Proceedings of the 2017 International Conference on Electromagnetic Devices and Processes in Environment Protection with Seminar Applications of Superconductors (ELMECO & AoS), Lublin, Poland, 3–6 December 2017; pp. 1–4. [Google Scholar]
- Seol, E.; Cho, C.H.; Choi, S.; Jung, D.; Min, S.; Seo, S.; Jung, S.; Lee, Y.; Lee, J.; Kim, G.; Cho, C.; Lee, S. “Drop the beat”: Virtual reality based mindfulness and cognitive behavioral therapy for panic disorder—A pilot study. In Proceedings of the 23rd ACM Symposium on Virtual Reality Software and Technology—VRST ’17, Gothenburg, Sweden, 8–10 November 2017; pp. 1–3. [Google Scholar]
- Suyanto, E.M.; Angkasa, D.; Turaga, H.; Sutoyo, R. Overcome Acrophobia with the Help of Virtual Reality and Kinect Technology. Procedia Comput. Sci. 2017, 116, 476–483. [Google Scholar] [CrossRef]
- Shunnaq, S.; Raeder, M. VirtualPhobia: A Model for Virtual Therapy of Phobias. In Proceedings of the 2016 XVIII Symposium on Virtual and Augmented Reality (SVR), Gramado, Brazil, 21–24 June 2016; pp. 59–63. [Google Scholar]
- Rauch, S.A.; Koola, C.; Post, L.; Yasinski, C.; Norrholm, S.D.; Black, K.; Rothbaum, B.O. In session extinction and outcome in Virtual Reality Exposure Therapy for PTSD. Behav. Res. Ther. 2018, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zinzow, H.M.; Brooks, J.O.; Rosopa, P.J.; Jeffirs, S.; Jenkins, C.; Seeanner, J.; McKeeman, A.; Hodges, L.F. Virtual Reality and Cognitive-Behavioral Therapy for Driving Anxiety and Aggression in Veterans: A Pilot Study. Cogn. Behav. Pract. 2018, 25, 296–309. [Google Scholar] [CrossRef]
- Bun, P.; Gorski, F.; Grajewski, D.; Wichniarek, R.; Zawadzki, P. Low—Cost Devices Used in Virtual Reality Exposure Therapy. Procedia Comput. Sci. 2017, 104, 445–451. [Google Scholar] [CrossRef]
- Marquardt, A.; Trepkowski, C.; Maiero, J.; Kruijff, E.; Hinkeniann, A. Multisensory Virtual Reality Exposure Therapy. In Proceedings of the 2018 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Reutlingen, Germany, 18–22 March 2018; pp. 769–770. [Google Scholar]
- Walkom, G. Virtual Reality Exposure Therapy: To Benefit Those Who Stutter and Treat Social Anxiety. In Proceedings of the 2016 International Conference on Interactive Technologies and Games (ITAG), Nottingham, UK, 26–27 October 2016; pp. 36–41. [Google Scholar]
- Christofi, M.; Michael-Grigoriou, D. Virtual environments design assessment for the treatment of claustrophobia. In Proceedings of the 22nd International Conference on Virtual System & Multimedia (VSMM), Kuala Lumpur, Malaysia, 17–21 October 2016; pp. 1–8. [Google Scholar]
- Poeschl, S.; Doering, N. Virtual training for Fear of Public Speaking—Design of an audience for immersive virtual environments. In Proceedings of the 2012 IEEE Virtual Reality (VR), Costa Mesa, CA, USA, 4–8 March 2012; pp. 101–102. [Google Scholar]
- Picard, R.; Vyzas, E.; Healey, J.N. Towards Machine Emotional Intelligence: Analysis of Affective Psychological State. IEEE Trans. Pattern Anal. Mach. Intell. 2001, 23, 1175–1191. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Value |
|---|---|
| Age | M = 26.85, SD = 4.189 |
| Sex | Female (13), Male (17) |
| Employment | Studies (7), Works (23) |
| VR experience | Never (13), Rare (16), Frequent (4) |
| Video games experience | Never (10), Rare (9), Frequent (11) |
| Measure | Rating |
|---|---|
| Highest anxiety/distress ever felt | 100 |
| Extremely anxious/distressed | 90 |
| Very anxious/distressed; can’t concentrate | 80 |
| Quite anxious/distressed; interference with functioning | 70 |
| Moderate to strong anxiety or distress | 60 |
| Moderate anxiety or distress, but can continue to function | 50 |
| Mild to moderate anxiety or distress | 40 |
| Mild anxiety or distress; no interference with functioning | 30 |
| Minimal anxiety or distress | 20 |
| Alert and awake | 10 |
| Measure | During Public Speaking | Public Speaking during VRET Session |
|---|---|---|
| Increased sweating | 26.09% | 39.13% |
| Dizziness | 8.70% | 13.04% |
| Increased heart rate | 78.26% | 69.57% |
| Shivers | 21.74% | 21.74% |
| Uneasiness, fear | 69.57% | 60.87% |
| Heavy chest | 8.70% | 8.70% |
| Muscle tension | 30.43% | 43.48% |
| Loss of balance | 8.70% | 26.09% |
| Nausea | 0.00% | 4.35% |
| Feature | Formula |
|---|---|
| Mean absolute of the raw signal | |
| Standard deviation of the raw signal | |
| Mean absolute of first difference (raw signal) | |
| Mean absolute of first difference (normalized signal) | |
| Mean absolute of second difference (raw signal) | |
| Mean absolute of second difference (normalized signal) |
| Feature | Baseline GSR/Skin temp. | Session GSR/Skin temp. | VRET GSR/Skin temp. |
|---|---|---|---|
| Raw signal mean absolute | 1.152/29.74 | 1.257/30.72 | 1.372/31.21 |
| Raw signal standard deviation | 0.07/0.04 | 0.22/0.023 | 0.106/0.019 |
| Raw signal absolute mean of first difference | 0.0044/0.0015 | 0.0121/0.011 | 0.0065/0.0011 |
| Normalized signal absolute mean of first difference | 0.056/0.058 | 0.036/0.018 | 0.021/0.019 |
| Raw signal absolute mean of second difference | 0.0008/0.0003 | 0.0019/0.00028 | 0.0014/0.0003 |
| Normalized signal absolute mean of second difference | 0.0116/0.0149 | 0.0077/0.0054 | 0.0049/0.0057 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šalkevičius, J.; Miškinytė, A.; Navickas, L. Cloud Based Virtual Reality Exposure Therapy Service for Public Speaking Anxiety. Information 2019, 10, 62. https://doi.org/10.3390/info10020062
Šalkevičius J, Miškinytė A, Navickas L. Cloud Based Virtual Reality Exposure Therapy Service for Public Speaking Anxiety. Information. 2019; 10(2):62. https://doi.org/10.3390/info10020062
Chicago/Turabian StyleŠalkevičius, Justas, Audronė Miškinytė, and Lukas Navickas. 2019. "Cloud Based Virtual Reality Exposure Therapy Service for Public Speaking Anxiety" Information 10, no. 2: 62. https://doi.org/10.3390/info10020062