2. STS in Religious Leaders
The literature exploring the negative impact of doing trauma work has highlighted the prevalence and salience of STS. In a survey of social workers,
Choi (
2011) found the existence of one or more STS symptoms in most of the respondents, with one-third of the social workers indicating moderate to severe symptoms. Overall, mild levels of PTSD were reported among the respondents; however, 65% of the participants testified to the occurrence of at least one symptom of STS. Over half of the participants informed the researchers of intrusive symptoms, and approximately 21% reported intrusion, avoidance, and arousal (
Choi 2011).
Similarly, a study conducted by
Bride (
2007) on a separate sample of social workers found that 70.2% experienced at least one symptom of STS in the prior week. Of these participants, 15.2% met the criteria for PTSD and 55% met the criteria for one of the main symptom clusters. Intrusive thoughts, avoidance of clients, and emotional numbing were the most prominently reported symptoms. In this pool of participants, 40.5% reported thinking about their work with clients without meaning to do so. Though 45% of social workers did not experience STS symptoms, over half the sample met at least one criterion for PTSD, and 15.2% met all the central diagnostic criteria. Finally, 86.7% of the respondents indicated feeling fear, horror, and helplessness in response to hearing about the trauma of their clients. Overall, research findings have suggested the high susceptibility of those who work closely with traumatized individuals to STS. However, documentation of the prevalence of STS in African American religious leaders is lacking.
Church congregants often seek out religious leaders for support in the aftermath of traumatic experiences (
Wang et al. 2014). Clergy members are typically in long-term relationships with individuals and their families in which they assist in providing specialized care not only immediately following traumatic experiences but also for those facing mental illnesses such as anxiety, depression, and PTSD. A 2003 study reported that clergy were called upon for such frontline work in greater amounts than even psychiatrists or medical doctors; notably, approximately 25% of those seeking treatment for mental disorders did so from the clergy (
Wang et al. 2003). Furthermore, clergy acted in noteworthy supportive roles following the 9/11 terrorist attacks, which led to the development of significant levels of compassion fatigue for some of the clergy (
Flannelly et al. 2005;
Taylor et al. 2006).
Another study that examined 99 Black pastors discovered that 40% of the pastors encountered severely mentally ill congregant members. Additionally, two-thirds of the pastors reported counseling congregants with suicidal proclivities, with ten percent of these involvements being linked to a crisis (
Payne 2014). Moreover, religious leaders are often called upon as a means for care and support for those who have faced or are currently facing the trauma of intimate partner violence and abuse as well as sexual abuse (
Davis and Johnson 2020;
Rudolfsson and Tidefors 2009;
St. Vil et al. 2016). In a qualitative study of thirteen African American clergy members, each one described having been contacted for guidance on this subject during their tenure (
Davis and Johnson 2020). Black women frequently mention religion as an important basis when looking for assistance to deal with intimate partner violence and abuse. In addition to their belief in God and their religion, many Black women shared in a semi-structured interview that clergy or other members of the church helped them bear or overcome the violence experienced by their abusers (
St. Vil et al. 2016).
The scores of religious leaders on common measures of STS symptomology have resembled the scores of mental health professionals (
Hendron et al. 2011;
Holaday et al. 2001). In a qualitative interview study of Irish clergy who work with trauma, half of the clergy were experiencing a high number of symptoms of STS, and half were experiencing a low number of symptoms. The clergy described the emotional, behavioral, physical, familial, and spiritual impacts of STS. They indicated feeling emotionally overwhelmed, guilty, sad, distanced, and detached, as well as having trouble sleeping and nightmares. Furthermore, some suggested tertiary traumatization as they described the strain put on their spouses as they listened to upsetting accounts. Though none signified that their faith in God had been negatively tainted, some stated that their faith in organized religion was damaged (
Hendron et al. 2011). A study of 1458 Roman Catholic ministers found that high levels of burnout existed within the sample. Over a third of the Catholic priests stated that they felt used up after a day of ministry and felt that parishioners blame them for some of their problems. Additionally, over a quarter stated that they are working too hard in their ministry, working with people all day puts a burden on them, they are less patient with parishioners than they used to be, and they find it difficult to attend to parishioners (
Francis et al. 2004).
The challenges that Black church leaders face related to burnout and STS are compounded by the need to shepherd congregants whose lives are deeply affected by living within racially unjust systems. In addition to the trauma faced by their congregants, many pastors are also processing their own experiences of racial trauma. Not only are they caring for their communities, but they also must find the time and resources to care for themselves.
Baum (
2014) found that when professionals faced double exposure due to the shared traumatic reality of the times, the main qualities of double exposure were significantly related to primary traumatization, secondary traumatization, and general symptomatology of distress. The key features of double exposure include intrusive anxiety, lapses in empathy, and changes in place and time of work (
Baum 2014). Additionally, those pastors serving in a “traumatic church”, which is categorized by elevated stress and conflict, were expected to have high emotional exhaustion that carried on even after they left that congregation (
Doolittle 2010).
Though it is evident that support is vital for helping professionals to aid them in coping with the struggles associated with providing care to traumatized individuals, clergy often differ from mental health professionals in their access to support and consultation services. Mental health professionals often have supervision and peer support built into the model of their practice and training. They are trained to recognize and care for the personal stress that comes with the emotional burden of caring. However, clergy often lack spaces to discuss the problems they encounter as well as their reactions to these problems (
Holaday et al. 2001). Furthermore, dual relationships cause issues for clergy in a way that mental health professionals do not often have to face. The numerous roles that pastors play in their communities sometimes constrain their ability to form intimate friendships within their church communities (
Holaday et al. 2001). Additionally, religious leaders typically receive limited training in basic counseling skills and providing trauma-informed care. Many have conveyed the wish that they had structured training in areas regarding mental health care. Moreover, many religious leaders have communicated that they remain interested in receiving further education about these subjects (
Holaday et al. 2001).
3. ACEs, Trauma, and STS in African American Communities
In conjunction with the Centers for Disease Control,
Felitti et al. (
1998) created the ACEs Questionnaire to explore the impact of trauma and other stressful experiences in childhood. Since the creation of the questionnaire, ACEs have become a major construct in mental and physical health research, which has led to countless studies showing the lingering negative physical and mental health outcomes of such adverse experiences (
Mosley-Johnson et al. 2021). In comparison with White individuals, those identifying as Latinx, Black, and American Indian are more likely to experience over four ACEs (
Assini-Meytin et al. 2021). Conversely, benevolent childhood experiences (BCEs) have recently emerged as a construct that counters some of the deleterious effects of ACEs (
Bethell et al. 2019;
Narayan et al. 2021).
Although White people experience depression and other mood disorders more frequently, research suggests that African Americans may experience them with increased severity and persistence (Pérez
Benítez et al. 2014;
Williams 2008). Historical institutional slavery and continuing expressions of racism continue to negatively impact the quality of life of African Americans. Depression and trauma often go hand in hand, and these societal issues compound the stress of African Americans. The stress and the consequences of trauma that many African Americans experience daily frequently aggravate these symptoms even further (
Streets 2015;
Williams and Mohammed 2009;
Woods-Giscombe 2010). Many individuals within the Black community experience depression as a symptom that is secondary to prior trauma exposure. Thus, their situation does not always fit deftly into the DSM-V criteria for depression or the diagnosis of PTSD but rather bears some facets of both conditions (
Streets 2015).
PTSD and other trauma spectrum disorders can be extremely incapacitating and trouble African Americans at disproportionately higher rates than the rest of the population (
Alegría et al. 2013;
Williams et al. 2014). The lifetime prevalence of PTSD in African Americans was measured as 8.7 percent. Non-Hispanic European Americans, Hispanics, and Asians experience a lifetime prevalence of PTSD at 7.4 percent, 7.1 percent, and 4.0 percent, respectively (
Roberts et al. 2011). Though the number of traumatic events documented by African Americans is lower than those of other races and ethnicities, the degree of the traumatic events is often more severe and violent. Common occurrences include assaultive violence, such as domestic violence, rape, homicide, physical attacks, and kidnappings, as well as exposure to child abuse. On the contrary, European Americans are more likely to report a traumatic experience such as learning of the unexpected death of a loved one (
Asnaani and Hall-Clark 2017; Pérez
Benítez et al. 2014). Moreover, racism, discrimination, and stigmatization that frequently occur in addition to other traumatic events may result in a composite reaction to the trauma, influencing the symptom severity. Studies have reported that increased perceived discrimination makes one more apt to a PTSD diagnosis or greater severity of PTSD. Furthermore, increased rates of hypervigilance and emotions such as guilt, shame, and low self-worth, which are also associated with PTSD, have been evident based on racial discrimination (
Alegría et al. 2013;
Asnaani and Hall-Clark 2017;
Williams et al. 2014).
4. Barriers and Mistrust toward Healthcare
Research has continually identified a gap in the diagnosis and treatment of PTSD among African Americans. A large degree of racial discrepancies in PTSD prevalence and the rate of seeking treatment for PTSD are the result of the hesitation among many minority groups to utilize professional psychological services. African Americans are one-third to one-half as likely to consult a mental health provider, almost twice as likely to prematurely discontinue therapy, and three times more likely not to begin therapy in comparison with European Americans (
Fiscella et al. 2002;
Spoont et al. 2015;
Williams et al. 2014). Research findings have indicated that African Americans with mental illnesses make healthcare appointments later in the progression of their illnesses and arrive more disabled than European Americans (
Williams and Earl 2007). African Americans experience lower rates of recovery from PTSD. Several factors contribute to this disparity, including less access to financial resources for mental health care as well as over-representation in lower socioeconomic and underprivileged communities (
Hays 2015; Pérez
Benítez et al. 2014). However, even after adjusting for predisposing factors such as insurance availability, Black patients are significantly less likely to have had an appointment with a mental health provider (
Fiscella et al. 2002).
Though African Americans account for thirteen percent of the population, they only comprise four percent of psychologists (
Lin et al. 2018). They endorse greater levels of mental health stigma, more negative attitudes regarding mental health treatment, and increased fears of being discriminated against by mental health providers. Furthermore, the racial incompetency of some therapists serves as a barrier to treatment for many. They may also feel differently towards Caucasian clinicians due to cultural mistrust (
Williams 2008;
Williams et al. 2014). Mental health professionals often do not understand the impact of racism on psychopathology because of a societal tendency to deny or rationalize the presence of racism (
Williams et al. 2014).
Past and recent experiences of discrimination in healthcare settings have led African American patients to demonstrate lower trust in the healthcare system than European Americans. Experiences of discrimination largely account for the existence of this mistrust. Even after studies have adjusted for healthcare disparities, there is still a large degree of association between the African American race and distrust in the healthcare system (
Armstrong et al. 2013;
Cuevas and O’Brien 2019). In many cases, greater perceived racism and greater mistrust in the healthcare system leads to poorer health outcomes for African Americans. Mistrust of physicians has been seen to influence African American patients in such a way that they are less forthcoming with doctors about health information, more submissive to doctors, and less likely to follow treatment protocol. Overall, mistrust of the healthcare system results in decreased patient satisfaction with care and the utilization of services (
Hammond et al. 2010a,
2010b;
Peek et al. 2010).
Cuevas et al. (
2016) conducted a qualitative study recording the first-hand healthcare experiences of African Americans. Participants described experiencing discrimination from both the office staff and doctors. For example, African American women stated that they had to continually declare their interests to obtain reasonable treatment. They also spoke of incidents in which White doctors did not try to take the time to listen to their concerns or ensure they comprehended their treatment (
Cuevas et al. 2016). This sentiment is corroborated by a study that found that patients that were the same race as their physicians had visits that were an average of ten percent longer than those of differing races (
Cooper et al. 2003). Moreover, African American men relayed experiences in which mistrust was connected to perceived discrimination and poor communication. Overall, the results of this study suggested that the healthcare system is structured in such a way that African Americans feel depersonalized and objectified. Healthcare visits feel rushed and disrespectful and lack advocacy from the doctor. Thus, a cycle of mistrust is created in which African American patients do not trust their doctors and believe that their doctors do not trust them (
Cuevas et al. 2016).
African American patients may also have developed a mistrust of healthcare institutions in response to physician bias and discrimination as well as cultural discordance, which in turn impact the physician’s behaviors. For example, physicians may be less likely to share medical information and more likely to be authoritarian toward African American patients. A lack of cultural competence among physicians is often displayed both verbally and nonverbally (
Kennedy et al. 2007;
Peek et al. 2010). In a study of race-concordant and race-discordant medical encounters, healthcare visits in which the doctor and patient were of the same race received higher coder ratings of positive affect-reflections of voice tone qualities, which is suggestive of the emotional framework of the appointment. These visits were further depicted as having greater scores of patient satisfaction and positive judgments of physicians’ use of shared decision making. Patients and physicians that are members of the same race or ethnic groups are more likely to have similar beliefs, values, and experiences in society, which results in increased security with each other (
Cooper et al. 2003;
Kennedy et al. 2007).
It is vital not to interpret findings regarding mistrust of the healthcare system as a problematic characteristic of a patient. Often, factors that relate to mistrust, such as identification with one’s racial group, can be imperative to one’s mental health and well-being. Medical mistrust is not simply an attitudinal obstacle. Instead, it is a barrier that is prompted by proximal, first-hand experiences (
Cuevas and O’Brien 2019;
Powell et al. 2019). Mistrust can very well be a reasonable and adaptive reaction to historic and ongoing discriminatory experiences. Though there are negative health outcomes linked to mistrust of healthcare systems, it can also safeguard a person by circumventing some race-based stressors (
Cuevas and O’Brien 2019).
5. The African American Church
Most African Americans are either past or current churchgoers, with approximately 85 percent identifying as fairly or very religious and 80 percent praying daily (
Taylor et al. 2004). A sizable margin of 70 to 80 percent of African Americans denoted on one national survey that religion is an important component of their lives. Out of all racial and ethnic groups in the United States, African Americans have the highest documented rate of church attendance (
Adofoli and Ullman 2014;
Taylor et al. 2004;
Williams 2008;
Williams et al. 2014). The Black church in the U.S. has always served as a spiritual, psychological, and social bulwark against anti-Black racism and a prophetic witness to the humanity of Black personhood. The Black church has been a refuge throughout slavery to Freedom, reconstruction, Jim Crow, civil rights, and the discrimination of the current times (
Streets 2015;
Williams 2008). During slavery, the church, by law, was the sole forum where African Americans could assemble in groups and have a sense of freedom. The teachings, songs, and social support found in the church brought hope and confirmed humanity. It has been a voice advocating for social change and equality. The Black church has also set an example of the way that living a life of faith, values, and ethics can assist in handling injustice and adversity (
Plunkett 2014;
Williams 2008). Moreover, the Black church has continuously afforded tangible support services to people in their community by offering food, shelter, financial assistance, and direction (
Streets 2015;
Wingfield 1988).
African Americans often use faith-based resources for their mental health care over other clinical resources (
Adofoli and Ullman 2014;
Hankerson and Weissman 2012;
Hays 2015). Some have called the Black church “a spiritual hospital”. The Black church has undertaken the position of a therapist to tackle numerous emotional, psychiatric, and psychological mental health issues among its congregants. Seeking support and healing from the church is often more appealing than working with a mental health professional. Whereas the language of psychology may be foreign, the spiritual language of healing and transformation found in the church has deep cultural resonance (
Plunkett 2014;
Williams 2008). Faith-based programs offered through churches to promote mental and physical healthcare are culturally fitted to highlight Black culture and spirituality (
Hankerson and Weissman 2012). Furthermore, the pastor of the church is someone that the congregants already trust, contrasting with a therapist with whom one must build up a relationship and trust. They are also familiar with the life circumstances and resources of the congregants and are thus better able to anticipate and respond to secondary issues. Moreover, both therapy and the church meet weekly; however, church is free (
Payne and Hays 2016;
Williams 2008). At large, many African American congregants see formal counseling as unwarranted because they often set their hope for healing in the promises of the Bible and prayer. Professional counseling is thus sometimes seen as a lack of faith (
Plunkett 2014). Further,
Payne (
2009) found that African American pastors were more likely to concur that the etiology of depression was a lack of trust in God rather than a biological disorder. African American religious services have continued to operate as imperative social events, tending to shield individuals from feelings of estrangement and helplessness. Attendance at religious services has been negatively correlated with psychological distress in this community (
Jarvis et al. 2005). Generally, the literature has shown that resources from the church are largely effective in symptom reduction; however, more research is needed in this area (
Hankerson and Weissman 2012).
Two of the highest contributors to the disposition toward seeking mental health care among African American congregants are the beliefs of the religious leader and church doctrine. Clinicians are often unable to sufficiently address the cultural differences at play such as their religious and spiritual beliefs and the ideologies that impact mental health treatment (
Hays 2015). African Americans who seek professional therapeutic help eventually turn to a pastor also. However, those who seek the pastor first turn to few additional resources afterward (
Neighbors et al. 1998).
The number and types of crises and disruptions that antagonize the congregants of African American churches result in pastors accepting various leadership roles for which they are not always equipped. The expectation to be there for the congregants, serve as an outstanding pastor, and always display integrity leads to added stress on pastors (
Streets 2015).
Some have raised the concern that church-based mental health care, provided by non-professionals, could be harmful to the congregants. A sizeable number of clergy are unqualified to handle mental health crises. Many pastors report feeling inadequate to deliver such care. Moreover, some hold beliefs that discourage seeking help from mental health professionals. Further education and training are needed for religious leaders in mental health services (
Asamoah et al. 2014;
Hall and Gjesfjeld 2013).
The African American church’s role in guidance, support, and communication places it in a unique and pivotal position for healthcare promotion efforts. The unique situation of the church as well as its concern for the well-being of its congregants can lead to partnerships that may reduce health disparities (
Goldmon and Roberson 2004). Prior research has indicated that faith-based interventions have been impactful for smoking cessation, reductions in cardiovascular disease, and increasing the consumption of healthy foods among African Americans (
Whitt-Glover et al. 2008). Moreover, a general readiness to change has been observed following these church-based interventions (
DeHaven et al. 2004). Of note, barriers remain in the implementation of church-based health programs within the African American church. For example, historically, due to the separation of church and state, religious organizations were limited in acquiring the required funding to facilitate such programming (
Lasater et al. 1997).
11. Discussion
The present study aimed to explore the prevalence of and relationships among ACEs, BCEs, negative religious coping and church interactions, attitudes toward the medical system, and various negative mental health outcomes in African American religious leaders and church congregants. Given the likelihood of African American church congregants to seek out support from their religious leaders as well as the probability that these church leaders have experienced their own trauma, a variety of negative mental health symptoms have been documented among both African American religious leaders and their church congregants. The literature has documented the prevalence of STS in religious leaders (
Hendron et al. 2011). Furthermore,
Baum (
2014) found that when professionals faced double exposure to the shared traumatic reality of the times, their mental health presentation consisted of a combination of primary traumatization, secondary traumatization, and general symptomology of distress. Research also suggests that African Americans exhibit depression with increased severity and persistence and PTSD at a higher rate than those of different races (Pérez
Benítez et al. 2014;
Roberts et al. 2011). Based on the findings of the literature, the current study expected that moderate to high levels of ACEs, STS, PTSD, depression, and anxiety would be present among African American leaders and their church congregants.
Descriptive statistics revealed that 80% of the sample experienced at least one type of adverse childhood experience, and 30.9% experienced three or more, compared to 61.5% and 24.6%, respectively, of a national sample (CDC). With a mean ACEs score of 2.27, the participants of this study averaged higher ACEs than a nationally representative sample of Black persons in the U.S. (1.69) (
Merrick et al. 2018, p. 1042). The most common ACEs included the divorce or separation of parents, living with someone who was a problematic drinker or alcoholic or used street drugs, and having a household member who was depressed or mentally ill or attempted suicide.
Moreover, over half of the African American religious leaders endorsed experiencing moderate to severe levels of STS. The study further discovered that 28% of the African American pastors and congregants endorsed moderate to severe anxiety symptoms, 12% endorsed moderate to severe depressive symptoms, and 26.5% endorsed experiencing at least one symptom of PTSD on a checklist of five symptoms. Bivariate correlations specifically indicated that ACEs are positively correlated with anxiety symptoms among this population. Moreover, STS was positively correlated with anxiety, depression, and PTSD in the initial sample of religious leaders, which indicated that participants were experiencing distress related to being both a shepherd of a congregation as well as someone with his or her own challenging life experiences. The relationship of STS in the religious leaders with these negative mental health outcomes further suggests that the symptoms of depression and anxiety within this population could be trauma-based, whether it be based on personal traumatic experiences or secondary trauma. As previously mentioned, there is a lack of research on clergy and STS, but the findings of this study corroborate qualitative studies that show more attention needs to be given to the experience of clergy with STS (
Francis et al. 2004;
Hendron et al. 2011).
The literature has documented African American clergy members as key personnel for their congregants in times of crisis. Specifically, Black women shared in a semi-structured interview that clergy and other members of the church helped them deal with a crisis (
Davis and Johnson 2020;
St. Vil et al. 2016). Likewise, the results of the present study indicated that interaction with those who have experienced trauma and are currently experiencing negative mental health symptomology is a significant aspect of the African American church experience. Trauma exposure, ACEs, depression, anxiety, STS, and PTSD have associations with loss of faith in organized religion, interpersonal conflict, substance abuse, health issues, suicidal ideation, and overall general distress (
Williams and Mohammed 2009;
Hendron et al. 2011;
McCormick et al. 2017). Thus, ACEs, depression, anxiety, STS, and PTSD are all prevalent within the African American church and should not be ignored.
Despite the troubling prevalence of ACEs and STS, it is important to recognize the large number of BCEs reported as well. Most of the participants (92.2%) endorsed eight or more BCEs. The most reported BCEs included having beliefs that provided comfort, opportunities to have a good time, good neighbors, at least one caregiver who provided a sense of safety, and at least one good friend. Conversely, the most commonly unendorsed BCEs included liking or feeling comfortable with oneself, having an adult other than a parent/caregiver to provide advice and support, and liking school.
It is noteworthy that despite having higher ACEs scores than average and relatively high STS scores, the average participant did not meet the cutoff scores for anxiety and depression. The mean score on the GAD-7 for anxiety was 5.72, which places this group of participants at the low end of mild anxiety, and the average depression score on the PHQ-9 was 3.81, which is at the high end of minimal depression. As shown in a growing number of studies, the abnormally high rates of BCEs for this group may have served as a protective factor against at least two of the most common mental health diagnoses (
Bethell et al. 2019;
Narayan et al. 2021). Most BCEs are relational in nature and can be found within growth-fostering communities. The church is potentially one such community as it often provides children with experiences of having at least one good friend, obtaining beliefs that provide comfort, an adult who is not in the home who can provide support or advice, and opportunities to have a good time. These are all factors found to be benevolent childhood experiences.
Throughout history, the African American church has undertaken roles that mirror BCEs. It has provided a place of refuge, social support, advocacy, validation, and tangible resources such as food, shelter, financial assistance, and further direction. Given the protective nature of BCEs documented throughout the literature (
Crandall et al. 2019;
Doom et al. 2021;
Narayan et al. 2021), it is encouraging to discover the high prevalence of BCEs documented throughout this sample. Moreover, the church can continue to foster a community that provides advice, support, and direction for its congregants across all age groups to continue this trend.
Many unique stressors accompany leading a church. The literature has documented the emotional and mental challenges faced by clergy who experienced high demands from their church congregations (
Doolittle 2010;
Jacobson et al. 2013;
Roberts et al. 2011). The current study discovered that the unfair expectations that the African American religious leaders felt their congregants put on them predicted STS symptoms. Specifically, religious leaders who felt that the people in the congregation made too many demands on them and/or were critical of them and the things they did reported increased STS. Vocational STS has been associated with departing from the ministry, emotional exhaustion, and relational difficulties (
Spencer et al. 2012;
Hendron et al. 2011). Thus, the demands and criticisms communicated to religious leaders may threaten not only their well-being but their longevity in the ministry as well.
Throughout the literature, spirituality has been thought of as beneficial to one’s overall health and well-being, often focusing on the protective aspects of religious coping and connection to God. However, research has also discovered a relationship between negative religious coping and higher levels of distress (
Park et al. 2018). In a study of African Americans who had experienced trauma, religious coping did not reduce PTSD and depressive symptoms, leading researchers to hypothesize potential harmful uses of religious coping (
Bryant-Davis et al. 2011). The researchers proposed that the participants may have been utilizing negative religious coping (
Bryant-Davis et al. 2011). While positive religious coping emphasizes the benevolence of God, negative religious coping focuses primarily on a condemning God (
Pargament et al. 2011). In the current study, negative religious coping in times of challenges was characterized by feeling punished by God, a sense of abandonment from God and the church, blaming hardship on the devil, and questioning the power and love of God.
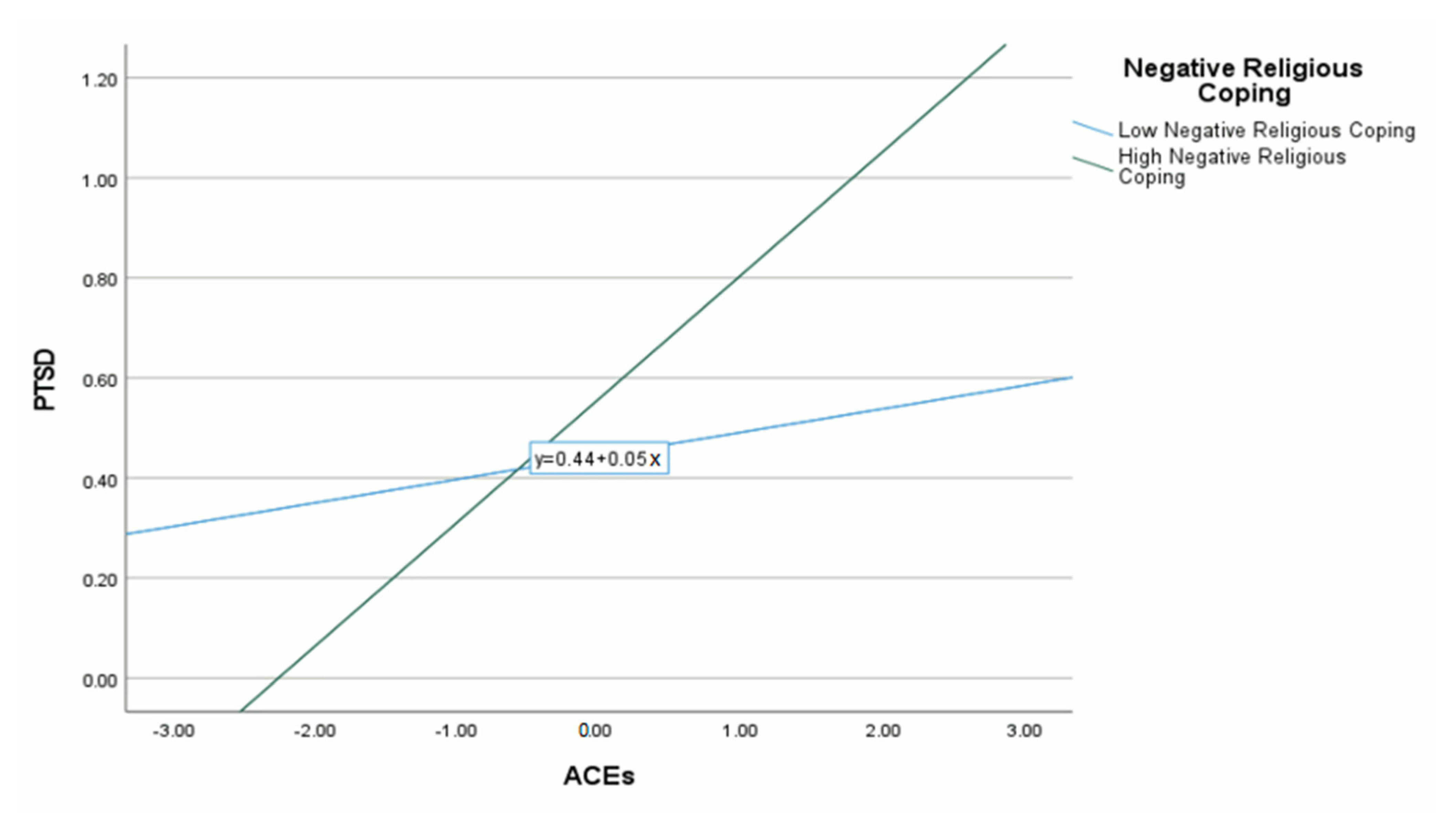
The present study discovered that negative religious coping moderated the relationship between ACEs and PTSD (
Bryant-Davis et al. 2011;
Bryant-Davis et al. 2015). African American church leaders and congregants who reported using negative religious coping in times of hardship were at greater risk of PTSD following ACEs, which provides further support for the findings of
Bryant-Davis et al. (
2011). Previous research has suggested, and the current study substantiates, that individuals might consider re-evaluating their understanding of God following challenging life events because their implicit and/or explicit view of God may exacerbate vulnerabilities to mental illness. Notably, the significant moderation effect applied to individuals demonstrating high levels of negative religious coping; for those demonstrating low and average levels of negative religious coping, such coping did not moderate the relationship between ACEs and PTSD. Therefore, negative religious coping is only a risk factor that exacerbates the relationship between ACEs and PTSD for those who frequently engage in it.
These findings suggest that religion does not inherently lead to positive mental health outcomes. The way one approaches their religiosity and spirituality, particularly when responding to stressful life events, is an important consideration, as not all forms of religious coping are beneficial. Traumatic events can leave individuals struggling to make meaning of their situation and the world. Religion is often a context that people lean upon to make sense, find meaning, and recover from challenging circumstances throughout their lifespan (
Bryant-Davis et al. 2011;
De Luna and Wang 2021). Though it does not appear to be harmful for individuals to question God’s benevolence every so often, frequent feelings of abandonment and punishment from God and the church, as well as other forms of negative religious coping, appear to result in poorer outcomes. More specifically, in response to dealing with a critical life event, participants in the current study most often reported wondering whether God had abandoned them, feeling punished by God for their lack of devotion, deciding the devil made it happen, and wondering what they did for God to punish them. African American church leaders may keep in mind that their congregations may benefit from support in coping and making sense of stressful life events, particularly with those who have been exposed to trauma.
Given the history of racism and barriers to healthcare, mistrust of the medical system and hesitancy to seek mental health support is often present among African Americans. Research indicates that African Americans experience lower rates of recovery from PTSD, resulting from several disparities. However, even after controlling for several predisposing factors, research has indicated that African American patients are less likely to have had an appointment with a mental health provider (
Fiscella et al. 2002;
Hays 2015). Moreover, a longitudinal study of African Americans with anxiety revealed that those with PTSD were less likely to seek treatment (Pérez
Benítez et al. 2014). Finally, research has suggested that African Americans experience increased feelings of mental health stigma, negative attitudes toward mental health treatment, and fears of discrimination in a mental health setting (
Williams 2008;
Williams et al. 2014). The reasonable and adaptive reactions of many African Americans to healthcare lead to greater dependence on the Black church for mental health support (
Adofoli and Ullman 2014;
Hankerson and Weissman 2012;
Hays 2015).
Though previous research has postulated medical mistrust, mental health stigma, limited interactions with mental health providers, and increased mental health symptomology among African Americans, the specific relationship among these variables has not yet been determined (
Fiscella et al. 2002;
Hays 2015; Pérez
Benítez et al. 2014). Based on the results of this study, it appears that the mental health of African American churchgoers with varying numbers of ACEs is impacted by medical mistrust. Though low and average amounts of distrust of healthcare organizations have an insignificant impact on PTSD, high levels of medical mistrust are a risk factor moderating the relationship between ACEs and PTSD. It may be beneficial for future research to further explore the relationship between medical mistrust and mental health symptoms to understand the specific avenues for this finding. However, it can be postulated that those with high levels of medical mistrust may be underutilizing health care services and, therefore, not getting the mental and physical care needed.
The moderating relationships of both negative religious coping and medical mistrust on the relationship between ACEs and PTSD have important implications for the health and well-being of African American leaders and churchgoers. The findings of the current study offer two empirically supported interventions that can be used in reducing PTSD symptoms in this population. Mental health clinicians and church leaders can focus efforts on diminishing negative religious coping and medical mistrust in African American Christians. In efforts to promote culturally competent treatment when working with African Americans, therapists can employ interventions that aim to reduce negative religious coping. Specifically, therapists can integrate spiritual and religious issues related to clients’ feeling punished by God and abandoned by God and the church as well as blaming hardship on the devil and questioning the power and love of God. Additionally, both clinicians and trusted church personnel can provide psychoeducation designed to correct misconceptions regarding the medical system. Churches may consider partnering with healthcare institutions to build relationships and overcome some of the barriers. However, the results ultimately shed light on the imperativeness of cultivating a medical system that warrants the trust of African Americans.
Limitations and Directions for Future Research
There are several limitations to the present study. First, the data were collected from a sample of African American churches in the state of Texas, and most of the sample (69.7%) identified as female. Therefore, the findings may be impacted by the cultural context of the specific region and gender, affecting the universality of the results. Furthermore, the study may have been impacted by self-selection and self-report biases. It is possible that only those interested in the topic chose to participate. Potential respondents with higher levels of symptomatology may not have wanted to participate due to the nature of the survey questions or current life stressors. Moreover, this study solely used self-report measures, which are subject to various aspects of bias by the respondents. Though the measures utilized in this study have good reliability and validity, most of the surveys were shortened to a few items or subscales to reduce the time commitment for the participants. Finally, the symptom severity of respondents was very diverse, which initially resulted in skewed data. Therefore, outliers had to be deleted for high depression and PTSD scores as well as low BCEs scores.
As this study confirmed the prevalence of STS, anxiety, depression, and PTSD among African American religious leaders and church congregants, future research should continue to explore the best avenues of support for this population. Possible constructs to be explored in relation to trauma and mental health in the African American church include positive religious coping, spiritual experiences, experiences of discrimination, and education surrounding trauma and mental health. Trauma exposure may also be expanded in future research to include experiences after the age of 18 as well. Future research might also investigate the variables that make one more at risk for high levels of negative religious coping and medical mistrust. Additionally, future research can also explore variables (especially those that are religiously oriented) that may contribute to post-traumatic growth, such as self-compassion (
Yuhan et al. 2021) and different forms of prayer (
Lowe et al. 2022).

 ,
, 


{kind=link}
{kind=link}