Severe Acute Kidney Injury in Cardiovascular Surgery: Thrombotic Microangiopathy as a Differential Diagnosis to Ischemia Reperfusion Injury. A Retrospective Study


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
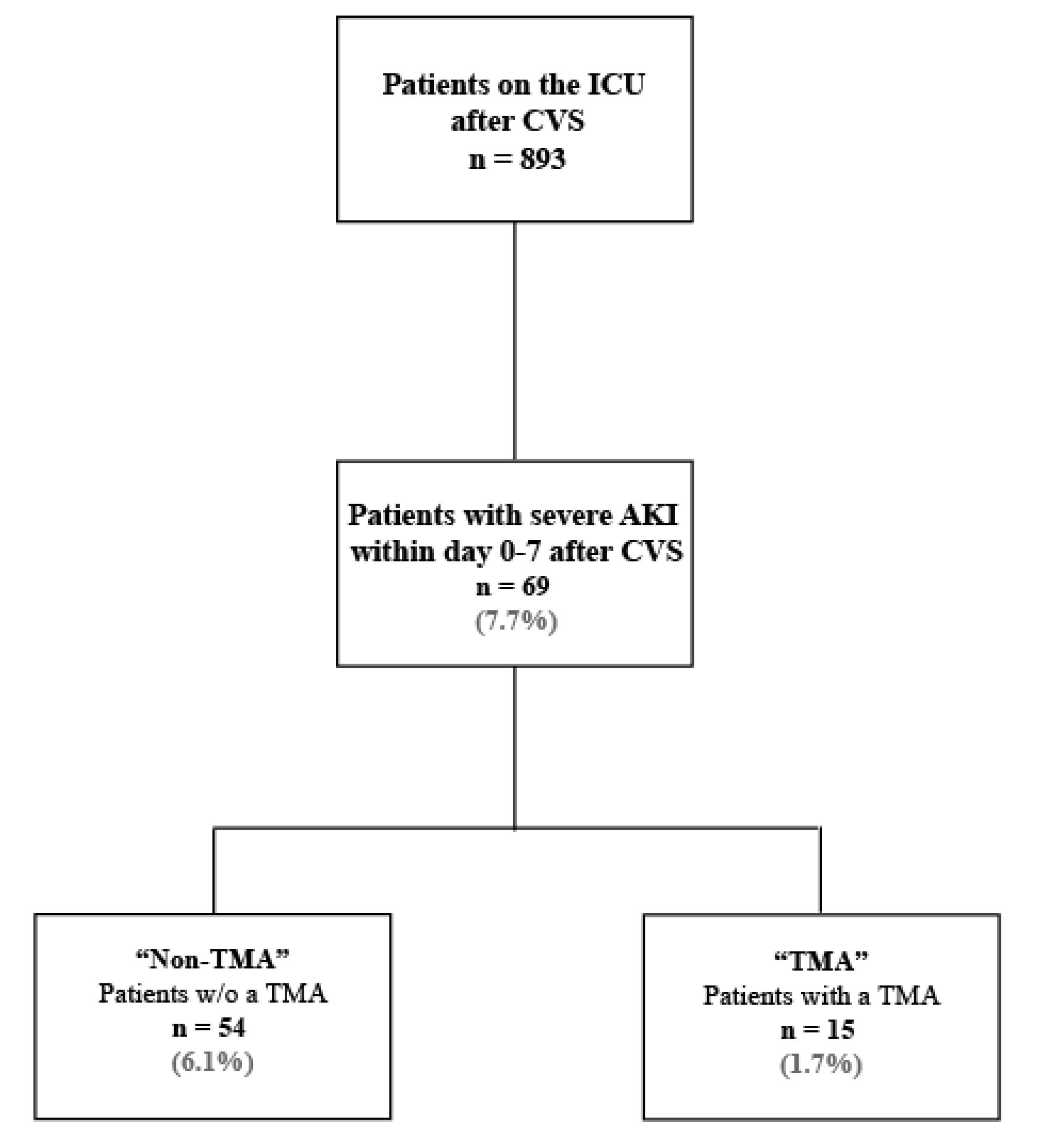
2.1. Subjects
2.2. Kidney Function and Laboratory Parameters
2.3. Data Analysis and Endpoints
3. Results
3.1. Baseline Characteristics
3.2. Baseline Kidney Function
3.3. Surgery Characteristics
3.4. Postsurgical Outcomes
3.4.1. Thrombotic Microangiopathy
3.4.2. TMA Treatment
3.4.3. Renal Outcome and Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ADAMTS13 | A Disintegrin And Metalloprotease with a ThromboSpondin type 1 motif, member 13 |
| aHUS | Atypical hemolytic uremic syndrome |
| AKI | Acute kidney injury |
| CAD | Coronary artery disease |
| CPB | Cardiopulmonary bypass |
| CFH | Complement factor H |
| CSA-AKI | Cardiovascular surgery-associated acute kidney injury |
| CVS | Cardiovascular surgery |
| ECMO | Extracorporeal membrane oxygenation |
| eGFR | Estimated glomerular filtration rate |
| ESKD | End-stage kidney disease |
| HCA | Hypothermic circulatory arrest |
| IQR | Interquartile range |
| INR | International normalized ratio |
| IRI | Ischemia reperfusion injury |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| LDH | Lactate dehydrogenase |
| MAHA | Microangiopathic hemolytic anemia |
| SACP | Selective antegrade cerebral perfusion |
| STEC-HUS | Shiga toxin-producing Escherichia coli-associated HUS |
| RRT | Renal replacement therapy |
| TMA | Thrombotic microangiopathies |
| TTP | Thrombotic thrombocytopenic purpura |
References
- Wang, A.Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef]
- Lassnigg, A.; Schmidlin, D.; Mouhieddine, M.; Bachmann, L.M.; Druml, W.; Bauer, P.; Hiesmayr, M. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: A prospective cohort study. J. Am. Soc. Nephrol. 2004, 15, 1597–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobson, C.E.; Yavas, S.; Segal, M.S.; Schold, J.D.; Tribble, C.G.; Layon, A.J.; Bihorac, A. Acute Kidney Injury Is Associated With Increased Long-Term Mortality After Cardiothoracic Surgery. Circulation 2009, 119, 2444–2453. [Google Scholar] [CrossRef] [Green Version]
- Bellomo, R.; Auriemma, S.; Fabbri, A.; D’Onofrio, A.; Katz, N.; McCullough, P.; Ricci, Z.; Shaw, A.D.S.; Ronco, C. The pathophysiology of cardiac surgery-associated acute kidney injury (CSA-AKI). Int. J. Artif. Organs 2008, 31, 166–178. [Google Scholar] [CrossRef]
- George, J.N.; Nester, C.M. Syndromes of Thrombotic Microangiopathy. N. Engl. J. Med. 2014, 371, 654–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schönermarck, U.; Ries, W.; Schröppel, B.; Pape, L.; Dunaj-Kazmierowska, M.; Burst, V.; Mitzner, S.; Basara, N.; Starck, M.; Schmidbauer, D.; et al. Relative incidence of thrombotic thrombocytopenic purpura and haemolytic uraemic syndrome in clinically suspected cases of thrombotic microangiopathy. Clin. Kidney J. 2019, 13, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Goodship, T.H.; Cook, H.T.; Fakhouri, F.; Fervenza, F.; Frémeaux-Bacchi, V.; Kavanagh, D.; Nester, C.M.; Noris, M.; Pickering, M.C.; De Cordoba, S.R.; et al. Atypical hemolytic uremic syndrome and C3 glomerulopathy: Conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2017, 91, 539–551. [Google Scholar] [CrossRef] [Green Version]
- Noris, M.; Caprioli, J.; Bresin, E.; Mossali, C.; Pianetti, G.; Gamba, S.; Daina, E.; Fenili, C.; Castelletti, F.; Sorosina, A.; et al. Relative Role of Genetic Complement Abnormalities in Sporadic and Familial aHUS and Their Impact on Clinical Phenotype. Clin. J. Am. Soc. Nephrol. 2010, 5, 1844–1859. [Google Scholar] [CrossRef]
- Sridharan, M.; Hook, C.C.; Leung, N.; Winters, J.L.; Go, R.S.; Mayo Clinic Complement Alternative Pathway-Thrombotic Microangiopathy Disease-Oriented Group. Postsurgical thrombotic microangiopathy: Case series and review of the literature. Eur. J. Haematol. 2019, 103, 307–318. [Google Scholar] [CrossRef]
- Markakis, K.; Westhoff, T.H.; Pagonas, N. Aortic Valve Replacement as a Trigger of Atypical Hemolytic Uremic Syndrome. Ann. Thorac. Surg. 2017, 104, e255–e256. [Google Scholar] [CrossRef] [Green Version]
- Ikushima, E.; Hisahara, M.; Nishijima, T.; Uchiyama, H.; Onzuka, T.; Ochiai, Y.; Muta, T.; Tokunaga, S. Atypical Hemolytic Uremic Syndrome following Acute Type A Aortic Dissection. Case Rep. Hematol. 2020, 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Matsukuma, E.; Imamura, A.; Iwata, Y.; Takeuchi, T.; Yoshida, Y.; Fujimura, Y.; Fan, X.; Miyata, T.; Kuwahara, T. Postoperative Atypical Hemolytic Uremic Syndrome Associated with Complement C3 Mutation. Case Rep. Nephrol. 2014, 2014, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Yamamoto, M.; Fukuda, T.; Ohtsuka, Y.; Miura, O. Postoperative Atypical Hemolytic Uremic Syndrome Treated Successfully with Eculizumab. Intern. Med. 2016, 55, 1171–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellum, J.A.; Lameire, N. KDIGO AKI Guideline Work Group Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [Green Version]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron 2012, 120, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Chen, Y.-C. Acute kidney injury classification: AKIN and RIFLE criteria in critical patients. World J. Crit. Care Med. 2012, 1, 40–45. [Google Scholar] [CrossRef]
- Villa, G.; Katz, N.; Ronco, C. Extracorporeal Membrane Oxygenation and the Kidney. Cardiorenal Med. 2015, 6, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Roh, G.U.; Lee, J.W.; Nam, S.B.; Lee, J.; Choi, J.-R.; Shim, Y.H. Incidence and Risk Factors of Acute Kidney Injury After Thoracic Aortic Surgery for Acute Dissection. Ann. Thorac. Surg. 2012, 94, 766–771. [Google Scholar] [CrossRef]
- Englberger, L.; Suri, R.M.; Greason, K.L.; Burkhart, H.M.; Sundt, T.M.; Daly, R.C.; Schaff, H.V. Deep hypothermic circulatory arrest is not a risk factor for acute kidney injury in thoracic aortic surgery. J. Thorac. Cardiovasc. Surg. 2011, 141, 552–558. [Google Scholar] [CrossRef] [Green Version]
- Saltzman, D.J.; Chang, J.C.; Jiménez, J.C.; Carson, J.G.; Abolhoda, A.; Newman, R.S.; Milliken, J.C. Postoperative Thrombotic Thrombocytopenic Purpura After Open Heart Operations. Ann. Thorac. Surg. 2010, 89, 119–123. [Google Scholar] [CrossRef]
- Kavanagh, D.; Goodship, T.H.; Richards, A. Atypical Hemolytic Uremic Syndrome. Semin. Nephrol. 2013, 33, 508–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruins, P.; Velthuis, H.T.; Yazdanbakhsh, A.P.; Jansen, P.G.M.; Van Hardevelt, F.W.J.; De Beaumont, E.M.F.H.; Wildevuur, C.R.H.; Eijsman, L.; Trouwborst, A.; Hack, C.E. Activation of the Complement System During and After Cardiopulmonary Bypass Surgery. Circulation 1997, 96, 3542–3548. [Google Scholar] [CrossRef] [PubMed]
- Campistol, J.M.; Arias, M.; Ariceta, G.; Blasco, M.; Espinosa, L.; Espinosa, M.; Grinyó, J.M.; Macia, M.; Mendizábal, S.; Praga, M.; et al. An update for atypical haemolytic uraemic syndrome: Diagnosis and treatment. A consensus document. Nefrología (Engl. Ed.) 2015, 35, 421–447. [Google Scholar] [CrossRef]
- Legendre, C.; Licht, C.; Muus, P.; Greenbaum, L.; Babu, S.; Bedrosian, C.; Bingham, C.; Cohen, D.; Delmas, Y.; Douglas, K.; et al. Terminal Complement Inhibitor Eculizumab in Atypical Hemolytic–Uremic Syndrome. N. Engl. J. Med. 2013, 368, 2169–2181. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| TMA (n = 15) | Non-TMA (n = 54) | p-Value | |||
|---|---|---|---|---|---|
| Baseline characteristics | Median (IQR) | Median (IQR) | |||
| Female (n, %) | 9 | (60) | 18 | (33.3) | 0.063 |
| Age (years) | 66 | (45–72) | 70 | (62–76) | 0.112 |
| Body-mass index (kg/m2) | 23.2 | (20.8–30.4) | 25.8 | (22.4–28.9) | 0.531 |
| Height (m) | 1.68 | (1.63–1.75) | 1.75 | (1.65–1.85) | 0.098 |
| Weight (kg) | 76 | (63–85) | 78 | (69–94) | 0.284 |
| Diagnosis on admission | n (%) | n (%) | p-value | ||
| Aortic valve disease | |||||
| Aortic stenosis | 1 | (6.7) | 10 | (18.5) | 0.434 |
| Aortic insufficiency | 8 | (53.3) | 19 | (35.2) | 0.240 |
| Aortic endocarditis | 2 | (13.3) | 6 | (11.1) | 1.000 |
| Mitral valve disease | |||||
| Mitral stenosis | 0 | (0.0) | 5 | (9.3) | 0.578 |
| Mitral insufficiency | 5 | (33.3) | 23 | (42.6) | 0.568 |
| Mitral endocarditis | 0 | (0.0) | 5 | (9.3) | 0.578 |
| Tricuspid valve disease | |||||
| Tricuspid insufficiency | 3 | (20.0) | 14 | (25.9) | 0.746 |
| Tricuspid stenosis | 0 | (0.0) | 0 | (0.0) | NA |
| Aortic disease | |||||
| Aortic aneurysm | 7 | (46.7) | 8 | (14.8) | 0.014 |
| Aortic dissection Type A | 1 | (6.7) | 9 | (16.7) | 0.442 |
| Coronary artery disease (CAD) | 7 | (46.7) | 34 | (57.4) | 0.561 |
| Reduced LVEF | 4 | (26.7) | 27 | (42.6) | 0.373 |
| End stage heart failure | 0 | (0.0) | 11 | (16.7) | 0.189 |
| Previous heart surgery | 7 | (46.7) | 19 | (33.3) | 0.375 |
| TMA (n = 15) | Non-TMA (n = 54) | p-Value | |||
| Cardiovascular history & risk factors | n (%) | n (%) | |||
| Diabetes mellitus (Type 1 or 2) | 2 | (13.3) | 12 | (22.2) | 0.718 |
| Arterial hypertension | 10 | (66.7) | 38 | (70.4) | 0.761 |
| Hypercholesterinemia | 10 | (66.7) | 27 | (50.0) | 0.381 |
| Family history for CAD | 6 | (40.0) | 6 | (14.8) | 0.063 |
| Obesity | 4 | (26.7) | 17 | (31.5) | 1.000 |
| History of smoking | 6 | (40.0) | 23 | (42.6) | 1.000 |
| Macroangiopathy (cerebral or peripheral) | 10 | (66.7) | 28 | (51.9) | 0.386 |
| Renal history | n (%) | n (%) | p-value | ||
| Chronic kidney disease (eGFR≤ 60ml/min) | 3 | (20.0) | 26 | (48.2) | 0.076 |
| Other pathologies | n (%) | n (%) | p-value | ||
| Autoimmune disease | 3 | (20.0) | 3 | (5.7) | 0.112 |
| History of malignancy | 1 | (6.7) | 9 | (16.7) | 0.442 |
| Medication | n (%) | n (%) | p-value | ||
| ACE-Inhibitors/AT1-Blockers | 8 | (53.3) | 31 | (57.4) | 0.778 |
| Beta blockers | 9 | (60.0) | 38 | (70.3) | 0.535 |
| Statins | 8 | (53.3) | 24 | (44.4) | 0.572 |
| Aspirin/Clopidogrel | 7 | (46.7) | 24 | (44.4) | 1.000 |
| Ticlopidine | 0 | (0.0) | 1 | (1.9) | 1.000 |
| OAC (Marcumar/NOACs) | 6 | (40.0) | 25 | (46.3) | 0.773 |
| Immunosuppression | 2 | (13.3) | 2 | (3.7) | 0.204 |
| TMA (n = 15) | Non-TMA (n = 54) | p-Value | |||
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | ||||
| Bilirubin (mg/dL) | 0.7 | (0.4–0.9) | 0.9 | (0.6–1.4) | 0.075 |
| LDH (U/L) | 314 | (202–388) | 326 | (226–445) | 0.755 |
| Hemoglobin (g/dL) | 12.3 | (11.2–14.1) | 12.7 | (10.4–13.9) | 0.788 |
| Thrombocytes (G/L) | 189 | (152–250) | 202 | (147–251) | 0.884 |
| INR | 1.1 | (1.0–1.2) | 1.1 | (1.0–1.4) | 0.142 |
| Kidney function parameters | |||||
| Creatinine (mg/dL) | 0.9 | (0.8–1.3) | 1.3 | (1.0–1.7) | 0.005 |
| eGFR (mL/min) | 92 | (57–100) | 60.5 | (44–79) | 0.004 |
| Urea (mg/dL) | 38 | (30–48) | 55 | (39–79) | 0.025 |
| TMA (n = 15) | Non-TMA (n = 54) | OR | 95% CI | ||||
|---|---|---|---|---|---|---|---|
| Surgery type * | n (%) | n (%) | |||||
| Aortic valve repair | 3 | (20.0) | 13 | (24.1) | 0.78 | (0.19–3.23) | |
| w/o aortic replacement | |||||||
| Mitral valve | 3 | (20.0) | 15 | (27.8) | 0.65 | (0.16–2.63) | |
| Tricuspid valve | 3 | (20.0) | 11 | (20.4) | 0.97 | (0.23–4.08) | |
| Aortic replacement with or w/o aortic valve procedure | 9 | (60.0) | 17 | (31.5) | 3.26 | (1.0013–10.64) | |
| Aortocoronary bypass | 3 | (20.0) | 13 | (24.1) | 0.79 | (0.19–3.23) | |
| Heart transplantation | 0 | (0.0) | 4 | (7.4) | 0.00 | NA | |
| Postoperative interventions | |||||||
| Postoperative v-a ECMO | 2 | (13.3) | 22 | (40.7) | 0.22 | (0.05–1.09) | |
| Multiple surgeries (2 or more) | 9 | (60.0) | 31 | (57.4) | 1.11 | (0.34–3.56) | |
| Intraoperative characteristics | |||||||
| HCA | 7 | (46.7) | 17 | (31.5) | 1.9 | (0.59–6.11) | |
| Aortic cross-clamping | 13 | (86.7) | 43 | (79.6) | 1.6 | (0.33–8.48) | |
| Median (IQR) | Median (IQR) | p-value | |||||
| CPB time (min) | 230 | (156–272) | 190 | (145–243) | 0.299 | ||
| Cross-clamp time (min) # | 161 | (109–181) | 121 | (74.5–144) | 0.048 | ||
| HCA time (min) Δ | 26 | (22–35) | 59 | (54–75) | 0.003 | ||
| SACP time (min) Δ | 22 | (21–35) | 59 | (44–75) | 0.005 | ||
| Lowest core temperature (°C) | 32 | (25–35) | 33.5 | (25.5–35.5) | 0.413 | ||
| SACP temperature (°C) Δ | 22 | (22–23) | 22 | (22–22.3) | 0.820 | ||
| Preoperative | Postoperative (Day 0–7) | p-Value | Normal Range | |||
|---|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | |||||
| Bilirubin (mg/dL) | 0.7 | (0.4–0.9) | 3.6 | (2.9–5.7) | 0.002 | <1.2 |
| LDH (U/L) | 314 | (202–388) | 1777 | (859–2631) | 0.005 | <249 |
| Hemoglobin (g/dL) | 12.3 | (11.2–14.1) | 7.8 | (7.2–8.0) | 0.0007 | 11.5–15.4 |
| Thrombocytes (G/L) | 189 | (152–250) | 40 | (28–45) | 0.0007 | 176–391 |
| Haptoglobin (g/L) | n.d. | 0.07 | (0.07–0.07) | NA | 0.3–2.0 | |
| INR | 1.1 | (1.0–1.2) | 1.2 | (1.1–1.5) | 0.409 | 0.8–1.2 |
| Fibrinogen (mg/dL) | n.d. | 419 | (338–590) | NA | 210–400 | |
| D-Dimer (ug/dL) | n.d. | 8 | (5.4–12.2) | NA | <0.5 | |
| Schistocyte count (‰) | n.d. | 9 | (6–20) | NA | <1 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigorescu, M.; Kamla, C.-E.; Wassilowsky, D.; Joskowiak, D.; Peterss, S.; Kemmner, S.; Pichlmaier, M.; Hagl, C.; Fischereder, M.; Schönermarck, U. Severe Acute Kidney Injury in Cardiovascular Surgery: Thrombotic Microangiopathy as a Differential Diagnosis to Ischemia Reperfusion Injury. A Retrospective Study. J. Clin. Med. 2020, 9, 2900. https://doi.org/10.3390/jcm9092900
Grigorescu M, Kamla C-E, Wassilowsky D, Joskowiak D, Peterss S, Kemmner S, Pichlmaier M, Hagl C, Fischereder M, Schönermarck U. Severe Acute Kidney Injury in Cardiovascular Surgery: Thrombotic Microangiopathy as a Differential Diagnosis to Ischemia Reperfusion Injury. A Retrospective Study. Journal of Clinical Medicine. 2020; 9(9):2900. https://doi.org/10.3390/jcm9092900
Chicago/Turabian StyleGrigorescu, Melissa, Christine-Elena Kamla, Dietmar Wassilowsky, Dominik Joskowiak, Sven Peterss, Stephan Kemmner, Maximilian Pichlmaier, Christian Hagl, Michael Fischereder, and Ulf Schönermarck. 2020. "Severe Acute Kidney Injury in Cardiovascular Surgery: Thrombotic Microangiopathy as a Differential Diagnosis to Ischemia Reperfusion Injury. A Retrospective Study" Journal of Clinical Medicine 9, no. 9: 2900. https://doi.org/10.3390/jcm9092900