Self-Limiting versus Rotary Subjective Carious Tissue Removal: A Randomized Controlled Clinical Trial—2-Year Results

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Method
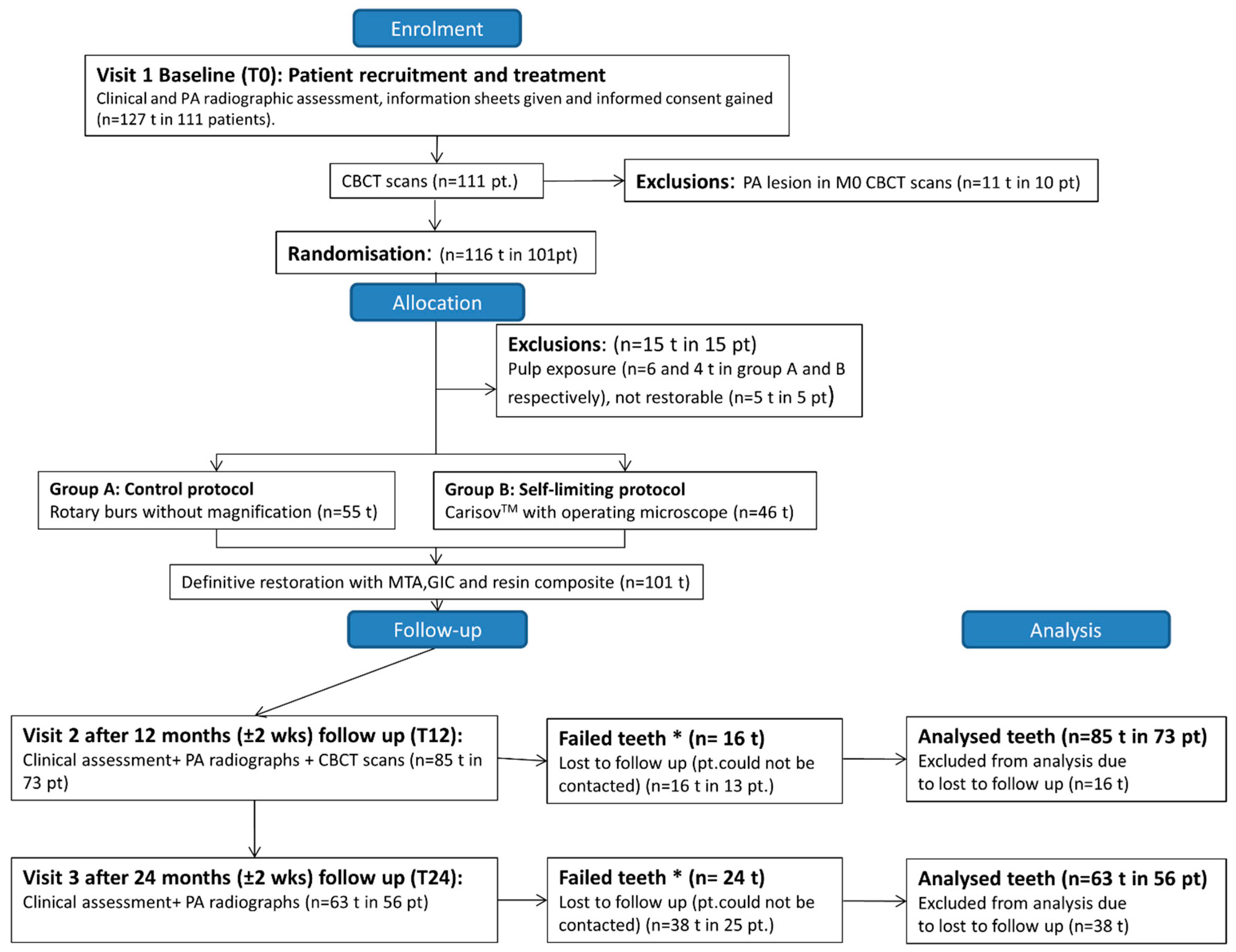
2.1. Study Design, Sample Size and Randomization
2.2. Clinical Excavation Procedures
2.3. Clinical and Radiographic Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
References
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; Markvart, M.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwendicke, F.; Göstemeyer, G. Understanding dentists’ management of deep carious lesions in permanent teeth: A systematic review and meta-analysis. Implement. Sci. 2016, 11, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjørndal, L.; Fransson, H.; Bruun, G.; Markvart, M.; Kjældgaard, M.; Hedenbjörk-Lager, A.; Dige, I.; Thordrup, M.; Näsman, P. Randomized clinical trials on deep carious lesions: 5-year follow-up. J. Dent. Res. 2017, 96, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Kidd, E.A. Clinical threshold for carious tissue removal. Dent. Clin. N. Am. 2010, 54, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Bjørndal, L.; Simon, S.; Tomson, P.L.; Duncan, H.F. Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 949–973. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Ahmadyar, M. Vital pulp therapy using calcium-enriched mixture: An evidence-based review. J. Conserv. Dent. 2013, 16, 92–98. [Google Scholar] [CrossRef]
- Asgary, S.; Torabzadeh, H. Indirect pulp therapy in a symptomatic mature molar using calcium enriched mixture cement. J. Conserv. Dent. 2013, 16, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Ricketts, D.; Lamont, T.; Innes, N.; Kidd, E.; Clarkson, J.E. Operative caries management in adults and children. Cochrane Database Syst. Rev. 2013, 3, CD003808. [Google Scholar] [CrossRef]
- Banerjee, A. Selective Removal of Carious Dentin. In Management of Deep Carious Lesions; Springer: New York, NY, USA, 2018; pp. 55–70. [Google Scholar]
- Banerjee, A.; Kidd, E.; Watson, T. In Vitro evaluation of five alternative methods of carious dentine excavation. Caries Res. 2000, 34, 144–150. [Google Scholar] [CrossRef]
- Banerjee, A.; Kellow, S.; Mannocci, F.; Cook, R.; Watson, T. An In Vitro evaluation of microtensile bond strengths of two adhesive bonding agents to residual dentine after caries removal using three excavation techniques. J. Dent. 2010, 38, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Köller, G.; Foschi, F.; Andiappan, M.; Bruce, K.; Banerjee, A.; Mannocci, F. Self-limiting versus conventional caries removal: A randomized clinical trial. J. Dent. Res. 2018, 97, 1207–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; Van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S. Managing carious lesions: Consensus recommendations on carious tissue removal. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, A.; Frencken, J.E.; Schwendicke, F.; Innes, N. Contemporary operative caries management: Consensus recommendations on minimally invasive caries removal. Br. Dent. J. 2017, 223, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Splieth, C.H.; Rosin, M.; Gellissen, B. Determination of residual dentine caries after conventional mechanical and chemomechanical caries removal with Carisolv. Clin. Oral Investig. 2001, 5, 250–253. [Google Scholar] [CrossRef]
- Neves, A.; Coutinho, E.; De Munck, J.; Van Meerbeek, B. Caries-removal effectiveness and minimal-invasiveness potential of caries-excavation techniques: A micro-CT investigation. J. Dent. 2011, 39, 154–162. [Google Scholar] [CrossRef]
- Banerjee, A.; Watson, T.; Kidd, E. Conservative dentistry: Dentine caries excavation: A review of current clinical techniques. Br. Dent. J. 2000, 188, 476. [Google Scholar] [CrossRef] [Green Version]
- Mjör, I.A. Pulp-dentin biology in restorative dentistry. Quintessence Int. 2002, 33, 113–135. [Google Scholar]
- Mejàre, I.; Axelsson, S.; Davidson, T.; Frisk, F.; Hakeberg, M.; Kvist, T.; Norlund, A.; Petersson, A.; Portenier, I.; Sandberg, H.; et al. Diagnosis of the condition of the dental pulp: A systematic review. Int. Endod. J. 2012, 45, 597–613. [Google Scholar] [CrossRef]
- Bender, I.B. Pulpal pain diagnosis—A review. J. Endod. 2000, 26, 175–179. [Google Scholar] [CrossRef]
- Aguilar, P.; Linsuwanont, P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: A systematic review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Hashem, D.; Mannocci, F.; Patel, S.; Manoharan, A.; Brown, J.; Watson, T.; Banerjee, A. Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: A randomized controlled clinical trial. J. Dent. Res. 2015, 94, 562–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashem, D.; Mannocci, F.; Patel, S.; Manoharan, A.; Watson, T.F.; Banerjee, A. Evaluation of the efficacy of calcium silicate vs. glass ionomer cement indirect pulp capping and restoration assessment criteria: A randomised controlled clinical trial—2-year results. Clin. Oral Investig. 2018, 23, 1931–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.; Wilson, R.; Dawood, A.; Foschi, F.; Mannocci, F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography—Part 2: A 1-year post-treatment follow-up. Int. Endod. J. 2012, 45, 711–723. [Google Scholar] [CrossRef]
- Ali, A.; Almaroof, A.; Festy, F.; Banerjee, A.; Mannocci, F. In Vitro remineralization of caries-affected dentin after selective carious tissue removal. World J. Dent. 2018, 9, 170–179. [Google Scholar] [CrossRef]
- Ali, A. The Assessment of a Minimally Invasive Procedure in the Treatment of Deep Carious Lesions: In Vivo and In Vitro Studies. Ph.D. Thesis, Kings College London, London, UK, 2017. [Google Scholar]
- Rupf, S.; Hannig, M.; Breitung, K.; Schellenberger, W.; Eschrich, K.; Remmerbach, T.; Kneist, S. Phenotypic heterogeneity ofstreptococcus mutansin dentin. J. Dent. Res. 2008, 87, 1172–1176. [Google Scholar] [CrossRef]
- Lager, A.H. Dentine Caries: Acid-Tolerant Microorganisms and Aspects on Collagen Degradation. Ph.D. Thesis, Faculty of Odontology, Malmö University, Malmö, Sweden, 2014. [Google Scholar]
- Caviedes-Bucheli, J.; Lombana, N.; Azuero-Holguín, M.M.; Muñoz, H.R. Quantification of neuropeptides (calcitonin gene-related peptide, substance P, neurokinin A, neuropeptide Y and vasoactive intestinal polypeptide) expressed in healthy and inflamed human dental pulp. Int. Endod. J. 2006, 39, 394–400. [Google Scholar] [CrossRef]
- Hørsted, P.; Søndergaard, B.; Thylstrup, A.; El Attar, K.; Fejerskov, O. A retrospective study of direct pulp capping with calcium hydroxide compounds. Dent. Traumatol. 1985, 1, 29–34. [Google Scholar] [CrossRef]
- Schwendicke, F.; Dörfer, C.; Paris, S. Incomplete caries removal. J. Dent. Res. 2013, 92, 306–314. [Google Scholar] [CrossRef]
- Ali, A.; Banerjee, A.; Mannocci, F. Effect of adhesive materials on shear bond strength of a mineral trioxide aggregate. Am. J. Dent. 2016, 29. [Google Scholar]
- Patel, S.; Durack, C.; Abella, F.; Roig, M.; Shemesh, H.; Lambrechts, P.; Lemberg, K. European Society of Endodontology position statement: The use of CBCT in endodontics. Int. Endod. J. 2014, 47, 502–504. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Clinical Aspects | p-Value |
|---|---|
| Age | 0.966 |
| Symptom Severity | 0.677 |
| Cavity Size | 0.692 |
| Gender | 0.929 |
| Arch | 0.691 |
| Outcome | Radiographic Outcome | Total n (%) | Kappa p-Value | ||
|---|---|---|---|---|---|
| Success/Failure n (%) | Radiographic success | Radiographic failure | 0.28 | ||
| Clinical Success | 39 (61.9%) | 7 (11.1%) | 46 (73%) a | ||
| Clinical failure | 10 (15.9%) | 7 (11.1%) | 17 (26.9%) a | ||
| Total n (%) | 49 (77.8%) b | 14 (22.2%)b | 63 (100%) | ||
| Outcome | Control Group n = 33 (%) (CI 95%) | Self-Limiting Group n = 30 (%) (CI 95%) | Total n = 63 (%) (CI 95%) | |||
|---|---|---|---|---|---|---|
| Premolar n = 6 | Molar n = 27 | Premolar n = 13 | Molar n = 17 | Premolar n = 19 | Molar n = 44 | |
| Failure n (%) | 5 (83%) (0.41–0.98) | 12 (44.4%) (0.27–0.62) a | 6 (46.2%) (0.23–0.7) | 1 (5.8%) (0.01–0.28) a | 11 (57.8%) (0.36–0.76) | 13 (29.5%) (0.18–0.44) |
| p-value | p = 0.85 | p = 0.009 * | p = 0.03 * | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, A.H.; Thani, F.B.; Foschi, F.; Banerjee, A.; Mannocci, F. Self-Limiting versus Rotary Subjective Carious Tissue Removal: A Randomized Controlled Clinical Trial—2-Year Results. J. Clin. Med. 2020, 9, 2738. https://doi.org/10.3390/jcm9092738
Ali AH, Thani FB, Foschi F, Banerjee A, Mannocci F. Self-Limiting versus Rotary Subjective Carious Tissue Removal: A Randomized Controlled Clinical Trial—2-Year Results. Journal of Clinical Medicine. 2020; 9(9):2738. https://doi.org/10.3390/jcm9092738
Chicago/Turabian StyleAli, Ahmed H., Farah Ben Thani, Federico Foschi, Avijit Banerjee, and Francesco Mannocci. 2020. "Self-Limiting versus Rotary Subjective Carious Tissue Removal: A Randomized Controlled Clinical Trial—2-Year Results" Journal of Clinical Medicine 9, no. 9: 2738. https://doi.org/10.3390/jcm9092738