Antimicrobial Effectiveness of Calcium Silicate Sealers against a Nutrient-Stressed Multispecies Biofilm

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Direct Contact Test
2.2. Multispecies Biofilm Inhibition Test
2.2.1. Specimen Preparation
2.2.2. Multispecies Biofilm Growth
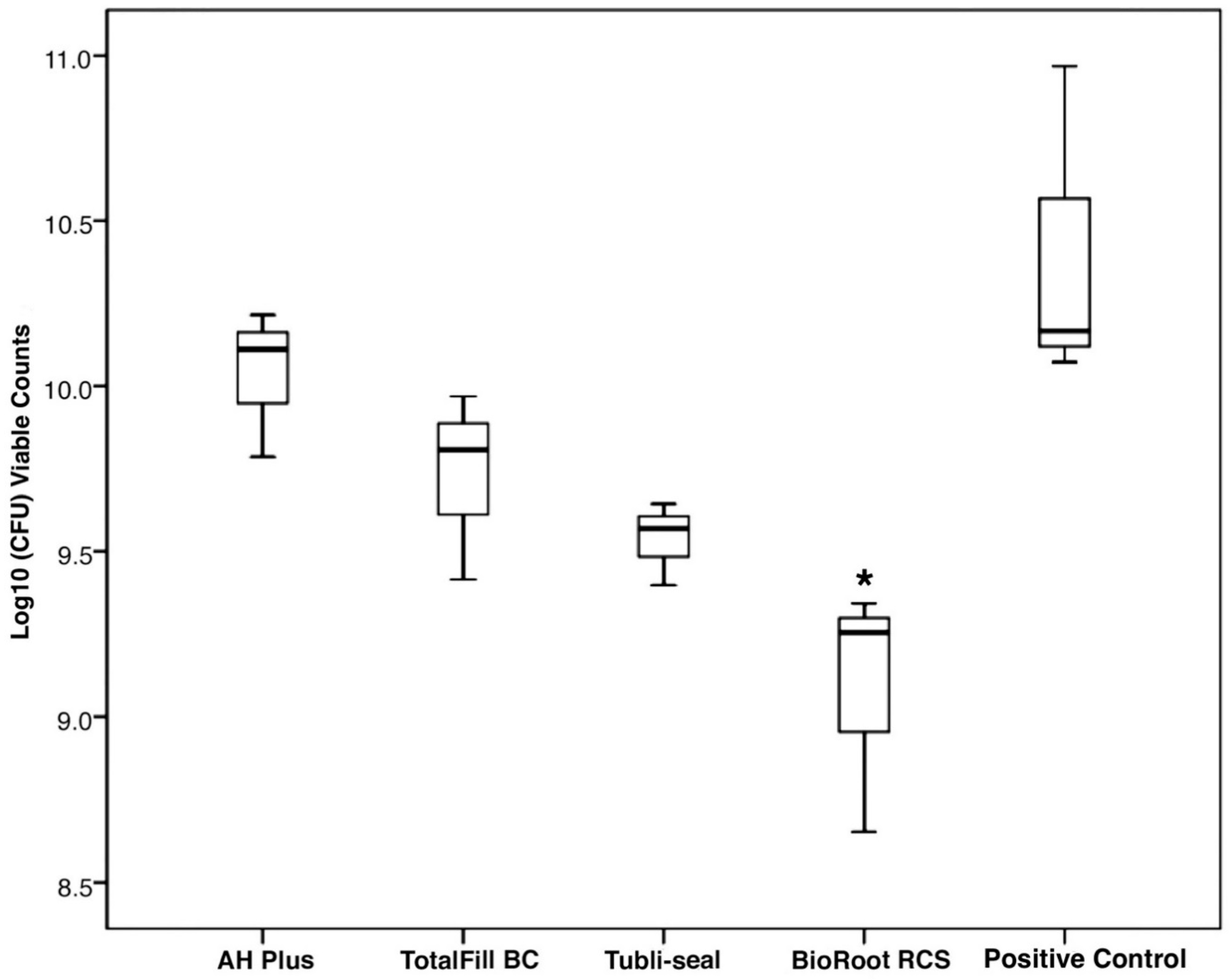
2.2.3. Determination of Quantitative Viable Counts of the Biofilms after 14 Days
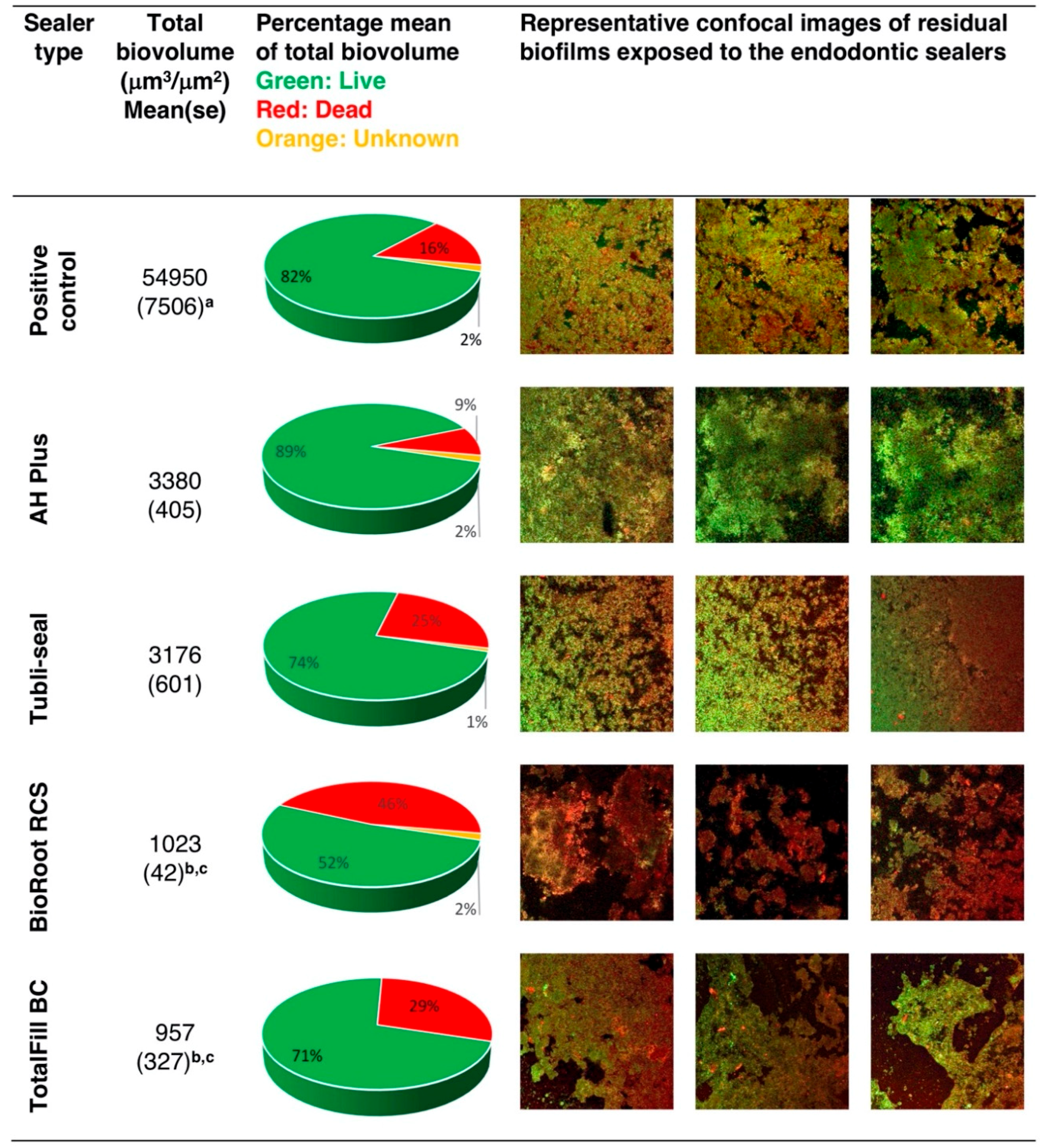
2.2.4. Confocal Laser Scanning Microscopy (CLSM) Analysis of the Multispecies Biofilm
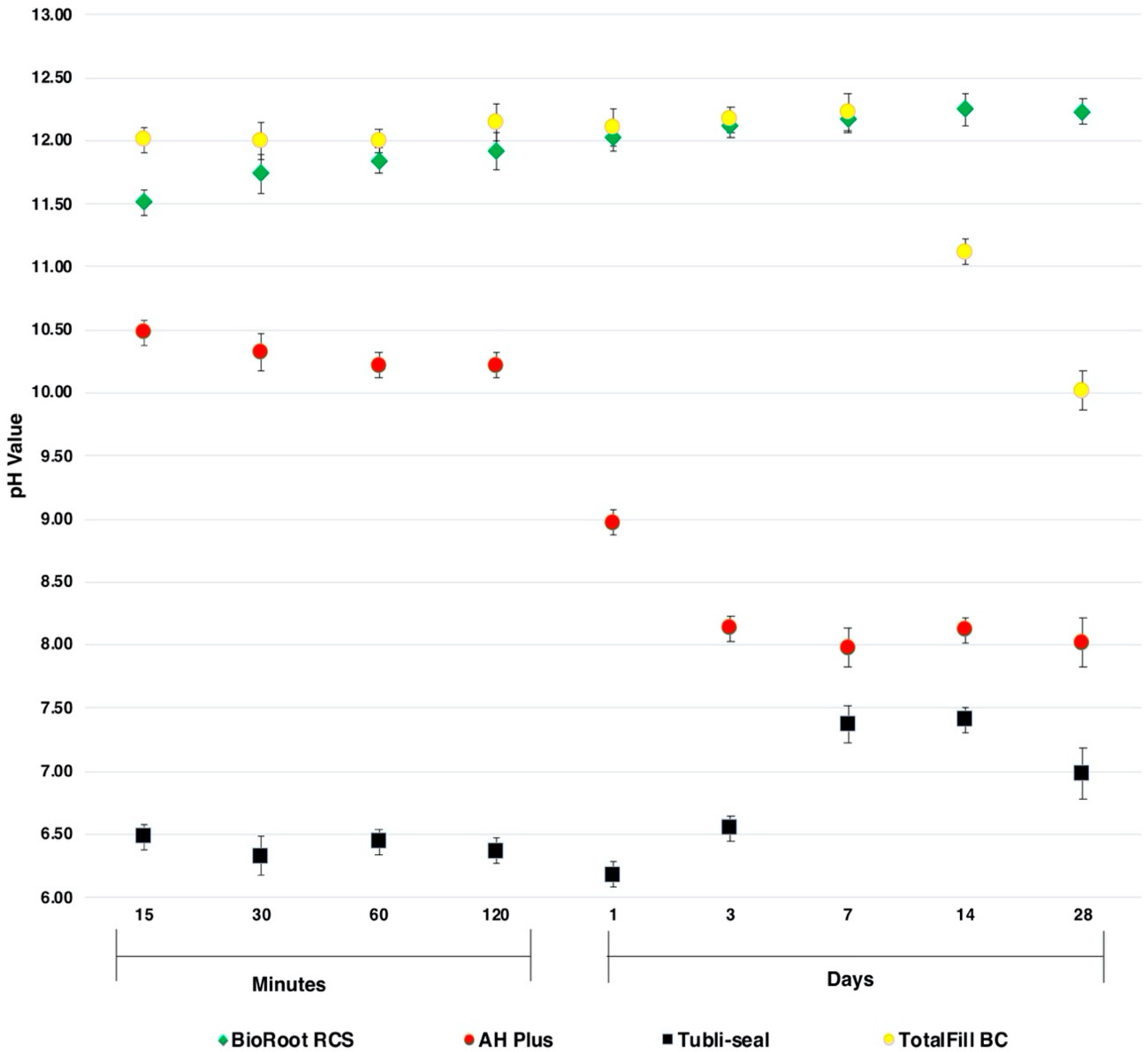
2.3. Determination of pH
2.4. Statistical Analysis
3. Results
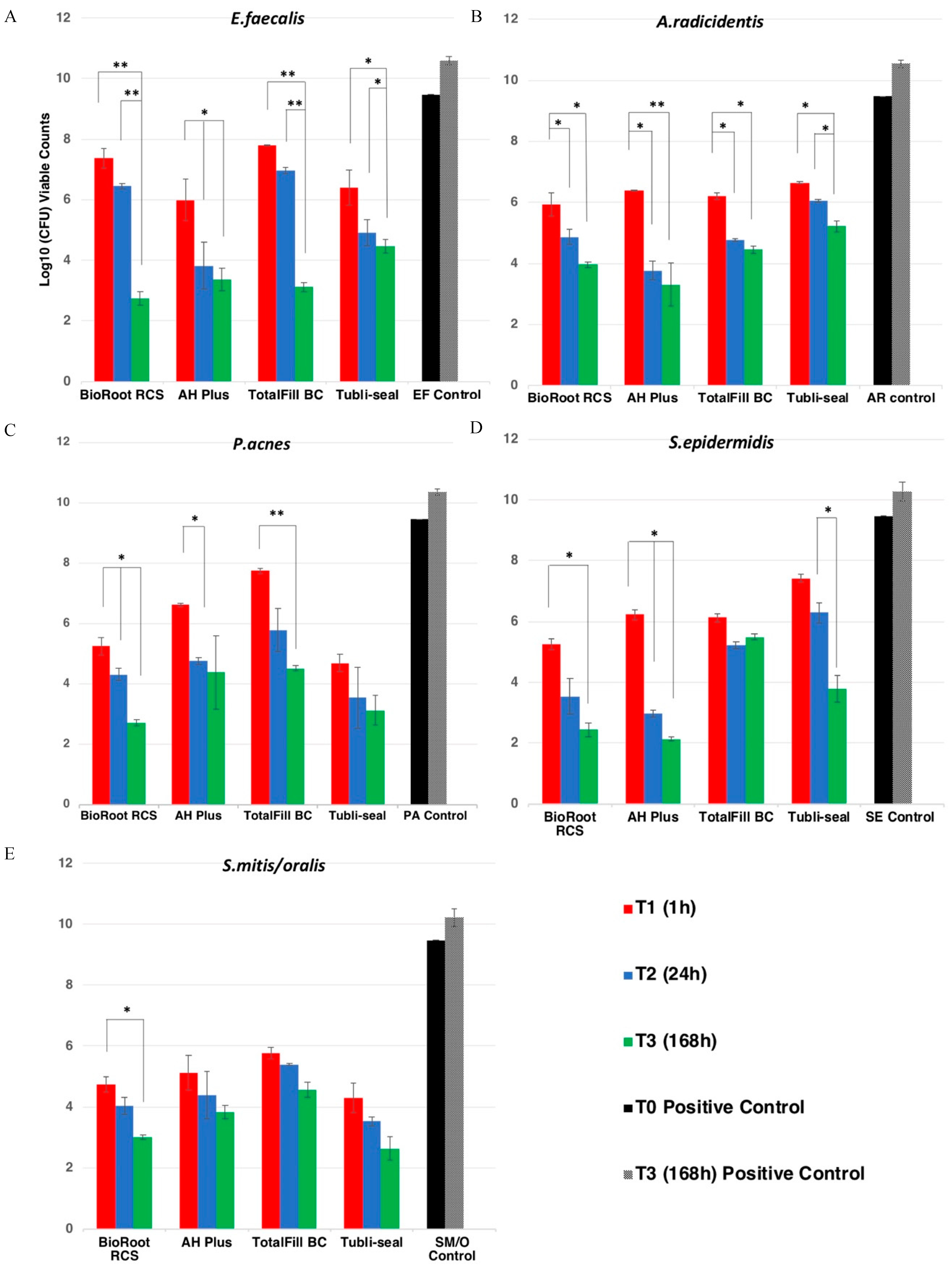
3.1. Direct Contact Test
3.1.1. Effect of Sealers on Enterococcus faecalis
3.1.2. Effect of Sealers on Actinomyces radicidentis
3.1.3. Effect of Sealers on Propionibacterium acnes
3.1.4. Effect of Sealers on Staphylococcus epidermidis
3.1.5. Effect of Sealers on Streptococcus mitis/oralis
3.2. Determination of Quantitative Viable Counts of the Biofilms after 14 Days
3.3. Confocal Laser Scanning Microscopy (CLSM) Analysis of the Effect of Endodontic Sealers on the Inhibition of Multispecies Biofilm
3.4. pH Values of the Endodontic Sealers
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R.J. The Effects of Surgical Exposures of Dental Pulps in Germ-Free and Conventional Laboratory Rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Moller, A.J.; Fabricius, L.; Dahlen, G.; Ohman, A.E.; Heyden, G. Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scand. J. Dent. Res. 1981, 89, 475–484. [Google Scholar] [CrossRef]
- Nair, P.N. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit. Rev. Oral Biol. Med. 2004, 15, 348–381. [Google Scholar] [CrossRef] [Green Version]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial biofilms: A common cause of persistent infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [Green Version]
- Peters, O.A.; Boessler, C.; Paque, F. Root canal preparation with a novel nickel-titanium instrument evaluated with micro-computed tomography: Canal surface preparation over time. J. Endod. 2010, 36, 1068–1072. [Google Scholar] [CrossRef]
- Nair, P.N. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Saunders, W.P.; Saunders, E.M. Coronal leakage as a cause of failure in root-canal therapy: A review. Dent. Traumatol. 1994, 10, 105–108. [Google Scholar] [CrossRef]
- Tronstad, L.; Asbjornsen, K.; Doving, L.; Pedersen, I.; Eriksen, H.M. Influence of coronal restorations on the periapical health of endodontically treated teeth. Dent. Traumatol. 2000, 16, 218–221. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Johansson, A.A.; Akeel, R.F.; Bergenholtz, A.; Omar, R. A retrospective analysis of factors associated with the periapical status of restored, endodontically treated teeth. Int. J. Prosthodont. 2003, 16, 31–38. [Google Scholar]
- Spångberg, L.S.W.; Haapasalo, M. Rationale and efficacy of root canal medicaments and root filling materials with emphasis on treatment outcome. Endod. Topics 2002, 2, 35–58. [Google Scholar] [CrossRef]
- Candeiro, G.T.M.; Moura-Netto, C.; D’Almeida-Couto, R.S.; Azambuja-Junior, N.; Marques, M.M.; Cai, S.; Gavini, G. Cytotoxicity, genotoxicity and antibacterial effectiveness of a bioceramic endodontic sealer. Int. Endod. J. 2016, 49, 858–864. [Google Scholar] [CrossRef]
- Jung, S.; Libricht, V.; Sielker, S.; Hanisch, M.R.; Schafer, E.; Dammaschke, T. Evaluation of the biocompatibility of root canal sealers on human periodontal ligament cells ex vivo. Odontology 2019, 107, 54–63. [Google Scholar] [CrossRef]
- Siboni, F.; Taddei, P.; Zamparini, F.; Prati, C.; Gandolfi, M.G. Properties of BioRoot RCS, a tricalcium silicate endodontic sealer modified with povidone and polycarboxylate. Int. Endod. J. 2017, 50 (Suppl. 2), e120–e136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Shen, Y.; Ruse, N.D.; Haapasalo, M. Antibacterial activity of endodontic sealers by modified direct contact test against Enterococcus faecalis. J. Endod. 2009, 35, 1051–1055. [Google Scholar] [CrossRef] [PubMed]
- Alsubait, S.; Albader, S.; Alajlan, N.; Alkhunaini, N.; Niazy, A.; Almahdy, A. Comparison of the antibacterial activity of calcium silicate- and epoxy resin-based endodontic sealers against Enterococcus faecalis biofilms: A confocal laser-scanning microscopy analysis. Odontology 2019, 107, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Karabucak, B. The Antimicrobial Effect of Bioceramic Sealer on an 8-week Matured Enterococcus faecalis Biofilm Attached to Root Canal Dentinal Surface. J. Endod. 2019, 45, 1047–1052. [Google Scholar] [CrossRef]
- Kapralos, V.; Koutroulis, A.; Orstavik, D.; Sunde, P.T.; Rukke, H.V. Antibacterial Activity of Endodontic Sealers against Planktonic Bacteria and Bacteria in Biofilms. J. Endod. 2018, 44, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Long, J.; Kreft, J.U.; Camilleri, J. Antimicrobial and ultrastructural properties of root canal filling materials exposed to bacterial challenge. J. Dent. 2020, 93, 103283. [Google Scholar] [CrossRef]
- Zakaria, M.N.; Takeshita, T.; Shibata, Y.; Maeda, H.; Wada, N.; Akamine, A.; Yamashita, Y. Microbial community in persistent apical periodontitis: A 16S rRNA gene clone library analysis. Int. Endod. J. 2015, 48, 717–728. [Google Scholar] [CrossRef]
- Ioannidis, K.; Niazi, S.; Mylonas, P.; Mannocci, F.; Deb, S. The synthesis of nano silver-graphene oxide system and its efficacy against endodontic biofilms using a novel tooth model. Dent. Mater. 2019, 35, 1614–1629. [Google Scholar] [CrossRef]
- Niazi, S.A.; Clark, D.; Do, T.; Gilbert, S.C.; Foschi, F.; Mannocci, F.; Beighton, D. The effectiveness of enzymic irrigation in removing a nutrient-stressed endodontic multispecies biofilm. Int. Endod. J. 2014, 47, 756–768. [Google Scholar] [CrossRef]
- Dahlen, G.; Konradsson, K.; Eriksson, S.; Teanpaisan, R.; Piwat, S.; Carlen, A. A microbiological study in relation to the presence of caries and calculus. Acta Odontol. Scand. 2010, 68, 199–206. [Google Scholar] [CrossRef]
- Niazi, S.A.; Clarke, D.; Do, T.; Gilbert, S.C.; Mannocci, F.; Beighton, D. Propionibacterium acnes and Staphylococcus epidermidis isolated from refractory endodontic lesions are opportunistic pathogens. J. Clin. Microbiol. 2010, 48, 3859–3869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gmur, R.; Guggenheim, B. Antigenic heterogeneity of Bacteroides intermedius as recognized by monoclonal antibodies. Infect. Immun. 1983, 42, 459–470. [Google Scholar] [CrossRef] [Green Version]
- de Chavez Paz, L.E. Image analysis software based on color segmentation for characterization of viability and physiological activity of biofilms. Appl. Environ. Microbiol. 2009, 75, 1734–1739. [Google Scholar] [CrossRef] [Green Version]
- Weiss, E.I.; Shalhav, M.; Fuss, Z. Assessment of antibacterial activity of endodontic sealers by a direct contact test. Endod. Dent. Traumatol. 1996, 12, 179–184. [Google Scholar] [CrossRef]
- Bowden, G.H.; Li, Y.H. Nutritional influences on biofilm development. Adv. Dent. Res. 1997, 11, 81–99. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N. Polymerase chain reaction detection of Propionibacterium propionicus and Actinomyces radicidentis in primary and persistent endodontic infections. Oral Surg. Oral Med. Oral Pathol. 2003, 96, 215–222. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N. Diversity of endodontic microbiota revisited. J. Dent. Res. 2009, 88, 969–981. [Google Scholar] [CrossRef]
- Ceri, H.; Olson, M.E.; Stremick, C.; Read, R.R.; Morck, D.; Buret, A. The Calgary Biofilm Device: New technology for rapid determination of antibiotic susceptibilities of bacterial biofilms. J. Clin. Microbiol. 1999, 37, 1771–1776. [Google Scholar] [CrossRef] [Green Version]
- Prosser, B.L.; Taylor, D.; Dix, B.A.; Cleeland, R. Method of evaluating effects of antibiotics on bacterial biofilm. Antimicrob. Agents Chemother. 1987, 31, 1502–1506. [Google Scholar] [CrossRef] [Green Version]
- Koutroulis, A.; Kuehne, S.A.; Cooper, P.R.; Camilleri, J. The role of calcium ion release on biocompatibility and antimicrobial properties of hydraulic cements. Sci. Rep. 2019, 9, 19019. [Google Scholar] [CrossRef] [Green Version]
- Kebudi Benezra, M.; Schembri Wismayer, P.; Camilleri, J. Influence of environment on testing of hydraulic sealers. Sci. Rep. 2017, 7, 17927. [Google Scholar] [CrossRef] [PubMed]
- Urban, K.; Neuhaus, J.; Donnermeyer, D.; Schafer, E.; Dammaschke, T. Solubility and pH Value of 3 Different Root Canal Sealers: A Long-term Investigation. J. Endod. 2018, 44, 1736–1740. [Google Scholar] [CrossRef]
- Zamparini, F.; Siboni, F.; Prati, C.; Taddei, P.; Gandolfi, M.G. Properties of calcium silicate-monobasic calcium phosphate materials for endodontics containing tantalum pentoxide and zirconium oxide. Clin. Oral Investig. 2019, 23, 445–457. [Google Scholar] [CrossRef]
- Slutzky-Goldberg, I.; Slutzky, H.; Solomonov, M.; Moshonov, J.; Weiss, E.I.; Matalon, S. Antibacterial properties of four endodontic sealers. J. Endod. 2008, 34, 735–738. [Google Scholar] [CrossRef]
- Huang, T.H.; Yang, J.J.; Li, H.; Kao, C.T. The biocompatibility evaluation of epoxy resin-based root canal sealers in vitro. Biomaterials 2002, 23, 77–83. [Google Scholar] [CrossRef]
- Orstavik, D.; Mjor, I.A. Histopathology and x-ray microanalysis of the subcutaneous tissue response to endodontic sealers. J. Endod. 1988, 14, 13–23. [Google Scholar] [CrossRef]
- Orstavik, D. Weight loss of endodontic sealers, cements and pastes in water. Scand. J. Dent. Res. 1983, 91, 316–319. [Google Scholar] [CrossRef]
- Meryon, S.D.; Johnson, S.G.; Smith, A.J. Eugenol release and the cytotoxicity of different zinc oxide-eugenol combination. J. Dent. 1988, 16, 66–70. [Google Scholar] [CrossRef]
- Kontakiotis, E.G.; Wu, M.K.; Wesselink, P.R. Effect of sealer thickness on long-term sealing ability: A 2-year follow-up study. Int. Endod. J. 1997, 30, 307–312. [Google Scholar] [CrossRef]
- Colombo, M.; Poggio, C.; Dagna, A.; Meravini, M.V.; Riva, P.; Trovati, F.; Pietrocola, G. Biological and physico-chemical properties of new root canal sealers. J. Clin. Exp. Dent. 2018, 10, e120–e126. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Li, L.; Zheng, Y.F.; Haapasalo, M. Physical properties of 5 root canal sealers. J. Endod. 2013, 39, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y.; Fleury, A.; Solomon, E.; He, J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis. J. Endod. 2018, 44, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Zavattini, A.; Knight, A.; Foschi, F.; Mannocci, F. Outcome of Root Canal Treatments Using a New Calcium Silicate Root Canal Sealer: A Non-Randomized Clinical Trial. J. Clin. Med. 2020, 9, 782. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sealer | Type | Availability | Composition |
|---|---|---|---|
| TotalFill BC | Calcium silicate | Preloaded syringe | 35.0−45.0% Zirconium Oxide 20.0−35.0% Tricalcium silicate 7.0−15.0% Dicalcium silicate 1.0−4.0% Calcium hydroxide |
| BioRoot RCS | Calcium silicate | Hand-mix presentation | (a) Powder: Tricalcium silicate, zirconium oxide, Povidone (b) Liquid: Aqueous solution of calcium chloride and polycarboxylate |
| AH Plus | Epoxy resin | Mixing syringe | (a) Epoxide paste: Diepoxide, Calcium tungstate, Zirconium Oxide, Aerosil, Pigment (b) Amine Paste:1-adamantane-amine, N,N′-dibenyl-5-oxa-nonandiamine-1-9,TCD-Diamine, Calcium tungstate, Aerosil, Silicone oil |
| Tubli-seal | Zinc Oxide Eugenol | Mixing syringe | (a) Accelerator: 10−50% eugenol, 20% 5,5′-diisopropyl-2,2′-dimethylbiphenyl-4,4′-diyl dihypoiodite <2.5% zinc acetate dihydrate (b)Base: 50−80% zinc oxide,1−30%, Petroleum, barium sulphate, Starch |
| Sealer | Setting Times |
|---|---|
| TotalFill BC | 4–10 h |
| BioRoot RCS | 4 h |
| AH Plus | 24 h |
| Tubli-seal | 2 h |
| Bacteria | Sealers | T1, Mean ± SE | T2, Mean ± SE | T3, Mean ± SE |
|---|---|---|---|---|
| EF | BioRoot RCS | 7.36 (0.32) | 6.45 (0.09) * | 2.74 (0.21) * ***** |
| AH Plus | 5.98 (0.68) * ** **** | 3.81 (0.77) * | 3.36 (0.36) * | |
| TotalFill BC | 7.71 (0.02) | 6.97 (0.1) | 3.12 (0.15) * | |
| Tubli-seal | 6.40 (0.58) * | 4.91 (0.44) * | 4.47 (0.23) * | |
| AR | BioRoot RCS | 5.42 (0.38) * | 4.21 (0.24) * ***** | 3.96 (0.09) * |
| AH Plus | 6.39 (0.02) * | 3.77 (0.32) * ***** | 3.31 (0.71) * | |
| TotalFill BC | 6.21 (0.1) * | 4.77 (0.05) * ***** | 4.54 (0.12) * | |
| Tubli-seal | 6.65 (0.03) * | 6.06 (0.04) * | 5.22 (0.19) * | |
| PA | BioRoot RCS | 5.26 (0.28) * *** **** | 4.33 (0.21) * | 2.72 (0.11) * **** |
| AH Plus | 6.63 (0.06) * **** | 4.77 (0.12) * | 4.40 (1.21) * | |
| TotalFill BC | 7.75 (0.09) | 5.80 (0.70) * | 4.53 (0.09) * | |
| Tubli-seal | 4.69 (0.29) * *** **** | 3.56 (1.01) * | 3.14 (0.49) * | |
| SE | BioRoot RCS | 5.27 (0.18) * ***** | 3.54 (0.60) * **** ***** | 2.44 (0.23) * **** |
| AH Plus | 6.23 (0.16) * ***** | 2.97 (0.12) * **** ***** | 2.13 (0.07) * **** | |
| TotalFill BC | 6.13 (0.13) * ***** | 5.22 (0.11) * | 5.50 (0.10) * | |
| Tubli-seal | 7.42 (0.13) | 6.29 (0.32) * | 3.79 (0.43) * **** | |
| Sm/o | BioRoot RCS | 4.73 (0.25) * **** | 4.03 (0.28) * **** | 3.01 (0.08) * *** **** |
| AH Plus | 5.11 (0.57) * | 4.39 (0.77) * | 3.84 (0.22) * | |
| TotalFill BC | 5.77 (0.18) * | 5.39 (0.03) * | 4.56 (0.25) * | |
| Tubli-seal | 4.30 (0.47) * *** **** | 3.53 (0.14) * **** | 3.34 (0.05) * *** **** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bose, R.; Ioannidis, K.; Foschi, F.; Bakhsh, A.; Kelly, R.D.; Deb, S.; Mannocci, F.; Niazi, S.A. Antimicrobial Effectiveness of Calcium Silicate Sealers against a Nutrient-Stressed Multispecies Biofilm. J. Clin. Med. 2020, 9, 2722. https://doi.org/10.3390/jcm9092722
Bose R, Ioannidis K, Foschi F, Bakhsh A, Kelly RD, Deb S, Mannocci F, Niazi SA. Antimicrobial Effectiveness of Calcium Silicate Sealers against a Nutrient-Stressed Multispecies Biofilm. Journal of Clinical Medicine. 2020; 9(9):2722. https://doi.org/10.3390/jcm9092722
Chicago/Turabian StyleBose, Rahul, Konstantinos Ioannidis, Federico Foschi, Abdulaziz Bakhsh, Robert D. Kelly, Sanjukta Deb, Francesco Mannocci, and Sadia Ambreen Niazi. 2020. "Antimicrobial Effectiveness of Calcium Silicate Sealers against a Nutrient-Stressed Multispecies Biofilm" Journal of Clinical Medicine 9, no. 9: 2722. https://doi.org/10.3390/jcm9092722