Optimizing Preparative Regimen for Umbilical Cord Blood Transplantation in Adult Acute Leukemia Patients: Acute Lymphoblastic Leukemia Requires Myeloablative Conditioning but Not Acute Myeloid Leukemia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. HLA Typing and Donor Selection
2.3. Conditioning Regimen and GVHD Prophylaxis
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Engraftment
3.3. GVHD
3.4. Complications other than GVHD
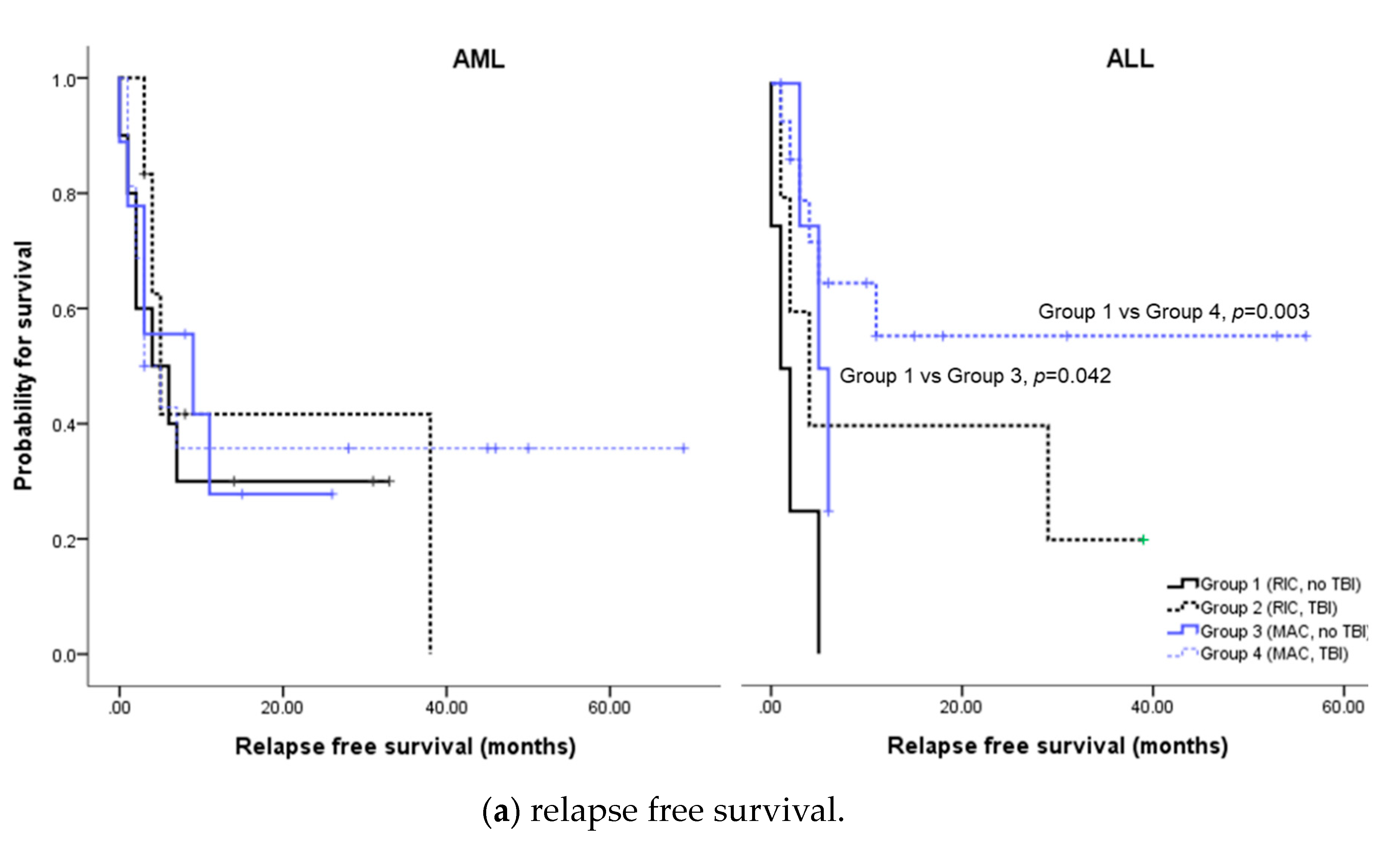
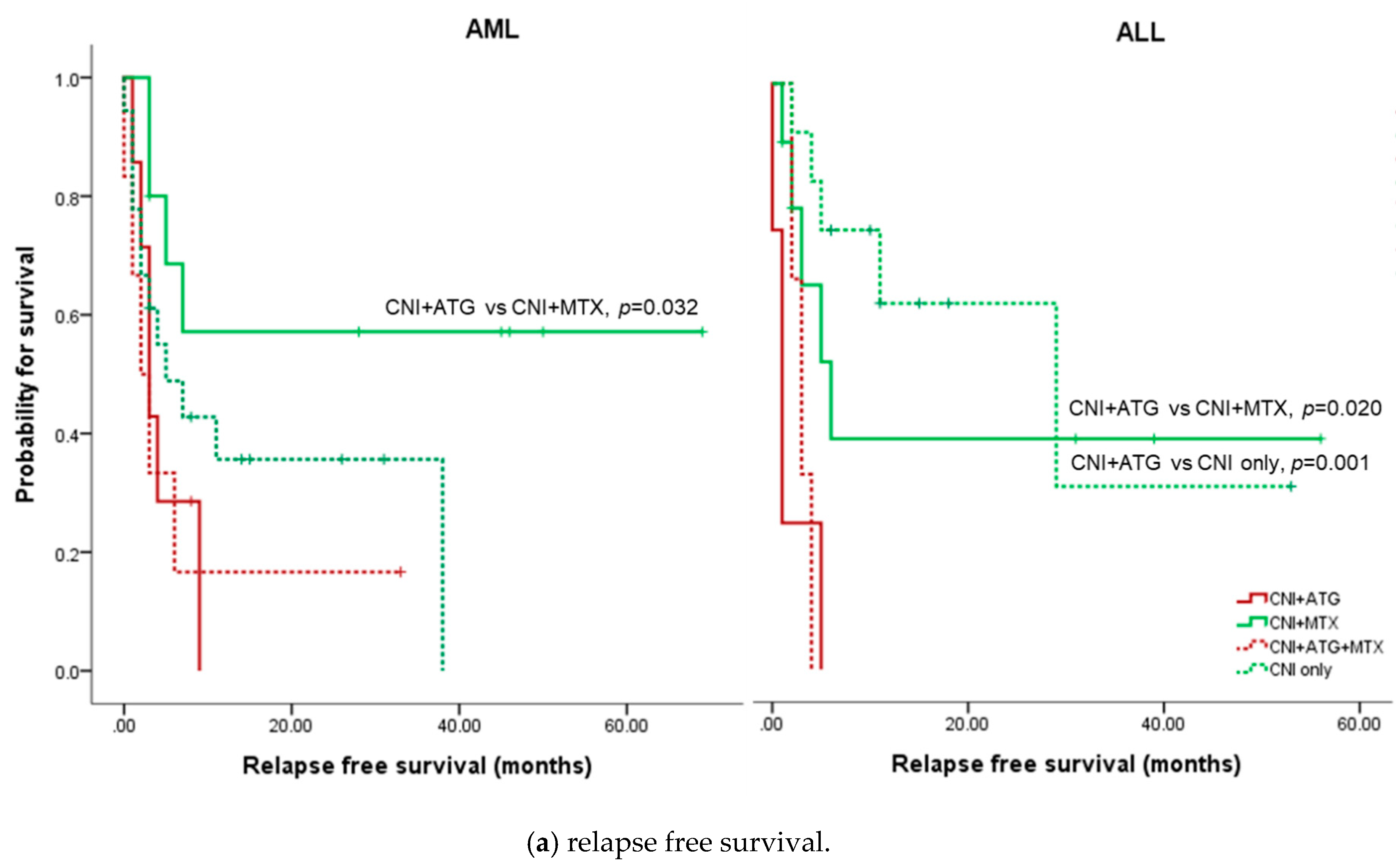
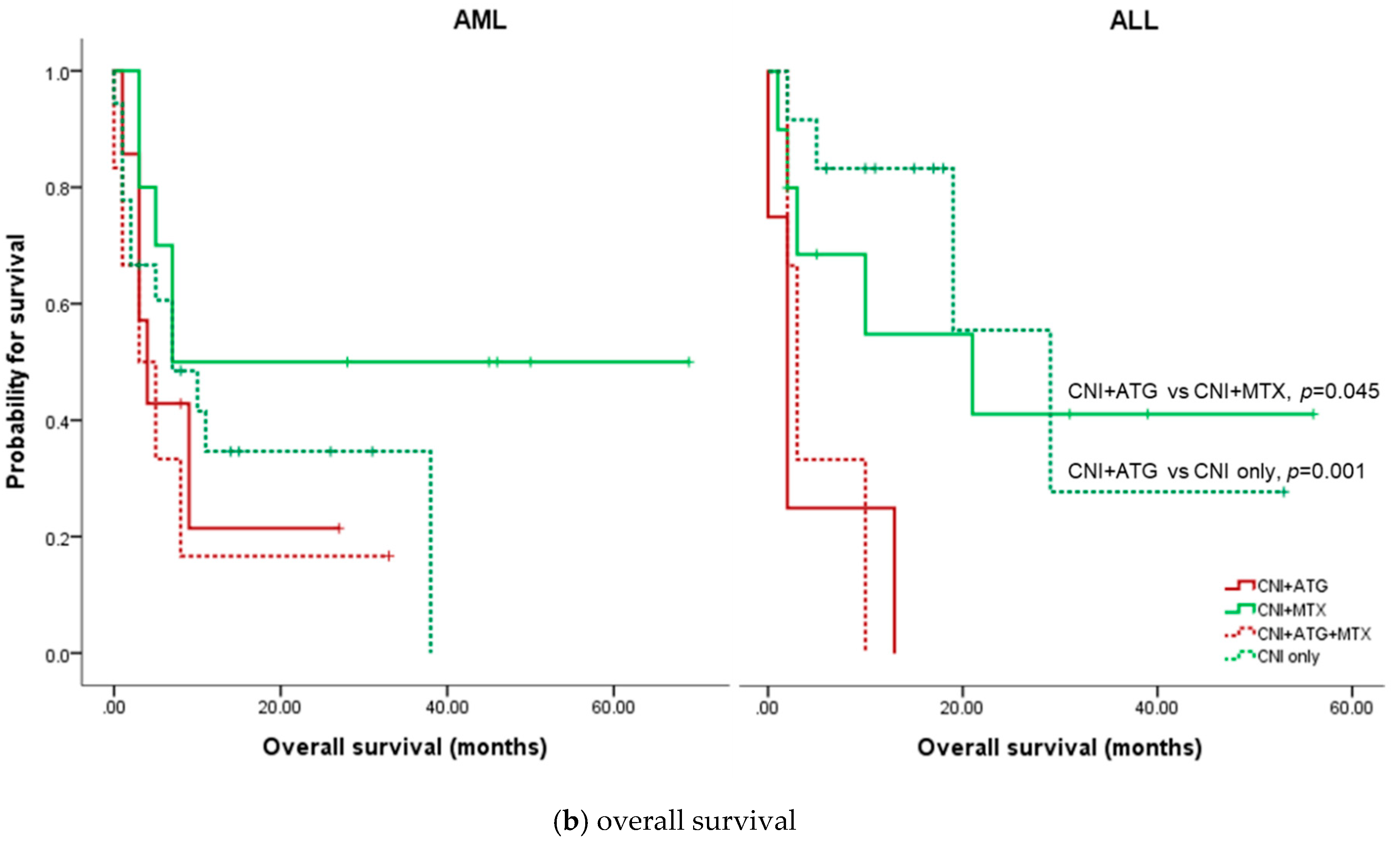
3.5. Relapse free Survival and overall survival of AML
3.6. Relapse Free Survival and Overall Survival of ALL
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schoemans, H.; Theunissen, K.; Maertens, J.; Boogaerts, M.; Verfaillie, C.M.; Wagner, J. Adult umbilical cord blood transplantation: A comprehensive review. Bone Marrow Transplant. 2006, 38, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.A.; Boussiotis, V.A. Umbilical cord blood transplantation: Basic biology and clinical challenges to immune reconstitution. Clin. Immunol. 2008, 127, 286–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robin, M.; Ruggeri, A.; Labopin, M.; Niederwieser, D.; Tabrizi, R.; Sanz, G.; Bourhis, J.-H.; Van Biezen, A.; Koenecke, C.; Blaise, D.; et al. Comparison of Unrelated Cord Blood and Peripheral Blood Stem Cell Transplantation in Adults with Myelodysplastic Syndrome after Reduced-Intensity Conditioning Regimen: A Collaborative Study from Eurocord (Cord blood Committee of Cellular Therapy & Immunobiology Working Party of EBMT) and Chronic Malignancies Working Party. Biol. Blood Marrow Transplant. 2015, 21, 489–495. [Google Scholar]
- Atsuta, Y.; Suzuki, R.; Nagamura-Inoue, T.; Taniguchi, S.; Takahashi, S.; Kai, S.; Sakamaki, H.; Kouzai, Y.; Kasai, M.; Fukuda, T.; et al. Disease-specific analyses of unrelated cord blood transplantation compared with unrelated bone marrow transplantation in adult patients with acute leukemia. Blood 2009, 113, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Milano, F.; Gooley, T.; Wood, B.; Woolfrey, A.; Flowers, M.E.; Doney, K.; Witherspoon, R.; Mielcarek, M.; Deeg, J.H.; Sorror, M.; et al. Cord-Blood Transplantation in Patients with Minimal Residual Disease. N. Engl. J. Med. 2016, 375, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Eapen, M.; Rocha, V.; Sanz, G.; Scaradavou, A.; Zhang, M.-J.; Arcese, W.; Sirvent, A.; Champlin, R.E.; Chao, N.; Gee, A.P.; et al. Effect of graft source on unrelated donor haemopoietic stem-cell transplantation in adults with acute leukaemia: A retrospective analysis. Lancet Oncol. 2010, 11, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Eapen, M.; Rubinstein, P.; Zhang, M.-J.; Stevens, C.; Kurtzberg, J.; Scaradavou, A.; Loberiza, F.R.; E Champlin, R.; Klein, J.P.; Horowitz, M.M.; et al. Outcomes of transplantation of unrelated donor umbilical cord blood and bone marrow in children with acute leukaemia: A comparison study. Lancet 2007, 369, 1947–1954. [Google Scholar] [CrossRef]
- Atsuta, Y.; Morishima, Y.; Suzuki, R.; Nagamura-Inoue, T.; Taniguchi, S.; Takahashi, S.; Kai, S.; Sakamaki, H.; Kouzai, Y.; Kobayashi, N.; et al. Comparison of Unrelated Cord Blood Transplantation and HLA-Mismatched Unrelated Bone Marrow Transplantation for Adults with Leukemia. Biol. Blood Marrow Transplant. 2012, 18, 780–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, V.; Labopin, M.; Sanz, G.; Arcese, W.; Schwerdtfeger, R.; Bosi, A.; Jacobsen, N.; Ruutu, T.; De Lima, M.; Finke, J.; et al. Transplants of Umbilical-Cord Blood or Bone Marrow from Unrelated Donors in Adults with Acute Leukemia. N. Engl. J. Med. 2004, 351, 2276–2285. [Google Scholar] [CrossRef]
- Takahashi, S.; Ooi, J.; Tomonari, A.; Konuma, T.; Tsukada, N.; Oiwa-Monna, M.; Fukuno, K.; Uchiyama, M.; Takasugi, K.; Iseki, T.; et al. Comparative single-institute analysis of cord blood transplantation from unrelated donors with bone marrow or peripheral blood stem-cell transplants from related donors in adult patients with hematologic malignancies after myeloablative conditioning regimen. Blood 2006, 109, 1322–1330. [Google Scholar]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol. Blood Marrow Transplant. 2015, 21, 389–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascal, L.; Tucunduva, L.; Ruggeri, A.; Blaise, D.; Ceballos, P.; Chevallier, P.; Cornelissen, J.; Maillard, N.; Tabrizi, R.; Petersen, E.; et al. Impact of ATG-containing reduced-intensity conditioning after single- or double-unit allogeneic cord blood transplantation. Blood 2015, 126, 1027–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascal, L.; Mohty, M.; Ruggeri, A.; Tucunduva, L.; Milpied, N.; Chevallier, P.; Tabrizi, R.; Labalette, M.; Gluckman, E.; Labopin, M.; et al. Impact of rabbit ATG-containing myeloablative conditioning regimens on the outcome of patients undergoing unrelated single-unit cord blood transplantation for hematological malignancies. Bone Marrow Transplant. 2014, 50, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, J.N.; Weisdorf, D.J.; DeFor, T.; Blazar, B.R.; Miller, J.S.; E Wagner, J. Rapid and complete donor chimerism in adult recipients of unrelated donor umbilical cord blood transplantation after reduced-intensity conditioning. Blood 2003, 102, 1915–1919. [Google Scholar] [CrossRef] [Green Version]
- Ballen, K.K.; Spitzer, T.R.; Yeap, B.Y.; McAfee, S.; Dey, B.R.; Attar, E.; Haspel, R.; Kao, G.; Liney, D.; Alyea, E.; et al. Double Unrelated Reduced-Intensity Umbilical Cord Blood Transplantation in Adults. Biol. Blood Marrow Transplant. 2007, 13, 82–89. [Google Scholar] [CrossRef] [Green Version]
- Brunstein, C.G.; Gutman, J.A.; Weisdorf, D.J.; Woolfrey, A.E.; DeFor, T.E.; Gooley, T.A.; Verneris, M.R.; Appelbaum, F.R.; Wagner, J.E.; Delaney, C. Allogeneic hematopoietic cell transplantation for hematologic malignancy: Relative risks and benefits of double umbilical cord blood. Blood 2010, 116, 4693–4699. [Google Scholar] [CrossRef] [Green Version]
- Weisdorf, D.; Eapen, M.; Ruggeri, A.; Zhang, M.-J.; Zhong, X.; Brunstein, C.; Ustun, C.; Rocha, V.; Gluckman, E. Alternative donor transplantation for older patients with acute myeloid leukemia in first complete remission: A center for international blood and marrow transplant research-eurocord analysis. Biol. Blood Marrow Transplant. 2014, 20, 816–822. [Google Scholar] [CrossRef] [Green Version]
- De Latour, R.P.; Brunstein, C.G.; Porcher, R.; Chevallier, P.; Robin, M.; Warlick, E.; Xhaard, A.; Ustun, C.; Larghéro, J.; Dhédin, N.; et al. Similar Overall Survival Using Sibling, Unrelated Donor, and Cord Blood Grafts after Reduced-Intensity Conditioning for Older Patients with Acute Myelogenous Leukemia. Biol. Blood Marrow Transplant. 2013, 19, 1355–1360. [Google Scholar] [CrossRef] [Green Version]
- Brunstein, C.G.; Fuchs, E.J.; Carter, S.L.; Karanes, C.; Costa, L.J.; Wu, J.; Devine, S.M.; Wingard, J.R.; Aljitawi, O.S.; Cutler, C.S.; et al. Alternative donor transplantation after reduced intensity conditioning: Results of parallel phase 2 trials using partially HLA-mismatched related bone marrow or unrelated double umbilical cord blood grafts. Blood 2011, 118, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Ballen, K.K.; Lazarus, H. Cord blood transplant for acute myeloid leukaemia. Br. J. Haematol. 2016, 173, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narimatsu, H.; for the Nagoya Blood and Marrow Transplantation Group (NBMTG); Terakura, S.; Matsuo, K.; Oba, T.; Uchida, T.; Iida, H.; Hamaguchi, M.; Watanabe, M.; Kohno, A.; Murata, M.; et al. Short-term methotrexate could reduce early immune reactions and improve outcomes in umbilical cord blood transplantation for adults. Bone Marrow Transplant. 2006, 39, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terakura, S.; Azuma, E.; Murata, M.; Kumamoto, T.; Hirayama, M.; Atsuta, Y.; Kodera, Y.; Yazaki, M.; Naoe, T.; Kato, K. Hematopoietic Engraftment in Recipients of Unrelated Donor Umbilical Cord Blood Is Affected by the CD34+ and CD8+ Cell Doses. Biol. Blood Marrow Transplant. 2007, 13, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S.; Iseki, T.; Ooi, J.; Tomonari, A.; Takasugi, K.; Shimohakamada, Y.; Yamada, T.; Uchimaru, K.; Tojo, A.; Shirafuji, N.; et al. Single-institute comparative analysis of unrelated bone marrow transplantation and cord blood transplantation for adult patients with hematologic malignancies. Blood 2004, 104, 3813–3820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, K.; Yoshimi, A.; Ito, E.; Oki, K.; Hara, J.; Nagatoshi, Y.; Kikuchi, A.; Kobayashi, R.; Nagamura-Inoue, T.; Kai, S.; et al. Cord Blood Transplantation from Unrelated Donors for Children with Acute Lymphoblastic Leukemia in Japan: The Impact of Methotrexate on Clinical Outcomes. Biol. Blood Marrow Transplant. 2011, 17, 1814–1821. [Google Scholar] [CrossRef] [Green Version]
- Komanduri, K.V.; John, L.S.S.; De Lima, M.; McMannis, J.; Rosinski, S.; Mcniece, I.; Bryan, S.G.; Kaur, I.; Martin, S.; Wieder, E.D.; et al. Delayed immune reconstitution after cord blood transplantation is characterized by impaired thymopoiesis and late memory T-cell skewing. Blood 2007, 110, 4543–4551. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, T.; Network, F.T.J.C.B.B.; Kami, M.; Yamaguchi, T.; Yuji, K.; Kusumi, E.; Taniguchi, S.; Takahashi, S.; Okada, M.; Sakamaki, H.; et al. Allogeneic cord blood transplantation for adult acute lymphoblastic leukemia: Retrospective survey involving 256 patients in Japan. Leukemia 2012, 26, 1482–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- I Marks, D.; Aversa, F.; Lazarus, H.M. Alternative donor transplants for adult acute lymphoblastic leukaemia: A comparison of the three major options. Bone Marrow Transplant. 2006, 38, 467–475. [Google Scholar] [CrossRef] [Green Version]
- Marks, D.I.; Woo, K.A.; Zhong, X.; Appelbaum, F.R.; Bachanova, V.; Barker, J.N.; Brunstein, C.G.; Gibson, J.; Kebriaei, P.; Lazarus, H.M.; et al. Unrelated umbilical cord blood transplant for adult acute lymphoblastic leukemia in first and second complete remission: A comparison with allografts from adult unrelated donors. Haematologica 2013, 99, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Davies, S.M.; Ramsay, N.K.C.; Klein, J.P.; Weisdorf, D.J.; Bolwell, B.; Cahn, J.-Y.; Camitta, B.M.; Gale, R.P.; Giralt, S.; Heilmann, C.; et al. Comparison of Preparative Regimens in Transplants for Children With Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2000, 18, 340. [Google Scholar] [CrossRef]
- Bunin, N.J.; Aplenc, R.; Kamani, N.; Shaw, K.; Cnaan, A.; Simms, S. Randomized trial of busulfan vs total body irradiation containing conditioning regimens for children with acute lymphoblastic leukemia: A Pediatric Blood and Marrow Transplant Consortium study. Bone Marrow Transplant. 2003, 32, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahu, X.; Ebmt, O.B.O.T.A.L.W.P.O.; Labopin, M.; Giebel, S.; Aljurf, M.; Kyrcz-Krzemien, S.; Socie, G.; Eder, M.; Bonifazi, F.; Bunjes, D.; et al. Impact of conditioning with TBI in adult patients with T-cell ALL who receive a myeloablative allogeneic stem cell transplantation: A report from the acute leukemia working party of EBMT. Bone Marrow Transplant. 2015, 51, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labopin, M.; Ruggeri, A.; Gorin, N.C.; Gluckman, E.; Blaise, D.; Mannone, L.; Milpied, N.; Yakoub-Agha, I.; Deconinck, E.; Michallet, M.; et al. Cost-effectiveness and clinical outcomes of double versus single cord blood transplantation in adults with acute leukemia in France. Haematologica 2013, 99, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, J.N.; Scaradavou, A.; Stevens, C.E. Combined effect of total nucleated cell dose and HLA match on transplantation outcome in 1061 cord blood recipients with hematologic malignancies. Blood 2010, 115, 1843–1849. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.S. Introduction: Health of the Health Care System in Korea. Soc. Work. Public Health 2010, 25, 127–141. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All N = 70 (%) | AML N = 41 (%) | ALL N = 29 (%) | P | |
|---|---|---|---|---|
| Age at transplantation, years (median, range) | 44 (18–66) | 47 (22–66) | 29 (18–64) | <0.001 |
| Sex, male | 35 (50.0) | 18 (43.9) | 17 (58.6) | 0.225 |
| Body weight, kg (median, range) | 59.5 (43–98) | 60 (43–90) | 58 (45–98) | 0.787 |
| Diagnosis to transplantation, months (median, range) | 7 (2–85) | 9 (3–85) | 7 (2–76) | 0.425 |
| Transplantation period | ||||
| 2001–2004 | 5 (7.1) | 4 (9.8) | 1 (3.4) | 0.542 |
| 2005–2009 | 17 (24.3) | 9 (22.0) | 8 (27.6) | |
| 2010–2014 | 20 (28.6) | 10 (24.4) | 10 (34.5) | |
| 2015–2019 | 28 (40.0) | 18 (43.9) | 10 (34.5) | |
| Disease status at transplantation | ||||
| CR1 | 43 (61.4) | 24 (58.5) | 19 (65.5) | 0.195 |
| CR2 | 13 (18.6) | 6 (14.6) | 7 (24.1) | |
| Others* | 14 (20.0) | 11 (26.8) | 3 (10.3) | |
| Conditioning regimen | ||||
| Myeloablative | ||||
| TBI containing | 31 (44.3) | 16 (39.0) | 15 (51.7) | 0.608 |
| Non-TBI containing | 14 (20.0) | 9 (22.0) | 5 (17.2) | |
| Reduced intensity | ||||
| TBI containing | 11 (15.7) | 6 (14.6) | 5 (17.2) | 0.600 |
| Non-TBI containing | 14 (20.0) | 10 (24.4) | 4 (13.8) | |
| GVHD prophylaxis | ||||
| CNI + ATG | 11 (15.7) | 7 (17.1) | 4 (13.8) | 0.804 |
| CNI + MTX | 20 (28.6) | 10 (24.4) | 10 (34.5) | |
| CNI + MTX + ATG | 9 (12.9) | 6 (14.6) | 3 (10.3) | |
| CNI only | 30 (42.9) | 18 (43.9) | 12 (41.4) | |
| Infused cord blood | ||||
| Total nucleated cells, 107/kg (median, range) | 2.5 (1.0–5.2) | 2.4 (1.0–5.2) | 2.5 (1.0–4.1) | 0.947 |
| CD34+ cells, 105/kg (median, range) | 1.0 (0.1–4.1) | 1.2 (0.1–4.1) | 1.0 (0.1–2.7) | 0.413 |
| Single unit HLA matching (N = 13) | ||||
| 6/6 | 1 (7.7) | 1 (10.0) | 0 | 0.557 |
| 5/6 | 2 (15.4) | 1 (10.0) | 1 (33.3) | |
| 4/6 | 10 (76.9) | 8 (80.0) | 2 (66.7) | |
| Double unit HLA matching (N = 57) | ||||
| 4/6 + 4/6 | 8 (14.0) | 6 (19.4) | 2 (7.7) | 0.443 |
| 5/6 + 5/6 | 18 (31.6) | 12 (38.7) | 6 (23.1) | |
| 6/6 + 6/6 | 5 (8.8) | 2 (6.5) | 3 (11.5) | |
| 6/6 + 5/6 | 2 (3.5) | 0 | 2 (7.7) | |
| 6/6 + 4/6 | 2 (3.5) | 1 (3.2) | 1 (3.8) | |
| 6/6 + 3/6 | 1 (1.8) | 0 | 1 (3.8) | |
| 5/6 + 4/6 | 19 (33.3) | 9 (29.0) | 10 (38.5) | |
| 5/6 + 3/6 | 2 (3.5) | 1 (3.8) | 1 (3.8) | |
| ECOG performance status at transplantation | ||||
| 0 | 22 (31.4) | 13 (31.7) | 9 (31.0) | 0.747 |
| 1 | 41 (58.6) | 23 (56.1) | 18 (62.1) | |
| 2 | 7 (10.0) | 5 (12.2) | 2 (6.9) |
| All N = 70 (%) | AML N = 41 (%) | ALL N = 29 (%) | |
|---|---|---|---|
| Neutrophil engraftment | 55 (78.6) | 32 (78.0) | 23 (79.3) |
| Time to neutrophil engraftment, days (median, range) | 22 (8–74) | 21 (8–64) | 26 (11–74) |
| Platelet recovery | 46 (65.7) | 27 (65.9) | 19 (65.5) |
| Time to platelet recovery, days (median, range) | 41 (15–182) | 39 (15–182) | 46 (20–131) |
| Cumulative incidence of any acute GVHD at Day 100 * | 33.5 | 29.3 | 39.9 |
| Grade II-IV acute GVHD | 24.7 | 26.8 | 21.7 |
| Cumulative incidence of any chronic GVHD at 1 year * | 17.8 | 13.5 | 24.5 |
| Moderate-severe chronic GVHD | 3.2 | 2.5 | 4.4 |
| Any infection | 45 (64.3) | 28 (68.3) | 17 (58.6) |
| Bacterial † | 34 (75.6) | 19 (70.4) | 15 (83.3) |
| Fungal † | 6 (13.3) | 5 (18.5) | 1 (5.6) |
| Viral † | 5 (11.1) | 3 (11.1) | 2 (11.1) |
| CMV antigenemia | 45 (65.2) | 31 (75.6) | 14 (48.3) |
| Pneumonitis | 5 | 4 | 1 |
| Retinitis | 4 | 4 | 0 |
| GI tract infection | 5 | 4 | 1 |
| Cumulative incidence of TRM at Day 100 * | 29.2 | 29.3 | 28.9 |
| Cumulative incidence of TRM at 1 year * | 36.9 | 39.5 | 32.7 |
| Variable | HR (95% CI) | p | ||
|---|---|---|---|---|
| AML, relapse free survival | Year of CBT | 2001–2004 | 1 | |
| 2005–2009 | 0.304 (0.084–1.099) | 0.069 | ||
| 2010–2014 | 0.285 (0.078–1.044) | 0.058 | ||
| 2015–2019 | 0.147 (0.040–0.535) | 0.004 | ||
| GVHD prophylaxis | CNI + ATG | 1 | ||
| CNI + MTX | 0.260 (0.070–0.968) | 0.045 | ||
| CNI + ATG + MTX | 1.147 (0.349–3.773) | 0.822 | ||
| CNI only | 0.647 (0.240–1.747) | 0.391 | ||
| AML, overall survival | Year of CBT | 2001–2004 | 1 | |
| 2005–2009 | 0.325 (0.090–1.168) | 0.085 | ||
| 2010–2014 | 0.226 (0.058–0.874) | 0.031 | ||
| 2015–2019 | 0.151 (0.041–0.556) | 0.004 | ||
| ALL, relapse free survival | Conditioning regimen | Group 1 | 1 | |
| Group 2 | 0.292 (0.053–1.604) | 0.157 | ||
| Group 3 | 0.364 (0.072–1.841) | 0.222 | ||
| Group 4 | 0.150 (0.033–0.678) | 0.014 | ||
| Year of CBT | 2001–2004 | 1 | ||
| 2005–2009 | 0.048 (0.003–0.853) | 0.039 | ||
| 2010–2014 | 0.062 (0.004–1.031) | 0.053 | ||
| 2015–2019 | 0.012 (0.001–0.267) | 0.005 | ||
| GVHD prophylaxis | CNI + ATG | 1 | ||
| CNI + MTX | 0.290 (0.052–1.604) | 0.156 | ||
| CNI + ATG + MTX | 1.107 (0.173–7.068) | 0.914 | ||
| CNI only | 0.150 (0.026–0.873) | 0.035 | ||
| ALL, overall survival | Conditioning regimen | Group 1 | 1 | |
| Group 2 | 0.183 (0.027–1.243) | 0.082 | ||
| Group 3 | 0.398 (0.076–2.069) | 0.273 | ||
| Group 4 | 0.189 (0.042–0.857) | 0.031 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, J.M.; Hong, J.; Oh, D.; Yhim, H.-Y.; Do, Y.R.; Park, J.S.; Jung, C.W.; Yang, D.-H.; Won, J.-H.; Lee, H.G.; et al. Optimizing Preparative Regimen for Umbilical Cord Blood Transplantation in Adult Acute Leukemia Patients: Acute Lymphoblastic Leukemia Requires Myeloablative Conditioning but Not Acute Myeloid Leukemia. J. Clin. Med. 2020, 9, 2310. https://doi.org/10.3390/jcm9072310
Byun JM, Hong J, Oh D, Yhim H-Y, Do YR, Park JS, Jung CW, Yang D-H, Won J-H, Lee HG, et al. Optimizing Preparative Regimen for Umbilical Cord Blood Transplantation in Adult Acute Leukemia Patients: Acute Lymphoblastic Leukemia Requires Myeloablative Conditioning but Not Acute Myeloid Leukemia. Journal of Clinical Medicine. 2020; 9(7):2310. https://doi.org/10.3390/jcm9072310
Chicago/Turabian StyleByun, Ja Min, Junshik Hong, Doyeun Oh, Ho-Young Yhim, Young Rok Do, Joon Seong Park, Chul Won Jung, Deok-Hwan Yang, Jong-Ho Won, Hong Ghi Lee, and et al. 2020. "Optimizing Preparative Regimen for Umbilical Cord Blood Transplantation in Adult Acute Leukemia Patients: Acute Lymphoblastic Leukemia Requires Myeloablative Conditioning but Not Acute Myeloid Leukemia" Journal of Clinical Medicine 9, no. 7: 2310. https://doi.org/10.3390/jcm9072310