Identification of a Clinical Cutoff Value for Multiplex KRASG12/G13 Mutation Detection in Colorectal Adenocarcinoma Patients Using Digital Droplet PCR, and Comparison with Sanger Sequencing and PNA Clamping Assay

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection and DNA Isolation
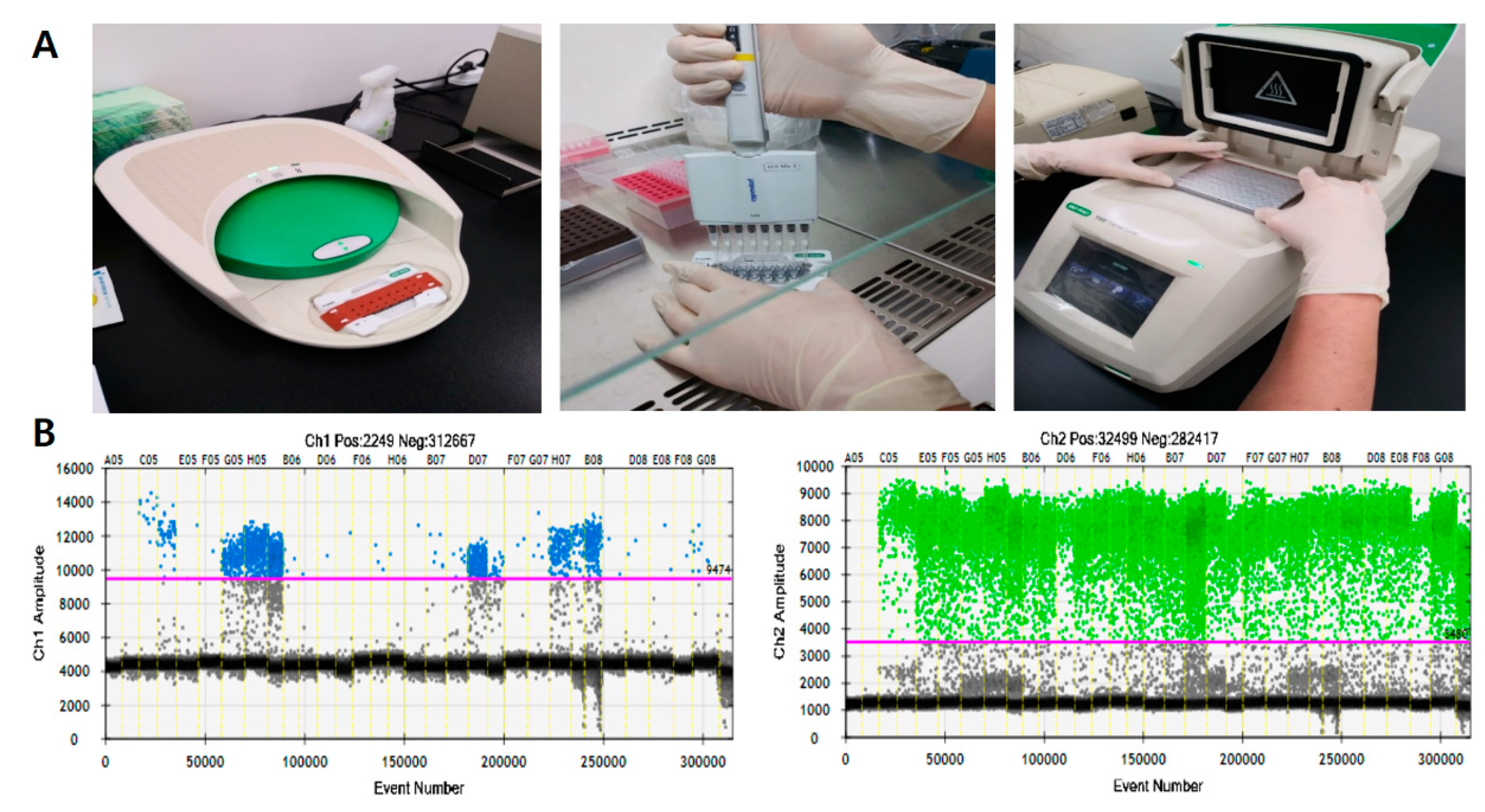
2.2. Droplet Digital Polymerase Chain Reaction (ddPCR)
2.3. Sanger Sequencing
2.4. Peptide Nucleic Acid (PNA)-Clamping Assay (PCR with PNA-Mediated Clamping)
2.5. Statistical Analysis
3. Results
3.1. Detection of KRASG12/G13 Mutation by ddPCR, Sanger Sequencing and PNA Clamping Assay
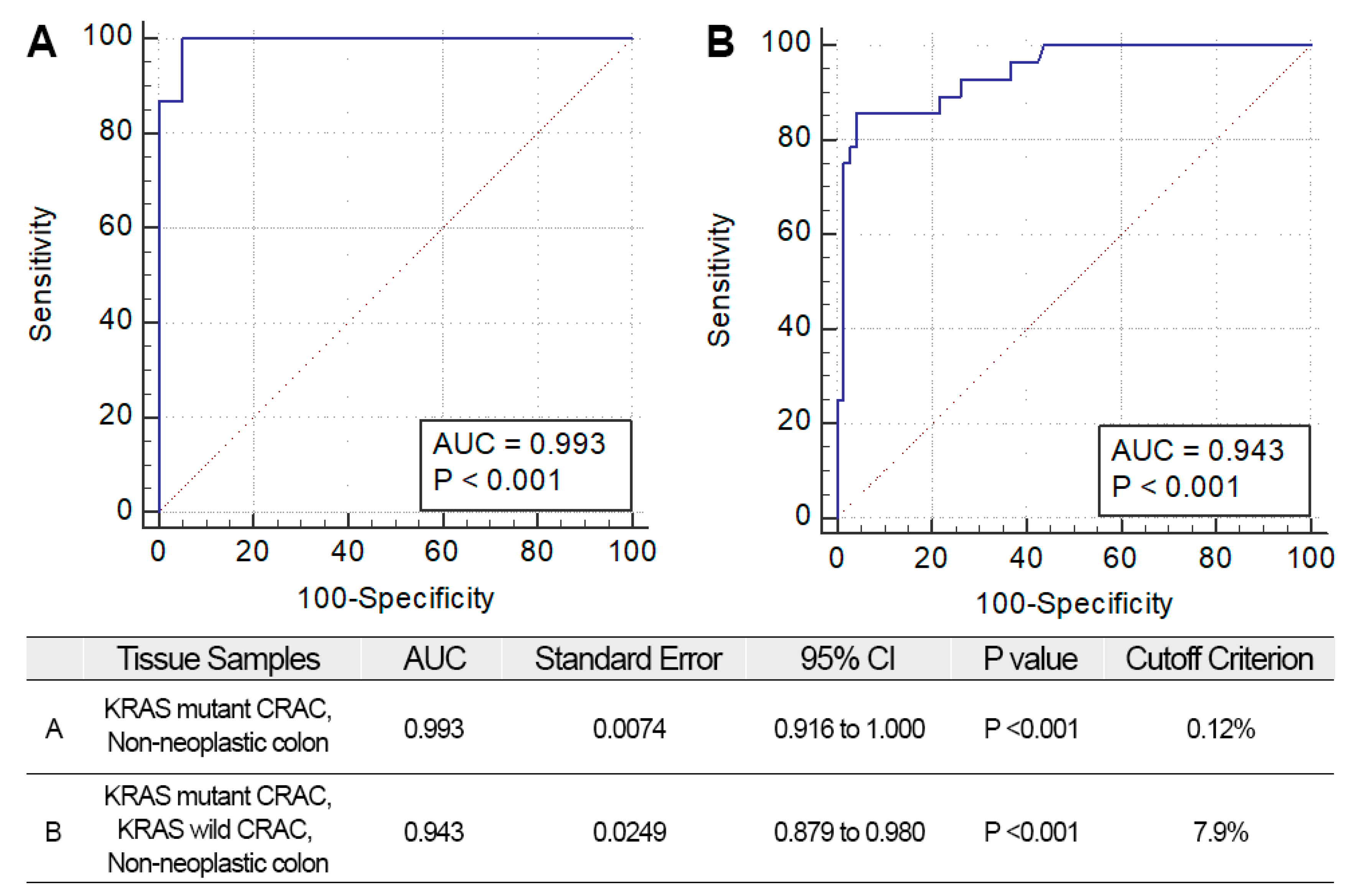
3.2. Receiver Operating Characteristic (ROC) Curves in Determination of KRASG12/G13 Mutation by ddPCR
3.3. Repetitive Measurement of KRASG12/G13 Mutation by ddPCR
3.4. Comparison of KRASG12/G13 Mutation Analysis by ddPCR, Sanger Sequencing, and PNA-Clamping Assay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Malafosse, R.; Penna, C.; Cunha, A.S.; Nordlinger, B. Surgical management of hepatic metastases from colorectal malignancies. Ann. Oncol. 2001, 12, 887–894. [Google Scholar] [CrossRef]
- Alcaide, M.; Cheung, M.; Bushell, K.; Arthur, S.E.; Wong, H.L.; Karasinska, J.; Renouf, D.; Schaeffer, D.F.; McNamara, S.; Tertre, M.C.D.; et al. A Novel Multiplex Droplet Digital PCR Assay to Identify and Quantify KRAS Mutations in Clinical Specimens. J. Mol. Diagn. 2019, 21, 214–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Q.-Y.; Wei, Y.; Chen, J.-W.; Chang, W.-J.; Ye, L.-C.; Zhu, D.-X.; Xu, J.-M. Anti-EGFR and anti-VEGF agents: Important targeted therapies of colorectal liver metastases. World J. Gastroenterol. 2014, 20, 4263–4275. [Google Scholar] [CrossRef]
- Matsunaga, M.; Kaneta, T.; Miwa, K.; Ichikawa, W.; Fujita, K.-I.; Nagashima, F.; Furuse, J.; Kage, M.; Akagi, Y.; Sasaki, Y. A comparison of four methods for detecting KRAS mutations in formalin-fixed specimens from metastatic colorectal cancer patients. Oncol. Lett. 2016, 12, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Rakhit, C.; Ottolini, B.; Jones, C.; Pringle, J.; Shaw, J.; Martins, L.M. Peptide nucleic acid clamping to improve the sensitivity of Ion Torrent-based detection of an oncogenic mutation in KRAS. Matters 2017, 3, e201706000001. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S.; Kim, W.H.; Kwak, Y.; Koh, J.; Bae, J.M.; Kim, K.-M.; Chang, M.S.; Han, H.S.; Kim, J.M.; Kim, H.W. Molecular testing for gastrointestinal cancer. J. Pathol. Transl. Med. 2017, 51, 103–121. [Google Scholar] [CrossRef] [Green Version]
- Miotke, L.; Lau, B.T.; Rumma, R.T.; Ji, H.P. High sensitivity detection and quantitation of DNA copy number and single nucleotide variants with single color droplet digital PCR. Anal. Chem. 2014, 86, 2618–2624. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Williams, J.; Gartner, K.; Phillips, R.; Hurst, J.; Frater, J. Low copy target detection by Droplet Digital PCR through application of a novel open access bioinformatic pipeline, ‘definetherain’. J. Virol. Methods 2014, 202, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Trypsteen, W.; Vynck, M.; De Neve, J.; Bonczkowski, P.; Kiselinova, M.; Malatinkova, E.; Vervisch, K.; Thas, O.; Vandekerckhove, L.; De Spiegelaere, W. ddpcRquant: Threshold determination for single channel droplet digital PCR experiments. Anal. Bioanal. Chem. 2015, 407, 5827–5834. [Google Scholar] [CrossRef] [PubMed]
- Hughesman, C.B.; Lu, X.J.D.; Liu, K.Y.P.; Zhu, Y.; Poh, C.F.; Haynes, C. A Robust Protocol for Using Multiplexed Droplet Digital PCR to Quantify Somatic Copy Number Alterations in Clinical Tissue Specimens. PLoS ONE 2016, 11, e0161274. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Wang, S.; Fu, B.; Wang, J. Evaluation of droplet digital PCR and next generation sequencing for characterizing DNA reference material for KRAS mutation detection. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanova, B.; Kalman, M.; Jasek, K.; Kasubova, I.; Burjanivova, T.; Farkasova, A.; Kruzliak, P.; Busselberg, D.; Plank, L.; Lasabova, Z. Droplet digital PCR revealed high concordance between primary tumors and lymph node metastases in multiplex screening of KRAS mutations in colorectal cancer. Clin. Exp. Med. 2019, 19, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Laurent-Puig, P.; Pekin, D.; Normand, C.; Kotsopoulos, S.K.; Nizard, P.; Perez-Toralla, K.; Rowell, R.; Olson, J.; Srinivasan, P.; Le Corre, D.; et al. Clinical relevance of KRAS-mutated subclones detected with picodroplet digital PCR in advanced colorectal cancer treated with anti-EGFR therapy. Clin. Cancer Res. 2015, 21, 1087–1097. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Shelton, D.N.; Berman, J.R.; Zhang, B.; Cooper, S.; Tzonev, S.; Hefner, E.; Regan, J.F. Droplet digital™ PCR: Multiplex detection of KRAS mutations in formalin-fixed, paraffin-embedded colorectal cancer samples. Biotechniques 2015, 58, 205–206. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, L.B.; Coleman, V.A.; Hindson, C.M.; Herrmann, J.; Hindson, B.J.; Bhat, S.; Emslie, K.R. Evaluation of a droplet digital polymerase chain reaction format for DNA copy number quantification. Anal. Chem. 2012, 84, 1003–1011. [Google Scholar] [CrossRef]
- Gerdes, L.; Iwobi, A.; Busch, U.; Pecoraro, S. Optimization of digital droplet polymerase chain reaction for quantification of genetically modified organisms. Biomol. Detect. Quantif. 2016, 7, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.C.; Laperriere, G.; Germain, H. Droplet Digital PCR versus qPCR for gene expression analysis with low abundant targets: From variable nonsense to publication quality data. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Messa, F.; Tonissi, F.; Millo, E.; Bracco, E.; Ungari, S.; Lattanzio, L.; Merlano, M.; Damonte, G.; Lo Nigro, C. A PNA-mediated clamping PCR for routine detection of KRAS mutations in colorectal carcinoma. Int. J. Biol. Markers 2014, 29, e55–e61. [Google Scholar] [CrossRef]
- Dinu, D.; Dobre, M.; Panaitescu, E.; Bîrlă, R.; Iosif, C.; Hoara, P.; Caragui, A.; Boeriu, M.; Constantinoiu, S.; Ardeleanu, C. Prognostic significance of KRAS gene mutations in colorectal cancer-preliminary study. J. Med. Life 2014, 7, 581–587. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| KRAS Mutant CRAC & Non-Neoplastic Colon (0.12% Cutoff) | KRAS Mutant and KRAS Wild CRAC & Non-Neoplastic Colon (7.9% Cutoff) | |
|---|---|---|
| Sensitivity | 100.0% (89.11–100.00) | 84.38% (67.21–94.72) |
| Specificity | 30.61% (18.25–45.42) | 97.96% (89.15–99.95) |
| PPV | 48.48% (43.87–53.13) | 96.43% (79.42–99.47) |
| NPV | 100.0% (100.00–100.00) | 90.57% (81.09–97.23) |
| Sample ID | First KRAS ddPCR | Second KRAS ddPCR | Third KRAS ddPCR | Mean KRAS ddPCR | ||||
|---|---|---|---|---|---|---|---|---|
| MAF | MAF | MAF | MAF | |||||
| T1 | 0 | Wild-type | 0 | Wild-type | 0 | Wild-type | 0 | Wild-type |
| T2 | 0 | Wild-type | 0.07 | Wild-type | 0 | Wild-type | 0.02 | Wild-type |
| T3 | 0.05 | Wild-type | 0 | Wild-type | 0 | Wild-type | 0.02 | Wild-type |
| T4 | 0.05 | Wild-type | 0 | Wild-type | 0 | Wild-type | 0.02 | Wild-type |
| T5 | 0.04 | Wild-type | 0 | Wild-type | 0.04 | Wild-type | 0.03 | Wild-type |
| T6 | 0 | Wild-type | 0 | Wild-type | 0.11 | Wild-type | 0.04 | Wild-type |
| T7 | 0.04 | Wild-type | 0.04 | Wild-type | 0.09 | Wild-type | 0.05 | Wild-type |
| T8 | 0 | Wild-type | 0.19 | Wild-type | 0 | Wild-type | 0.06 | Wild-type |
| T9 | 0.08 | Wild-type | 0.13 | Wild-type | 0 | Wild-type | 0.07 | Wild-type |
| T10 | 0 | Wild-type | 0.14 | Wild-type | 0.1 | Wild-type | 0.08 | Wild-type |
| T11 | 0.09 | Wild-type | 0.09 | Wild-type | 0.07 | Wild-type | 0.09 | Wild-type |
| T12 | 0 | Wild-type | 0.15 | Wild-type | 0.11 | Wild-type | 0.09 | Wild-type |
| T13 | 0.1 | Wild-type | 0.07 | Wild-type | 0.1 | Wild-type | 0.09 | Wild-type |
| T14 | 0 | Wild-type | 0.13 | Wild-type | 0.19 | Wild-type | 0.11 | Wild-type |
| T15 | 0 | Wild-type | 0.08 | Wild-type | 0.26 | Wild-type | 0.11 | Wild-type |
| T16 | 0.11 | Wild-type | 0.27 | Wild-type | 0 | Wild-type | 0.12 | Wild-type |
| T17 | 0 | Wild-type | 0.2 | Wild-type | 0.2 | Wild-type | 0.13 | Wild-type |
| T18 | 0.02 | Wild-type | 0.15 | Wild-type | 0.27 | Wild-type | 0.15 | Wild-type |
| T19 | 0.21 | Wild-type | 0.12 | Wild-type | 0.17 | Wild-type | 0.16 | Wild-type |
| T20 | 0 | Wild-type | 0.13 | Wild-type | 0.36 | Wild-type | 0.16 | Wild-type |
| T21 | 0.11 | Wild-type | 0.11 | Wild-type | 0.25 | Wild-type | 0.16 | Wild-type |
| T22 | 0.09 | Wild-type | 0 | Wild-type | 0.4 | Wild-type | 0.16 | Wild-type |
| T23 | 0 | Wild-type | 0.16 | Wild-type | 0.36 | Wild-type | 0.17 | Wild-type |
| T24 | 0.07 | Wild-type | 0.11 | Wild-type | 0.33 | Wild-type | 0.17 | Wild-type |
| T25 | 0 | Wild-type | 0.28 | Wild-type | 0.3 | Wild-type | 0.19 | Wild-type |
| T26 | 0 | Wild-type | 0.46 | Wild-type | 0.12 | Wild-type | 0.19 | Wild-type |
| T27 | 0.19 | Wild-type | 0.23 | Wild-type | 0.24 | Wild-type | 0.22 | Wild-type |
| T28 | 0 | Wild-type | 0.48 | Wild-type | 0.26 | Wild-type | 0.25 | Wild-type |
| T29 | 0.3 | Wild-type | 0.16 | Wild-type | 0.31 | Wild-type | 0.26 | Wild-type |
| T30 | 0.28 | Wild-type | 0.19 | Wild-type | 0.41 | Wild-type | 0.29 | Wild-type |
| T31 | 0.26 | Wild-type | 0.09 | Wild-type | 0.54 | Wild-type | 0.3 | Wild-type |
| T32 | 0.06 | Wild-type | 0.53 | Wild-type | 0.3 | Wild-type | 0.3 | Wild-type |
| T33 | 0 | Wild-type | 0.49 | Wild-type | 0.45 | Wild-type | 0.31 | Wild-type |
| T34 | 0.34 | Wild-type | 0.23 | Wild-type | 0.39 | Wild-type | 0.32 | Wild-type |
| T35 | 0.06 | Wild-type | 0.44 | Wild-type | 0.5 | Wild-type | 0.33 | Wild-type |
| T36 | 0.07 | Wild-type | 0.12 | Wild-type | 0.79 | Wild-type | 0.33 | Wild-type |
| T37 | 0.14 | Wild-type | 0.37 | Wild-type | 0.47 | Wild-type | 0.33 | Wild-type |
| T38 | 0.04 | Wild-type | 0.55 | Wild-type | 0.58 | Wild-type | 0.39 | Wild-type |
| T39 | 0 | Wild-type | 0.75 | Wild-type | 0.51 | Wild-type | 0.42 | Wild-type |
| T40 | 0.27 | Wild-type | 0.4 | Wild-type | 0.76 | Wild-type | 0.48 | Wild-type |
| T41 | 0 | Wild-type | 0.73 | Wild-type | 0.71 | Wild-type | 0.48 | Wild-type |
| T42 | 0.22 | Wild-type | 0 | Wild-type | 1.4 | Wild-type | 0.54 | Wild-type |
| T43 | 0.21 | Wild-type | 0.6 | Wild-type | 0.85 | Wild-type | 0.55 | Wild-type |
| T44 | 0.7 | Wild-type | 1.08 | Wild-type | 0.69 | Wild-type | 0.82 | Wild-type |
| T45 | 2.65 | Wild-type | 0 | Wild-type | 0 | Wild-type | 0.88 | Wild-type |
| T46 | 0.97 | Wild-type | 0.8 | Wild-type | 0.97 | Wild-type | 0.91 | Wild-type |
| T47 | 0.52 | Wild-type | 1.38 | Wild-type | 1.23 | Wild-type | 1.04 | Wild-type |
| T48 | 3.69 | Wild-type | 1 | Wild-type | 0.66 | Wild-type | 1.78 | Wild-type |
| T49 | 5.76 | Wild-type | 0.49 | Wild-type | 0.16 | Wild-type | 2.14 | Wild-type |
| T50 | 5.79 | Wild-type | 1.04 | Wild-type | 0.42 | Wild-type | 2.42 | Wild-type |
| T51 | 7.42 | Wild-type | 1.56 | Wild-type | 3.01 | Wild-type | 4 | Wild-type |
| * T52 | 2.17 | Wild-type | 5.62 | Wild-type | 8.65 | Mutant | 5.48 | Wild-type |
| * T53 | 3.61 | Wild-type | 9.11 | Mutant | 9.87 | Mutant | 7.53 | Wild-type |
| * T54 | 5.48 | Wild-type | 7.74 | Wild-type | 10.49 | Mutant | 7.9 | Mutant |
| T55 | 13.94 | Mutant | 15.08 | Mutant | 13.29 | Mutant | 14.1 | Mutant |
| * T56 | 0.75 | Wild-type | 22.36 | Mutant | 22.88 | Mutant | 15.33 | Mutant |
| T57 | 10.48 | Mutant | 17.56 | Mutant | 18.47 | Mutant | 15.51 | Mutant |
| * T58 | 4.71 | Wild-type | 22.75 | Mutant | 21.34 | Mutant | 16.27 | Mutant |
| T59 | 13.39 | Mutant | 20.33 | Mutant | 20.88 | Mutant | 18.2 | Mutant |
| T60 | 16.62 | Mutant | 18.76 | Mutant | 21.23 | Mutant | 18.87 | Mutant |
| T61 | 16.58 | Mutant | 17.12 | Mutant | 24.37 | Mutant | 19.36 | Mutant |
| T62 | 15.04 | Mutant | 21.44 | Mutant | 22.65 | Mutant | 19.71 | Mutant |
| T63 | 10.82 | Mutant | 24.39 | Mutant | 28.47 | Mutant | 21.23 | Mutant |
| T64 | 9.23 | Mutant | 26.74 | Mutant | 28 | Mutant | 21.32 | Mutant |
| * T65 | 2.04 | Wild-type | 29.01 | Mutant | 38.62 | Mutant | 23.22 | Mutant |
| T66 | 15.63 | Mutant | 27.81 | Mutant | 29.46 | Mutant | 24.3 | Mutant |
| T67 | 27.78 | Mutant | 23.06 | Mutant | 23.44 | Mutant | 24.76 | Mutant |
| T68 | 24.88 | Mutant | 30.54 | Mutant | 31.24 | Mutant | 28.89 | Mutant |
| T69 | 25 | Mutant | 32.61 | Mutant | 31.67 | Mutant | 29.76 | Mutant |
| T70 | 9.47 | Mutant | 46.99 | Mutant | 50.34 | Mutant | 35.6 | Mutant |
| T71 | 34.96 | Mutant | 34.48 | Mutant | 38.13 | Mutant | 35.85 | Mutant |
| T72 | 20.1 | Mutant | 42.43 | Mutant | 45.5 | Mutant | 36.01 | Mutant |
| T73 | 38.23 | Mutant | 32.7 | Mutant | 38.13 | Mutant | 36.36 | Mutant |
| T74 | 36.08 | Mutant | 40.95 | Mutant | 43.71 | Mutant | 40.25 | Mutant |
| * T75 | 4.29 | Wild-type | 55.56 | Mutant | 60.95 | Mutant | 40.27 | Mutant |
| T76 | 30.18 | Mutant | 50.53 | Mutant | 49.34 | Mutant | 43.35 | Mutant |
| T77 | 41.87 | Mutant | 42.24 | Mutant | 46.7 | Mutant | 43.6 | Mutant |
| T78 | 41.14 | Mutant | 44.78 | Mutant | 48.95 | Mutant | 44.96 | Mutant |
| T79 | 60.77 | Mutant | 45.28 | Mutant | 49.33 | Mutant | 51.79 | Mutant |
| T80 | 53.88 | Mutant | 60.45 | Mutant | 58.23 | Mutant | 57.52 | Mutant |
| T81 | 83.77 | Mutant | 78.03 | Mutant | 81.71 | Mutant | 81.17 | Mutant |
| First ddPCR | Second ddPCR | Third ddPCR | Mean ddPCR | |
|---|---|---|---|---|
| Sensitivity | 71.88% | 84.38% | 84.38% | 84.38% |
| Specificity | 100% | 97.96% | 93.88% | 97.96% |
| PPV | 100% | 96.43% | 90.00% | 96.43% |
| NPV | 84.48% | 90.57% | 90.20% | 90.57% |
| Sample ID | KRAS ddPCR | KRAS ddPCR | KRAS Sanger | KRAS PNA |
|---|---|---|---|---|
| MAF | Cutoff Result | Sequencing | Clamping Assay | |
| T1 | 0.00 | Wild-type | Wild-type | Wild-type |
| T2 | 0.02 | Wild-type | Wild-type | Wild-type |
| T3 | 0.02 | Wild-type | Wild-type | Wild-type |
| T4 | 0.02 | Wild-type | Wild-type | Wild-type |
| T5 | 0.03 | Wild-type | Wild-type | Wild-type |
| T6 | 0.04 | Wild-type | Wild-type | Wild-type |
| T7 | 0.05 | Wild-type | Wild-type | Wild-type |
| T8 | 0.06 | Wild-type | Wild-type | Wild-type |
| T9 | 0.07 | Wild-type | Wild-type | Wild-type |
| T10 | 0.08 | Wild-type | Wild-type | Wild-type |
| T11 | 0.09 | Wild-type | Wild-type | Wild-type |
| T12 | 0.09 | Wild-type | Wild-type | Wild-type |
| T13 | 0.09 | Wild-type | Wild-type | Wild-type |
| T14 | 0.11 | Wild-type | Wild-type | Wild-type |
| * T15 | 0.11 | Wild-type | Wild-type | * Mutant |
| T16 | 0.12 | Wild-type | Wild-type | Wild-type |
| T17 | 0.13 | Wild-type | Wild-type | Wild-type |
| T18 | 0.15 | Wild-type | Wild-type | Wild-type |
| T19 | 0.16 | Wild-type | Wild-type | Wild-type |
| T20 | 0.16 | Wild-type | Wild-type | Wild-type |
| T21 | 0.16 | Wild-type | Wild-type | Wild-type |
| T22 | 0.16 | Wild-type | Wild-type | Wild-type |
| * T23 | 0.17 | Wild-type | * Mutant | Wild-type |
| T24 | 0.17 | Wild-type | Wild-type | Wild-type |
| T25 | 0.19 | Wild-type | Wild-type | Wild-type |
| T26 | 0.19 | Wild-type | Wild-type | Wild-type |
| T27 | 0.22 | Wild-type | Wild-type | Wild-type |
| T28 | 0.25 | Wild-type | Wild-type | Wild-type |
| * T29 | 0.26 | Wild-type | * Mutant | Wild-type |
| T30 | 0.29 | Wild-type | Wild-type | Wild-type |
| T31 | 0.3 | Wild-type | Wild-type | Wild-type |
| T32 | 0.3 | Wild-type | Wild-type | Wild-type |
| T33 | 0.31 | Wild-type | Wild-type | Wild-type |
| T34 | 0.32 | Wild-type | Wild-type | Wild-type |
| T35 | 0.33 | Wild-type | Wild-type | Wild-type |
| T36 | 0.33 | Wild-type | Wild-type | Wild-type |
| T37 | 0.33 | Wild-type | Wild-type | Wild-type |
| * T38 | 0.39 | Wild-type | * Mutant | Wild-type |
| T39 | 0.42 | Wild-type | Wild-type | Wild-type |
| T40 | 0.48 | Wild-type | Wild-type | Wild-type |
| T41 | 0.48 | Wild-type | Wild-type | Wild-type |
| * T42 | 0.54 | Wild-type | * Mutant | Wild-type |
| T43 | 0.55 | Wild-type | Wild-type | Wild-type |
| T44 | 0.82 | Wild-type | Wild-type | Wild-type |
| T45 | 0.88 | Wild-type | Wild-type | Wild-type |
| T46 | 0.91 | Wild-type | Wild-type | Wild-type |
| * T47 | 1.04 | Wild-type | Wild-type | * Mutant |
| * T48 | 1.78 | Wild-type | * Mutant | Wild-type |
| * T49 | 2.14 | Wild-type | Wild-type | * Mutant |
| * T50 | 2.42 | Wild-type | Wild-type | * Mutant |
| * T51 | 4.00 | Wild-type | Wild-type | * Mutant |
| * T52 | 5.48 | Wild-type | Wild-type | * Mutant |
| * T53 | 7.53 | Wild-type | Wild-type | * Mutant |
| * T54 | 7.90 | Mutant | * Wild-type | Mutant |
| T55 | 14.1 | Mutant | Mutant | Mutant |
| T56 | 15.33 | Mutant | Mutant | Mutant |
| T57 | 15.51 | Mutant | Mutant | Mutant |
| T58 | 16.27 | Mutant | Mutant | Mutant |
| * T59 | 18.20 | Mutant | Mutant | * Wild-type |
| T60 | 18.87 | Mutant | Mutant | Mutant |
| * T61 | 19.36 | Mutant | Mutant | * Wild-type |
| T62 | 19.71 | Mutant | Mutant | Mutant |
| T63 | 21.23 | Mutant | Mutant | Mutant |
| T64 | 21.32 | Mutant | Mutant | Mutant |
| T65 | 23.22 | Mutant | Mutant | Mutant |
| T66 | 24.30 | Mutant | Mutant | Mutant |
| T67 | 24.76 | Mutant | Mutant | Mutant |
| T68 | 28.89 | Mutant | Mutant | Mutant |
| T69 | 29.76 | Mutant | Mutant | Mutant |
| T70 | 35.60 | Mutant | Mutant | Mutant |
| T71 | 35.85 | Mutant | Mutant | Mutant |
| T72 | 36.01 | Mutant | Mutant | Mutant |
| T73 | 36.36 | Mutant | Mutant | Mutant |
| T74 | 40.25 | Mutant | Mutant | Mutant |
| T75 | 40.27 | Mutant | Mutant | Mutant |
| T76 | 43.35 | Mutant | Mutant | Mutant |
| T77 | 43.60 | Mutant | Mutant | Mutant |
| T78 | 44.96 | Mutant | Mutant | Mutant |
| T79 | 51.79 | Mutant | Mutant | Mutant |
| T80 | 57.52 | Mutant | Mutant | Mutant |
| T81 | 81.17 | Mutant | Mutant | Mutant |
| Detection of KRAG12/13 Mutation | |||
|---|---|---|---|
| ddPCR | Sanger Sequencing | PNA-Clamping Assay | |
| Sensitivity | 100% | 96.43% | 92.86% |
| Specificity | 100% | 90.57% | 86.79% |
| PPV | 100% | 84.38% | 78.79% |
| NPV | 100% | 97.96% | 95.83% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.H.; Lee, T.H.; Choi, M.K.; Kwon, I.S.; Bae, G.E.; Yeo, M.-K. Identification of a Clinical Cutoff Value for Multiplex KRASG12/G13 Mutation Detection in Colorectal Adenocarcinoma Patients Using Digital Droplet PCR, and Comparison with Sanger Sequencing and PNA Clamping Assay. J. Clin. Med. 2020, 9, 2283. https://doi.org/10.3390/jcm9072283
Lee KH, Lee TH, Choi MK, Kwon IS, Bae GE, Yeo M-K. Identification of a Clinical Cutoff Value for Multiplex KRASG12/G13 Mutation Detection in Colorectal Adenocarcinoma Patients Using Digital Droplet PCR, and Comparison with Sanger Sequencing and PNA Clamping Assay. Journal of Clinical Medicine. 2020; 9(7):2283. https://doi.org/10.3390/jcm9072283
Chicago/Turabian StyleLee, Kyung Ha, Tae Hee Lee, Min Kyung Choi, In Sun Kwon, Go Eun Bae, and Min-Kyung Yeo. 2020. "Identification of a Clinical Cutoff Value for Multiplex KRASG12/G13 Mutation Detection in Colorectal Adenocarcinoma Patients Using Digital Droplet PCR, and Comparison with Sanger Sequencing and PNA Clamping Assay" Journal of Clinical Medicine 9, no. 7: 2283. https://doi.org/10.3390/jcm9072283