The Efficacy of Rotary, Reciprocating, and Combined Non-Surgical Endodontic Retreatment Techniques in Removing a Carrier-Based Root Canal Filling Material from Straight Root Canal Systems: A Micro-Computed Tomography Analysis

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Experimental Procedure
2.3. Micro-CT Scanning Procedures and Evaluation
2.4. Measurement Procedure
2.5. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siqueira, J.F., Jr.; Rôças, I.N. Polymerase chain reaction–based analysis of microorganisms associated with failed endodontic treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2014, 97, 85–94. [Google Scholar] [CrossRef]
- Kielbassa, A.M.; Frank, W.; Madaus, T. Radiologic assessment of quality of root canal fillings and periapical status in an Austrian subpopulation—An observational study. PLoS ONE 2017, 12, e0176724. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torabinejad, M.; Corr, R.; Handysides, R.; Shabahang, S. Outcomes of nonsurgical retreatment and endodontic surgery: A systematic review. J. Endod. 2009, 35, 930–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulsmann, M.; Stotz, S. Efficacy, cleaning ability and safety of different devices for gutta-percha removal in root canal retreatment. Int. Endod. J. 1997, 30, 227–233. [Google Scholar] [CrossRef]
- Silva, E.J.; Orlowsky, N.B.; Herrera, D.R.; Machado, R.; Krebs, R.L.; Coutinho-Filho, T.D.S. Effectiveness of rotatory and reciprocating movements in root canal filling material removal. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodig, T.; Reicherts, P.; Konietschke, F.; Dullin, C.; Hahn, W.; Hülsmann, M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int. Endod. J. 2014, 47, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Zamin, C.; Silva-Sousa, Y.T.C.; Souza-Gabriel, A.E.; Messias, D.F.; Sousa-Neto, M.D. Fracture susceptibility of endodontically treated teeth. Dent. Traumatol. 2012, 28, 282–286. [Google Scholar] [CrossRef]
- Alghamdi, F.; Alhaddad, A.J.; Abuzinadah, S. Healing of Periapical Lesions After Surgical Endodontic Retreatment: A Systematic Review. Cureus 2020, 12, e6916. [Google Scholar] [CrossRef] [Green Version]
- Zandi, H.; Petronijevic, N.; Mdala, I.; Kristoffersen, A.K.; Enersen, M.; Rôças, I.N.; Siqueira, J.F., Jr.; Ørstavik, D. Outcome of Endodontic Retreatment Using 2 Root Canal Irrigants and Influence of Infection on Healing as Determined by a Molecular Method: A Randomized Clinical Trial. J. Endod. 2019, 45, 1089–1098. [Google Scholar] [CrossRef]
- Kirsch, J.; Basche, S.; Neunzehn, J.; Dede, M.; Dannemann, M.; Hannig, C.; Weber, M.T. Is it really penetration? Locomotion of devitalized Enterococcus faecalis cells within dentinal tubules of bovine teeth. Arch. Oral Biol. 2017, 83, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Love, R.M. Enterococcus faecalis—A mechanism for its role in endodontic failure. Int. Endod. J. 2001, 34, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr. Endodontic infections: Concepts, paradigms, and perspectives. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Marques da Silva, B.; Baratto-Filho, F.; Leonardi, D.P.; Henrique Borges, A.; Volpato, L.; Branco Barletta, F. Effectiveness of ProTaper, D-RaCe, and Mtwo retreatment files with and without supplementary instruments in the removal of root canal filling material. Int. Endod. J. 2012, 45, 927–932. [Google Scholar] [CrossRef]
- Khalighinejad, N.; Aminoshariae, A.; Kulild, J.C.; Williams, K.A.; Wang, J.; Mickel, A. The effect of the dental operating microscope on the outcome of nonsurgical root canal treatment: A retrospective case-control study. J. Endod. 2017, 43, 728–732. [Google Scholar] [CrossRef]
- Kikly, A.; Jaâfoura, S.; Kammoun, D.; Sahtout, S. Sealing Ability of Endodontic Cements: An In Vitro Study. Int. J. Dent. 2020, 2020, 5862598. [Google Scholar] [CrossRef] [Green Version]
- Akhavan, H.; Azdadi, Y.K.; Azimi, S.; Dadresanfar, B.; Ahmadi, A. Comparing the efficacy of Mtwo and D-RaCe retreatment systems in removing residual gutta-percha and sealer in the root canal. Iran. Endod. J. 2012, 7, 122–126. [Google Scholar]
- Barletta, F.B.; Rahde, N.d.M.R.; Limongi, O.; Moura, A.A.M.; Zanesco, C.; Mazocatto, G. In vitro comparative analysis of 2 mechanical techniques for removing gutta-percha during retreatment. J. Can. Dent. Assoc. 2007, 73, 65. [Google Scholar]
- Versiani, M.A.; Ordinola-Zapata, R.; Keleş, A.; Alcin, H.; Bramante, C.M.; Pécora, J.D.; Sousa-Neto, M.D. Middle canals in mandibular first molars: A micro CT study in different populations. Arch. Oral Biol. 2016, 61, 130–137. [Google Scholar] [CrossRef]
- Monquilhott Crozeta, B.; Silva-Sousa, Y.T.; Leoni, G.B.; Mazzi-Chaves, J.F.; Fantinato, T.; Baratto-Filho, F.; Sousa-Neto, M.D. Micro-computed tomography study of filling material removal from oval-shaped canals by using rotary, reciprocating, and adaptative motion systems. J. Endod. 2016, 42, 793–797. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Faus-Matoses, V.; Pasarín-Linares, C.; Faus-Matoses, I.; Foschi, F.; Sauro, S.; Faus-Llácer, V.J. Comparison of Obturation Removal Efficiency from Straight Root Canals with ProTaper Gold or Reciproc Blue: A Micro-Computed Tomography Study. J. Clin. Med. 2020, 9, 1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bago, I.; Suk, M.; Katić, M.; Gabrić, D.; Anić, I. Comparison of the effectiveness of various rotary and reciprocating systems with different surface treatments to remove gutta-percha and an epoxy resin-based sealer from straight root canals. Int. Endod. J. 2019, 52, 105–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colaco, A.S.; Pai, V.A.R. Comparative evaluation of the efficiency of manual and rotary gutta-percha removal techniques. J. Endod. 2015, 41, 1871–1874. [Google Scholar] [CrossRef]
- Alves, F.R.; Marceliano-Alves, M.F.; Sousa, J.C.; Silveira, S.B.; Provenzano, J.C.; Siqueira, J.F., Jr. Removal of root canal fillings in curved canals using either reciprocating single- or rotary multi-instrument systems and a supplementary step with the XP-Endo Finisher. J. Endod. 2016, 42, 1114–1119. [Google Scholar] [CrossRef]
- Bernardes, R.A.; Duarte, M.A.; Vivian, R.R.; Alcalde, M.P.; Vasconcelos, B.C.; Bramante, C.M. Comparison of three retreatment techniques with ultrasonic activation in flattened canals using micro-computed tomography and scanning electron microscopy. Int. Endod. J. 2015, 49, 890–897. [Google Scholar] [CrossRef]
- Zuolo, A.S.; Mello, J.E., Jr.; Cunha, R.S.; Zuolo, M.L.; Bueno, C.E.S. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. Int. Endod. J. 2013, 46, 947–953. [Google Scholar] [CrossRef]
- Hammad, M.; Qualtrough, A.; Silikas, N. Three-dimensional evaluation of effectiveness of hand and rotary instrumentation for retreatment of canals filled with different materials. J. Endod. 2008, 34, 1370–1373. [Google Scholar] [CrossRef]
- Betti, L.V.; Bramante, C.M.; Quantec, S.C. Rotary instruments versus hand files for guttapercha removal in root canal retreatment. Int. Endod. J. 2001, 34, 514–519. [Google Scholar] [CrossRef]
- Roggendorf, M.J.; Legner, M.; Ebert, J.; Fillery, E.; Frankenberger, R.; Friedman, S. Micro-CT evaluation of residual material in canals filled with Activ GP or GuttaFlow following removal with NiTi instruments. Int. Endod. J. 2010, 43, 200–209. [Google Scholar] [CrossRef]
- Gambarini, G.; Piasecki, L.; Schianchi, G.; Di Nardo, D.; Miccoli, G.; Al Sudani, D.; Di Giorgio, R.; Testarelli, L. In vitro evaluation of carrier based obturation technique: A CBCT study. Ann. Stomatol. (Roma) 2016, 7, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Helvacioglu-Yigit, D.; Yilmaz, A.; Kiziltas-Sendur, G.; Aslan, O.S.; Abbott, P.V. Efficacy of reciprocating and rotary systems for removing root filling material: A micro-computed tomography study. Scanning 2014, 36, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.S.; Ling, J.Q.; Wei, X.; Huang, X.Y. Efficacy of ProTaper Universal rotary retreatment system for gutta-percha removal from root canals. Int. Endod. J. 2008, 41, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Berutti, E.; Chiandussi, G.; Paolino, D.S.; Scotti, N.; Cantatore, G.; Castellucci, A.; Pasqualini, D. Effect of canal length and curvature on working length alteration with WaveOne reciprocating files. J. Endod. 2011, 37, 1687–1690. [Google Scholar] [CrossRef] [Green Version]
- Franco, V.; Fabiani, C.; Taschieri, S.; Malentacca, A.; Bortolin, M.; Del Fabbro, M. Investigation on the shaping ability of nickel- titanium files when used with a reciprocating motion. J. Endod. 2011, 37, 1398–1401. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
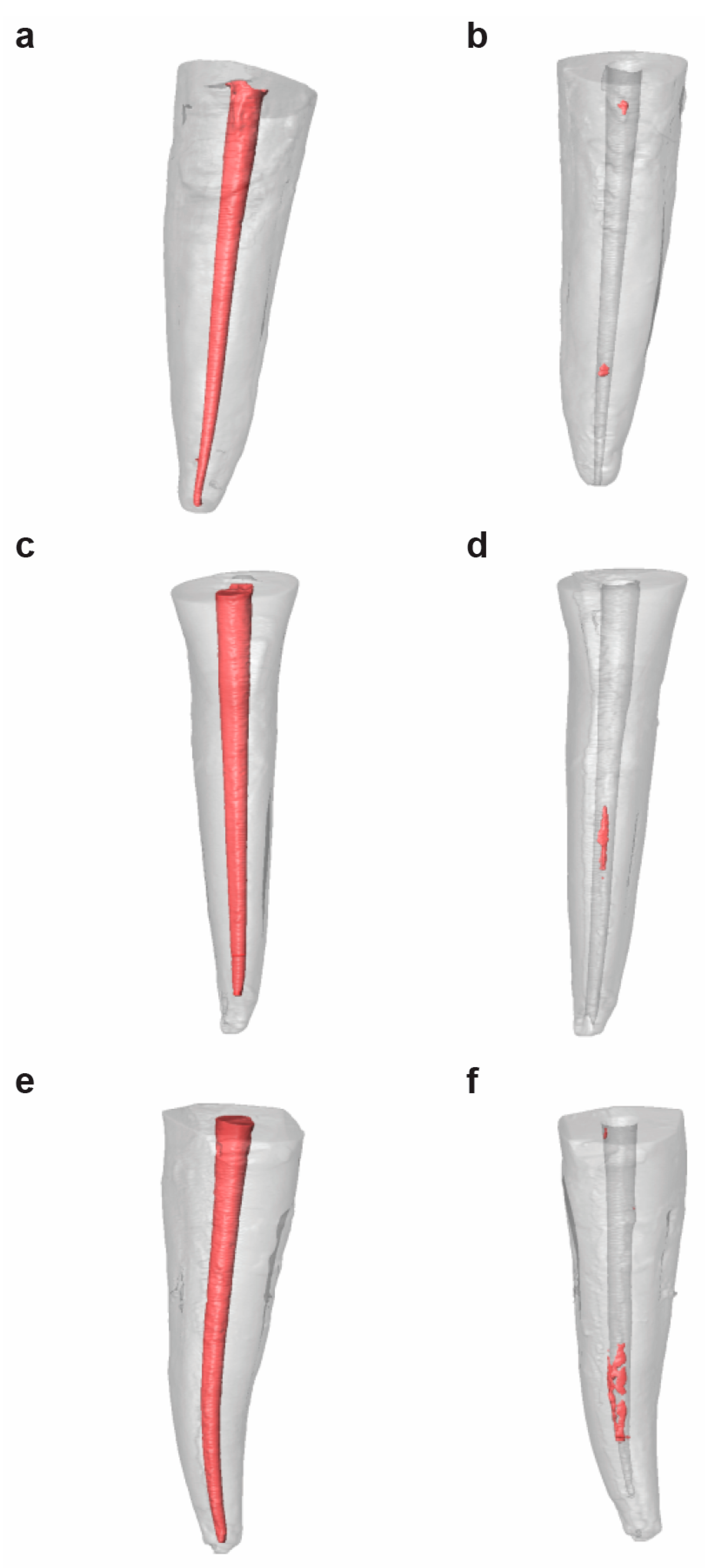
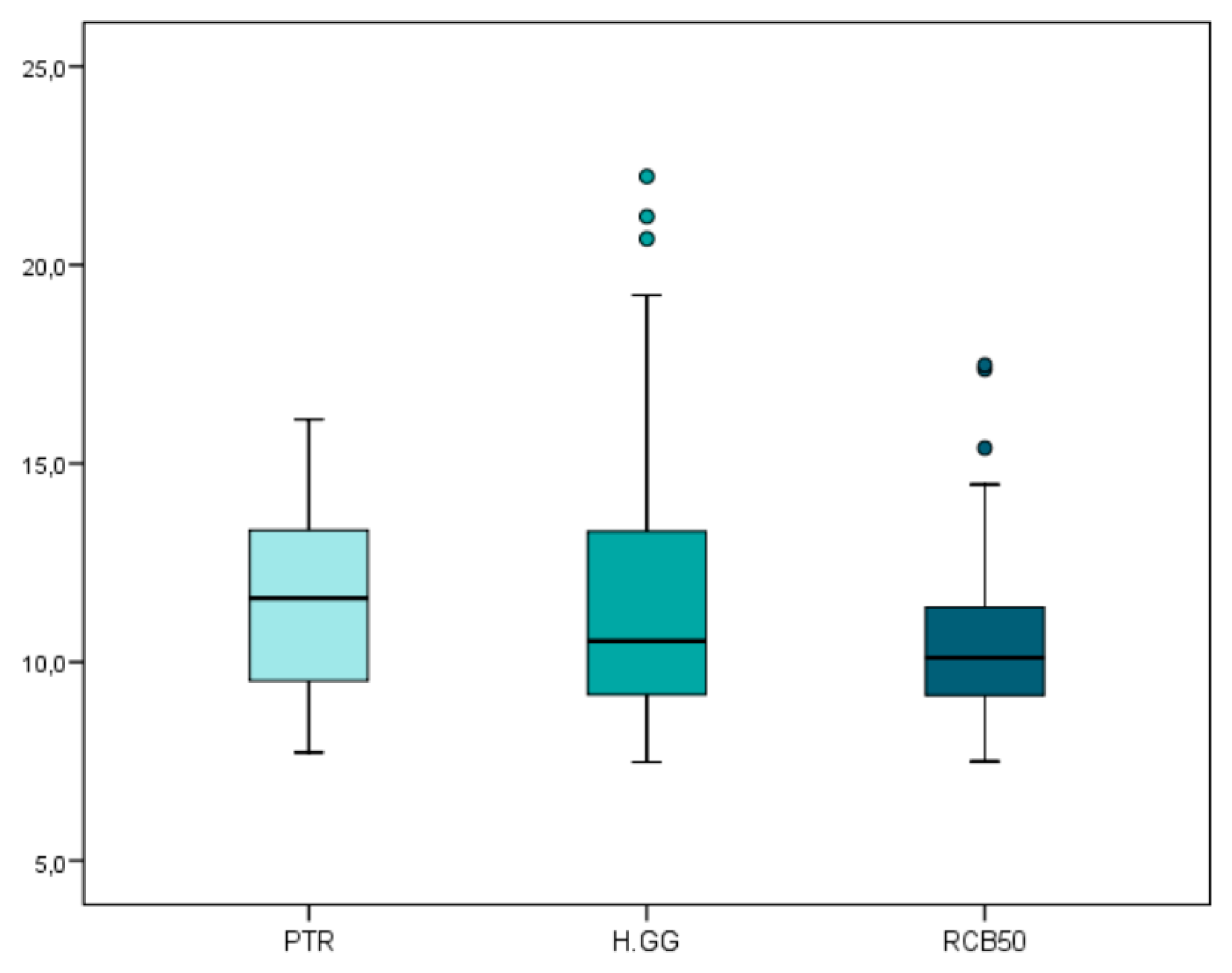
| Root Canal Filling Material Volume | PTR | 33 | 11.63 * | 2.47 | 7.72 | 16.11 |
| RCB50 | 33 | 10.70 * | 2.63 | 7.50 | 17.48 | |
| H-GG | 33 | 12.02 * | 3.99 | 7.48 | 22.23 |
| n | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
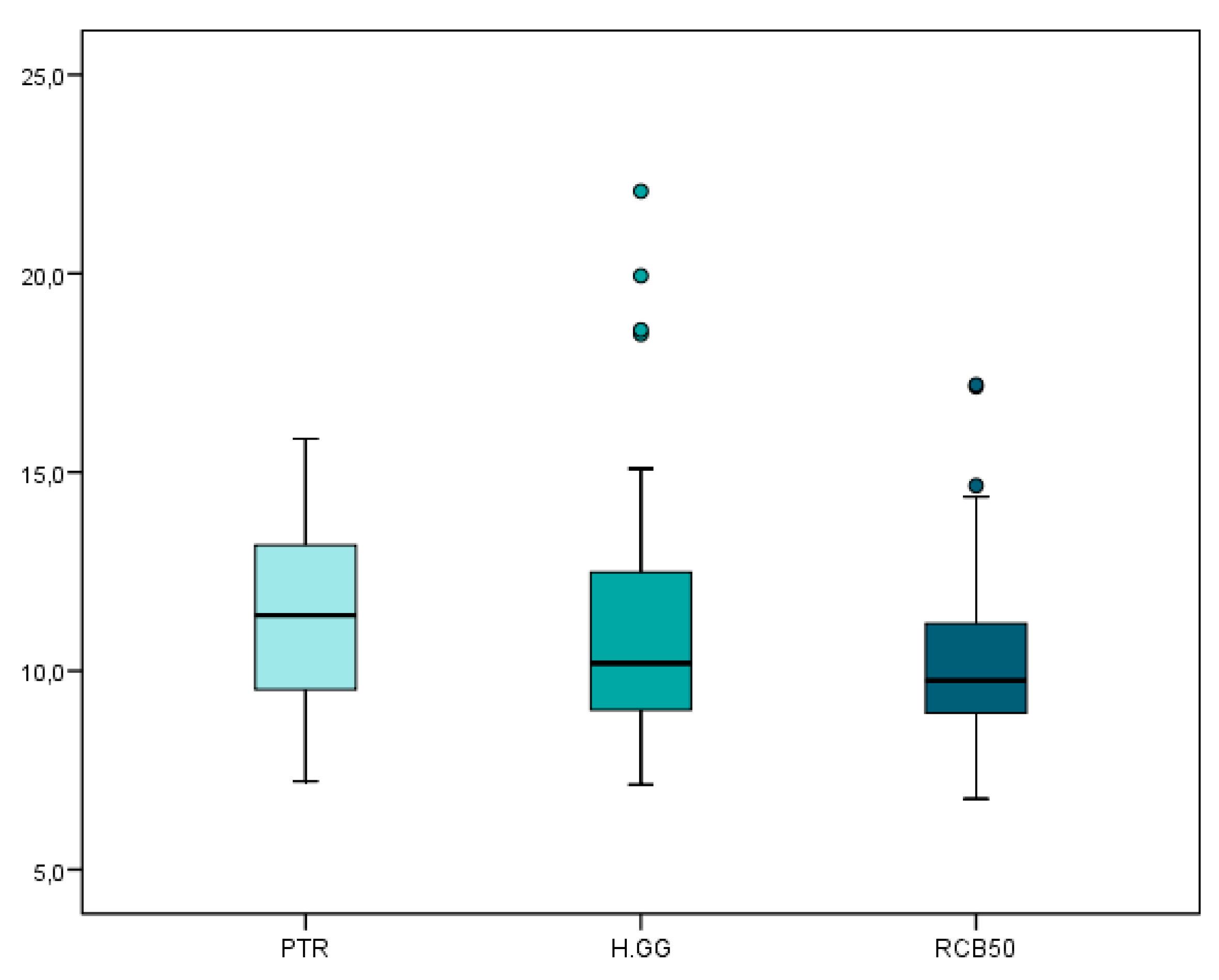
| Root Canal Filling Material Remaining Volume | PTR | 33 | 11.47 * | 2.45 | 7.22 | 15.84 |
| RCB50 | 33 | 10.49 * | 2.65 | 6.78 | 17.20 | |
| H-GG | 33 | 11.56 * | 3.72 | 7.14 | 22.07 |
| n | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
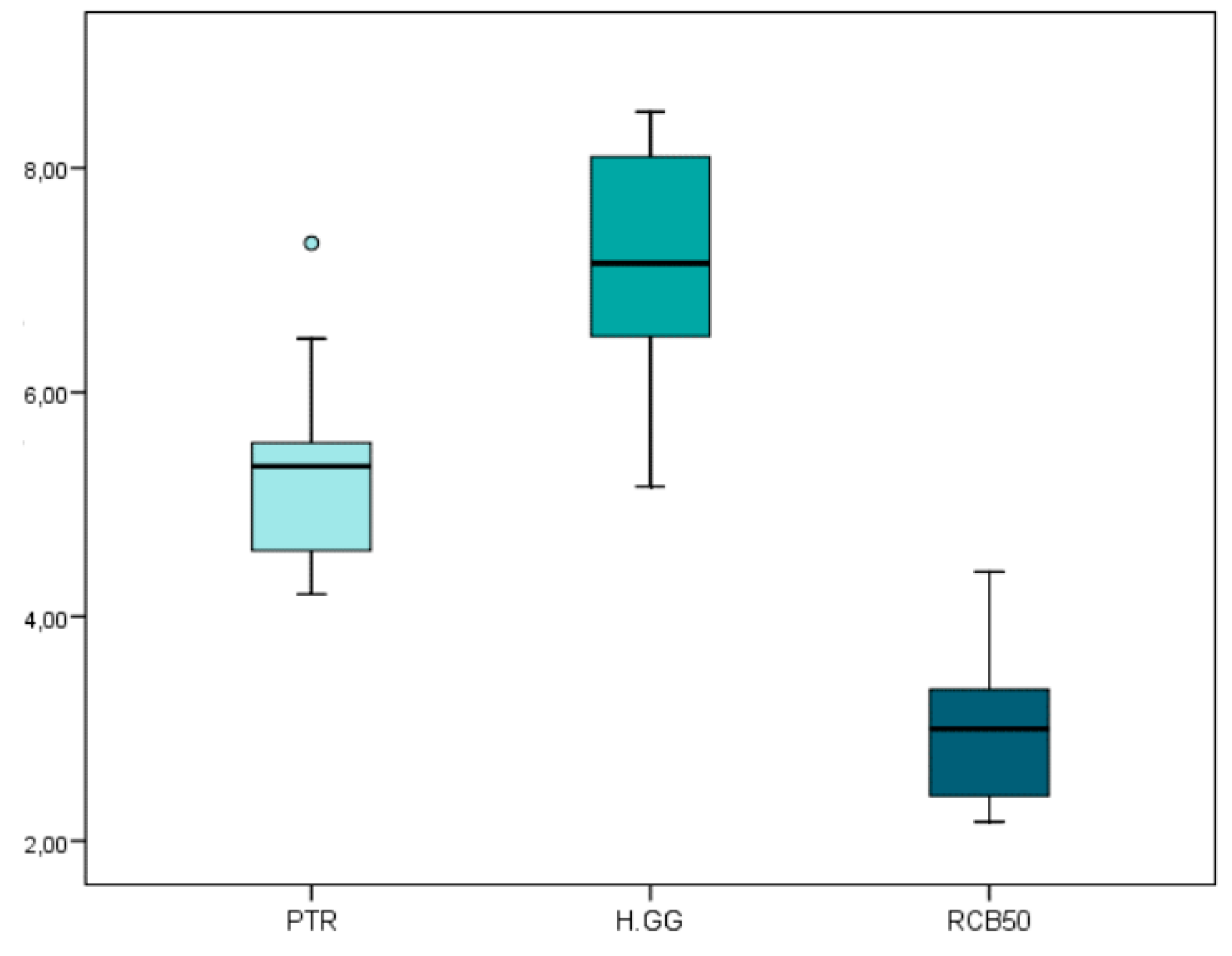
| Non-Surgical Endodontic Retreatment Working Time | PTR | 33 | 5.27 * | 0.72 | 4.20 | 7.33 |
| RCB50 | 33 | 2.93 * | 0.61 | 2.17 | 4.40 | |
| H-GG | 33 | 7.13 * | 0.87 | 5.16 | 8.50 |
| n | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
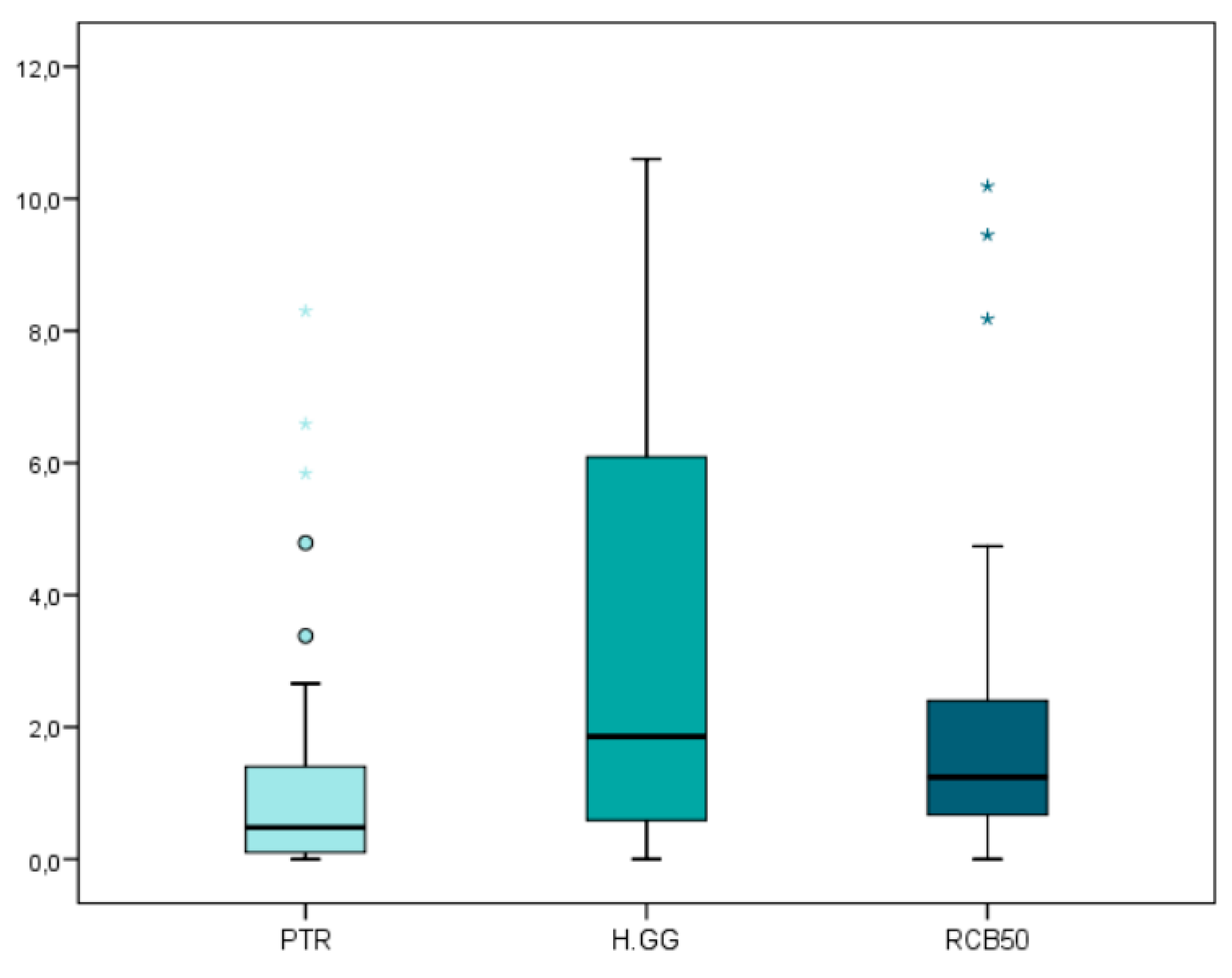
| Remaining Root Canal Filling Material | PTR | 33 | 1.43 * | 2.09 | 0.00 | 8.30 |
| RCB50 | 33 | 2.07 * | 2.57 | 0.00 | 10.19 | |
| H-GG | 33 | 3.52 * | 3.66 | 0.00 | 10.60 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alakabani, T.-F.; Faus-Llácer, V.; Faus-Matoses, I.; Ruiz-Sánchez, C.; Zubizarreta-Macho, Á.; Sauro, S.; Faus-Matoses, V. The Efficacy of Rotary, Reciprocating, and Combined Non-Surgical Endodontic Retreatment Techniques in Removing a Carrier-Based Root Canal Filling Material from Straight Root Canal Systems: A Micro-Computed Tomography Analysis. J. Clin. Med. 2020, 9, 1989. https://doi.org/10.3390/jcm9061989
Alakabani T-F, Faus-Llácer V, Faus-Matoses I, Ruiz-Sánchez C, Zubizarreta-Macho Á, Sauro S, Faus-Matoses V. The Efficacy of Rotary, Reciprocating, and Combined Non-Surgical Endodontic Retreatment Techniques in Removing a Carrier-Based Root Canal Filling Material from Straight Root Canal Systems: A Micro-Computed Tomography Analysis. Journal of Clinical Medicine. 2020; 9(6):1989. https://doi.org/10.3390/jcm9061989
Chicago/Turabian StyleAlakabani, Tarek-Fahed, Vicente Faus-Llácer, Ignacio Faus-Matoses, Celia Ruiz-Sánchez, Álvaro Zubizarreta-Macho, Salvatore Sauro, and Vicente Faus-Matoses. 2020. "The Efficacy of Rotary, Reciprocating, and Combined Non-Surgical Endodontic Retreatment Techniques in Removing a Carrier-Based Root Canal Filling Material from Straight Root Canal Systems: A Micro-Computed Tomography Analysis" Journal of Clinical Medicine 9, no. 6: 1989. https://doi.org/10.3390/jcm9061989