Supportive Implant Therapy (SIT): A Prospective 10-Year Study of Patient Compliance Rates and Impacting Factors




Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
- -
- age ≥ 18 years;
- -
- receiving surgical and prosthetic implant therapy in the study center;
- -
- implant surgery received between January 2005 and December 2008; and
- -
- available data including anamnesis and clinical data during an observation period of at least 10 years.
- -
- taking medication that influences bone metabolism (i.e., bisphosphonates) or causes gingival hyperplasia;
- -
- having allergies against the materials used; and
- -
- exclusively referred for implant surgery.
2.2. Treatment
2.3. Data Analysis
- -
- age (at the time of implant insertion);
- -
- gender;
- -
- smoking habits;
- -
- medical history (heart disease, diabetes);
- -
- number of implants (after the examination time of 10 years);
- -
- implant position;
- -
- pre-existing experience in prophylactic programs;
- -
- geographical distance to the practice; and
- -
- surgical procedure of the implant insertion (immediate implant placement, sinus lift procedure)
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Implant Treatments
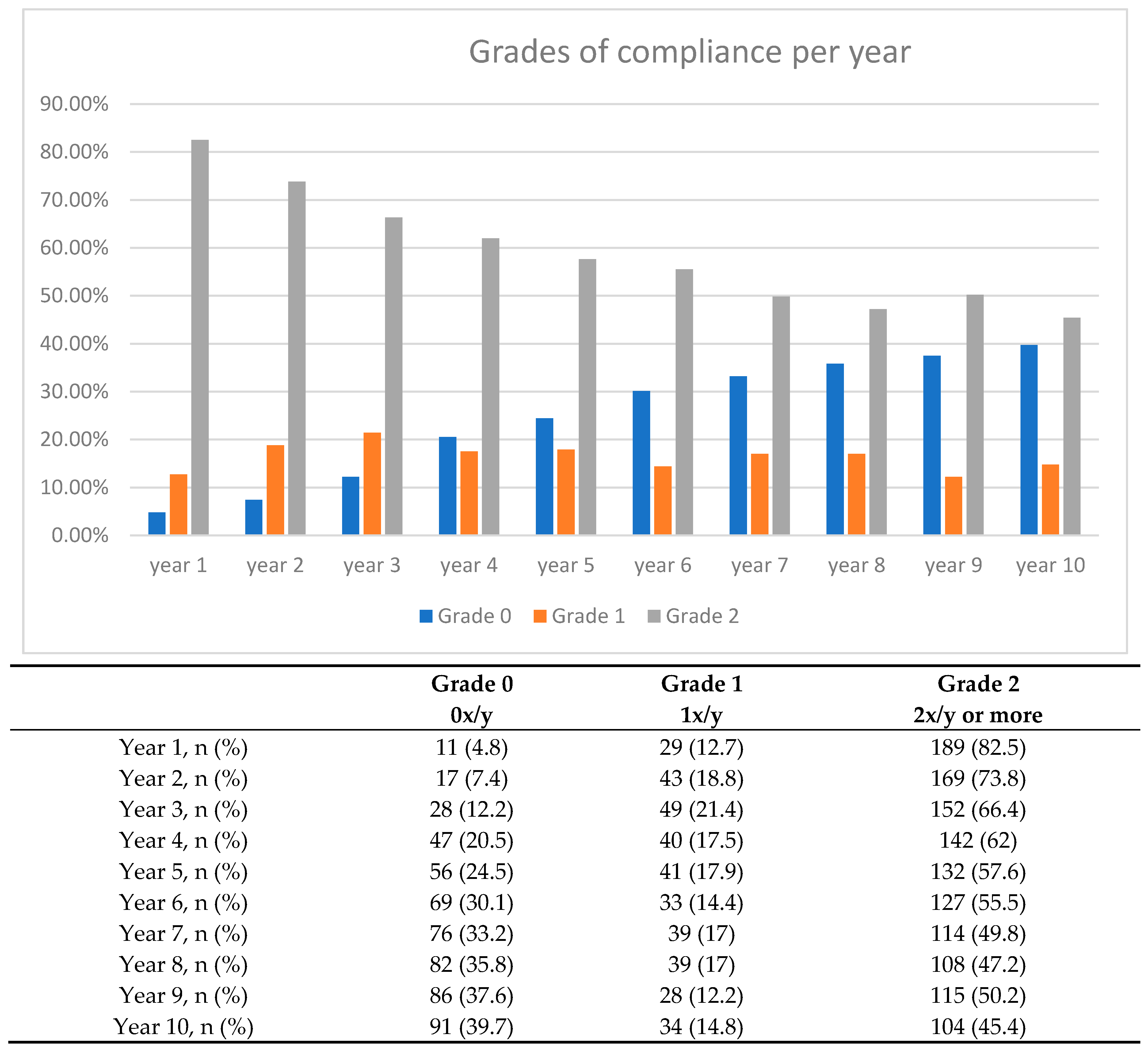
3.3. SIT Compliance
3.4. Analysis of Influence on Compliance
3.4.1. Number of Implants Per Patient
3.4.2. Type of Implant-Supported Prostheses
3.4.3. Geographical Distance to Study Center
3.4.4. Cardiovascular Diseases and Smoking
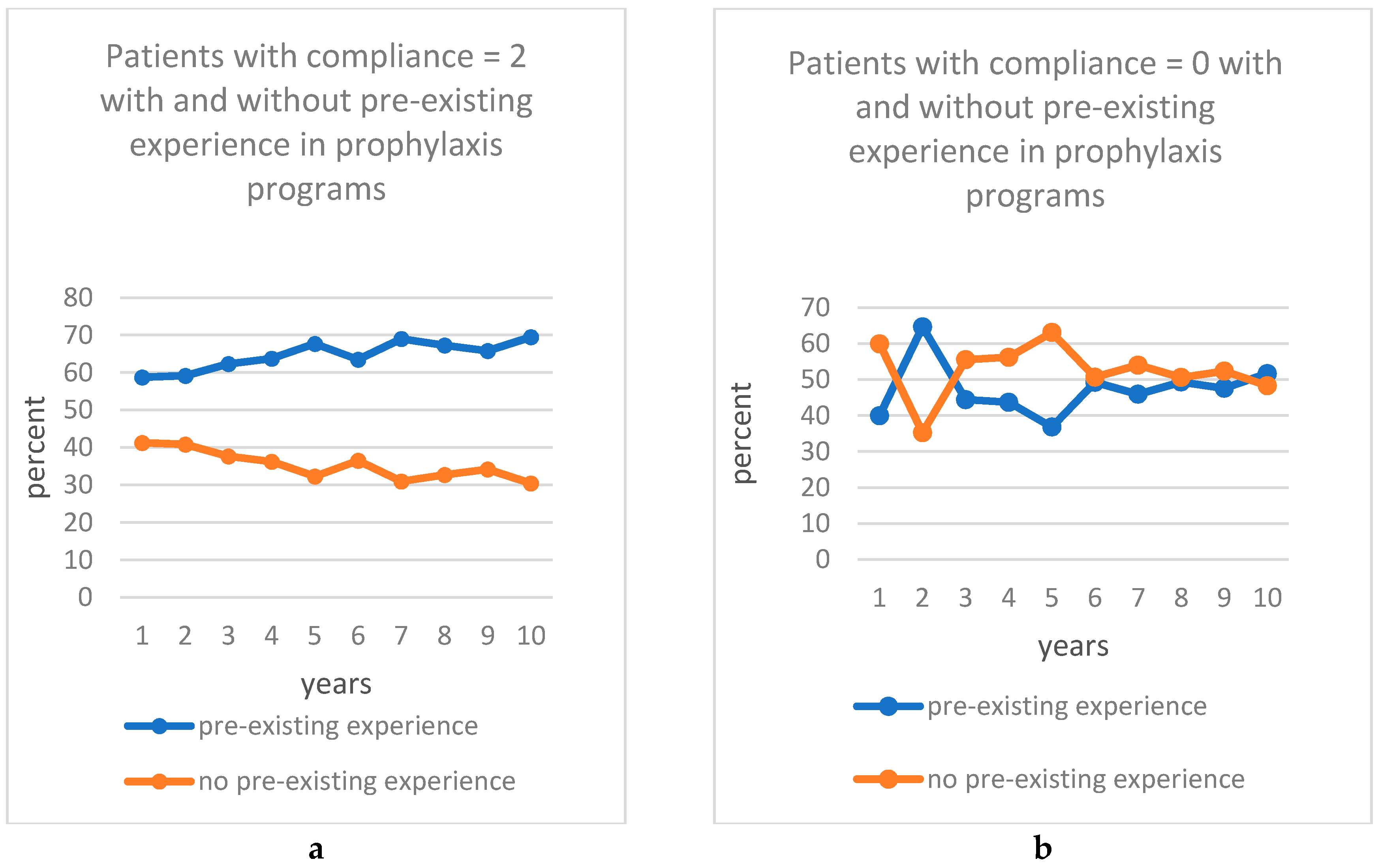
3.4.5. Pre-Existing Experience in a Prophylaxis Program
3.4.6. Reasons for Dropout
4. Discussion
4.1. Main Results
4.2. Limitations and Strengths
4.3. Interpretation
5. Conclusions and Implications for Clinical Practice
Author Contributions
Funding
Conflicts of Interest
References
- Axelsson, P.; Lindhe, J. The significance of maintenance care in the treatment of periodontal disease. J. Clin. Periodontol. 1981, 8, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; McHuon, R.B.; Oliphant, T.H.; Ortiz-Campos, C. Comparison of surgical and nonsurgical treatment of periodontal disease A review of current studies and additional results after 6 1/2 years. J. Clin. Periodontol. 1983, 10, 524–541. [Google Scholar] [CrossRef] [PubMed]
- Rosling, B.; Serino, G.; Hellstrom, M.K.; Socransky, S.S.; Lindhe, J. Longitudinal periodontal tissue alterations during supportive therapy. Findings from subjects with normal and high susceptibility to periodontal disease. J. Clin. Periodontol. 2001, 28, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, L.; Wasserman, B. A long-term survey of tooth loss in 600 treated periodontal patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFall, W.T. Tooth loss in 100 treated patients with periodontal disease: A long-term study. J. Periodontol. 1982, 53, 539–549. [Google Scholar] [CrossRef] [PubMed]
- McGuire, M.K.; Nunn, M.E. Prognosis versus actual outcome. III. The effectiveness of clinical parameters in accurately predicting tooth survival. J. Periodontol. 1996, 67, 666–674. [Google Scholar] [CrossRef] [Green Version]
- Fardal, O.; Johannessen, A.C.; Linden, G.J. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J. Clin. Periodontol. 2004, 31, 550–555. [Google Scholar] [CrossRef]
- Chambrone, L.A.; Chambrone, L. Tooth loss in well-maintained patients with chronic periodontitis during long-term supportive therapy in Brazil. J. Clin. Periodontol. 2006, 33, 759–764. [Google Scholar] [CrossRef]
- Faggion, C.M.; Petersilka, G.; Lange, D.E.; Gerss, J.; Flemmig, T.F. Prognostic model for tooth survival in patients treated for periodontitis. J. Clin. Periodontol. 2007, 34, 226–231. [Google Scholar] [CrossRef]
- Pretzl, B.; Kaltschmitt, J.; Kim, T.-S.; Reitmeir, P.; Eickholz, P. Tooth loss after active periodontal therapy. 2: Tooth-related factors. J. Clin. Periodontol. 2008, 35, 175–182. [Google Scholar] [CrossRef]
- König, J.; Plagmann, H.C.; Rühling, A.; Kocher, T. Tooth loss and pocket probing depths in compliant periodontally treated patients: A retrospective analysis. J. Clin. Periodontol. 2002, 29, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, A.R.; Newcomb, G.M.; Nixon, K.C. Compliance with supportive periodontal therapy. J. Periodontol. 1991, 62, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Ojima, M.; Hanioka, T.; Shizukuishi, S. Survival analysis for degree of compliance with supportive periodontal therapy. J. Clin. Periodontol. 2001, 28, 1091–1095. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G.; Glover, M.E.; Schoen, J.; Baus, C.; Jacobs, T. Compliance with maintenance therapy in a private periodontal practice. J. Periodontol. 1984, 55, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, D.; Gaveglio, L. Supportive periodontal therapy and dental implants: An analysis of patients’ compliance. Clin. Oral Impl. Res. 2012, 23, 1385–1388. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, S.; Favril, C.; De Nutte, M.; Teughels, W.; Quirynen, M. Patient compliance as a risk factor for the outcome of implant treatment. Periodontol. 2000 2019, 81, 209–225. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Eickholz, P.; Loos, B.G.; Papapanou, P.; van der Velden, U.; Armitage, G.; Bouchard, P.; Deinzer, R.; Dietrich, T.; Hughes, F.; et al. Principles in prevention of periodontal diseases. J. Clin. Periodontol. 2015, 42, S5–S11. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef]
- Thoma, D.S.; Naenni, N.; Figuero, E.; Hämmerle, C.H.F.; Schwarz, F.; Jung, R.E.; Sanz-Sánchez, I. Effects of soft tissue augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 32–49. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45, S237–S245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyer, H.; Grischke, J.; Tiede, C.; Eberhard, J.; Schweitzer, A.; Toikkanen, S.E.; Glöckner, S.; Krause, G.; Stiesch, M. Epidemiology and risk factors of peri-implantitis: A systematic review. J. Periodontal Res. 2018, 53, 657–681. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Clin. Periodontol. 2018, 45, S246–S266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinidis, I.K.; Kotsakis, G.A.; Gerdes, S.; Walter, M.H. Cross-sectional study on the prevalence and risk indicators of peri-implant diseases. Eur. J. Oral Implantol. 2015, 8, 75–88. [Google Scholar] [PubMed]
- Salvi, G.; Lang, N. Diagnostic parameters for monitoring peri-implant conditions. Int. J. Oral Maxillofac. Implants 2004, 19, 116–127. [Google Scholar] [PubMed]
- Zangrando, M.S.; Damante, C.A.; Sant’Ana, A.C.; Rubo de Rezende, M.L.; Greghi, S.L.; Chambrone, L. Long-term evaluation of periodontal parameters and implant outcomes in periodontally compromised patients: A systematic review. J. Periodontol. 2015, 86, 201–221. [Google Scholar] [CrossRef]
- Menini, M.; Setti, P.; Pera, P.; Pera, F.; Pesce, P. Peri-implant Tissue Health and Bone Resorption in Patients with Immediately Loaded, Implant-Supported, Full-Arch Prostheses. Int. J. Prosthodont. 2018, 31, 327–333. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.M.; Faggion, C.M.; Duncan, W.J. The frequency of peri-implant diseases: A systematic review and meta-analysis. J. Periodontol. 2013, 84, 1586–1598. [Google Scholar] [CrossRef] [Green Version]
- Frisch, E.; Vach, K.; Ratka-Krueger, P. Impact of supportive implant therapy on peri-implant diseases: A retrospective 7-year study. J. Clin. Periodontol. 2019, 47, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Frisch, E.; Ziebolz, D.; Vach, K.; Ratka-Krüger, P. Supportive post-implant therapy: Patient compliance rates and impacting factors: 3-year follow-up. J. Clin. Periodontol. 2014, 41, 1007–1014. [Google Scholar] [CrossRef]
- Mombelli, A.; Marxer, M.; Gaberthüel, T.; Grander, U.; Lang, N.P. The microbiota of osseointegrated implants in patients with a history of periodontal disease. J. Clin. Periodontol. 1995, 22, 124–130. [Google Scholar] [CrossRef]
- Lee, D.W. Validated surrogate endpoints needed for peri-implantitis. Evid. Based Dent. 2011, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Wennstrom, J.L.; Ekestubbe, A.; Grondahl, K.; Karlsson, S.; Lindhe, J. Oral rehabilitation with implant-supported fixed partial dentures in periodontitis-susceptible subjects. A 5-year prospective study. J. Clin. Periodontol. 2004, 31, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Anner, R.; Grossmann, Y.; Anner, Y.; Levin, L. Smoking, diabetes mellitus, periodontitis, and supportive periodontal treatment as factors associated with dental implant survival: A long-term retrospective evaluation of patients followed for up to 10 years. Implant Dent. 2010, 19, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinke, S.; Ohl, S.; Ziebolz, D.; Lange, K.; Eickholz, P. Prevalence of periimplant disease in partially edentulous patients: A practice- based cross-sectional study. Clin. Oral. Implants Res. 2010, 22, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Takenaka-Martinez, S.; Cota, L.O.; Ferreira, S.D.; Silva, G.L.; Costa, J.E. Peri-implant disease in subjects with and without preventive maintenance: A 5-year follow-up. J. Clin. Periodontol. 2012, 39, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Frisch, E.; Ziebolz, D.; Ratka-Kruger, P.; Rinke, S. Double crown-retained maxillary overdentures: 5-Year follow-up. Clin. Implant. Dent. Relat. Res. 2015, 17, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Frisch, E.; Ziebolz, D.; Rinke, S. Longterm results of implant-supported over-dentures retained by double crowns: A practice-based retrospective study after minimally 10 years follow-up. Clin. Oral. Implants Res. 2013, 12, 1281–1287. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Observational Period | 10 Years | ||
|---|---|---|---|
| Gender | Male | 94 | 41% |
| Female | 135 | 59% | |
| Illnesses | Diabetes mellitus | 8 | 3.5% |
| Cardiovascular diseases | 68 | 29.7% | |
| Active smoker | 16 | 7% | |
| Average age in years | 64.34 | ||
| Experience with the prophylaxis program | Yes | 138 | 60.3% |
| No | 91 | 39.7% |
| Number of Implants | Percentage | |
|---|---|---|
| Ankylos | 416 | 81 |
| Branemark | 68 | 13 |
| ITI Bonefit | 1 | 0.2 |
| Astra | 25 | 5 |
| 3i | 4 | 0.8 |
| Total | 514 | 100 |
| Number of Implants | Frequency | Percent |
|---|---|---|
| 1 | 72 | 31.4 |
| 2 | 68 | 29.7 |
| 3 | 20 | 8.7 |
| 4 | 31 | 13.5 |
| 5 | 9 | 3.9 |
| 6 | 10 | 4.4 |
| 7 | 4 | 1.7 |
| 8 | 6 | 2.6 |
| 9 | 4 | 1.7 |
| 10 | 2 | 0.9 |
| 11 | 1 | 0.4 |
| 12 | 1 | 0.4 |
| 16 | 1 | 0.4 |
| Total | 229 | 99.7 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitschke, J.; Peikert, S.A.; Vach, K.; Frisch, E. Supportive Implant Therapy (SIT): A Prospective 10-Year Study of Patient Compliance Rates and Impacting Factors. J. Clin. Med. 2020, 9, 1988. https://doi.org/10.3390/jcm9061988
Mitschke J, Peikert SA, Vach K, Frisch E. Supportive Implant Therapy (SIT): A Prospective 10-Year Study of Patient Compliance Rates and Impacting Factors. Journal of Clinical Medicine. 2020; 9(6):1988. https://doi.org/10.3390/jcm9061988
Chicago/Turabian StyleMitschke, Julia, Stefanie Anna Peikert, Kirstin Vach, and Eberhard Frisch. 2020. "Supportive Implant Therapy (SIT): A Prospective 10-Year Study of Patient Compliance Rates and Impacting Factors" Journal of Clinical Medicine 9, no. 6: 1988. https://doi.org/10.3390/jcm9061988