Non-Vitamin K Oral Anticoagulants in Adults with Congenital Heart Disease: A Systematic Review

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
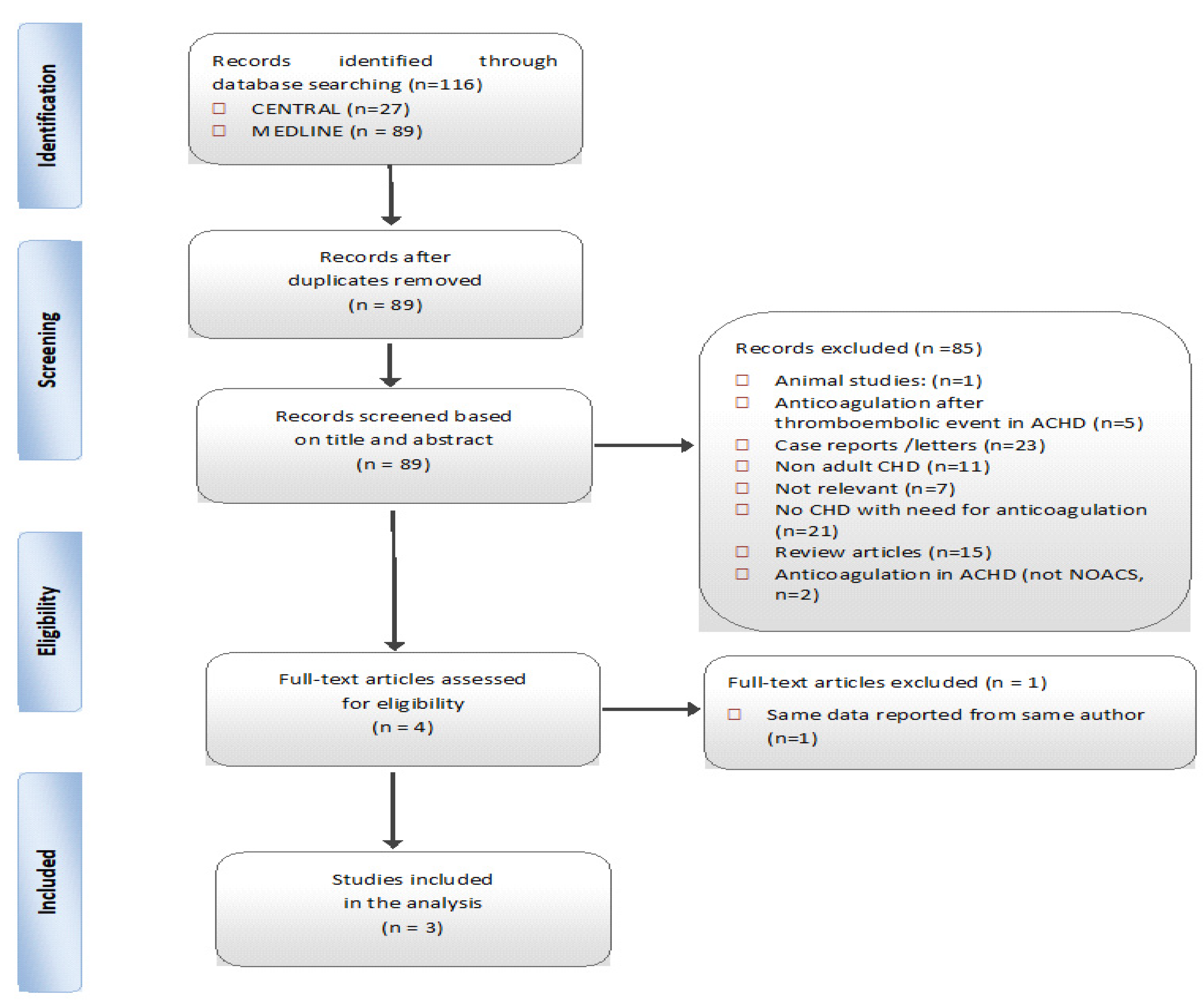
2.3. Selection of Studies
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Synthesis–Statistics
3. Results
3.1. Cumulative Data and Individual Study Characteristics
3.2. Cumulative Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| ACHD | adult patients with congenital heart disease |
| CHD | congenital heart disease |
| VKA | Vitamin K antagonist |
| NOACs | Non-vitamin K oral anticoagulants |
| NOS | Newcastle-Ottawa scale |
| QoL | Quality of Life |
Appendix A
- Adult congenital heart disease
- Grown–up congenital heart disease
- Aortic stenosis
- Atrial septal defect
- Atrioventricular septal defect
- Bicuspid aortic valve
- Dextrocardia
- Double inlet left ventricle
- Double outlet right ventricle
- Ebstein’s anomaly
- Hypoplastic left heart syndrome
- Hypoplastic right heart syndrome
- Mitral stenosis
- Persistent truncus arteriosus
- Pulmonary atresia
- Pulmonary stenosis
- Transposition of the great vessels
- Tricuspid atresia
- Ventricular septal defect (VSD)
- New oral anticoagulants
- NOACs
- DOACs
- Xarelto
- Eliquis
- Pradaxa
- Rivaroxaban
- Apixaban
- Edoxaban
- Dabigatran
- Factor X inhibitors
- 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19
- 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26 OR 27 OR 28 OR 29 OR 30
- 31 AND 32
- 34.
- “Factor Xa Inhibitors” [MESH]
- 35.
- “Antithrombins” [MESH]
- 36.
- “Adult Congenital heart disease” [MESH]
- 37.
- 1 OR 2
- 38.
- 4 AND 5
- #1 MeSH descriptor: [Heart Defects, Congenital] explode all trees
- #2 MeSH descriptor: [Anticoagulants] explode all trees
- #3 1 AND #2


References
- Yap, S.-C.; Harris, L.; Chauhan, V.S.; Oechslin, E.N.; Silversides, C.K. Identifying High Risk in Adults with Congenital Heart Disease and Atrial Arrhythmias. Am. J. Cardiol. 2011, 108, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Verheugt, C.L.; Uiterwaal, C.S.P.M.; van der Velde, E.T.; Meijboom, F.J.; Pieper, P.G.; van Dijk, A.P.J.; Vliegen, H.W.; Grobbee, D.E.; Mulder, B.J.M. Mortality in adult congenital heart disease. Eur. Heart J. 2010, 31, 1220–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelfriet, P.; Boersma, E.; Oechslin, E.; Tijssen, J.; Gatzoulis, M.A.; Thilén, U.; Kaemmerer, H.; Moons, P.; Meijboom, F.; Popelová, J.; et al. The spectrum of adult congenital heart disease in Europe: Morbidity and mortality in a 5 year follow-up period. The Euro Heart Survey on adult congenital heart disease. Eur. Heart J. 2005, 26, 2325–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanz, J.; Brophy, J.M.; Therrien, J.; Kaouache, M.; Guo, L.; Marelli, A.J. Stroke in Adults with Congenital Heart Disease: Incidence, Cumulative Risk, and Predictors. Circulation 2015, 132, 2385–2394. [Google Scholar] [CrossRef]
- Giannakoulas, G.; Boutsikou, M. The Gordian knot of thromboembolism in congenital heart disease. Heart 2015, 101, 1523–1524. [Google Scholar] [CrossRef]
- Hoffmann, A.; Chockalingam, P.; Balint, O.H.; Dadashev, A.; Dimopoulos, K.; Engel, R.; Schmid, M.; Schwerzmann, M.; Gatzoulis, M.A.; Mulder, B.; et al. Cerebrovascular accidents in adult patients with congenital heart disease. Heart 2010, 96, 1223–1226. [Google Scholar] [CrossRef]
- Brotschi, B.; Hug, M.I.; Latal, B.; Neuhaus, D.; Buerki, C.; Kroiss, S.; Spoerri, C.; Albisetti, M. Incidence and predictors of indwelling arterial catheter-related thrombosis in children. J. Thromb. Haemost. 2011, 9, 1157–1162. [Google Scholar] [CrossRef]
- Diab, Y.A.; Ramakrishnan, K.; Alfares, F.A.; Hynes, C.F.; Chounoune, R.; Shankar, V.; Kanter, J.P.; Nath, D.S. Transcatheter Treatment of Thrombosis in the Single Ventricle Pathway: An Institutional Experience. Congenit. Heart Dis. 2016, 11, 39–44. [Google Scholar] [CrossRef]
- Khairy, P.; Landzberg, M.J.; Gatzoulis, M.A.; Mercier, L.A.; Fernandes, S.M.; Lavoie, J.P.; Guerra, P.G.; Frogoudaki, A.; Walsh, E.P.; Dore, A.; et al. Transvenous pacing leads and systemic thromboemboli in patients with intracardiac shunts: A multicenter study. Circulation 2006, 113, 2391–2397. [Google Scholar] [CrossRef] [Green Version]
- Bouchardy, J.; Therrien, J.; Pilote, L.; Ionescu-Ittu, R.; Martucci, G.; Bottega, N.; Marelli, A.J. Atrial arrhythmias in adults with congenital heart disease. Circulation 2009, 120, 1679–1686. [Google Scholar] [CrossRef] [Green Version]
- Giannakoulas, G.; Dimopoulos, K.; Yuksel, S.; Inuzuka, R.; Pijuan-Domenech, A.; Hussain, W.; Tay, E.L.; Gatzoulis, M.A.; Wong, T. Atrial tachyarrhythmias late after Fontan operation are related to increase in mortality and hospitalization. Int. J. Cardiol. 2012, 157, 221–226. [Google Scholar] [CrossRef]
- Khairy, P.; van Hare, G.F.; Balaji, S.; Berul, C.I.; Cecchin, F.; Cohen, M.I.; Daniels, C.J.; Deal, B.J.; Dearani, J.A.; De Groot, N.; et al. PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease. Can. J. Cardiol. 2014, 30, 1–63. [Google Scholar] [CrossRef] [PubMed]
- Lane, D.A.; Lip, G.Y.H. Use of the CHA2DS2-VASc and HAS-BLED Scores to Aid Decision Making for Thromboprophylaxis in Nonvalvular Atrial Fibrillation. Circulation 2012, 126, 860–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khairy, P.; Aboulhosn, J.; Broberg, C.S.; Cohen, S.; Cook, S.; Dore, A.; Fernandes, S.M.; Fournier, A.; Kay, J.; Levesque, S.; et al. Thromboprophylaxis for atrial arrhythmias in congenital heart disease: A multicenter study. Int. J. Cardiol. 2016, 223, 729–735. [Google Scholar] [CrossRef]
- Masuda, K.; Ishizu, T.; Niwa, K.; Takechi, F.; Tateno, S.; Horigome, H.; Aonuma, K. Increased risk of thromboembolic events in adult congenital heart disease patients with atrial tachyarrhythmias. Int. J. Cardiol. 2017, 234, 69–75. [Google Scholar] [CrossRef]
- Freisinger, E.; Koeppe, J.; Bronstein, L.; Makowski, L.; Reinecke, H.; Gerss, J.; Baumgartner, H.; Diller, G. P4161Oral anticoagulation in 13,344 adult patients with congenital heart disease (ACHD) in a longitudinal real-world setting in 2005–2017. Eur. Heart J. 2019, 40, ehz745. 0733. [Google Scholar] [CrossRef]
- Yang, H.; Bouma, B.J.; Mulder, B.J.M. Is Initiating NOACs for Atrial Arrhythmias Safe in Adults with Congenital Heart Disease? Cardiovasc. Drugs Ther. 2017, 31, 413–417. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, 1–28. [Google Scholar] [CrossRef]
- Home—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 17 April 2020).
- Warnes, C.A.; Liberthson, R.; Danielson, G.K.; Dore, A.; Harris, L.; Hoffman, J.I.; Somerville, J.; Williams, R.G.; Webb, G.D. Task force 1: The changing profile of congenital heart disease in adult life. J. Am. Coll. Cardiol. 2001, 37, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Schulman, S.; Anger, S.U.; Bergqvist, D.B.; Lassen, M.R.; Fisher, W. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J. Thromb. Haemost. 2010, 8, 202–204. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) For Assessing the Quality of Nonrandomised Studies in Meta-analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 March 2020).
- Stijnen, T.; Hamza, T.H.; Özdemir, P. Random effects meta-analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat. Med. 2010, 29, 3046–3067. [Google Scholar] [CrossRef]
- Julious, S.A. Two-sided confidence intervals for the single proportion: Comparison of seven methods by Robert G. Newcombe. Stat. Med. 2005, 24, 3383–3384. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rucker, G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 12 April 2020).
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis. In Meta-Analysis with R; Springer, Cham: Basel, Switzerland, 2015; pp. 187–216. [Google Scholar]
- Yang, H.; Bouma, B.J.; Dimopoulos, K.; Khairy, P.; Ladouceur, M.; Niwa, K.; Greutmann, M.; Schwerzmann, M.; Egbe, A.; Scognamiglio, G.; et al. Non-vitamin K antagonist oral anticoagulants (NOACs) for thromboembolic prevention, are they safe in congenital heart disease? Results of a worldwide study. Int. J. Cardiol. 2020, 299, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujol, C.; Müssigmann, M.; Schiele, S.; Nagdyman, N.; Niesert, A.C.; Kaemmerer, H.; Ewert, P.; Tutarel, O. Direct oral anticoagulants in adults with congenital heart disease—A single centre study. Int. J. Cardiol. 2020, 300, 127–131. [Google Scholar] [CrossRef]
- Georgekutty, J.; Kazerouninia, A.; Wang, Y.; Ermis, P.R.; Parekh, D.R.; Franklin, W.J.; Lam, W.W. Novel oral anticoagulant use in adult Fontan patients: A single center experience. Congenit. Heart Dis. 2018, 13, 541–547. [Google Scholar] [CrossRef]
- Heidendael, J.F.; Bokma, J.P.; de Groot, J.R.; Koolbergen, D.R.; Mulder, B.J.M.; Bouma, B.J. Weighing the risks: Thrombotic and bleeding events in adults with atrial arrhythmias and congenital heart disease. Int. J. Cardiol. 2015, 186, 315–320. [Google Scholar] [CrossRef]
- Clift, P.; Celermajer, D. Managing adult Fontan patients: Where do we stand? Eur. Respir. Rev. 2016, 25, 438–450. [Google Scholar] [CrossRef] [Green Version]
- Balling, G.; Vogt, M.; Kaemmerer, H.; Eicken, A.; Meisner, H.; Hess, J. Intracardiac thrombus formation after the Fontan operation. J. Thorac. Cardiovasc. Surg. 2000, 119, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Tsang, W.; Johansson, B.; Salehian, O.; Holm, J.; Webb, G.; Gatzoulis, M.A.; Therrien, J. Intracardiac thrombus in adults with the Fontan circulation. Cardiol. Young 2007, 17, 646–651. [Google Scholar] [CrossRef]
- Khairy, P.; Fernandes, S.M.; Mayer, J.E.; Triedman, J.K.; Walsh, E.P.; Lock, J.E.; Landzberg, M.J. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation 2008, 117, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsaied, T.; Alsidawi, S.; Allen, C.C.; Faircloth, J.; Palumbo, J.S.; Veldtman, G.R. Strategies for thromboprophylaxis in Fontan circulation: A meta-analysis. Heart 2015, 101, 1731–1737. [Google Scholar] [CrossRef] [PubMed]
- Mekaj, Y.H.; Mekaj, A.Y.; Duci, S.B.; Miftari, E.I. New oral anticoagulants: Their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events. Ther. Clin. Risk Manag. 2015, 11, 967–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, K.A. Pros and cons of new oral anticoagulants. Hematol. Am. Soc. Hematol. Educ. Progr. 2013, 2013, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Thomson Mangnall, L.J.; Sibbritt, D.W.; Al-Sheyab, N.; Gallagher, R.D. Predictors of warfarin non-adherence in younger adults after valve replacement surgery in the South Pacific. Heart Asia 2016, 8, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Tzikas, A.; Samaras, A.; Kartas, A.; Vasdeki, D.; Fotos, G.; Dividis, G.; Paschou, E.; Forozidou, E.; Tsoukra, P.; Kotsi, E.; et al. Motivational Interviewing to Support Oral AntiCoagulation adherence in patients with non-valvular Atrial Fibrillation (MISOAC-AF): A randomised clinical trial. Eur. Heart J. Cardiovasc. Pharmacother. 2020. [Google Scholar] [CrossRef]
- Raparelli, V.; Proietti, M.; Cangemi, R.; Lip, G.Y.H.; Lane, D.A.; Basili, S. Adherence to oral anticoagulant therapy in patients with atrial fibrillation focus on non-vitamin k antagonist oral anticoagulants. Thromb. Haemost. 2017, 117, 209–218. [Google Scholar]
- Gallagher, A.M.; Rietbrock, S.; Plumb, J.; van Staa, T.P. Initiation and persistence of warfarin or aspirin in patients with chronic atrial fibrillation in general practice: Do the appropriate patients receive stroke prophylaxis? J. Thromb. Haemost. 2008, 6, 1500–1506. [Google Scholar] [CrossRef]
- Fang, M.C.; Go, A.S.; Chang, Y.; Borowsky, L.H.; Pomernacki, N.K.; Udaltsova, N.; Singer, D.E. Warfarin discontinuation after starting warfarin for atrial fibrillation. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 624–631. [Google Scholar] [CrossRef] [Green Version]
- Gomes, T.; Mamdani, M.M.; Holbrook, A.M.; Paterson, J.M.; Juurlink, D.N. Persistence with therapy among patients treated with warfarin for atrial fibrillation. Arch. Intern. Med. 2012, 172, 1687–1689. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singe, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| ACHD patients of any disease severity | Animal Studies |
| ACHD patients receiving NOAC for: ● Atrial arrhythmias (Intra-atrial reentrant tachycardia, AF, atrial flutter) ● Primary thromboprophylaxis ● Secondary thromboprophylaxis | Pediatric Population |
| ACHD patients with severe thrombocytopenia or recurrent hemorrhagic events. |
| Study | Cohort Representativeness | Selection of Non-Exposed Cohort | Ascertainment of Exposure | The Outcome of Interest Not Present | comparability of Cohorts | Assessment of Outcome | Follow-Up Long Enough | Adequacy of Follow Up of Cohorts | Total Score | Quality of Study |
|---|---|---|---|---|---|---|---|---|---|---|
| Yang et al. [28] | * | no | * | * | * | * | * | * | 7 | medium |
| Pujol et al. [29] | * | no | * | * | no | * | * | * | 6 | medium |
| Georgekutty et al. [30] | * | no | * | * | no | * | * | * | 6 | medium |
| Author | Year | Type of Study | Total Patients | Total Patient-Years of Follow-Up | Primary Endpoint |
|---|---|---|---|---|---|
| Yang et al. [28] | 2019 | Prospective Cohort | 530 | 613 | Thromboembolism and major bleeding |
| Pujol et al. [29] | 2019 | Retrospective Cohort | 215 | 283.8 | Thromboembolism and major, minor bleeding |
| Georgekutty et al. [30] | 2018 | Retrospective Cohort | 21 | 26.3 | Thromboembolism and major, non-major and minor bleeding |
| Author | Male Sex (%) | Age (Years) mean ± SD | Indication for Anticoagulation (%) | Severity of ACHD (%) | Thrombotic Events n (%) | Bleeding Events n (%) | CHA2ADSVA2Sc ≥ 2 (%) | HAS-BLED ≤ 2 (%) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AA | PTP | STP | Simple | Moderate | Complex | |||||||
| Yang et al. [28] | 55% | 47.0 ± 15.0 | 90.8 | 3.2 | 6.0 | 14.9 | 45.1 | 40.0 | 6 (1.1) | 7 (1.3) | 46.4 | 95.0 |
| Pujol et al. [29] | 48% | 48.4 ± 15.4 | 66.8 * | 5.6 * | 42.9 * | 32.1 | 23.7 | 44.2 | 2 (0.7) | 9 (3.1) | 49.3 | 87.5 |
| Georgekutty et al. [30] | 47% | 33.5 ± 8.0 | 57.0 | 9.5 | 33.3 | - | - | 100 | 1 (4.76) | 0 | 42.9 | 100 |
| Study | Patients (n = 9) | Sex | Age | ACHD Type | NOAC * | Thromboembolic Event | Indication | CHA2DS2-VASc | HAS -BLED | Risk Factors and Comorbidities |
|---|---|---|---|---|---|---|---|---|---|---|
| Georgekutty [30] | 1 | M | 21 | Fontan | Dabigatran 110 mg b.i.d | Deep Vein Thrombosis | Persistent Right-to-Left Shunt | 1 | 0 | Protein-losing enteropathy |
| Yang [28] | 2 | M | 30 | Coronary atriovenous fistula | Dabigatran | Deep Vein Thrombosis | Atrial Arrhythmias | 3 | 2 | Severe Tricuspid Regurgitation |
| Yang [28] | 3 | M | 42 | Fontan | Apixaban | Pulmonary Embolism | Atrial Arrhythmias | 0 | 3 | - |
| Yang [28] | 4 | M | 25 | Fontan | Rivaroxaban | Intracardiac Thrombus | Atrial Arrhythmias | 2 | 1 | - |
| Yang [28] | 5 | M | 44 | Tetralogy Fallot | Apixaban | Pulmonary Embolism | Atrial Arrhythmias | 1 | 1 | - |
| Yang [28] | 6 | M | 23 | Fontan | Apixaban | Ischemic Stroke | Atrial Arrhythmias | 1 | 0 | - |
| Yang [28] | 7 | F | 25 | Transposition of Great Arteries | Apixaban | Intracardiac Thrombus | Atrial Arrhythmias | 4 | 0 | Severe Tricuspid Regurgitation |
| Pujol [29] | 8 | M | 51 | VSD (corrected) | Dabigatran 150 mg b.i.d | Stroke | Primary Thromboprophylaxis | 3 | 3 | Stroke, TIA, Liver Disease, Arterial Hypertension |
| Pujol [29] | 9 | M | 50 | Aortic Aneurysm | Rivaroxaban 20 mg q.d | Deep Vein Thrombosis | Primary Thromboprophylaxis | 1 | 1 | Arterial Hypertension |
| Study | Patients (n = 16) | Sex | Age | ACHD type | NOAC * | Bleeding Location | Indication | CHA2D2-VASC | HAS-BLED | Risk Factors and Comorbidities |
|---|---|---|---|---|---|---|---|---|---|---|
| Yang [28] | 1 | F | 56 | Fontan | Apixaban | Gastrointestinal | AtrialArrhythmia | 2 | 1 | Mitral Regurgitation |
| Yang [28] | 2 | F | 71 | PAPVC | Rivaroxaban | Gastrointestinal | AtrialArrhythmia | 3 | 1 | Tricuspid Regurgitation |
| Yang [28] | 3 | F | 23 | CoA | Rivaroxaban | Menorrhagia | AtrialArrhythmia | 2 | 0 | Bioprosthetic AVand PV |
| Yang [28] | 4 | F | 42 | Eisenmenger | Rivaroxaban | Menorrhagia | Pulmonary Embolism | 3 | 2 | - |
| Yang [28] | 5 | F | 41 | Fontan | Apixaban | Menorrhagia | Atrial Arrhythmia | 4 | 0 | Mitral Valve Regurgitation |
| Yang [28] | 6 | M | 80 | ToF | Apixaban | Hematuria | AtrialArrhythmia | 4 | 1 | Pulmonary Stenosis |
| Yang [28] | 7 | F | 67 | Fontan | Rivaroxaban | Menorrhagia | AtrialArrhythmia | 2 | 2 | - |
| Pujol [29] | 8 | M | 59 | PFO | Apixaban 5 mg b.i.d | Cranial | PTP | 3 | 3 | Aspirin Arterial Hypertension |
| Pujol [29] | 9 | F | 48 | TGA-Mustard | Rivaroxaban 20 mg q.d | Cranial | PTP | 2 | 0 | Oral Contraception |
| Pujol [29] | 10 | M | 26 | PA + VSD, PH Deletion 22q11 | Rivaroxaban 10 mg q.d | Gastrointestinal | PTP | 1 | 3 | Renal Insufficiency, Cyanosis, Bleeding under VKA |
| Pujol [29] | 11 | M | 65 | ASD | Apixaban 2.5 mg b.i.d | Intraoccular | PTP | 3 | 2 | Arterial Hypertension Smoker |
| Pujol [29] | 12 | F | 44 | PA + VSDPAH | Apixaban 5 mg b.i.d | Intraarticular | PTP | 2 | 0 | Renal Insufficiency, Diabetes Mellitus |
| Pujol [29] | 13 | F | 46 | Marfan | Rivaroxaban 20 mg q.d | Intraarticular | PTP | 2 | 0 | Smoker |
| Pujol [29] | 14 | F | 43 | ASD | Rivaroxaban 20 mg q.d | Intramuscular | PTP | 1 | 0 | - |
| Pujol [29] | 15 | F | 34 | PFO | Edoxaban 60 mg q.d | Vaginal | PTP | 3 | 3 | Bleeding under VKA |
| Pujol [29] | 16 | F | 42 | VSD (corrected) | Rivaroxaban 20 mg q.d | Vaginal | PTP | 1 | 0 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stalikas, N.; Doundoulakis, I.; Karagiannidis, E.; Bouras, E.; Kartas, A.; Frogoudaki, A.; Karvounis, H.; Dimopoulos, K.; Giannakoulas, G. Non-Vitamin K Oral Anticoagulants in Adults with Congenital Heart Disease: A Systematic Review. J. Clin. Med. 2020, 9, 1794. https://doi.org/10.3390/jcm9061794
Stalikas N, Doundoulakis I, Karagiannidis E, Bouras E, Kartas A, Frogoudaki A, Karvounis H, Dimopoulos K, Giannakoulas G. Non-Vitamin K Oral Anticoagulants in Adults with Congenital Heart Disease: A Systematic Review. Journal of Clinical Medicine. 2020; 9(6):1794. https://doi.org/10.3390/jcm9061794
Chicago/Turabian StyleStalikas, Nikolaos, Ioannis Doundoulakis, Efstratios Karagiannidis, Emmanouil Bouras, Anastasios Kartas, Alexandra Frogoudaki, Haralambos Karvounis, Konstantinos Dimopoulos, and George Giannakoulas. 2020. "Non-Vitamin K Oral Anticoagulants in Adults with Congenital Heart Disease: A Systematic Review" Journal of Clinical Medicine 9, no. 6: 1794. https://doi.org/10.3390/jcm9061794