Association between Periodontal Diseases and Polycystic Ovary Syndrome: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. PICO Question
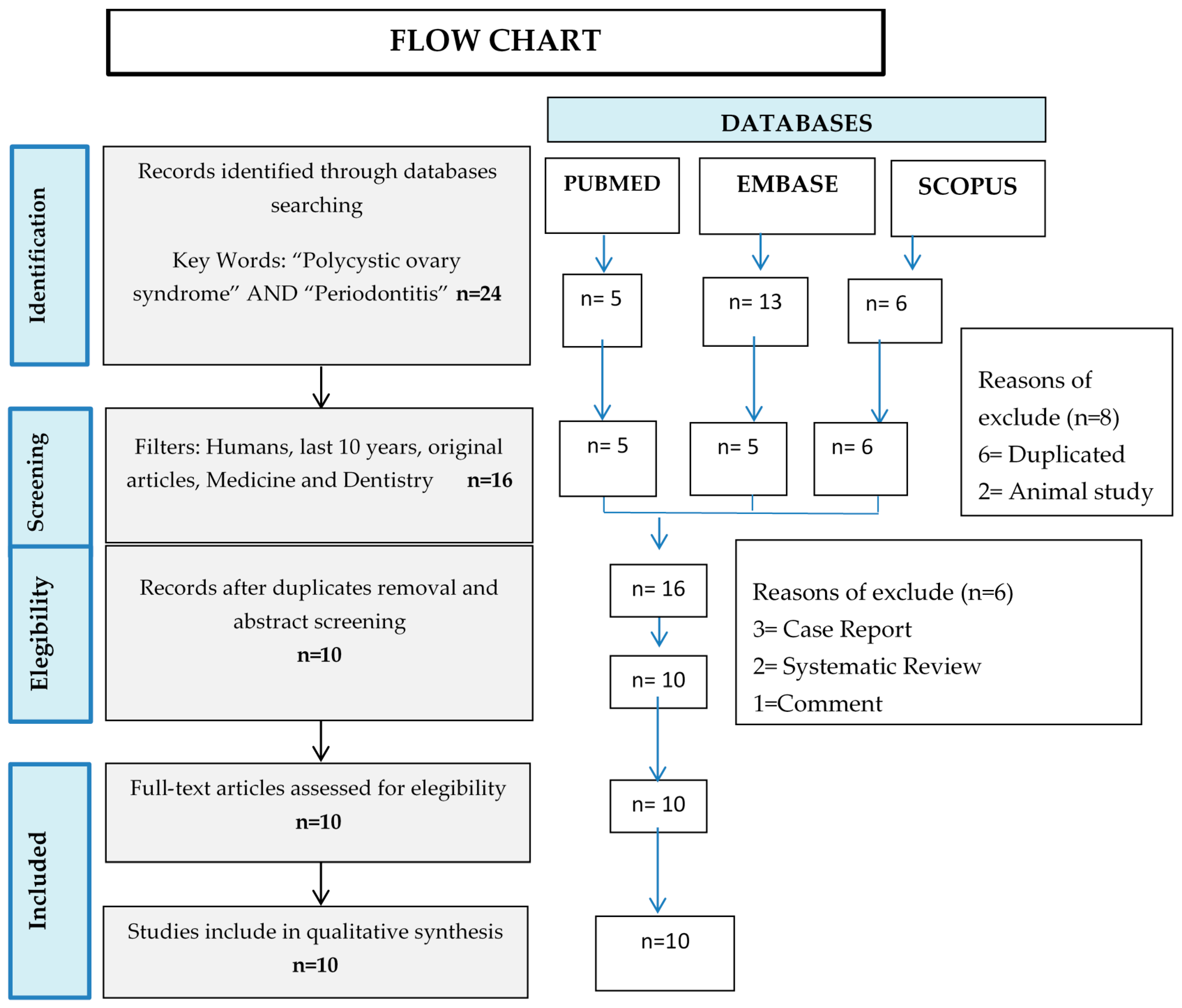
2.2. Selection of Articles
2.3. Quality of Articles
3. Results
3.1. PCOS Diagnostic Criteria
3.2. Periodontal Diagnostic Criteria
3.3. Confounding Variables
3.4. Inflammatory and Oxidative Stress Parameters
3.5. Periodontal Microbiota
3.6. Periodontal Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Khosravi, R.; Ka, K.; Huang, T.; Khalili, S.; Nguyen, B.H.; Nicolau, B.; Tran, S. Tumor Necrosis Factor-α and Interleukin-6: Potential Interorgan Inflammatory Mediators Contributing to Destructive Periodontal Disease in Obesity or Metabolic Syndrome. Mediators Inflamm. 2013, 2013, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudero-Castaño, N.; Perea-García, M.A.; Bascones-Martínez, A. Revisión de la periodontitis crónica: Evolución y su aplicación clínica. Av. Periodoncia Implantol. Oral 2008, 20, 29–34. [Google Scholar]
- Oppermann, R.V.; Weidlich, P.; Musskopf, M.L. Periodontal disease and systemic complications. Braz. Oral Res. 2012, 26, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uriarte, S.M.; Edmisson, J.S.; Jimenez-Flores, E. Human neutrophils and oral microbiota: A constant tug-of-war between a harmonious and a discordant coexistence. Immunol. Rev. 2016, 273, 282–298. [Google Scholar] [CrossRef]
- Hajishengallis, G. The inflammophilic character of the periodontitis-associated microbiota. Mol. Oral Microbiol. 2014, 29, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 19, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-Y.; Tang, C.Y.; Tan, T.-S.; Chen, K.-H.; Liao, K.-H.; Liou, M.-L. Subgingival microbiota in individuals with severe chronic periodontitis. J. Microbiol. Immunol. Infect. 2016, 51, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Wisse, B.E. The Inflammatory Syndrome: The Role of Adipose Tissue Cytokines in Metabolic Disorders Linked to Obesity. J. Am. Soc. Nephrol. 2004, 15, 2792–2800. [Google Scholar] [CrossRef] [Green Version]
- Bullon, P.; Newman, H.N.; Battino, M. Obesity, diabetes mellitus, atherosclerosis and chronic periodontitis: A shared pathology via oxidative stress and mitochondrial dysfunction? Periodontology 2000 2014, 64, 139–153. [Google Scholar] [CrossRef]
- Borrell, L.N.; Papapanou, P.N. Analytical epidemiology of periodontitis. J. Clin. Periodontol. 2005, 32, 132–158. [Google Scholar] [CrossRef]
- Linden, G.J.; Lyons, A.; Scannapieco, F.A. Periodontal systemic associations: Review of the evidence. J. Clin. Periodontol. 2013, 40, S8–S19. [Google Scholar] [CrossRef] [PubMed]
- Kakoly, N.; Moran, L.; Teede, H.; Joham, A. Cardiometabolic risks in PCOS: A review of the current state of knowledge. Expert Rev. Endocrinol. Metab. 2019, 14, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Victor, V.M.; Rocha, M.; Bañuls, C.; Alvarez, A.; De Pablo, C.; Sanchez-Serrano, M.; Gomez, M.; Hernandez-Mijares, A. Induction of Oxidative Stress and Human Leukocyte/Endothelial Cell Interactions in Polycystic Ovary Syndrome Patients with Insulin Resistance. J. Clin. Endocrinol. Metab. 2011, 96, 3115–3122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza dos Santos, A.C.; Soares, N.P.; Costa, E.C.; de Sá, J.C.F.; Azevedo, G.D.; Lemos, T.M.A.M. The impact of body mass on inflammatory markers and insulin resistance in polycystic ovary syndrome. Gynecol. Endocrinol. 2015, 31, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Victor, V.M.; Rovira-Llopis, S.; Bañuls, C.; Diaz-Morales, N.; Martinez de Marañon, A.; Rios-Navarro, C.; Alvarez, A.; Gomez, M.; Rocha, M.; Hernández-Mijares, A. Insulin Resistance in PCOS Patients Enhances Oxidative Stress and Leukocyte Adhesion: Role of Myeloperoxidase. PLoS ONE 2016, 11, e0151960. [Google Scholar] [CrossRef] [PubMed]
- Porwal, S.; Tewari, S.; Sharma, R.K.; Singhal, S.R.; Narula, S.C. Periodontal Status and High-Sensitivity C-Reactive Protein Levels in Polycystic Ovary Syndrome with and without Medical Treatment. J. Periodontol. 2014, 85, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Herrera, M.; Silvestre, F.J.; Silvestre-Rangil, J.; Bañuls, C.; Rocha, M.; Hernández-Mijares, A. Involvement of insulin resistance in normoglycaemic obese patients with periodontitis: A cross-sectional study. J. Clin. Periodontol. 2017, 44, 981–988. [Google Scholar] [CrossRef]
- Özçaka, Ö.; Buduneli, N.; Ceyhan, B.O.; Akcali, A.; Biçakci, N.; Lappin, D.F.; Buduneli, N. Is Interleukin-17 Involved in the Interaction between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2013, 84, 1827–1837. [Google Scholar]
- Hutton, B.; Catalá-López, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, J.S.W.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- CASP. Clinical Appraisal Skills Program Chort Study Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Case-Control-Study-Checklist-2018.pdf (accessed on 12 January 2019).
- CASP. Clinical Appraisal Skills Program Randomised Controlled Trial. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Randomised-Controlled-Trial-Checklist-2018.pdf (accessed on 12 January 2019).
- Dursun, E.; Akaln, F.A.; Güncü, G.N.; Çınar, N.; Aksoy, D.Y.; Tözüm, T.F.; Kılınc, K.; Yıldız, B.O. Periodontal disease in polycystic ovary syndrome. Fertil. Steril. 2011, 95, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Özçaka, Ö.; Ceyhan, B.Ö.; Akcali, A.; Biçakci, N.; Lappin, D.F.; Buduneli, N. Is There an Interaction Between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2012, 83, 1529–1537. [Google Scholar] [CrossRef]
- Akcali, A.; Bostanci, N.; Özçaka, Ö.; Öztürk-Ceyhan, B.; Gümüş, P.; Buduneli, N.; Belibasakis, G.N. Association between polycystic ovary syndrome, oral microbiota and systemic antibody responses. PLoS ONE 2014, 9, e108074. [Google Scholar] [CrossRef] [PubMed]
- Akcall, A.; Bostanci, N.; Özçaka, Ö.; Öztürk-Ceyhan, B.; Gümüş, P.; Tervahartiala, T.; Husu, H.; Buduneli, N.; Sorsa, T.; Belibasakis, G.N. Elevated matrix metalloproteinase-8 in saliva and serum in polycystic ovary syndrome and association with gingival inflammation. Innate Immun. 2015, 21, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Rahiminejad, M.E.; Moaddab, A.; Zaryoun, H.; Rabiee, S.; Moaddab, A.; Khodadoustan, A. Comparison of prevalence of periodontal disease in women with polycystic ovary syndrome and healthy controls. Dent. Res. J. 2015, 12, 507–512. [Google Scholar]
- Akcalı, A.; Bostanci, N.; Özçaka, Ö.; Gümüş, P.; Öztürk-Ceyhan, B.; Tervahartiala, T.; Husu, H.; Buduneli, N.; Sorsa, T.; Belibasakis, G.N. Gingival Inflammation and Salivary or Serum Granulocyte-Secreted Enzymes in Patients with Polycystic Ovary Syndrome. J. Periodontol. 2017, 88, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Saglam, E.; Canakcı, C.F.; Sebin, S.O.; Saruhan, N.; Ingec, M.; Canakci, H.; Sezer, U. Evaluation of Oxidative Status in Patients with Chronic Periodontitis and Polycystic Ovary Syndrome: A Cross-Sectional Study. J. Periodontol. 2018, 89, 76–84. [Google Scholar] [CrossRef]
- Deepti; Tewari, S.; Narula, S.C.; Singhal, S.R.; Sharma, R.K. Effect of Non-surgical Periodontal Therapy Along with Myo-Inositol on High Sensitivity C-Reactive Protein and Insulin Resistance in Polycystic Ovary Syndrome Women Having Chronic Periodontitis: A Randomized Controlled Trial. J. Periodontol. 2017, 88, 999–1011. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 Consensus on Diagnostic Criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Azziz, R.; Carmina, E.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Futterweit, W.; Janssen, O.E.; Legro, R.S.; Norman, R.J.; Taylor, A.E.; et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: The complete task force reportTask Force on the Phenotype of the Polycystic Ovary Syndrome of The Androgen Excess and PCOS Society*). Fertil. Steril. 2009, 91, 456–488. [Google Scholar] [CrossRef]
- Figueredo, C.M.S.; Fischer, R.G.; Gustafsson, A. Aberrant Neutrophil Reactions in Periodontitis. J. Periodontol. 2005, 76, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Ylöstalo, P.; Suominen-Taipale, L.; Reunanen, A.; Knuuttila, M. Association between body weight and periodontal infection. J. Clin. Periodontol. 2008, 35, 297–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genco, R.J.; Grossi, S.G.; Ho, A.; Nishimura, F.; Murayama, Y. A Proposed Model Linking Inflammation to Obesity, Diabetes, and Periodontal Infections. J. Periodontol. 2005, 76, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Al Aseri, Z.; Habib, S.S.; Marzouk, A. Predictive value of high sensitivity C-reactive protein on progression to heart failure occurring after the first myocardial infarction. Vasc. Health Risk Manag. 2019, 15, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Herrera, M.; López-Domènech, S.; Silvestre, F.J.; Silvestre-Rangil, J.; Bañuls, C.; Victor, V.M.; Rocha, M. Chronic periodontitis impairs polymorphonuclear leucocyte–endothelium cell interactions and oxidative stress in humans. J. Clin. Periodontol. 2018, 45, 1429–1439. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year | Section A: Are the Results of the Trial Valid? | Section B: What are the Results? | Section C: Will the Results Help Locally? | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Total Quality Score (0–11) | |
| Akcali A., 2014 [25] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Akcali A., 2015 [26] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Akcali A., 2017 [28] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Dursun E., 2011 [23] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Ozcaka O., 2012 [24] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Ozcaka O., 2013 [18] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Porwall S. 2014 [16] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Rahimnejad M., 2015 [27] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Saglam E., 2017 [29] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | 9 |
| Authors, Year | Section A: Are the Results of the Trial Valid? | Section B: What are the Results? | Section C: Will the Results Help Locally? | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Total Quality Score (0–11) | |
| Deepti, 2017 [30] | Yes | Yes | Yes | No | Yes | Yes | Treatment improved statistically (p < 0.05) PI, GI, BOP, PD, CAL. | P < 0.001 (in PI, GI, BOP, PD and CAL) Confidence Interval not available. | No | Yes | Yes | 9 |
| Authors, Year | Study Design | Population | Mean Age in Years | Periodontal Status Diagnostic Methods | PCOS Diagnostic Methods | Confounders Variables Assessed |
|---|---|---|---|---|---|---|
| Akcali A., 2014 [25] | Case–control | N = 125 PCOS-Healthy = 45 PCOS-Gingivitis = 20 Healthy-Controls = 25 Healthy-Gingivitis = 20 | 25.7 | Oral examination, PD, PI, BOP, Work Shop 1999 criteria, saliva and serum samples | Medical History Rotterdam Criteria Ultrasound | BMI > 30 kg/m2, hyperandrogenism, high BP, CVD, DM, hyperprolactinemia, congenital adrenal hyperplasia, thyroid disorder, Cushing’s syndrome, hepatic or renal dysfunction, oral contraceptives, steroid hormones, insulin-sensitizing medications |
| Akcali A., 2015 [26] | Case–control | N = 125 PCOS-Healthy = 45 PCOS-Gingivitis = 20 Healthy-Controls = 25 Healthy-Gingivitis = 20 | 25.7 | Oral examination, PD, PI, BOP, Work Shop 1999 criteria, saliva and serum samples, MMP-8, MMP-I | Medical History Rotterdam Criteria Ultrasound Serum levels | BMI > 30 kg/m2, hyperandrogenism, high BP, CVD, DM, hyperprolactinemia, congenital adrenal hyperplasia, thyroid disorder, Cushing´s syndrome, hepatic or renal dysfunction, oral contraceptives, steroid hormones, insulin-sensitizing medications |
| Akcali A., 2017 [28] | Case–control | N = 125 PCOS-Healthy = 45 PCOS-Gingivitis = 20 Healthy-Controls = 25 Healthy-Gingivitis = 20 | 25.7 | Oral examination, PD, PI, BOP, Work Shop 1999 criteria, saliva and serum samples | Medical History Rotterdam Criteria Ultrasound | BMI > 30 kg/m2, hyperandrogenism, high BP, CVD, DM, hyperprolactinemia, congenital adrenal hyperplasia, thyroid disorder, Cushing´s syndrome, hepatic or renal dysfunction, oral contraceptives, steroid hormones, insulin-sensitizing medications |
| Deepti 2017 [30] | Randomised controlled trail | N = 60 PCOS = 30 Controls = 30 | PCOS = 24.0 Controls = 22.6 | Oral examination, PI, GI, BOP, PD, CAL | Androgen Excess Society/2006 Criteria | Nephrotic syndrome, chronic renal failure, significant CVD, diabetes mellitus, active cancer, smokers and alcohol dependent, antibiotics, oral contraceptives in the last 3 months, periapical pathology/inflammatory conditions, periodontal treatment within 6 months prior to study |
| Dursun E., 2011 [23] | Case–control | N = 52 PCOS-Non-obese = 25 Controls = 27 | PCOS-non-obese = 22.7 Controls = 24.2 | Oral examination, PD, CAL, GI, BOP, PI, Rx, GCF sample, Spectrophotometric, MPO assay | Medical History Rotterdam Criteria Ultrasound Serum levels | BMI > 30 kg/m2, hyperprolactinemia, congenital adrenal hyperplasia, thyroid disorder, Cushing´s syndrome, androgen-secreting tumours, smoking, oral contraceptives |
| Ozcaka O., 2012 [24] | Case–control | N = 73 PCOS-gingivitis = 30 PCOS-healthy = 31 Controls = 12 | PCOS-gingivitis = 23.5 PCOS-healthy = 21.0 Controls = 28.5 | Oral examination, PD, BOP, PI, saliva sample, GCF sample | Medical History Rotterdam Criteria Ultrasound Serum levels Ferriman Gallwey score | BMI > 30 kg/m2, androgen-secreting tumours, congenital adrenal hyperplasia, thyroid disorders, DM, hyperprolactinemia, Cushing´s syndrome, high BP, hepatic and renal dysfunction, oral contraceptives, steroid hormones, insulin-sensitizing drugs, alcohol, smokers |
| Ozcaka O., 2013 [18] | Case–control | N = 73 PCOS-gingivitis = 30 PCOS-healthy = 31 Controls = 12 | PCOS-gingivitis = 23.5 PCOS-healthy = 21.0 Controls = 28.5 | Oral examination, PD, BOP, PI, saliva sample, GCF sample, | Medical History Rotterdam Criteria Ultrasound Serum levels Ferriman Gallwey score | BMI > 30 kg/m2, hyperandrogenism, thyroid disorders, hyperprolactinemia, CVD, DM, high BP, oral contraceptives, steroid hormone, insulin-sensitizing drugs |
| Porwal S., 2014 [16] | Case–control | n = 126 PCOS = 41 PCOS-treatment = 45 Healthy controls = 40 | PCOS = 23.1 PCOS-treatment = 22.7 Healthy controls = 23.5 | Oral examination, PD, PI, BOP, CAL, GI | Medical History Rotterdam Criteria Ultrasound Serum levels WC and WHR hsCRP serum level | BMI > 30 kg/m2, thyroid disorders, hyperprolactinemia, androgen-secreting tumours, chronic inflammatory diseases, DM, CVD, cancer, smoking, alcohol, antibiotics, periodontal treatment, aggressive periodontitis |
| Rahimnejad ME., 2015 [27] | Case–control | n = 196 PCOS = 98 Healthy controls = 98 | PCOS = 29.1 Healthy = 28.6 | Oral examination, BOP, PD, CAL, PI, tooth loss American Academy of Periodontology Criteria | Medical History Rotterdam Criteria Ultrasound Serum levels | BMI > 25 kg/m2, pregnancy, osteoporosis, antibiotics, smoking, periodontal treatment, malignancies |
| Saglam E., 2017 [29] | Case–control | n = 88 PCOS without CP = 22 PCOS with CP = 22 Healthy with CP = 22 Healthy without CP = 22 | PCOS without CP = 27.6 PCOS with CP = 28.6 Healthy with CP = 28.2 Healthy without CP = 27.8 | Oral examination, PD, CAL, GI, PI, BOP MDA level 8-OHdG level TAS | Medical History Rotterdam Criteria Ultrasound Serum levels WC and WHR | BMI > 25 kg/m2, HbA1c > 6,5%, OGTT-2h > 200 mg/dL, not taken medication within the previous 3 months including antibiotics, oral contraceptives, steroid hormones, hypertensive medications, insulin-sensitizing drugs, periodontal therapy in the previous 6 months, androgen-secreting tumours, congenital adrenal hyperplasia, thyroid disorders, DM, hyperprolactinemia, Cushing´s syndrome |
| Altered Parameters in Patients with PCOS and Periodontal Disease | |||
|---|---|---|---|
| Authors | Clinical | Immunoinflammatory | Microbiological |
| Akcali A., 2014 [25] | PD, BOP, PI | NA | Saliva: Porphyromona. gingivalis Fusobacterium nucleatum Serum antibodies: Prevotella. intermedia, Porphyromona gingivalis, Streptococcus oralis |
| Akcali A., 2015 [26] | PD, BOP, PI | MMP-8/TIMP-1 ratio | NA |
| Akcali A., 2017 [28] | PD, BOP, PI | Salivary MMP-9 and neutrophil elastase, MMP-9/TIMP-1 ratio Serum MMP-9 and MPO | NA |
| Deepti 2017 [30] | PD, BOP, PI, CAL, GI | Serum hsCRP | NA |
| Dursun E. 2011 [23] | PD, GI, BOP, PI | MPO and NO in GCF | NA |
| Ozcaka O., 2012 [24] | PD, BOP, PI | IL-6 in GCF, saliva and serum, TNFα in saliva | NA |
| Ozcaka O., 2013 [18] | PD, BOP, PI | IL-17A, IL-F and IL-A/F in serum, IL-17A and IL-17F in GCF and saliva | NA |
| Porwall S., 2014 [16] | PD, BOP, CAL PCOS newly diagnosed without medical treatment had 2.88 times increased likelihood of having moderate periodontitis. | hsCRP | NA |
| Rahimnejad ME., 2015 [27] | BOP, PI, CAL | NA | NA |
| Saglam E., 2017 [29] | PD, BOP, PI, CAL, GI | Serum and salivary 8-OHdG, MDA and TAS levels | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Márquez-Arrico, C.F.; Silvestre-Rangil, J.; Gutiérrez-Castillo, L.; Martinez-Herrera, M.; Silvestre, F.J.; Rocha, M. Association between Periodontal Diseases and Polycystic Ovary Syndrome: A Systematic Review. J. Clin. Med. 2020, 9, 1586. https://doi.org/10.3390/jcm9051586
Márquez-Arrico CF, Silvestre-Rangil J, Gutiérrez-Castillo L, Martinez-Herrera M, Silvestre FJ, Rocha M. Association between Periodontal Diseases and Polycystic Ovary Syndrome: A Systematic Review. Journal of Clinical Medicine. 2020; 9(5):1586. https://doi.org/10.3390/jcm9051586
Chicago/Turabian StyleMárquez-Arrico, Cecilia Fabiana, Javier Silvestre-Rangil, Laura Gutiérrez-Castillo, Mayte Martinez-Herrera, Francisco Javier Silvestre, and Milagros Rocha. 2020. "Association between Periodontal Diseases and Polycystic Ovary Syndrome: A Systematic Review" Journal of Clinical Medicine 9, no. 5: 1586. https://doi.org/10.3390/jcm9051586