Rethinking Radical Surgery in Interval Debulking Surgery for Advanced-Stage Ovarian Cancer Patients Undergoing Neoadjuvant Chemotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Treatment
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Effects of Disease Burden, SCS, and Residual Disease on Survival
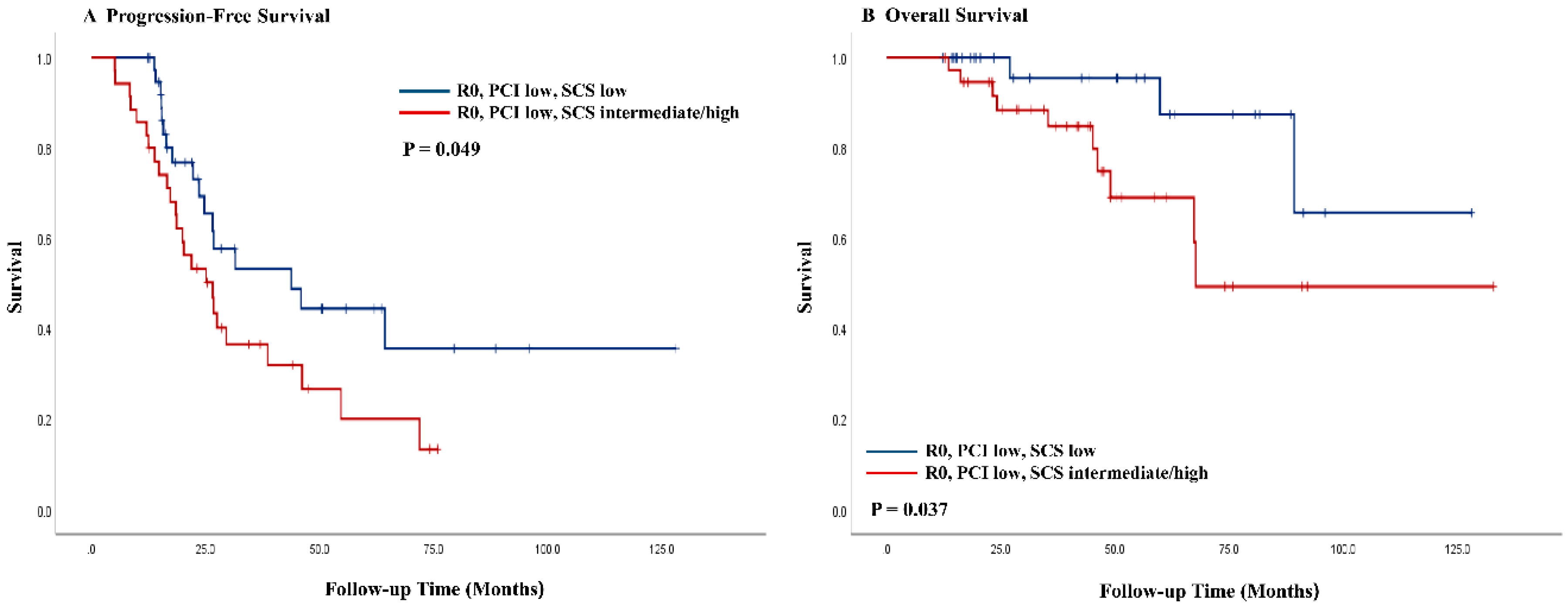
3.3. SCS on Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sant, M.; Chirlaque Lopez, M.D.; Agresti, R.; Sanchez Perez, M.J.; Holleczek, B.; Bielska-Lasota, M.; Dimitrova, N.; Innos, K.; Katalinic, A.; Langseth, H.; et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: Results of the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2191–2205. [Google Scholar] [CrossRef] [PubMed]
- Chi, D.S.; Eisenhauer, E.L.; Zivanovic, O.; Sonoda, Y.; Abu-Rustum, N.R.; Levine, D.A.; Guile, M.W.; Bristow, R.E.; Aghajanian, C.; Barakat, R.R. Improved progression-free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol. Oncol. 2009, 114, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. Am. J. Obstet. Gynecol. 2007, 197, 671.e1–676.e7. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Dowdy, S.C.; Gostout, B.S.; Jones, M.B.; Stanhope, C.R.; Wilson, T.O.; Podratz, K.C.; Cliby, W.A. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obstet. Gynecol. 2006, 107, 77–85. [Google Scholar] [CrossRef]
- Eisenhauer, E.L.; Abu-Rustum, N.R.; Sonoda, Y.; Levine, D.A.; Poynor, E.A.; Aghajanian, C.; Jarnagin, W.R.; DeMatteo, R.P.; D’Angelica, M.I.; Barakat, R.R.; et al. The addition of extensive upper abdominal surgery to achieve optimal cytoreduction improves survival in patients with stages IIIC-IV epithelial ovarian cancer. Gynecol. Oncol. 2006, 103, 1083–1090. [Google Scholar] [CrossRef]
- Crawford, S.C.; Vasey, P.A.; Paul, J.; Hay, A.; Davis, J.A.; Kaye, S.B. Does aggressive surgery only benefit patients with less advanced ovarian cancer? Results from an international comparison within the SCOTROC-1. Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 8802–8811. [Google Scholar] [CrossRef]
- Horowitz, N.S.; Miller, A.; Rungruang, B.; Richard, S.D.; Rodriguez, N.; Bookman, M.A.; Hamilton, C.A.; Krivak, T.C.; Maxwell, G.L. Does aggressive surgery improve outcomes? Interaction between preoperative disease burden and complex surgery in patients with advanced-stage ovarian cancer: An analysis of GOG 182. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 937–943. [Google Scholar] [CrossRef]
- Onda, T.; Matsumoto, K.; Shibata, T.; Sato, A.; Fukuda, H.; Konishi, I.; Kamura, T.; Yoshikawa, H. Phase III trial of upfront debulking surgery versus neoadjuvant chemotherapy for stage III/IV ovarian, tubal and peritoneal cancers: Japan Clinical Oncology Group Study JCOG0602. Jpn. J. Clin. Oncol. 2008, 38, 74–77. [Google Scholar] [CrossRef]
- Vergote, I.; Trope, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.; van der Burg, M.E.; Lacave, A.J.; Panici, P.B.; et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Fagotti, A.; Ferrandina, G.; Vizzielli, G.; Fanfani, F.; Gallotta, V.; Chiantera, V.; Costantini, B.; Margariti, P.A.; Gueli Alletti, S.; Cosentino, F.; et al. Phase III randomised clinical trial comparing primary surgery versus neoadjuvant chemotherapy in advanced epithelial ovarian cancer with high tumour load (SCORPION trial): Final analysis of peri-operative outcome. Eur. J. Cancer 2016, 59, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.A.; Broadwater, G.; Crim, A.; Boccacio, R.; Bixel, K.; Backes, F.; Previs, R.A.; Salinaro, J.; Salani, R.; Moore, K.; et al. Surgical complexity score and role of laparoscopy in women with advanced ovarian cancer treated with neoadjuvant chemotherapy. Gynecol. Oncol. 2019, 152, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, M.; van der Hel, O.; Sonke, G.S.; Van de Vijver, K.K.; van der Aa, M.A.; Kruitwagen, R.F. The prognostic value of residual disease after neoadjuvant chemotherapy in advanced ovarian cancer; A systematic review. Gynecol. Oncol. 2019, 153, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Chung, Y.S.; Lee, J.Y.; Nam, E.J.; Kim, S.W.; Kim, S.; Kim, Y.T. Impact of increased utilization of neoadjuvant chemotherapy on survival in patients with advanced ovarian cancer: Experience from a comprehensive cancer center. J. Gynecol. Oncol. 2018, 29, e63. [Google Scholar] [CrossRef]
- Harmon, R.L.; Sugarbaker, P.H. Prognostic indicators in peritoneal carcinomatosis from gastrointestinal cancer. Int. Semin. Surg. Oncol. ISSO 2005, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Aletti, G.D.; Eisenhauer, E.L.; Santillan, A.; Axtell, A.; Aletti, G.; Holschneider, C.; Chi, D.S.; Bristow, R.E.; Cliby, W.A. Identification of patient groups at highest risk from traditional approach to ovarian cancer treatment. Gynecol. Oncol. 2011, 120, 23–28. [Google Scholar] [CrossRef]
- Chang, S.J.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. Role of aggressive surgical cytoreduction in advanced ovarian cancer. J. Gynecol. Oncol. 2015, 26, 336–342. [Google Scholar] [CrossRef] [Green Version]
- Eisenkop, S.M.; Spirtos, N.M.; Friedman, R.L.; Lin, W.C.; Pisani, A.L.; Perticucci, S. Relative influences of tumor volume before surgery and the cytoreductive outcome on survival for patients with advanced ovarian cancer: A prospective study. Gynecol. Oncol. 2003, 90, 390–396. [Google Scholar] [CrossRef]
- Harter, P.; Muallem, Z.M.; Buhrmann, C.; Lorenz, D.; Kaub, C.; Hils, R.; Kommoss, S.; Heitz, F.; Traut, A.; du Bois, A. Impact of a structured quality management program on surgical outcome in primary advanced ovarian cancer. Gynecol. Oncol. 2011, 121, 615–619. [Google Scholar] [CrossRef]
- Chang, S.J.; Bristow, R.E.; Ryu, H.S. Impact of complete cytoreduction leaving no gross residual disease associated with radical cytoreductive surgical procedures on survival in advanced ovarian cancer. Ann. Surg. Oncol. 2012, 19, 4059–4067. [Google Scholar] [CrossRef]
- Rouzier, R.; Gouy, S.; Selle, F.; Lambaudie, E.; Floquet, A.; Fourchotte, V.; Pomel, C.; Colombo, P.E.; Kalbacher, E.; Martin-Francoise, S.; et al. Efficacy and safety of bevacizumab-containing neoadjuvant therapy followed by interval debulking surgery in advanced ovarian cancer: Results from the ANTHALYA trial. Eur. J. Cancer 2017, 70, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohm, S.; Montfort, A.; Pearce, O.M.; Topping, J.; Chakravarty, P.; Everitt, G.L.; Clear, A.; McDermott, J.R.; Ennis, D.; Dowe, T.; et al. Neoadjuvant Chemotherapy Modulates the Immune Microenvironment in Metastases of Tubo-Ovarian High-Grade Serous Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2016, 22, 3025–3036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.; Kim, J.W.; Lim, M.C.; Kim, S.; Kim, H.S.; Choi, C.H.; Yi, J.Y.; Park, S.Y.; Kim, B.G. A phase II study of neoadjuvant chemotherapy plus durvalumab and tremelimumab in advanced-stage ovarian cancer: A Korean Gynecologic Oncology Group Study (KGOG 3046), TRU-D. J. Gynecol. Oncol. 2019, 30, e112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagotti, A.; Gueli Alletti, S.; Corrado, G.; Cola, E.; Vizza, E.; Vieira, M.; Andrade, C.E.; Tsunoda, A.; Favero, G.; Zapardiel, I.; et al. The INTERNATIONAL MISSION study: Minimally invasive surgery in ovarian neoplasms after neoadjuvant chemotherapy. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.Y.; Yang, Y.C.; Chen, T.C.; Chen, J.R.; Chen, Y.J.; Wu, M.H.; Jan, Y.T.; Chang, C.L.; Lee, J. Muscle loss during primary debulking surgery and chemotherapy predicts poor survival in advanced-stage ovarian cancer. J. Cachexia Sarcopenia Muscle 2020, 11, 534–546. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.I.; Kim, T.M.; Lee, M.; Kim, H.S.; Chung, H.H.; Cho, J.Y.; Song, Y.S. Impact of CT-Determined Sarcopenia and Body Composition on Survival Outcome in Patients with Advanced-Stage High-Grade Serous Ovarian Carcinoma. Cancers 2020, 12, 559. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Burden | SCS | ||||||
|---|---|---|---|---|---|---|---|
| PCI ≤ 6 (n = 123) | PCI > 6 (n = 145) | p | Low (n = 52) | Intermediate (n = 141) | High (n = 75) | p | |
| Age, median (range), years | 58 (31–80) | 58 (31–78) | 0.624 | 59 (38–76) | 58 (31–80) | 56 (31–78) | 0.917 |
| ASA score, n (%) | 0.585 | 0.808 | |||||
| 1 | 21 (17.1%) | 21 (14.5%) | 10 (19.2%) | 24 (17.0%) | 8 (10.7%) | ||
| 2 | 64 (52.0%) | 68 (46.9%) | 26 (50.0%) | 70 (49.7%) | 36 (48.0%) | ||
| 3 | 38 (30.9%) | 54 (37.2%) | 16 (30.8%) | 45 (31.9%) | 31 (41.3%) | ||
| 4 | 0 (0%) | 1 (0.7%) | 0 (0%) | 1 (0.7%) | 0 (0%) | ||
| Not available | 0 (0%) | 1 (0.7%) | 0 (0%) | 1 (0.7%) | 0 (0%) | ||
| CA-125 level, median (range), U/mL | 1474.1 (44.3–30000.0) | 1999.5 (70.9–30000.0) | 0.066 | 1433.2 (44.3–30000.0) | 1758.0 (60.1–30000.0) | 1974.9 (75.2–20685.7) | 0.415 |
| FIGO stage, n (%) | 0.007 | 0.007 | |||||
| III | 68 (55.3%) | 56 (38.6%) | 32 (61.5%) | 67 (47.5%) | 25 (33.3%) | ||
| IV | 55 (44.7%) | 89 (61.4%) | 20 (38.5%) | 74 (52.5%) | 50 (66.7%) | ||
| Histologic type, n (%) | 0.170 | 0.006 | |||||
| HGSC | 117 (95.1%) | 135 (93.1%) | 51 (98.1%) | 134 (95.0%) | 67 (89.4%) | ||
| Endometrioid | 2 (1.6%) | 0 (0%) | 1 (1.9%) | 1 (0.7%) | 0 (0%) | ||
| Mucinous | 0 (0%) | 2 (1.4%) | 0 (0%) | 1 (0.7%) | 1 (1.3%) | ||
| Clear cell | 1 (0.8%) | 5 (3.4%) | 0 (0%) | 0 (0%) | 6 (8.0%) | ||
| Others | 3 (2.5%) | 3 (2.1%) | 0 (0%) | 5 (3.6%) | 1 (1.3%) | ||
| Grading | 0.172 | 0.092 | |||||
| 1 | 2 (1.6%) | 3 (2.1%) | 0 (0%) | 5 (3.5%) | 0 (0%) | ||
| 2 | 12 (9.8%) | 18 (12.4%) | 5 (9.6%) | 14 (9.9%) | 11 (14.7%) | ||
| 3 | 94 (76.4%) | 117 (80.7%) | 39 (75.0%) | 111 (78.7%) | 61 (81.3%) | ||
| Not available | 15 (12.2%) | 7 (4.8%) | 8 (15.4%) | 11 (7.8%) | 3 (4.0%) | ||
| Residual disease, n (%) | <0.001 | 0.001 | |||||
| 0 | 75 (61.0%) | 48 (33.1%) | 36 (69.2%) | 58 (41.1%) | 29 (38.7%) | ||
| <1 cm | 48 (39.0%) | 97 (66.9%) | 16 (30.8%) | 83 (58.9%) | 46 (61.3%) | ||
| SCS | <0.001 | ||||||
| Low (≤3) | 47 (38.2%) | 5 (3.4%) | - | - | - | ||
| Intermediate (4–7) | 63 (51.2%) | 78 (53.8%) | - | - | - | ||
| High (≥8) | 13 (10.6%) | 62 (42.8%) | - | - | - | ||
| Disease burden | <0.001 | ||||||
| PCI ≤ 6 | - | - | 47 (90.4%) | 63 (44.7%) | 13 (17.3%) | ||
| PCI > 6 | - | - | 5 (9.6%) | 78 (55.3%) | 62 (82.7%) | ||
| Variables | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Age, years | ||||||||
| ≤58 | 1 | 1 | 1 | 1 | ||||
| >58 | 1.05 (0.78–1.41) | 0.736 | 1.04 (0.75–1.45) | 0.810 | 1.09 (0.74–1.62) | 0.656 | 1.14 (0.75–1.74) | 0.536 |
| ASA score | ||||||||
| 1–2 | 1 | 1 | 1 | 1 | ||||
| 3–4 | 3.14 (0.43–22.66) | 0.257 | 3.04 (0.41–22.57) | 0.276 | 2.38 (0.33–17.26) | 0.391 | 1.69 (1.07–2.68) | 0.026 |
| FIGO stage | ||||||||
| III | 1 | 1 | 1 | 1 | ||||
| IV | 1.84 (1.36–2.49) | <0.001 | 1.70 (1.25–2.32) | 0.001 | 1.32 (0.88–1.97) | 0.177 | 1.18 (0.77–1.81) | 0.444 |
| Histology | ||||||||
| HGSC | 1 | 1 | 1 | 1 | ||||
| Non-HGSC | 0.75 (0.33–1.71) | 0.497 | 0.76 (0.33–1.72) | 0.759 | 1.95 (0.90–4.21) | 0.089 | 2.09 (0.95–4.64) | 0.069 |
| Residual disease x SCS | ||||||||
| R0, SCS low | 1 | 1 | 1 | 1 | ||||
| R0, SCS intermediate/high | 1.44 (0.88–2.34) | 0.144 | 1.80 (1.05–3.10) | 0.034 | 2.00 (0.93–4.33) | 0.075 | 5.59 (1.70–18.39) | 0.005 |
| MR, SCS low | 3.39 (1.17–9.80) | 0.024 | 2.25 (1.07–4.74) | 0.034 | 7.15 (2.19–23.38) | 0.001 | 9.92 (2.67–36.90) | 0.001 |
| MR, SCS intermediate/high | 3.02 (1.94–4.70) | <0.001 | 2.94 (1.74–4.97) | <0.001 | 3.98 (1.97–8.03) | <0.001 | 8.91 (2.78–28.63) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.J.; Lee, J.-Y.; Nam, E.J.; Kim, S.W.; Kim, S.; Kim, Y.T. Rethinking Radical Surgery in Interval Debulking Surgery for Advanced-Stage Ovarian Cancer Patients Undergoing Neoadjuvant Chemotherapy. J. Clin. Med. 2020, 9, 1235. https://doi.org/10.3390/jcm9041235
Lee YJ, Lee J-Y, Nam EJ, Kim SW, Kim S, Kim YT. Rethinking Radical Surgery in Interval Debulking Surgery for Advanced-Stage Ovarian Cancer Patients Undergoing Neoadjuvant Chemotherapy. Journal of Clinical Medicine. 2020; 9(4):1235. https://doi.org/10.3390/jcm9041235
Chicago/Turabian StyleLee, Yong Jae, Jung-Yun Lee, Eun Ji Nam, Sang Wun Kim, Sunghoon Kim, and Young Tae Kim. 2020. "Rethinking Radical Surgery in Interval Debulking Surgery for Advanced-Stage Ovarian Cancer Patients Undergoing Neoadjuvant Chemotherapy" Journal of Clinical Medicine 9, no. 4: 1235. https://doi.org/10.3390/jcm9041235