Incident Comorbidities, Aging and the Risk of Stroke in 608,108 Patients with Atrial Fibrillation: A Nationwide Analysis

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Baseline, Follow-Up, Delta CHA2DS2-VASc Scores, and Its Slope
2.3. Statistical Analyses
2.4. Data Access
3. Results
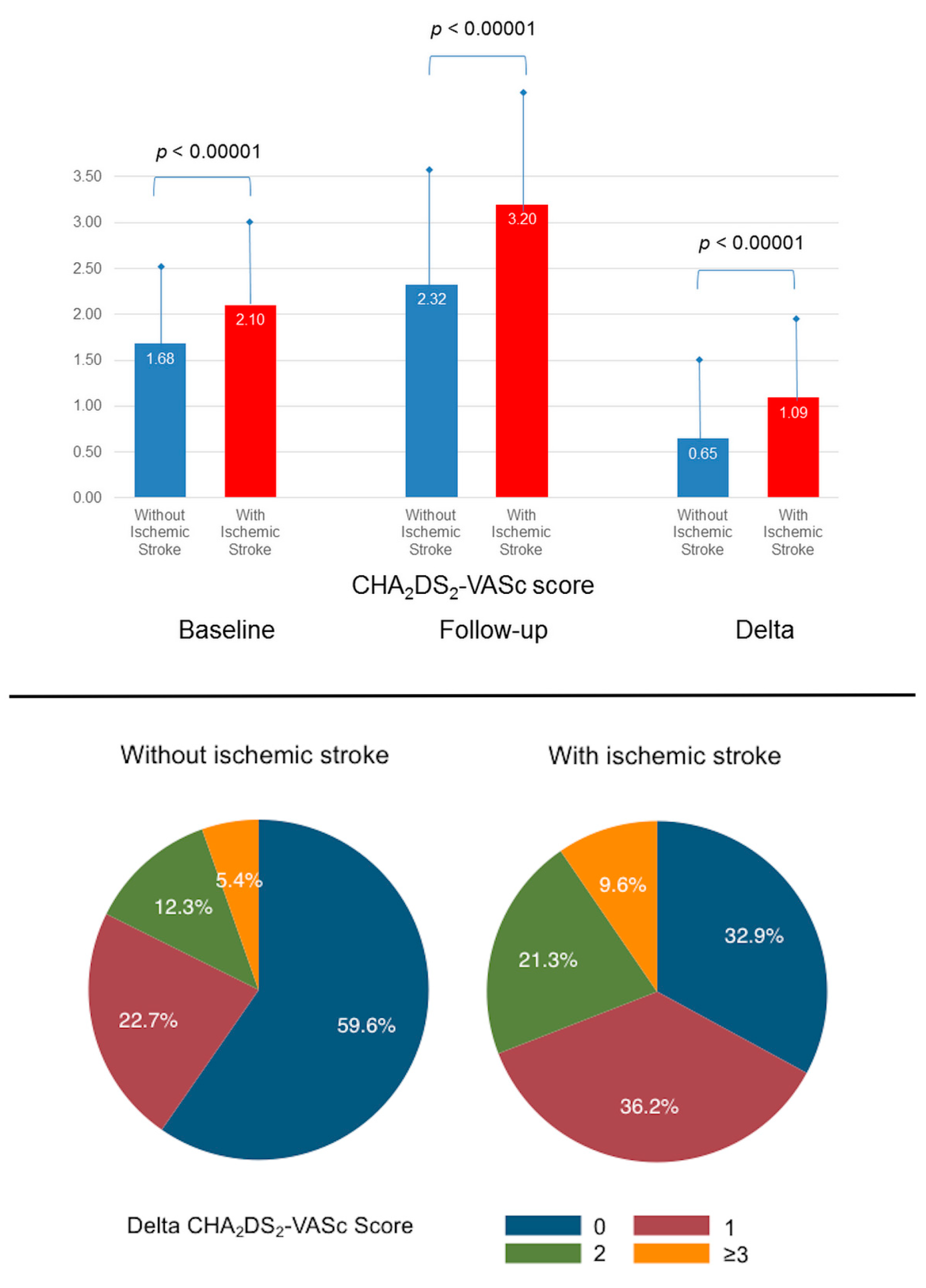
3.1. Baseline, Follow-Up and Delta CHA2DS2-VASc Scores, and the Risk of Ischemic Stroke
3.2. Slope of the Change in CHA2DS2-VASc Score
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Lip, G.Y.H.; Freedman, B.; De Caterina, R.; Potpara, T.S. Stroke prevention in atrial fibrillation: Past, present and future. Comparing the guidelines and practical decision-making. Thromb. Haemost. 2017, 117, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.F.; Lip, G.Y.H.; Liu, C.J.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P.; et al. Relationship of aging and incident comorbidities to stroke risk in patients with atrial fibrillation. J. Am. Coll. Cardiol. 2018, 71, 122–132. [Google Scholar] [CrossRef]
- Yoon, M.; Yang, P.S.; Jang, E.; Yu, H.T.; Kim, T.H.; Uhm, J.S.; Kim, J.Y.; Pak, H.N.; Lee, M.H.; Lip, G.Y.H.; et al. Dynamic changes of cha2ds2-vasc score and the risk of ischaemic stroke in asian patients with atrial fibrillation: A nationwide cohort study. Thromb. Haemost. 2018, 118, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Chantry, A.A.; Deneux-Tharaux, C.; Cans, C.; Ego, A.; Quantin, C.; Bouvier-Colle, M.-H.; Group, G.S. Hospital discharge data can be used for monitoring procedures and intensive care related to severe maternal morbidity. J. Clin. Epidemiol. 2011, 64, 1014–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorgis, L.; Cottenet, J.; Molins, G.; Benzenine, E.; Zeller, M.; Aube, H.; Touzery, C.; Hamblin, J.; Gudjoncik, A.; Cottin, Y.; et al. Outcomes after acute myocardial infarction in hiv-infected patients: Analysis of data from a french nationwide hospital medical information database. Circulation 2013, 127, 1767–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauchier, L.; Clementy, N.; Pelade, C.; Collignon, C.; Nicolle, E.; Lip, G.Y. Patients with ischemic stroke and incident atrial fibrillation: A nationwide cohort study. Stroke 2015, 46, 2432–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauchier, L.; Chaize, G.; Gaudin, A.F.; Vainchtock, A.; Rushton-Smith, S.K.; Cotte, F.E. Predictive ability of has-bled, hemorr2hages, and atria bleeding risk scores in patients with atrial fibrillation. A french nationwide cross-sectional study. Int. J. Cardiol. 2016, 217, 85–91. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A novel user-friendly score (has-bled) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The euro heart survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [Green Version]
- Chao, T.F.; Lip, G.Y.H.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P.; Chen, T.J.; et al. Incident risk factors and major bleeding in patients with atrial fibrillation treated with oral anticoagulants: A comparison of baseline, follow-up and delta has-bled scores with an approach focused on modifiable bleeding risk factors. Thromb. Haemost. 2018, 118, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Kokotailo, R.A.; Hill, M.D. Coding of stroke and stroke risk factors using international classification of diseases, revisions 9 and 10. Stroke 2005, 36, 1776–1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norberg, J.; Backstrom, S.; Jansson, J.H.; Johansson, L. Estimating the prevalence of atrial fibrillation in a general population using validated electronic health data. Clin. Epidemiol. 2013, 5, 475–481. [Google Scholar] [PubMed] [Green Version]
- Porter, J.; Mondor, L.; Kapral, M.K.; Fang, J.; Hall, R.E. How reliable are administrative data for capturing stroke patients and their care. Cerebrovasc. Dis. Extra 2016, 6, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Proietti, M.; Laroche, C.; Fauchier, L.; Marin, F.; Nabauer, M.; Potpara, T.; Dan, G.A.; Kalarus, Z.; Diemberger, I.; et al. Contemporary stroke prevention strategies in 11 096 european patients with atrial fibrillation: A report from the eurobservational research programme on atrial fibrillation (eorp-af) long-term general registry. Europace 2018, 20, 747–757. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | No Ischemic Stroke | Ischemic Stroke | p | |
|---|---|---|---|---|
| (n = 608108) | (n = 588026) | (n = 20082) | ||
| Characteristics at baseline | ||||
| Age, years | 72.7 ± 14.6 | 72.5 ± 14.6 | 78.3 ± 10.8 | <0.0001 |
| Age 65–74 yrs | 135994 (22.4) | 132380 (22.5) | 3614 (18.0) | <0.0001 |
| Age ≥75 yrs | 313332 (51.5) | 299213 (50.9) | 14119 (70.3) | <0.0001 |
| Gender (male) | 341299 (56.1) | 331608 (56.4) | 9691 (48.3) | <0.0001 |
| CHA2DS2-VASc score | 1.7 ± 1.1 | 1.7 ± 1.1 | 2.1 ± 0.9 | <0.0001 |
| CHA2DS2-VASc score = 0 | 110373 (18.2) | 108728 (18.5) | 1645 (8.2) | <0.0001 |
| CHA2DS2-VASc score = 1 | 131674 (21.7) | 128849 (21.9) | 2825 (14.1) | <0.0001 |
| CHA2DS2-VASc score = 2 | 197673 (32.5) | 190410 (32.4) | 7263 (36.2) | <0.0001 |
| CHA2DS2-VASc score = 3 | 168388 (27.7) | 160039 (27.2) | 8349 (41.6) | <0.0001 |
| Coronary artery disease | 52807 (8.7) | 50744 (8.6) | 2063 (10.3) | <0.0001 |
| Previous pacemaker or Defibrillator | 8317 (1.4) | 8022 (1.4) | 295 (1.5) | 0.21 |
| Smoker | 26202 (4.3) | 25687 (4.4) | 515 (2.6) | <0.0001 |
| Dyslipidemia | 38136 (6.3) | 36967 (6.3) | 1169 (5.8) | 0.01 |
| Obesity | 33410 (5.5) | 32700 (5.6) | 710 (3.5) | <0.0001 |
| Alcohol related diagnoses | 24514 (4.0) | 23803 (4.0) | 711 (3.5) | 0.0003 |
| Abnormal renal function | 10898 (1.8) | 10555 (1.8) | 343 (1.7) | 0.36 |
| Lung disease | 60242 (9.9) | 58721 (10.0) | 1521 (7.6) | <0.0001 |
| Liver disease | 13894 (2.3) | 13572 (2.3) | 322 (1.6) | <0.0001 |
| Thyroid diseases | 39551 (6.5) | 38244 (6.5) | 1307 (6.5) | 0.98 |
| Inflammatory disease | 22307 (3.7) | 21587 (3.7) | 720 (3.6) | 0.52 |
| Anemia | 54504 (9.0) | 52925 (9.0) | 1579 (7.9) | <0.0001 |
| Previous cancer | 93633 (15.4) | 91466 (15.6) | 2167 (10.8) | <0.0001 |
| Characteristics after the follow-up | ||||
| Age, years | 74.8 ± 14.6 | 74.6 ± 14.7 | 80.8 ± 10.8 | <0.0001 |
| Age 65–74 yrs | 128281 (21.1) | 125254 (21.3) | 3027 (15.1) | <0.0001 |
| Age ≥75 yrs | 343328 (56.5) | 328135 (55.8) | 15193 (75.7) | <0.0001 |
| CHA2DS2-VASc score | 2.4 ± 1.5 | 2.3 ± 1.5 | 3.2 ± 1.3 | <0.0001 |
| CHA2DS2-VASc score = 0 | 76845 (12.6) | 76186 (13.0) | 659 (3.3) | <0.0001 |
| CHA2DS2-VASc score = 1 | 100752 (16.6) | 99369 (16.9) | 1383 (6.9) | <0.0001 |
| CHA2DS2-VASc score = 2 | 144335 (23.7) | 140771 (23.9) | 3564 (17.7) | <0.0001 |
| CHA2DS2-VASc score = 3 | 160270 (26.4) | 154124 (26.2) | 6146 (30.6) | <0.0001 |
| CHA2DS2-VASc score = 4 | 78774 (13.0) | 73630 (12.5) | 5144 (25.6) | <0.0001 |
| CHA2DS2-VASc score = 5 | 37770 (6.2) | 35291 (6.0) | 2479 (12.3) | <0.0001 |
| CHA2DS2-VASc score = 6 | 8584 (1.4) | 7941 (1.4) | 643 (3.2) | <0.0001 |
| CHA2DS2-VASc score = 7 | 778 (0.1) | 714 (0.1) | 64 (0.3) | <0.0001 |
| New-onset comorbidities | ||||
| Hypertension | 156081 (25.7) | 146131 (24.9) | 9950 (49.5) | <0.0001 |
| Heart failure | 125684 (20.7) | 119795 (20.4) | 5889 (29.3) | <0.0001 |
| Diabetes mellitus | 27105 (4.5) | 25531 (4.3) | 1574 (7.8) | <0.0001 |
| Vascular disease | 40512 (6.7) | 37503 (6.4) | 3009 (15.0) | <0.0001 |
| Any new-onset comorbidity | 227993 (37.5) | 214952 (36.6) | 13041 (64.9) | <0.0001 |
| Delta CHA2DS2-VASc score | 0.7 ± 0.9 | 0.6 ± 0.9 | 1.1 ± 1.0 | <0.0001 |
| Delta CHA2DS2-VASc score = 0 | 357349 (58.8) | 350738 (59.6) | 6611 (32.9) | <0.0001 |
| Delta CHA2DS2-VASc score = 1 | 140768 (23.1) | 133503 (22.7) | 7265 (36.2) | <0.0001 |
| Delta CHA2DS2-VASc score = 2 | 76373 (12.6) | 72090 (12.3) | 4283 (21.3) | <0.0001 |
| Delta CHA2DS2-VASc score = 3 | 27067 (4.5) | 25498 (4.3) | 1569 (7.8) | <0.0001 |
| Delta CHA2DS2-VASc score = 4 | 5809 (1.0) | 5484 (0.9) | 325 (1.6) | <0.0001 |
| Delta CHA2DS2-VASc score = 5 | 742 (0.1) | 713 (0.1) | 29 (0.1) | 0.36 |
| Delta CHA2DS2-VASc score = 0 | Delta CHA2DS2-VASc score = 1 | Delta CHA2DS2-VASc score = 2 | Delta CHA2DS2-VASc score ≥3 | |
|---|---|---|---|---|
| (n = 357349) | (n = 140768) | (n = 76373) | (n = 33618) | |
| Characteristics at baseline | ||||
| Age, years | 70.7 ± 16.1 | 75.1 ± 12.2 | 76.7 ± 10.8 | 74.6 ± 9.6 |
| Age 65–74 yrs | 75426 (21.1) | 31574 (22.4) | 17578 (23.0) | 11416 (34.0) |
| Age ≥75 yrs | 171231 (47.9) | 79587 (56.5) | 46575 (61.0) | 15939 (47.4) |
| Gender (male) | 200713 (56.2) | 77384 (55.0) | 41750 (54.7) | 21452 (63.8) |
| CHA2DS2-VASc score | 1.6 ± 1.1 | 1.8 ± 1.0 | 1.9 ± 1.0 | 1.6 ± 1.0 |
| CHA2DS2-VASc score = 0 | 76841 (21.5) | 20344 (14.5) | 8444 (11.1) | 4607 (13.7) |
| CHA2DS2-VASc score = 1 | 79937 (22.4) | 28338 (20.1) | 14311 (18.7) | 9081 (27.0) |
| CHA2DS2-VASc score = 2 | 107111 (30.0) | 49157 (34.9) | 28689 (37.6) | 12829 (38.2) |
| CHA2DS2-VASc score = 3 | 93460 (26.2) | 42929 (30.5) | 24929 (32.6) | 7101 (21.1) |
| Coronary artery disease | 18290 (5.1) | 17106 (12.2) | 10545 (13.8) | 6866 (20.4) |
| Previous pacemaker or Defibrillator | 4331 (1.2) | 2237 (1.6) | 1244 (1.6) | 505 (1.5) |
| Smoker | 17859 (5.0) | 5074 (3.6) | 2231 (2.9) | 1038 (3.1) |
| Dyslipidemia | 21218 (5.9) | 9811 (7.0) | 4929 (6.5) | 2178 (6.5) |
| Obesity | 19348 (5.4) | 7493 (5.3) | 4323 (5.7) | 2246 (6.7) |
| Alcohol related diagnoses | 15704 (4.4) | 5050 (3.6) | 2492 (3.3) | 1268 (3.8) |
| Abnormal renal function | 5846 (1.6) | 2733 (1.9) | 1585 (2.1) | 734 (2.2) |
| Lung disease | 35331 (9.9) | 13682 (9.7) | 7692 (10.1) | 3537 (10.5) |
| Liver disease | 8938 (2.5) | 2956 (2.1) | 1407 (1.8) | 593 (1.8) |
| Thyroid diseases | 23446 (6.6) | 9591 (6.8) | 4866 (6.4) | 1648 (4.9) |
| Inflammatory disease | 13299 (3.7) | 5104 (3.6) | 2773 (3.6) | 1131 (3.4) |
| Anemia | 34058 (9.5) | 12223 (8.7) | 6011 (7.9) | 2212 (6.6) |
| Previous cancer | 61422 (17.2) | 20163 (14.3) | 8798 (11.5) | 3250 (9.7) |
| Characteristics after the follow-up | ||||
| Follow-up duration (years) | 1.2 ± 1.9 | 3.0 ± 2.4 | 3.8 ± 2.4 | 4.8 ± 2.3 |
| Age, years | 71.9 ± 15.9 | 78.1 ± 11.9 | 80.5 ± 10.4 | 79.3 ± 9.2 |
| Age 65–74 yrs | 75426 (21.1) | 31250 (22.2) | 14225 (18.6) | 7380 (22.0) |
| Age ≥75 yrs | 171231 (47.9) | 91132 (64.7) | 56420 (73.9) | 24545 (73.0) |
| CHA2DS2-VASc score | 1.6 ± 1.1 | 2.8 ± 1.0 | 3.9±1.0 | 4.9 ± 1.0 |
| CHA2DS2-VASc score = 0 | 76845 (21.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| CHA2DS2-VASc score = 1 | 79940 (22.4) | 20812 (14.8) | 0 (0.0) | 0 (0.0) |
| CHA2DS2-VASc score = 2 | 107108 (30.0) | 28419 (20.2) | 8808 (11.5) | 0 (0.0) |
| CHA2DS2-VASc score = 3 | 93456 (26.2) | 48898 (34.7) | 14432 (18.9) | 3484 (10.4) |
| CHA2DS2-VASc score = 4 | 0 (0.0) | 42639 (30.3) | 28480 (37.3) | 7655 (22.8) |
| CHA2DS2-VASc score = 5 | 0 (0.0) | 0 (0.0) | 24653 (32.3) | 13117 (39.0) |
| CHA2DS2-VASc score = 6 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 8584 (25.5) |
| CHA2DS2-VASc score = 7 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 778 (2.3) |
| Hypertension | 0 (0.0) | 61486 (43.7) | 62627 (82.0) | 31968 (95.1) |
| Heart failure | 0 (0.0) | 45143 (32.1) | 51028 (66.8) | 29513 (87.8) |
| Diabetes mellitus | 0 (0.0) | 4590 (3.3) | 9115 (11.9) | 13400 (39.9) |
| Vascular disease | 0 (0.0) | 6783 (4.8) | 13639 (17.9) | 20090 (59.8) |
| Any new-onset comorbidity | 0 (0.0) | 118002 (83.8) | 76373 (100.0) | 33618 (100.0) |
| Number of Patients | Number of Incident Ischemic Stroke | Incidence of Ischemic Stroke (%/year) | Hazard. Ratio (95%CI) | p | |
|---|---|---|---|---|---|
| Baseline CHA2DS2-VASc score | |||||
| 0 (reference group) | 111,269 | 1687 | 0.67 | 1.00 | |
| 1 | 131,937 | 2852 | 0.91 | 1.35 (1.27–1.43) | <0.0001 |
| 2 | 197,176 | 7238 | 1.69 | 2.54 (2.41–2.68) | <0.0001 |
| 3 | 167,726 | 8305 | 2.52 | 3.80 (3.61–4.01) | <0.0001 |
| Follow-up CHA2DS2-VASc score | |||||
| 0 (reference group) | 76,845 | 659 | 0.60 | 1.00 | |
| 1 | 100,752 | 1383 | 0.77 | 1.30 (1.18–1.42) | <0.0001 |
| 2 | 144,335 | 3564 | 1.34 | 2.25 (2.07–2.44) | <0.0001 |
| 3 | 160,270 | 6146 | 1.91 | 3.20 (2.95–3.47) | <0.0001 |
| 4 | 78,774 | 5144 | 1.98 | 3.38 (3.12–3.67) | <0.0001 |
| ≥5 | 47,132 | 3186 | 1.70 | 2.90 (2.66–3.15) | <0.0001 |
| Delta CHA2DS2-VASc score | |||||
| 0 (reference group) | 357,349 | 6611 | 1.50 | 1.00 | |
| 1 | 140,768 | 7265 | 1.69 | 1.16 (1.12–1.20) | <0.0001 |
| 2 | 76,373 | 4283 | 1.46 | 0.99 (0.96–1.03) | 0.75 |
| 3 | 27,067 | 1569 | 1.27 | 0.85 (0.81–0.90) | <0.0001 |
| ≥4 | 6551 | 354 | 0.99 | 0.65 (0.58–0.72) | <0.0001 |
| No Ischemic Stroke | Ischemic Stroke | p value | Odds Ratio (95% CI) of Ischemic Stroke Per Unit Slope Change | p value | |
|---|---|---|---|---|---|
| (n = 237288) | (n = 13471) | ||||
| Delta CHA2DS2-VASc Score | |||||
| All (≥1) | 0.7 ± 0.8 | 0.9 ± 1.2 | <0.0001 | 1.29 (1.27–1.31) | <0.0001 |
| 1 | 0.7 ± 0.9 | 0.9 ± 1.3 | <0.0001 | 1.22 (1.19–1.24) | <0.0001 |
| 2 | 0.7 ± 0.6 | 0.9 ± 1.2 | <0.0001 | 1.48 (1.44–1.53) | <0.0001 |
| 3 | 0.7 ± 0.5 | 0.9 ± 0.9 | <0.0001 | 1.54 (1.44–1.64) | <0.0001 |
| ≥ 4 | 0.6 ± 0.4 | 0.8 ± 0.8 | <0.0001 | 1.64 (1.37–1.96) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fauchier, L.; Bodin, A.; Bisson, A.; Herbert, J.; Spiesser, P.; Clementy, N.; Babuty, D.; Chao, T.-F.; Lip, G.Y.H. Incident Comorbidities, Aging and the Risk of Stroke in 608,108 Patients with Atrial Fibrillation: A Nationwide Analysis. J. Clin. Med. 2020, 9, 1234. https://doi.org/10.3390/jcm9041234
Fauchier L, Bodin A, Bisson A, Herbert J, Spiesser P, Clementy N, Babuty D, Chao T-F, Lip GYH. Incident Comorbidities, Aging and the Risk of Stroke in 608,108 Patients with Atrial Fibrillation: A Nationwide Analysis. Journal of Clinical Medicine. 2020; 9(4):1234. https://doi.org/10.3390/jcm9041234
Chicago/Turabian StyleFauchier, Laurent, Alexandre Bodin, Arnaud Bisson, Julien Herbert, Pascal Spiesser, Nicolas Clementy, Dominique Babuty, Tze-Fan Chao, and Gregory Y. H. Lip. 2020. "Incident Comorbidities, Aging and the Risk of Stroke in 608,108 Patients with Atrial Fibrillation: A Nationwide Analysis" Journal of Clinical Medicine 9, no. 4: 1234. https://doi.org/10.3390/jcm9041234