Factorial Structure and Validity of Depression (PHQ-9) and Anxiety (GAD-7) Scales after Traumatic Brain Injury


 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Ethical Approval
2.3. Instruments
2.4. Statistical Analysis
3. Results
3.1. Respondents Characteristics
3.2. Descriptive of Variables and Their Reliability
3.3. Factorial Structure of PHQ-ADS
3.4. Factorial Structure Reliability
3.5. Discriminant Validity
3.6. Prevalence, Comorbidity, and Construct Validity
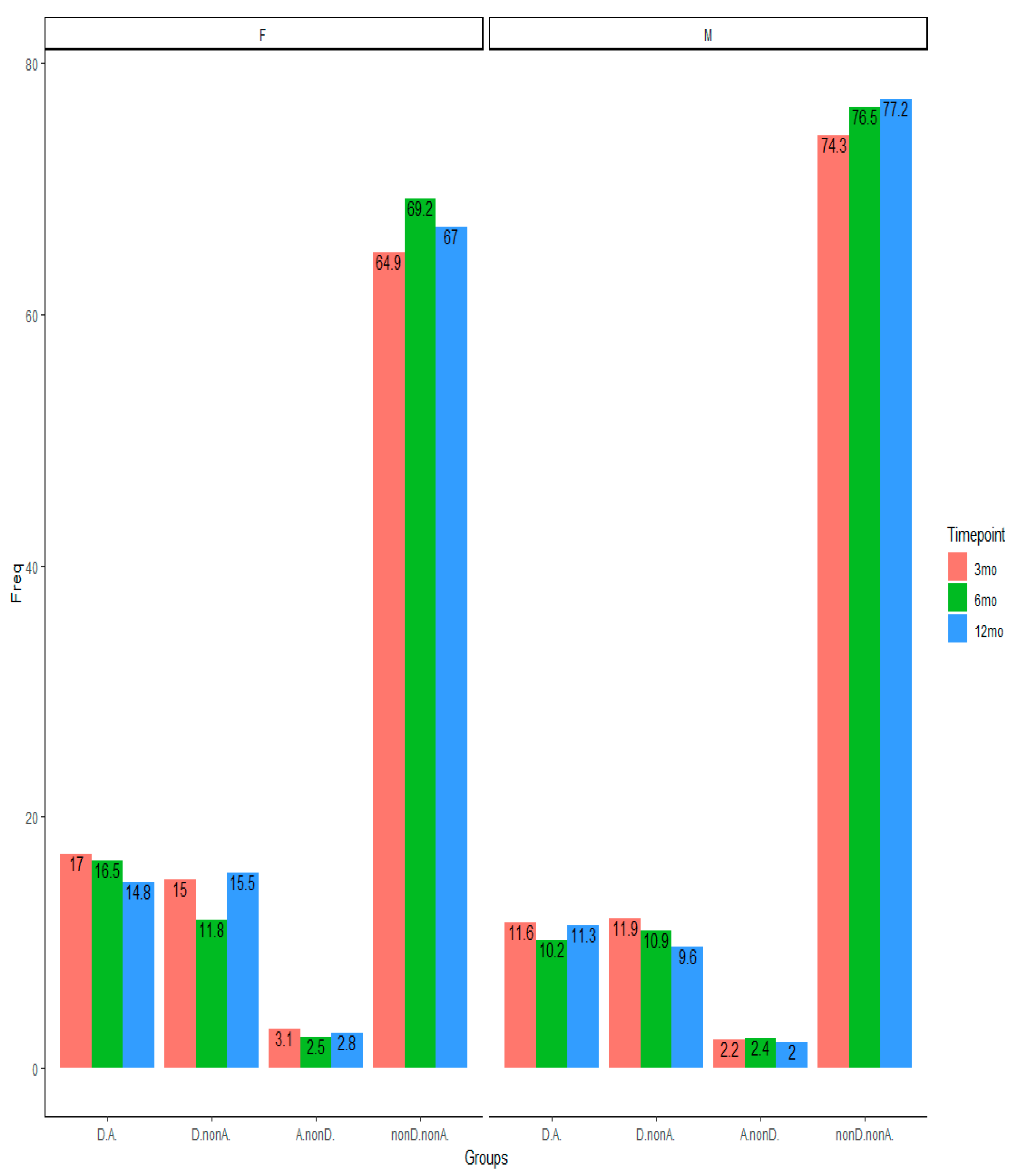
3.7. Predictive Validity and Changes of Depression and Anxiety Over Time
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | S.D. | Min-Max (Q1, Median, Q3) | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|
| GAD7 (Nervous) | 2122 | 0.60 | 0.80 | 0–3 (0, 0, 1) | 1.36 | 1.42 |
| GAD7 (NonStopWorry) | 2120 | 0.52 | 0.83 | 0–3 (0, 0, 1) | 1.61 | 1.81 |
| GAD7 (WorryTooMuch) | 2121 | 0.62 | 0.86 | 0–3 (0, 0, 1) | 1.34 | 1.00 |
| GAD7 (TrblRelax) | 2121 | 0.58 | 0.85 | 0–3 (0, 0, 1) | 1.45 | 1.32 |
| GAD7 (Restless) | 2120 | 0.36 | 0.71 | 0–3 (0, 0, 1) | 2.14 | 4.17 |
| GAD7 (Annoyed) | 2122 | 0.59 | 0.84 | 0–3 (0, 0, 1) | 1.41 | 1.25 |
| GAD7 (Afraid) | 2112 | 0.35 | 0.73 | 0–3 (0, 0, 0) | 2.26 | 4.61 |
| PHQ9 (IntrstPleasrActScre) | 2125 | 0.60 | 0.86 | 0–3 (0, 0, 1) | 1.44 | 1.32 |
| PHQ9 (DwnDeprssnHopelssScre) | 2126 | 0.55 | 0.80 | 0–3 (0, 0, 1) | 1.47 | 1.56 |
| PHQ9 (SleepProbScre) | 2125 | 0.86 | 1.03 | 0–3 (0, 1, 1) | 0.91 | −0.42 |
| PHQ9 (TirdLckEnrgyScre) | 2126 | 1.03 | 0.99 | 0–3 (0, 1, 2) | 0.69 | −0.56 |
| PHQ9 (AppteIssueScre) | 2123 | 0.52 | 0.87 | 0–3 (0, 0, 1) | 1.64 | 1.71 |
| PHQ9 (LowSlfEstmScre) | 2121 | 0.42 | 0.77 | 0–3 (0, 0, 1) | 1.93 | 3.04 |
| PHQ9 (ConcntrtnProbScre) | 2124 | 0.58 | 0.88 | 0–3 (0, 0, 1) | 1.46 | 1.17 |
| PHQ9 (SpdMovmntSpchScre) | 2124 | 0.31 | 0.71 | 0–3 (0, 0, 1) | 2.47 | 5.53 |
| PHQ9 (DthHrtThghtScre) | 2121 | 0.18 | 0.53 | 0–3 (0, 0, 0) | 3.53 | 13.50 |
Appendix B

Appendix C

Appendix D
| Schmid–Leiman | CFA | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Items | Gen. | Anx. | Dep. | Communality | EV | I-ECV | Gen. | Anx. | Dep. | |
| 1. PHQ9Int. | 0.78 | 0.33 | 0.72 | 0.28 | 0.85 | 0.83 *** | 0.15 ** | |||
| 2. PHQ9Dwn. | 0.85 | 0.26 | 0.81 | 0.19 | 0.89 | 0.93 *** | −0.02 | |||
| 3. PHQ9Sle. | 0.57 | 0.28 | 0.41 | 0.59 | 0.80 | 0.59 *** | 0.28 *** | |||
| 4. PHQ9Tir. | 0.73 | 0.38 | 0.68 | 0.32 | 0.78 | 0.76 *** | 0.52 * | |||
| 5. PHQ9App. | 0.64 | 0.32 | 0.50 | 0.50 | 0.80 | 0.67 *** | 0.19 *** | |||
| 6. PHQ9Low. | 0.77 | 0.23 | 0.66 | 0.34 | 0.89 | 0.84 *** | −0.06 | |||
| 7. PHQ9Con. | 0.69 | 0.23 | 0.54 | 0.46 | 0.89 | 0.73 *** | 0.10 * | |||
| 8. PHQ9Spd. | 0.67 | 0.20 | 0.50 | 0.50 | 0.89 | 0.72 *** | −0.02 | |||
| 9. PHQ9Dth. | 0.70 | 0.21 | 0.55 | 0.45 | 0.89 | 0.76 *** | −0.12 | |||
| 10. GAD7Ner. | 0.82 | 0.29 | 0.76 | 0.24 | 0.88 | 0.84 *** | 0.26 *** | |||
| 11. GAD7Non. | 0.83 | 0.39 | 0.85 | 0.15 | 0.82 | 0.81 *** | 0.45 *** | |||
| 12. GAD7Wor. | 0.79 | 0.42 | 0.80 | 0.20 | 0.78 | 0.74 *** | 0.57 *** | |||
| 13. GAD7Trb. | 0.82 | 0.25 | 0.76 | 0.24 | 0.89 | 0.83 *** | 0.26 *** | |||
| 14. GAD7Res. | 0.73 | 0.25 | 0.60 | 0.40 | 0.88 | 0.73 *** | 0.26 *** | |||
| 15. GAD7Ann. | 0.75 | 0.22 | 0.63 | 0.37 | 0.90 | 0.77 *** | 0.18 *** | |||
| 16. GAD7Afr. | 0.72 | 0.31 | 0.62 | 0.38 | 0.84 | 0.72 *** | 0.28 *** | |||
Appendix E

Appendix F
| PHQ9 at 6-Months | GAD7 at 6-Months | |||||
|---|---|---|---|---|---|---|
| 3 months | Beta (ER) | Z | OR (95%CI) | Beta (ER) | Z | OR (95%CI) |
| A.nonD | 0.97 (0.41) | 2.38 *** | 2.64 (1.11–5.61) | 2.25 (0.37) | 6.04 *** | 9.53 (4.45–19.46) |
| D.nonA | 2.44 (0.17) | 14.08 *** | 11.52 (8.22–16.23) | 1.74 (0.23) | 7.67 *** | 5.69 (3.64–8.88) |
| D.A. | 3.33 (0.18) | 18.26 *** | 27.99 (19.69–40.29) | 3.56(0.20) | 17.74 *** | 35.21 (23.93–52.64) |
Appendix G

Appendix H
| 6 Mo | 12 Mo | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3 Mo | nonD.nonA. | A.nonD. | D.nonA. | D.A. | Total | nonD.nonA. | A.nonD. | D.nonA. | D.A. | Total |
| nonD.nonA. | 1035 (90.0) | 18 (1.6) | 67 (5.8) | 30 (2.6) | 1150 | 703 (88.4) | 9 (1.1) | 46 (5.8) | 37 (4.7) | 795 |
| A.nonD. | 27 (65.9) | 6 (14.6) | 2 (4.9) | 6 (14.6) | 41 | 11 (45.8) | 6 (25.0) | 1 (4.2) | 6 (25.0) | 24 |
| D.nonA. | 100 (47.2) | 3 (1.4) | 70 (33.0) | 39 (18.4) | 212 | 66 (44.6) | 4 (2.7) | 51 (35.5) | 27 (18.2) | 148 |
| D.A. | 50 (22.2) | 13 (5.8) | 39 (17.3) | 123 (54.7) | 225 | 32 (25.2) | 8 (6.3) | 24 (18.9) | 63 (49.6) | 127 |
| Total | 1212 (74.4) | 40 (2.5) | 178 (10.9) | 198 (12.2) | 1628 | 812 (74.2) | 27 (2.5) | 122 (11.2) | 133 (12.2) | 1094 |
| 6 Mo | ||||||||||
| nonD.nonA. | - | - | - | - | - | 804 (89.1) | 12(1.3) | 54 (6.0) | 32 (3.5) | 902 |
| A.nonD. | - | - | - | - | - | 13 (40.6) | 7 (21.9) | 4 (12.5) | 8 (25.0) | 32 |
| D.nonA. | - | - | - | - | - | 49 (36.8) | 3 (2.3) | 56 (42.1) | 25 (18.8) | 133 |
| D.A. | - | - | - | - | - | 14 (10.5) | 3 (2.3) | 27 (20.3) | 89 (66.9) | 133 |
| Total | - | - | - | - | - | 880 (73.3) | 25 (2.1) | 141 (11.7) | 154 (12.8) | 1200 |
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merikangas, K.R.; He, J.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barkin, R.L.; Schwer, W.A.; Barkin, S.J. Recognition and management of depression in primary care: a focus on the elderly. A pharmacotherapeutic overview of the selection process among the traditional and new antidepressants. Am. J. Ther. 2000, 7, 205–226. [Google Scholar] [CrossRef] [PubMed]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [Green Version]
- Moore, E.L.; Terryberry-Spohr, L.; Hope, D.A. Mild traumatic brain injury and anxiety sequelae: a review of the literature. Brain Inj. 2006, 20, 117–132. [Google Scholar] [CrossRef]
- Perry, D.C.; Sturm, V.E.; Peterson, M.J.; Pieper, C.F.; Bullock, T.; Boeve, B.F.; Miller, B.L.; Guskiewicz, K.M.; Berger, M.S.; Kramer, J.H. Association of traumatic brain injury with subsequent neurological and psychiatric disease: a meta-analysis. J. Neurosurg. 2016, 124, 511–526. [Google Scholar] [CrossRef] [Green Version]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- Fann, J.R.; Bombardier, C.H.; Dikmen, S.; Esselman, P.; Warms, C.A.; Pelzer, E.; Rau, H.; Temkin, N. Validity of the Patient Health Questionnaire-9 in assessing depression following traumatic brain injury. J. Head Trauma Rehabil. 2005, 20, 501–511. [Google Scholar] [CrossRef]
- Jorge, R.E.; Robinson, R.G.; Moser, D.; Tateno, A.; Crespo-Facorro, B.; Arndt, S. Major depression following traumatic brain injury. Arch. Gen. Psychiatry 2004, 61, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Mooney, G.; Speed, J. The association between mild traumatic brain injury and psychiatric conditions. Brain Inj. 2001, 15, 865–877. [Google Scholar] [CrossRef]
- Seel, R.T.; Kreutzer, J.S.; Rosenthal, M.; Hammond, F.M.; Corrigan, J.D.; Black, K. Depression after traumatic brain injury: a National Institute on Disability and Rehabilitation Research Model Systems multicenter investigation. Arch. Phys. Med. Rehabil. 2003, 84, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; O’donnell, M.L.; Creamer, M.; McFarlane, A.C.; Clark, C.R.; Silove, D. The psychiatric sequelae of traumatic injury. Am. J. Psychiatry 2010, 167, 312–320. [Google Scholar] [CrossRef]
- Hanel, G.; Henningsen, P.; Herzog, W.; Sauer, N.; Schaefert, R.; Szecsenyi, J.; Löwe, B. Depression, anxiety, and somatoform disorders: vague or distinct categories in primary care? Results from a large cross-sectional study. J. Psychosom. Res. 2009, 67, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, R.M. The comorbidity of major depression and anxiety disorders: recognition and management in primary care. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 244. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Dobson, K.S. The relationship between anxiety and depression. Clin. Psychol. Rev. 1985, 5, 307–324. [Google Scholar] [CrossRef]
- Osman, A.; Wong, J.L.; Bagge, C.L.; Freedenthal, S.; Gutierrez, P.M.; Lozano, G. The depression anxiety stress Scales—21 (DASS-21): further examination of dimensions, scale reliability, and correlates. J. Clin. Psychol. 2012, 68, 1322–1338. [Google Scholar] [CrossRef] [PubMed]
- Buckby, J.A.; Yung, A.R.; Cosgrave, E.M.; Killackey, E.J. Clinical utility of the Mood and Anxiety Symptom Questionnaire (MASQ) in a sample of young help-seekers. BMC Psychiatry 2007, 7, 50. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Johnston, M.; Pollard, B.; Hennessey, P. Construct validation of the hospital anxiety and depression scale with clinical populations. J. Psychosom. Res. 2000, 48, 579–584. [Google Scholar] [CrossRef]
- Caci, H.; Baylé, F.J.; Mattei, V.; Dossios, C.; Robert, P.; Boyer, P. How does the Hospital and Anxiety and Depression Scale measure anxiety and depression in healthy subjects? Psychiatry Res. 2003, 118, 89–99. [Google Scholar] [CrossRef]
- Hinz, A.; Schwarz, R. [Anxiety and depression in the general population: normal values in the Hospital Anxiety and Depression Scale]. Psychother. Psychosom. Med. Psychol. 2001, 51, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, M.; Ford, G.; Hunt, K.; Der, G. A confirmatory factor analysis of the Hospital Anxiety and Depression scale: comparing empirically and theoretically derived structures. Br. J. Clin. Psychol. 2000, 39, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Iani, L.; Lauriola, M.; Costantini, M. A confirmatory bifactor analysis of the hospital anxiety and depression scale in an Italian community sample. Health Qual. Life Outcomes 2014, 12, 84. [Google Scholar] [CrossRef] [PubMed]
- Norton, S.; Cosco, T.; Doyle, F.; Done, J.; Sacker, A. The Hospital Anxiety and Depression Scale: a meta confirmatory factor analysis. J. Psychosom. Res. 2013, 74, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Cosco, T.D.; Doyle, F.; Ward, M.; McGee, H. Latent structure of the Hospital Anxiety And Depression Scale: a 10-year systematic review. J. Psychosom. Res. 2012, 72, 180–184. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Fogelberg, D.J.; Hoffman, J.M.; Dikmen, S.; Temkin, N.R.; Bell, K.R. Association of Sleep and Co-Occurring Psychological Conditions at 1 Year After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2012, 93, 1313–1318. [Google Scholar] [CrossRef]
- Boothroyd, L.; Dagnan, D.; Muncer, S. Psychometric analysis of the Generalized Anxiety Disorder Scale and the Patient Health Questionnaire using Mokken scaling and confirmatory factor analysis. Health Prim. Care 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Kroenke, K.; Wu, J.; Yu, Z.; Bair, M.J.; Kean, J.; Stump, T.; Monahan, P.O. The Patient Health Questionnaire Anxiety and Depression Scale (PHQ-ADS): Initial Validation in Three Clinical Trials. Psychosom. Med. 2016, 78, 716–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, A.I.R.; Menon, D.K.; Steyerberg, E.W.; Citerio, G.; Lecky, F.; Manley, G.T.; Hill, S.; Legrand, V.; Sorgner, A. Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI)A Prospective Longitudinal Observational Study. Neurosurgery 2015, 76, 67–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; Keyser, V.D.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 years: standing the test of time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef]
- Marmarou, A.; Lu, J.; Butcher, I.; McHugh, G.S.; Murray, G.D.; Steyerberg, E.W.; Mushkudiani, N.A.; Choi, S.; Maas, A.I. Prognostic value of the Glasgow Coma Scale and pupil reactivity in traumatic brain injury assessed pre-hospital and on enrollment: an IMPACT analysis. J. Neurotrauma 2007, 24, 270–280. [Google Scholar] [CrossRef]
- Wilson, J. t. L.; Pettigrew, L.E. l.; Teasdale, G.M. Structured Interviews for the Glasgow Outcome Scale and the Extended Glasgow Outcome Scale: Guidelines for Their Use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): a meta-analysis. CMAJ 2012, 184, E191–E196. [Google Scholar] [CrossRef] [Green Version]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Ware Jr, J.E.; Kosinski, M.; Bjorner, J.B.; Turner-Bowker, D.M.; Gandek, B.; Maruish, M.E. User’s manual for the SF-36v2 health survey, 2nd edn. QualityMetric. Inc Linc. 2007. [Google Scholar]
- Bullinger, M. The TBI Consensus Group Quality of life in patients with traumatic brain injury-basic issues, assessment and recommendations. Restor. Neurol. Neurosci. 2002, 20, 111–124. [Google Scholar] [PubMed]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5) in veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef] [PubMed]
- Krüger-Gottschalk, A.; Knaevelsrud, C.; Rau, H.; Dyer, A.; Schäfer, I.; Schellong, J.; Ehring, T. The German version of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): psychometric properties and diagnostic utility. BMC Psychiatry 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teymoori, A.; Real, R.; Gorbunova, A.; Haghish, E.F.; Andelic, N.; Wilson, L.; Asendorf, T.; Menon, D.; von Steinbüchel, N. Measurement invariance of assessments of depression (PHQ-9) and anxiety (GAD-7) across sex, strata and linguistic backgrounds in a European-wide sample of patients after Traumatic Brain Injury. J. Affect. Disord. 2020, 262, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Acquadro, C.; Conway, K.; Giroudet, C.; Mear, I. Linguistic Validation Manual for Health Outcome Assessments; Mapi Institute: Kerry Way Downey, CA, USA, 2012. [Google Scholar]
- Chen, F.F.; Hayes, A.; Carver, C.S.; Laurenceau, J.-P.; Zhang, Z. Modeling General and Specific Variance in Multifaceted Constructs: A Comparison of the Bifactor Model to Other Approaches. J. Pers. 2012, 80, 219–251. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, A.; Reise, S.P.; Haviland, M.G. Evaluating bifactor models: Calculating and interpreting statistical indices. Psychol. Methods 2016, 21, 137–150. [Google Scholar] [CrossRef]
- Bonifay, W.; Lane, S.P.; Reise, S.P. Three Concerns With Applying a Bifactor Model as a Structure of Psychopathology. Clin. Psychol. Sci. 2017, 5, 184–186. [Google Scholar] [CrossRef]
- Rodriguez, A.; Reise, S.P.; Haviland, M.G. Applying bifactor statistical indices in the evaluation of psychological measures. J. Pers. Assess. 2016, 98, 223–237. [Google Scholar] [CrossRef]
- Revelle, W. psych: Procedures for Personality and Psychological Research; Northwestern University: Evanston, IL, USA, 2017; Available online: http://CRAN.R-project.org/ (accessed on 21 March 2020).
- Garber, J.; Weersing, V.R. Comorbidity of Anxiety and Depression in Youth: Implications for Treatment and Prevention. Clin. Psychol. Sci. Pract. 2010, 17, 293–306. [Google Scholar] [CrossRef] [Green Version]
- McCrum-Gardner, E. Which is the correct statistical test to use? Br. J. Oral Maxillofac. Surg. 2008, 46, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling and more. Version 0.5–12 (BETA). J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Kline, P. An Easy Guide to Factor Analysis; Routledge: Abingdon, UK, 2014; ISBN 978-1-317-72560-2. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling With AMOS: Basic Concepts, Applications, and Programming, 3rd. ed.; Routledge: Abingdon, UK, 2016; ISBN 978-1-317-63313-6. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cummings, C.M.; Caporino, N.E.; Kendall, P.C. Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychol. Bull. 2014, 140, 816. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Wilhelm, K.; Mitchell, P.; Austin, M.-P.; Roussos, J.; Gladstone, G. The influence of anxiety as a risk to early onset major depression. J. Affect. Disord. 1999, 52, 11–17. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Harrington, H.; Caspi, A.; Kim-Cohen, J.; Goldberg, D.; Gregory, A.M.; Poulton, R. Depression and generalized anxiety disorder: cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Arch. Gen. Psychiatry 2007, 64, 651–660. [Google Scholar] [CrossRef]
- Whelan-Goodinson, R.; Ponsford, J.; Schönberger, M. Validity of the Hospital Anxiety and Depression Scale to assess depression and anxiety following traumatic brain injury as compared with the Structured Clinical Interview for DSM-IV. J. Affect. Disord. 2009, 114, 94–102. [Google Scholar] [CrossRef]
- Mendels, J.; Weinstein, N.; Cochrane, C. The relationship between depression and anxiety. Arch. Gen. Psychiatry 1972, 27, 649–653. [Google Scholar] [CrossRef]
- Toft, T.; Fink, P.E.R.; Oernboel, E.V.A.; Christensen, K.A.J.; Frostholm, L.; Olesen, F. Mental disorders in primary care: prevalence and co-morbidity among disorders. Results from the functional illness in primary care (FIP) study. Psychol. Med. 2005, 35, 1175–1184. [Google Scholar] [CrossRef]


| Variable | Overall | Stratified | |
|---|---|---|---|
| n | 2137 | Female (738) | Male (1399) |
| Countries (n, (%)) | |||
| The Netherlands | 498 (23.3) | 199 (40) | 299 (60) |
| Italy | 269 (12.6) | 84 (31.2) | 185 (68.8) |
| Norway | 260 (12.2) | 81 (31.2) | 179 (68.8) |
| Spain | 254 (11.9) | 76 (29.9) | 178 (70.1) |
| The UK | 207 (9.7) | 70 (33.8) | 137 (66.2) |
| Finland | 207(9.7) | 83 (40.1) | 124 (59.9) |
| Belgium | 154 (7.2) | 45 (29.2) | 109 (70.8) |
| Sweden | 60 (2.8) | 28 (46.7) | 32 (53.3) |
| France | 52 (2.4) | 9 (17.3) | 43 (82.7) |
| Others | 176 (8.2) | 63 (35.8) | 113 (64.2) |
| Age groups (n, (%)) | |||
| (16–24) | 325 (15.2) | 95 (29.2) | 230 (70.8) |
| (25–34) | 262 (12.3) | 78 (29.8) | 184 (70.2) |
| (35–44) | 274 (12.8) | 67 (24.5) | 207 (75.5) |
| (45–54) | 357 (16.8) | 130 (36.4) | 228 (63.9) |
| (55–64) | 397 (18.6) | 146 (36.8) | 251 (63.2) |
| (> = 65) | 521 (24.4) | 222 (42.6) | 299 (57.4) |
| Patient stratum (n, (%)) | |||
| ER | 447 (20.9) | 198 (44.3) | 249 (55.7) |
| Admission | 805 (37.7) | 297 (36.9) | 508 (63.1) |
| ICU | 885 (41.4) | 243 (27.5) | 642 (72.5) |
| GOSE (n, (%)) | |||
| Severe dis. (3, 4) | 221 (10.3) | 81 (36.7) | 140 (63.3) |
| Moderate dis. (5, 6) | 549 (25.7) | 185 (33.7) | 364 (66.3) |
| Good recovery (7, 8) | 1341 (62.8) | 459 (40.9) | 882 (65.8) |
| NA | 26 (1.2) | 13 (50) | 13 (50) |
| GCS (n, (%)) | |||
| Severe | 340 (16.4) | 90 (26.5) | 250 (73.5) |
| Moderate | 162 (7.8) | 55 (34) | 107 (66) |
| Mild | 1571 (75.8) | 575 (36.6) | 996 (63.4) |
| Education level (n, (%)) | |||
| None | 23 (1.2) | 12 (52.2) | 11 (47.8) |
| Currently studying | 58 (3.0) | 22 (37.9) | 36 (62.1) |
| Primary school | 240 (12.6) | 86 (35.8) | 154 (64.2) |
| Secondary/high school | 651 (34.1) | 213 (32.7) | 438 (67.3) |
| Post high school | 402 (21.1) | 109 (27.1) | 293 (72.9) |
| University/college | 533 (27.9) | 209 (39.2) | 324 (60.8) |
| α | λ2 | M | SD | Min–Max (Q1, Q2, Q3) | GAD-7 | PHQ-9 | PHQ-ADS | |
|---|---|---|---|---|---|---|---|---|
| GAD-7 | 0.91 | 0.91 | 3.63 | 4.54 | 0–21 (0, 2, 6) | 1.00 | ||
| PHQ-9 | 0.87 | 0.88 | 5.07 | 5.35 | 0–27 (1, 3, 8) | 0.80 | 1.00 | |
| PHQ-ADS | 0.94 | 0.94 | 8.71 | 9.40 | 0–48 (2, 6, 13) | 0.94 | 0.96 | 1.00 |
| PCL-5 | 0.93 | 0.94 | 12.20 | 13.61 | 0–80 (0, 8, 17) | 0.76 | 0.76 | 0.80 |
| SF-36, PF | 0.94 | 0.94 | 77.31 | 26.89 | 0–100 (65, 90, 100) | −0.32 | −0.42 | −0.39 |
| SF-36, RP | 0.95 | 0.94 | 64.18 | 31.94 | 0–100 (40, 69, 100) | −0.44 | −0.55 | −0.53 |
| SF-36, RE | 0.94 | 0.91 | 74.56 | 28.33 | 0–100 (50, 83, 100) | −0.60 | −0.65 | −0.66 |
| SF-36, SF | 0.85 | - | 75.06 | 26.49 | 0–100 (63, 87, 100) | −0.56 | −0.67 | −0.65 |
| SF-36, BP | 0.88 | - | 68.79 | 27.00 | 0–100 (51, 74, 100) | −0.45 | −0.52 | −0.51 |
| SF-36, VT | 0.84 | 0.83 | 57.77 | 21.86 | 0–100 (44, 62, 75) | −0.58 | −0.73 | −0.70 |
| SF-36, MH | 0.86 | 0.84 | 71.49 | 20.04 | 0–100 (60, 75, 90) | −0.76 | −0.76 | −0.80 |
| SF-36, GH | 0.76 | 0.73 | 66.41 | 22.28 | 0–100 (50, 70, 82) | −0.51 | −0.59 | −0.58 |
| χ2 (df) | χ2/df | p | RMSEA a | b RMSEA 95% CI | c SRMR | d CFI | e TLI | f NFI | g IFI | |
|---|---|---|---|---|---|---|---|---|---|---|
| One-factorial M. | 477.63 (104) | 4.49 | <0.001 | 0.042 | 0.038–0.045 | 0.048 | 0.995 | 0.994 | 0.994 | 0.995 |
| Two-factorial M. | 308.46 (103) | 2.99 | <0.001 | 0.031 | 0.027–0.035 | 0.039 | 0.997 | 0.997 | 0.996 | 0.997 |
| Bifactorial M. | 189.76 (88) | 2.15 | <0.001 | 0.024 | 0.019–0.028 | 0.032 | 0.999 | 0.998 | 0.998 | 0.999 |
| Generalized Anxiety Disorder (GAD-7) Categories at 3-Month Based on the Cut-Off Point of 8 | |||||||||||
| Low Anxiety at 3-Months | High Anxiety at 3-Months | ||||||||||
| Matched variable | Depression at 6 Mo | Depression at 6 Mo | |||||||||
| 0, n (%) | 1, n (%) | Total | Mc (df), p * | 0, n (%) | 1, n (%) | Total | Mc (df), p | ||||
| Depression at 3 mo | 0 | 1056 (91.6) | 97 (8.4) | 1153 | 0.18 (1), p = 0.61 | Depression at 3 mo | 0 | 33 (80.5) | 8 (19.5) | 41 | 42.61 (1), p < 0.001 |
| 1 | 103 (48.6) | 109 (51.4) | 212 | 1 | 63 (28.0) | 162 (72.0) | 225 | ||||
| Total | 1159 (84.9) | 206 (15.1) | Total | 96 (36.1) | 170 (63.9) | ||||||
| Generalized Anxiety Disorder (GAD-7) categories at 3-month based on the cut-off point of 8 | |||||||||||
| Low anxiety at 3-Months | High anxiety at 3-Months | ||||||||||
| Depression at 12 Mo | Depression at 12 Mo | ||||||||||
| 0, n (%) | 1, n (%) | Total | Mc (df), p | 0, n (%) | 1, n (%) | Total | Mc.(df), p | ||||
| Depression at 3 mo | 0 | 713 (89.6) | 83 (10.4) | 796 | 0.94 (1), p = 0.33 | Depression at 3 mo | 0 | 17 (70.8) | 7 (29.2) | 24 | 23.17 (1), p < 0.001 |
| 1 | 71 (47.7) | 78 (52.3) | 149 | 1 | 40 (31.5) | 87 (68.5) | 127 | ||||
| Total | 784 (83.0) | 161 (17.0) | Total | 57 (37.7) | 94 (62.3) | ||||||
| Generalized Anxiety Disorder (GAD-7) categories at 6-month based on the cut-off point of 8 | |||||||||||
| Low anxiety at 6-Months | High anxiety at 6-Months | ||||||||||
| Depression at 12 Mo | Depression at 12 Mo | ||||||||||
| 0, n (%) | 1, n (%) | Total | Mc (df), p | 0, n (%) | 1, n (%) | Total | Mc (df), p | ||||
| Depression at 6 mo | 0 | 818 (90.5) | 86 (9.5) | 904 | 8.38 (1), p < 0.01 | Depression at 6 mo | 0 | 20 (62.5) | 12 (37.5) | 32 | 0.86 (1), p = 0.353 |
| 1 | 52 (39.1) | 81 (60.9) | 133 | 1 | 17 (12.8) | 116 (87.2) | 133 | ||||
| Total | 870 (83.9) | 167 (16.1) | Total | 37 (22.4) | 128 (77.6) | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teymoori, A.; Gorbunova, A.; Haghish, F.E.; Real, R.; Zeldovich, M.; Wu, Y.-J.; Polinder, S.; Asendorf, T.; Menon, D.; CENTER-TBI Investigators and Participants; et al. Factorial Structure and Validity of Depression (PHQ-9) and Anxiety (GAD-7) Scales after Traumatic Brain Injury. J. Clin. Med. 2020, 9, 873. https://doi.org/10.3390/jcm9030873
Teymoori A, Gorbunova A, Haghish FE, Real R, Zeldovich M, Wu Y-J, Polinder S, Asendorf T, Menon D, CENTER-TBI Investigators and Participants, et al. Factorial Structure and Validity of Depression (PHQ-9) and Anxiety (GAD-7) Scales after Traumatic Brain Injury. Journal of Clinical Medicine. 2020; 9(3):873. https://doi.org/10.3390/jcm9030873
Chicago/Turabian StyleTeymoori, Ali, Anastasia Gorbunova, Fardzadeh E. Haghish, Ruben Real, Marina Zeldovich, Yi-Jhen Wu, Suzanne Polinder, Thomas Asendorf, David Menon, CENTER-TBI Investigators and Participants, and et al. 2020. "Factorial Structure and Validity of Depression (PHQ-9) and Anxiety (GAD-7) Scales after Traumatic Brain Injury" Journal of Clinical Medicine 9, no. 3: 873. https://doi.org/10.3390/jcm9030873