Expression Patterns of Circulating MicroRNAs in the Risk Stratification of Bicuspid Aortopathy

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.1.1. Bicuspid Aortic Valve Root Phenotype Cohort (BAV-AR)
2.1.2. Bicuspid Aortic Valve Stenosis Cohort (BAV-AS)
2.1.3. Tricuspid Aortic Valve Stenosis Cohort (TAV-AS)
2.2. Definitions and Measurements
2.3. MicroRNA Analysis
2.4. Statistical Analysis
3. Results
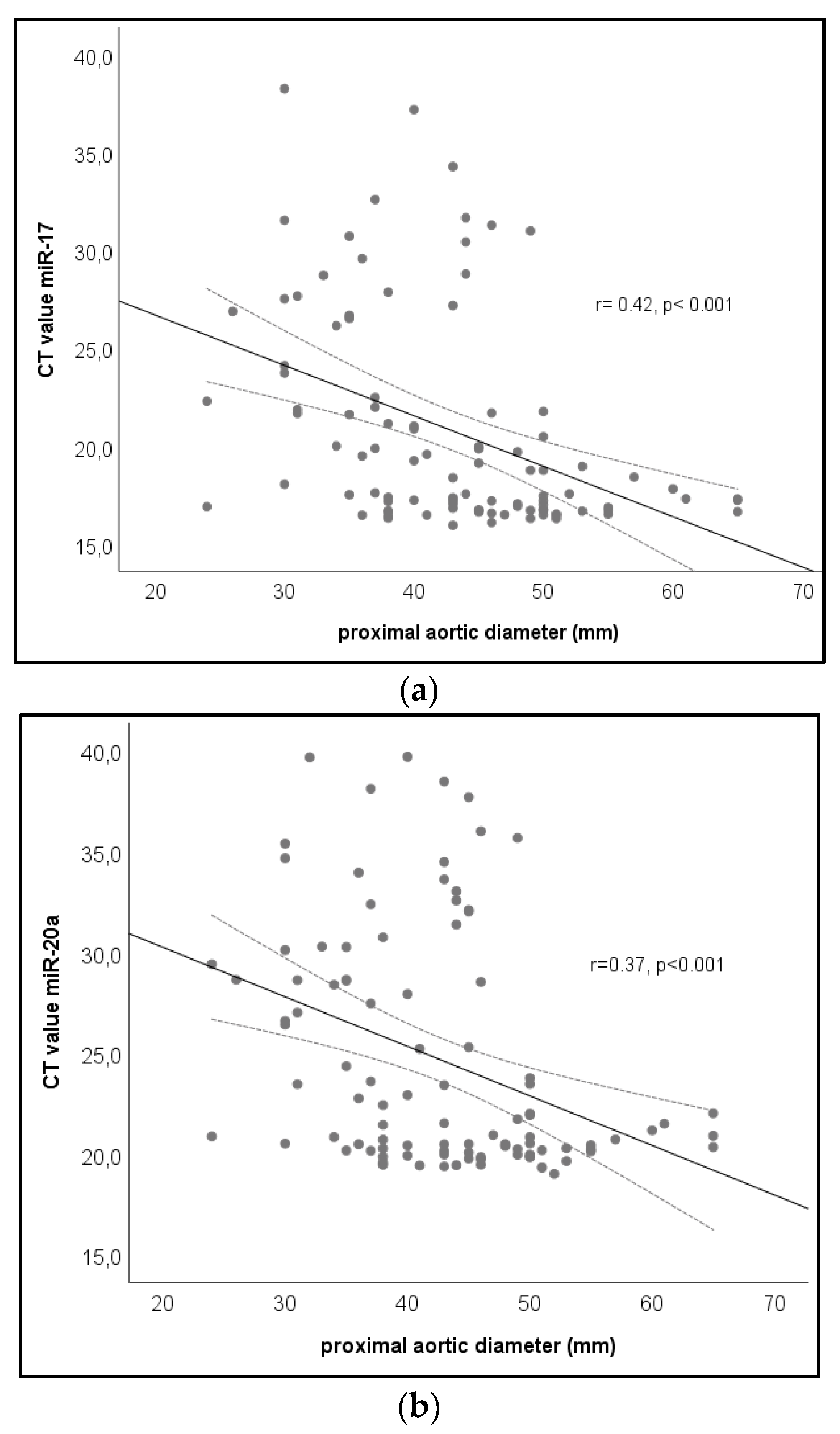
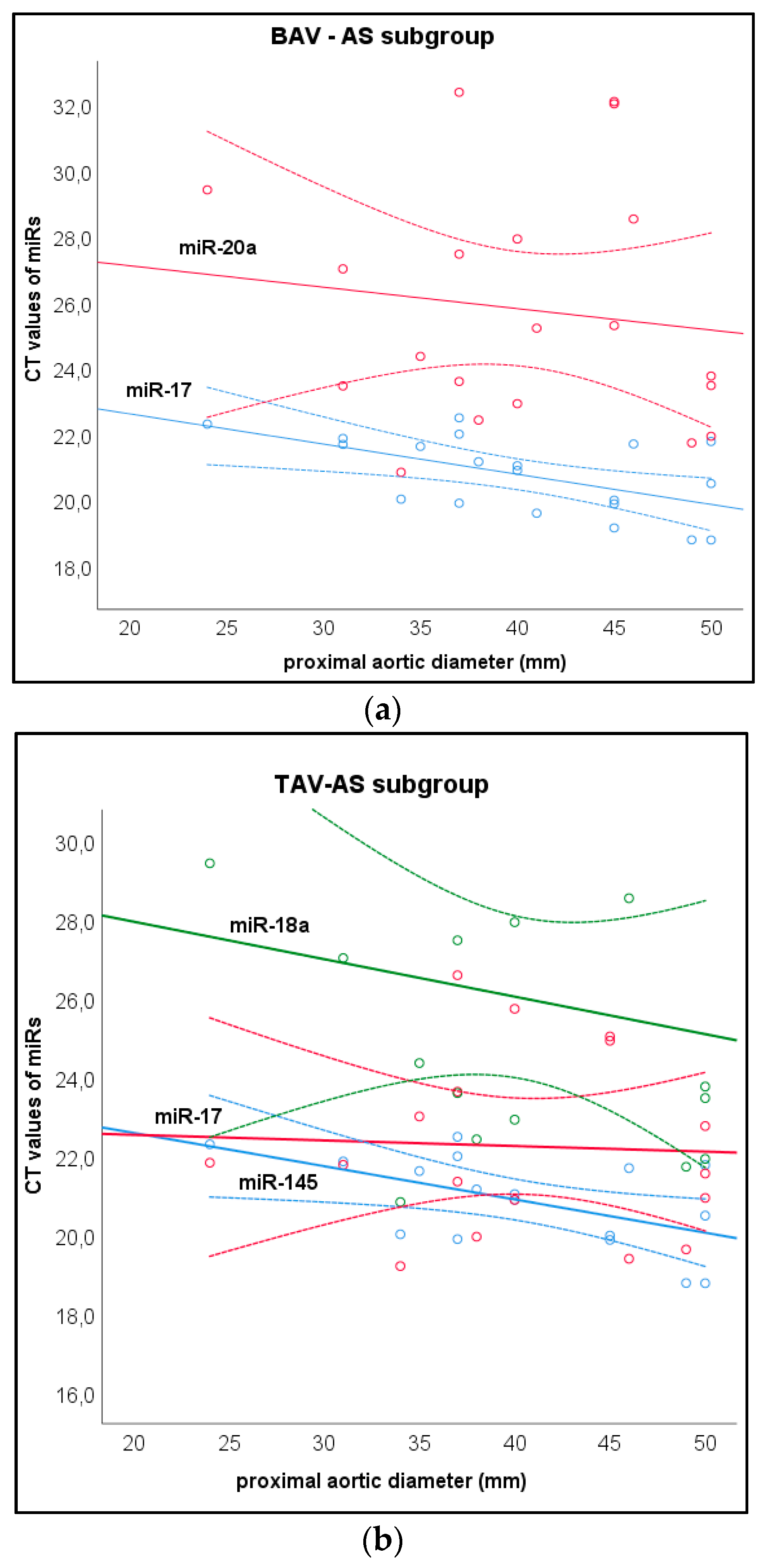
Biomarker Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Pape, L.A.; Tsai, T.T.; Isselbacher, E.M.; Oh, J.K.; O’Gara, P.T.; Evangelista, A.; Evangelista, A. Aortic diameter >or = 5.5 cm is not a good predictor of type A aortic dissection: Observations from the International Registry of Acute Aortic Dissection (IRAD). Circulation 2007, 116, 1120–1127. [Google Scholar] [CrossRef] [Green Version]
- Rylski, B.; Branchetti, E.; Bavaria, J.E.; Vallabhajosyula, P.; Szeto, W.Y.; Milewski, R.K.; Desai, N.D. Modeling of predissection aortic size in acute type A dissection: More than 90% fail to meet the guidelines for elective ascending replacement. J. Thorac. Cardiovasc. Surg. 2014, 148, 944–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, T.; Bossone, E.; Sawaki, D.; Janosi, R.A.; Erbel, R.; Eagle, K.; Nagai, R. Biomarkers of aortic diseases. Am. Heart J. 2013, 165, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, J.S.; Ivey, C.R.; Wheeler, J.B.; Akerman, A.W.; Rice, A.; Patel, R.K.; Mukherjee, R. Plasma biomarkers for distinguishing etiologic subtypes of thoracic aortic aneurysm disease. J. Thorac. Cardiovasc. Surg. 2013, 145, 1326–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedak, P.W.; Verma, S.; David, T.E.; Leask, R.L.; Weisel, R.D.; Butany, J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation 2002, 106, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, S.A.; Evangelista, A.; Abbara, S.; Arai, A.; Asch, F.M.; Badano, L.P.; Bolen, M.A.; Konnolly, H.M.; Czerny, M.; Devereux, R.B.; et al. Multimodality Imaging of Diseases of the Thoracic Aorta in Adults: From the American Society of Echocardiography and the European Association of Cardiovascular Imaging: Endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2015, 28, 119–182. [Google Scholar]
- Mendoza, D.D.; Kochar, M.; Devereux, R.B.; Basson, C.T.; Min, J.K.; Holmes, K.; Dietz, H.C.; Milewicz, D.M.; LeMaire, S.A.; Pyeritz, R.E.; et al. Impact of image analysis methodology on diagnostic and surgical classification of patients with thoracic aortic aneurysms. Ann. Thorac. Surg. 2011, 92, 904–912. [Google Scholar] [CrossRef]
- Wu, J.; Song, H.F.; Li, S.H.; Guo, J.; Tsang, K.; Tumiati, L.; Butany, J.; Yau, T.M.; Ouzounian, M.; Fu, S.; et al. Progressive Aortic Dilation Is Regulated by miR-17-Associated miRNAs. J. Am. Coll. Cardiol. 2016, 67, 2965–2977. [Google Scholar] [CrossRef]
- Cho, W.C. MicroRNAs as therapeutic targets for lung cancer. Chin. J. Lung Cancer 2010, 13, C58–C60. [Google Scholar] [CrossRef]
- Furukawa, H.; Yamane, N.; Honda, T.; Yamasawa, T.; Kanaoka, Y.; Tanemoto, K. Initial clinical evaluation of preoperative frailty in surgical patients with Stanford type A acute aortic dissection. Gen. Thorac. Cardiovasc. Surg. 2018, 67, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Grootes, I.; Barrett, J.K.; Ulug, P.; Rohlffs, F.; Laukontaus, S.J.; Tulamo, R.; Venermo, M.; Greenhalgh, R.M.; Sweeting, M.J. Predicting risk of rupture and rupture-preventing reinterventions following endovascular abdominal aortic aneurysm repair. Br. J. Surg. 2018, 105, 1294–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, W.; Peng, Z.; Chai, X.; Zhu, Q.; Yang, G.; Zhao, Q.; Zhou, S. Potential biomarkers for early diagnosis of acute aortic dissection. Heart & Lung. J. Acute Crit. Care 2015, 44, 205–208. [Google Scholar]
- Joviliano, E.E.; Ribeiro, M.S.; Tenorio, E.J.R. MicroRNAs and Current Concepts on the Pathogenesis of Abdominal Aortic Aneurysm. Braz. J. Cardiovasc. Surg. 2017, 32, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Kusenda, B.; Mraz, M.; Mayer, J.; Pospisilova, S. MicroRNA biogenesis, functionality and cancer relevance. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. 2006, 150, 205–215. [Google Scholar] [CrossRef] [Green Version]
- Lynam-Lennon, N.; Maher, S.G.; Reynolds, J.V. The roles of microRNA in cancer and apoptosis. Biol. Rev. Camb. Philos. Soc. 2009, 84, 55–71. [Google Scholar] [CrossRef]
- Greco, S.; Gorospe, M.; Martelli, F. Noncoding RNA in age-related cardiovascular diseases. J. Mol. Cell. Cardiol. 2015, 83, 142–155. [Google Scholar] [CrossRef] [Green Version]
- Adamo, L.; Braverman, A.C. Surgical threshold for bicuspid aortic valve aneurysm: A case for individual decision-making. Heart 2015, 101, 1361–1367. [Google Scholar] [CrossRef]
- Pepe, G.; Nistri, S.; Giusti, B.; Sticchi, E.; Attanasio, M.; Porciani, C.; Abbate, R.; Bonow, R.O.; Tacoub, M.; Gensini, G.F. Identification of fibrillin 1 gene mutations in patients with bicuspid aortic valve (BAV) without Marfan syndrome. BMC Med. Genet. 2014, 15, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foffa, I.; Ait Ali, L.; Panesi, P.; Mariani, M.; Festa, P.; Botto, N.; Vecoli, C.; Andreassi, M.G. Sequencing of NOTCH1, GATA5, TGFBR1 and TGFBR2 genes in familial cases of bicuspid aortic valve. BMC Med. Genet. 2013, 14, 44. [Google Scholar] [CrossRef] [Green Version]
- Girdauskas, E.; Petersen, J.; Neumann, N.; Gross, T.; Naito, S.; Hillebrand, M.; Zeller, T.; Reichenspurner, H.; Blankenberg, S. Evaluation of microribonucleic acids as potential biomarkers in the bicuspid aortic valve-associated aortopathy. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Ying, Z.; Qi, X.; Shi, Y.; Tang, Q. MicroRNA-1 regulates the proliferation of vascular smooth muscle cells by targeting insulin-like growth factor 1. Int. J. Mol. Med. 2015, 36, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Maegdefessel, L.; Azuma, J.; Toh, R.; Deng, A.; Merk, D.R.; Raiesdana, A.; Leeper, N.; Raaz, U.; Schoelmerich, A.; Dalman, R.; et al. MicroRNA-21 blocks abdominal aortic aneurysm development and nicotine-augmented expansion. Sci. Transl. Med. 2012, 4, 122ra22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.; Li, D.Y.; Chernogubova, E.; Sun, C.; Busch, A.; Eken, S.M.; Winter, H.; Winski, G.; Raaz, U.; Simon, N.; et al. Local Delivery of miR-21 Stabilizes Fibrous Caps in Vulnerable Atherosclerotic Lesions. Molecular therapy. J. Am. Soc. Gene Ther. 2018, 26, 1040–1055. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Liu, X.; Yang, J.; Lin, Y.; Xu, D.Z.; Lu, Q.; Deitch, E.A.; Huo, Y.; Delphin, E.S.; Zhang, C. MicroRNA-145, a novel smooth muscle cell phenotypic marker and modulator, controls vascular neointimal lesion formation. Circ. Res. 2009, 105, 158–166. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, B.; Shi, Y.; Xu, C.; Xiao, H.L.; Ma, L.N.; Xu, S.L.; Yang, L.; Wang, Q.L.; Dang, W.Q.; et al. Oncogenic miR-20a and miR-106a enhance the invasiveness of human glioma stem cells by directly targeting TIMP-2. Oncogene 2015, 34, 1407–1419. [Google Scholar] [CrossRef]
- Martinez-Micaelo, N.; Beltran-Debon, R.; Baiges, I.; Faiges, M.; Alegret, J.M. Specific circulating microRNA signature of bicuspid aortic valve disease. J. Transl. Med. 2017, 15, 76. [Google Scholar] [CrossRef] [Green Version]
- Sabatino, J.; Wicik, Z.; De Rosa, S.; Eyileten, C.; Jakubik, D.; Spaccarotella, C.; Mongiardo, A.; Postula, M.; Indolfi, C. MicroRNAs fingerprint of bicuspid aortic valve. J. Mol. Cell. Cardiol. 2019, 134, 98–106. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | BAV-AR (n = 63) | BAV-AS (n = 32) | TAV-AS (n = 50) | p-Value |
|---|---|---|---|---|
| Mean age (years) | 47 ± 11.3 | 59 ± 9.7 | 56 ± 14 | <0.001 |
| Male gender | 58 (92) | 22 (70) | 26 (55) | <0.001 |
| BSA (m²) | 2.01 ± 0.2 | 1,98 ± 0.2 | 2.10 ± 0.6 | 0.496 |
| NYHA class III/IV | 10 (43) | 10 (31) | 26 (52) | 0.181 |
| Aortic root diameter (mm) | 46 ± 8 | 40 ± 7 | 37 ± 7 | 0.000 |
| Arterial hypertension | 6 (30) | 17 (53) | 33 (66) | 0.023 |
| Diabetes | 1 (5) | 4 (12.5) | 7 (14) | 0.566 |
| History of smoking | 11 (55) | 15 (60) | 19 (44) | 0.42 |
| Mean AVR * prosthesis size (mm) | 27.8 ± 1.3 | 24.8 ± 1.7 | 24.5 ± 1.5 | <0.001 |
| MicroRNA Values | Whole Cohort (n = 145) | BAV-AR (n = 63) | BAV-AS (n = 32) | TAV-AS (n = 50) | p-Value |
|---|---|---|---|---|---|
| miR-17 | 21.8 ± 5.7 | 17.1 ± 0.8 | 21.2 ± 1.8 | 29.0 ± 3.9 | <0.001 |
| miR-18a | 25.0 ± 4.9 | 21.8 ± 4.1 | 24.1 ± 1.5 | 29.8 ± 3.2 | <0.001 |
| miR-19a | 23.6 ± 5.3 | 21.5 ± 1.0 | 22.5 ± 2.2 | 26.9 ± 7.7 | <0.001 |
| miR-20a | 25.5 ± 6.0 | 20.3 ± 0.8 | 26.1 ± 4.0 | 32.0 ± 4.3 | <0.001 |
| miR-21 | 24.1 ± 4.6 | 20.5 ± 1.0 | 24.6 ± 3.2 | 28.3 ± 4.3 | <0.001 |
| miR-106a | 25.8 ± 5.7 | 21.0 ± 0.7 | 28.5 ± 3.7 | 32.4 ± 3.4 | <0.001 |
| miR-145 | 23.8 ± 3.8 | 20.7 ± 0.6 | 26.9 ± 2.5 | 25.9 ± 4.0 | <0.001 |
| Correlation Coefficient | miR-17 | miR-18a | miR-19a | miR-20a | miR-21 | miR-106a | miR-145 |
|---|---|---|---|---|---|---|---|
| Aortic diameter (mm) | −0.285 | 0.044 | 0.105 | −0.215 | 0.215 | −0.221 | 0.234 |
| p-Value | 0.005 | 0.666 | 0.301 | 0.031 | 0.58 | 0.5 | 0.1 |
| Variables | Regression Coefficient B | Standard Error | p-Value |
|---|---|---|---|
| Aortic valve phenotype (BAV vs. TAV) | −8.521 | 0.644 | 0.000 |
| Aortopathy (proximal aorta ≥ 40 mm) | −1.677 | 0.702 | 0.019 |
| Gender | 0.017 | 0.554 | 0.976 |
| Age | 0.064 | 0.018 | 0.001 |
| Maximal aortic diameter (mm) | 0.001 | 0.029 | 0.961 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girdauskas, E.; Neumann, N.; Petersen, J.; Sequeira-Gross, T.; Naito, S.; von Stumm, M.; von Kodolitsch, Y.; Reichenspurner, H.; Zeller, T. Expression Patterns of Circulating MicroRNAs in the Risk Stratification of Bicuspid Aortopathy. J. Clin. Med. 2020, 9, 276. https://doi.org/10.3390/jcm9010276
Girdauskas E, Neumann N, Petersen J, Sequeira-Gross T, Naito S, von Stumm M, von Kodolitsch Y, Reichenspurner H, Zeller T. Expression Patterns of Circulating MicroRNAs in the Risk Stratification of Bicuspid Aortopathy. Journal of Clinical Medicine. 2020; 9(1):276. https://doi.org/10.3390/jcm9010276
Chicago/Turabian StyleGirdauskas, Evaldas, Niklas Neumann, Johannes Petersen, Tatiana Sequeira-Gross, Shiho Naito, Maria von Stumm, Yskert von Kodolitsch, Hermann Reichenspurner, and Tanja Zeller. 2020. "Expression Patterns of Circulating MicroRNAs in the Risk Stratification of Bicuspid Aortopathy" Journal of Clinical Medicine 9, no. 1: 276. https://doi.org/10.3390/jcm9010276