Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Protocol
2.2. Selection Criteria
2.3. Surgical and Restorative Procedures
2.4. Radiographic Measurements
2.5. Predictor and Outcome Variables
- early MBL (up to 12 months from prosthetic loading).
- implant failure: implant mobility or implant removal due to progressive marginal bone loss. Implant stability was tested by tightening abutment screws (35 N/cm) at prosthesis delivery.
- any complication or adverse event.
2.6. Statistical Analysis
- Model B: T1
- Model C: T1, T2
- Model D: T2, T3, T4
3. Results
3.1. Demographics and Clinical Outcomes
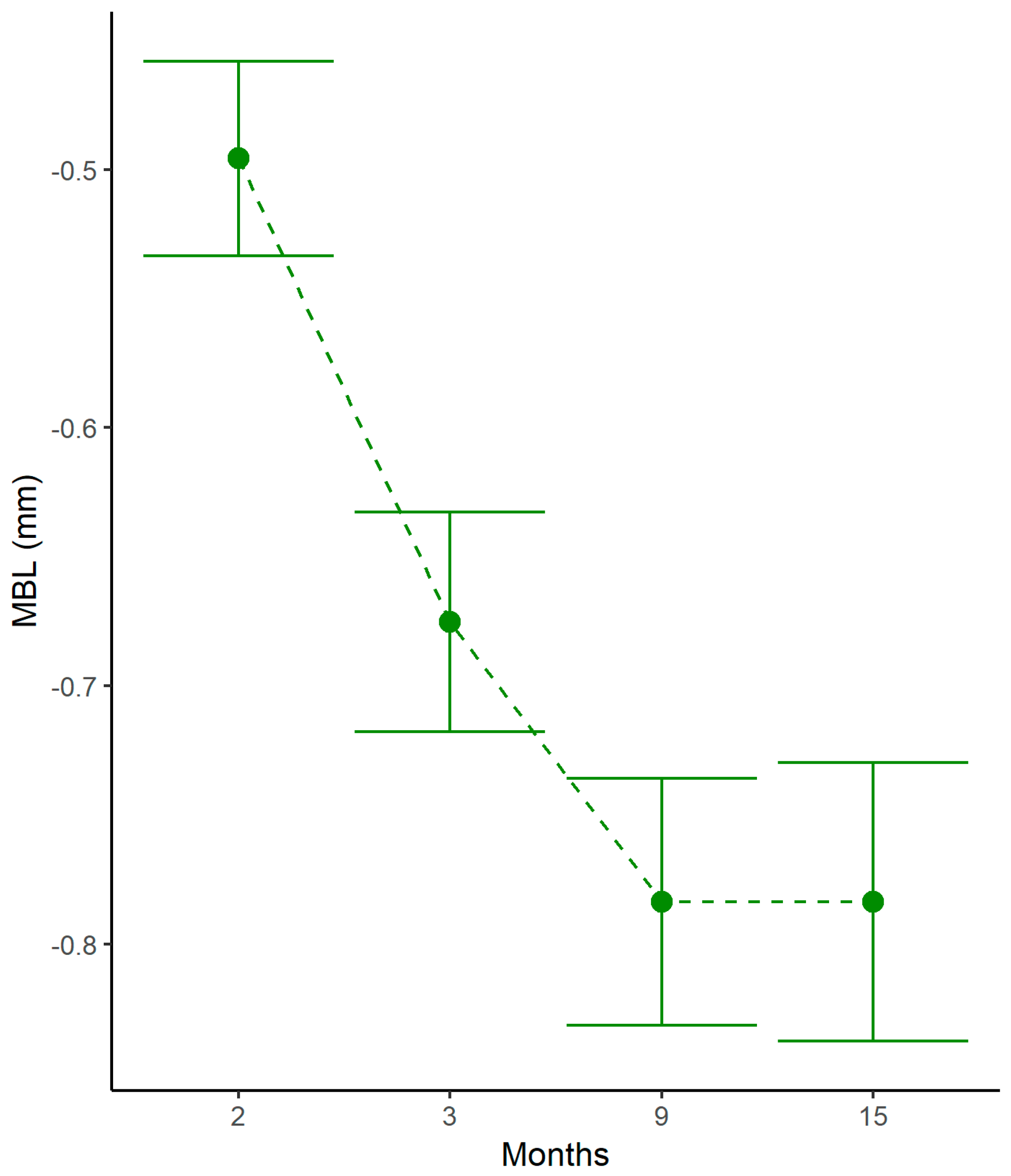
3.2. Marginal Bone Level Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Donath, K. Pathogenesis of bony pocket formation around dental implants. J. Dent. Assoc. S. Afr. 1992, 47, 204–208. [Google Scholar] [PubMed]
- Donath, K.; Laass, M.; Günzl, H.J. The histopathology of different foreign body reactions in oral soft tissue and bone tissue. Virchows Arch. A Pathol. Anat. Histopathol. 1992, 420, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Jacobsson, M.; Wennerberg, A. Osseointegration of implants—A biological and clinical overview. JSM Dent. Surg. 2017, 2, 1022–1027. [Google Scholar]
- Trindade, R.; Albrektsson, T.; Tengvall, P.; Wennerberg, A. Foreign body reaction to biomaterials: On mechanisms for buildup and breakdown of osseointegration. Clin. Implant Dent. Relat. Res. 2016, 18, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Oh, T.J.; Yoon, J.; Misch, C.E.; Wang, H.-L. The causes of early implant bone loss: Myth or science? J. Periodontol. 2002, 73, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Tatarakis, N.; Bashutski, J.; Wang, H.-L.; Oh, T.J. Early implant bone loss: Preventable or inevitable? Implant Dent. 2012, 21, 379–386. [Google Scholar] [CrossRef]
- Qian, J.; Wennerberg, A.; Albrektsson, T. Reasons for marginal bone loss around oral implants. Clin. Implant Dent. Relat. Res. 2012, 14, 792–807. [Google Scholar] [CrossRef]
- Spinato, S.; Stacchi, C.; Lombardi, T.; Bernardello, F.; Messina, M.; Zaffe, D. Biological width establishment around dental implants is influenced by abutment height irrespective of vertical mucosal thickness: A cluster randomized controlled trial. Clin. Oral Implant. Res. 2019, 30, 649–659. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; O’Valle, F.; Catena, A. Marginal bone loss as success criterion in implant dentistry: Beyond 2 mm. Clin. Oral Implant. Res. 2015, 26, e28–e34. [Google Scholar] [CrossRef]
- Santiago, J.F., Jr.; Batista, V.E.; Verri, F.R.; Honório, H.M.; de Mello, C.C.; Almeida, D.A.; Pellizzer, E.P. Platform-switching implants and bone preservation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.T.; Lin, G.H.; Wang, H.L. Effects of platform-switching on peri-implant soft and hard tissue outcomes: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, e9–e24. [Google Scholar] [CrossRef] [PubMed]
- Donovan, R.; Fetner, A.; Koutouzis, T.; Lundgren, T. Crestal bone changes around implants with reduced abutment diameter placed non-submerged and at subcrestal positions: A 1-year radiographic evaluation. J. Periodontol. 2010, 81, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Ferrarotti, F.; Mariani, G.M.; Ghelardoni, C.; Romano, F. Soft tissue and crestal bone changes around implants with platform-switched abutments placed nonsubmerged at subcrestal position: A 2-year clinical and radiographic evaluation. Int. J. Oral Maxillofac. Implant. 2015, 30, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Broggini, N.; McManus, L.M.; Hermann, J.S. Periimplant inflammation defined by the implant-abutment interface. J. Dent. Res. 2006, 85, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Gatti, C.; Gatti, F.; Silvestri, M.; Mintrone, F.; Rossi, R.; Tridondani, G.; Piacentini, G.; Borrelli, P. A prospective multicenter study on radiographic crestal bone changes around dental implants placed at crestal or subcrestal level: One-year findings. Int. J. Oral Maxillofac. Implant. 2018, 33, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. The influence of soft tissue thickness on crestal bone changes around implants: A 1-year prospective controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2009, 24, 712–719. [Google Scholar]
- Sentineri, R.; Lombardi, T.; Berton, F.; Stacchi, C. Laurell-Gottlow suture modified by Sentineri for tight closure of a wound with a single line of sutures. Br. J. Oral Maxillofac. Surg. 2016, 54, e18–e19. [Google Scholar] [CrossRef]
- Mombelli, A.; van Oosten, M.A.; Schurch, E.; Lang, N. The microbiota associated with successful or failing implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Gomez-Roman, G.; Launer, S. Peri-implant bone changes in immediate and non-immediate root-analog stepped implants-a matched comparative prospective study up to 10 years. Int. J. Implant Dent. 2016, 2, 15. [Google Scholar] [CrossRef]
- Fickl, S.; Zuhr, O.; Stein, J.M.; Hurzeler, M.B. Peri-implant bone level around implants with platform-switched abutments. Int. J. Oral Maxillofac. Implant. 2010, 25, 577–581. [Google Scholar]
- Froum, S.J.; Cho, S.C.; Suzuki, T.; Yu, P.; Corby, P.; Khouly, I. Epicrestal and subcrestal placement of platform-switched implants: 18 month-result of a randomized, controlled, split-mouth, prospective clinical trial. Clin. Oral Implant. Res. 2018, 29, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Koutouzis, T.; Neiva, R.; Nonhoff, J.; Lundgren, T. Placement of implants with platform-switched Morse taper connections with the implant-abutment interface at different levels in relation to the alveolar crest: A short-term (1-year) randomized prospective controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 1553–1563. [Google Scholar] [CrossRef] [PubMed]
- Collaert, B.; De Bruyn, H. Immediate functional loading of TiOblast dental implants in full-arch edentulous maxillae: A 3-year prospective study. Clin. Oral Implant. Res. 2008, 19, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, S.; Collaert, B.; Cosyn, J.; De Bruyn, H. A 9-year prospective case series using multivariate analyses to identify predictors of early and late peri-implant bone loss. Clin. Implant Dent. Relat. Res. 2016, 18, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Borges, T.; Leitão, B.; Pereira, M.; Carvalho, Á.; Galindo-Moreno, P. Influence of the abutment height and connection timing in early peri-implant marginal bone changes: A prospective randomized clinical trial. Clin. Oral Implant. Res. 2018, 29, 907–914. [Google Scholar] [CrossRef]
- Atieh, M.A.; Tawse-Smith, A.; Alsabeeha, N.H.M.; Ma, S.; Duncan, W.J. The one abutment-one time protocol: A systematic review and meta-analysis. J. Periodontol. 2017, 88, 1173–1185. [Google Scholar] [CrossRef]
- Khayat, P.G.; Arnal, H.M.; Tourbah, B.I.; Sennerby, L. Clinical outcome of dental implants placed with high insertion torques (up to 176 Ncm). Clin. Implant Dent. Relat. Res. 2013, 15, 227–233. [Google Scholar] [CrossRef]
- Grandi, T.; Guazzi, P.; Samarani, R.; Grandi, G. Clinical outcome and bone healing of implants placed with high insertion torque: 12-month results from a multicenter controlled cohort study. Int. J. Oral Maxillofac. Surg. 2013, 42, 516–520. [Google Scholar] [CrossRef]
- Duyck, J.; Roesems, R.; Cardoso, M.V.; Ogawa, T.; De Villa Camargos, G.; Vandamme, K. Effect of insertion torque on titanium implant osseointegration: An animal experimental study. Clin. Oral Implant. Res. 2015, 26, 191–196. [Google Scholar] [CrossRef]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The effect of insertion torque on the clinical outcome of single implants: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2016, 18, 588–600. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Giammarinaro, E.; Toti, P.; Alfonsi, F.; Covani, U.; Barone, A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study. Clin. Implant Dent. Relat. Res. 2018, 20, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Norton, M. Primary stability versus viable constraint—A need to redefine. Int. J. Oral Maxillofac. Implant. 2013, 28, 19–21. [Google Scholar]
- Spray, J.R.; Black, C.G.; Morris, H.F.; Ochi, S. The influence of bone thickness on facial marginal bone response: Stage 1 placement through stage 2 uncovering. Ann. Periodontol. 2000, 5, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J.; Ericsson, I.; Marinello, C.P.; Liljenberg, B.; Thomsen, P. The soft tissue barrier at implants and teeth. Clin. Oral Implant. Res. 1991, 2, 81–90. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Wennström, J.; Lindhe, J. The peri-implant hard and soft tissues at different implant systems. A comparative study in the dog. Clin. Oral Implant. Res. 1996, 7, 212–219. [Google Scholar] [CrossRef]
- Judgar, R.; Giro, G.; Zenobio, E.; Coelho, P.G.; Feres, M.; Rodrigues, J.A.; Mangano, C.; Iezzi, G.; Piattelli, A.; Shibli, J.A. Biological width around one-and two-piece implants retrieved from human jaws. BioMed Res. Int. 2014, 2014, 850120. [Google Scholar] [CrossRef]
- Tomasi, C.; Tessarolo, F.; Caola, I.; Wennström, J.; Nollo, G.; Berglundh, T. Morphogenesis of peri-implant mucosa revisited: An experimental study in humans. Clin. Oral Implant. Res. 2014, 25, 997–1003. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; Suárez, F.; O’Valle, F.; Spinato, S.; Catena, A. Prosthetic abutment height is a key factor in peri-implant marginal bone loss. J. Dent. Res. 2014, 93, 80S–85S. [Google Scholar] [CrossRef]
- Vervaeke, S.; Dierens, M.; Besseler, J.; De Bruyn, H. The influence of initial soft tissue thickness on peri-implant bone remodeling. Clin. Implant Dent. Relat. Res. 2014, 16, 238–247. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; León-Cano, A.; Monje, A.; Ortega-Oller, I.; O’Valle, F.; Catena, A. Abutment height influences the effect of platform switching on peri-implant marginal bone loss. Clin. Oral Implant. Res. 2016, 27, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Spinato, S.; Galindo-Moreno, P.; Bernardello, F.; Zaffe, D. Minimum abutment height to eliminate bone loss: Influence of implant neck design and platform switching. Int. J. Oral Maxillofac. Implant. 2018, 33, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lin, C.Y.; Li, J.; Wang, H.L.; Yu, H. Influence of abutment height on peri-implant marginal bone loss: A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 122, 14–21.e2. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.; Pico, A.; Caneiro, L.; Nóvoa, L.; Batalla, P.; Martín-Lancharro, P. Effect of abutment height on interproximal implant bone level in the early healing: A randomized clinical trial. Clin. Oral Implant. Res. 2018, 29, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, S.; Matthys, C.; Nassar, R.; Christiaens, V.; Cosyn, J.; De Bruyn, H. Adapting the vertical position of implants with a conical connection in relation to soft tissue thickness prevents early implant surface exposure: A 2-year prospective intra-subject comparison. J. Clin. Periodontol. 2018, 45, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Pico, A.; Martín-Lancharro, P.; Caneiro, L.; Nóvoa, L.; Batalla, P.; Blanco, J. Influence of abutment height and implant depth position on interproximal peri-implant bone in sites with thin mucosa: A 1-year randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Palaska, I.; Tsaousoglou, P.; Vouros, I.; Konstantinidis, A.; Menexes, G. Influence of placement depth and abutment connection pattern on bone remodeling around 1-stage implants: A prospective randomized controlled clinical trial. Clin. Oral Implant. Res. 2016, 27, e47–e56. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | % | |
|---|---|---|
| Age | ||
| Male | 56.2 ± 13.8 | - |
| Female | 59.2 ± 12.3 | - |
| Gender | ||
| Male | 25 | 50 |
| Female | 25 | 50 |
| Smoking Status | ||
| Smoker | 7 | 14 |
| Non Smoker | 43 | 86 |
| Periodontal Status | ||
| Periodontal Health | 37 | 74 |
| Chronic Periodontitis | 13 | 26 |
| MBL (mm) | Std. Error | d.f. | t-Value | p-Value | |
|---|---|---|---|---|---|
| Age | 0.00 | 0.00 | 49 | −0.49 | 0.63 |
| Gender | −0.02 | 0.08 | 49 | −0.21 | 0.83 |
| Smoking Status | 0.12 | 0.10 | 49 | 1.15 | 0.26 |
| Periodontal Status | −0.02 | 0.09 | 49 | −0.25 | 0.80 |
| Multiple Abutment Disconnections | 0.03 | 0.08 | 30 | 0.43 | 0.67 |
| MBL (mm) | Std. Error | d.f. | t-Value | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| Vertical Mucosal Thickness | 0.24 | 0.08 | 30 | 2.91 | 0.01 | 0.07; 0.41 |
| Depth of Implant Insertion | −0.23 | 0.07 | 30 | −3.37 | <0.01 | −0.37; −0.09 |
| Time Interval | MBL (mm) | Std. Error | d.f. | t-Value | p-Value | 95% CI | |
| Healing Abutment Height Short (vs. Long) | T0–T2 | −0.27 | 0.07 | 29 | −3.83 | <0.01 | −0.41; −0.13 |
| Prosthetic Abutment Height Short (vs. Long) | T2–T4 | −0.44 | 0.07 | 29 | −6.42 | <0.01 | −0.58; −0.3 |
| Insertion Depth | N° Of Implants | Mean Depth At T0 | Mean Depth At T4 |
|---|---|---|---|
| >1.5 mm | 20 | 2.01 ± 0.48 mm | 0.94 ± 0.76 mm |
| <1.5 mm | 63 | 1.00 ± 0.34 mm | 0.31 ± 0.42 mm |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, T.; Berton, F.; Salgarello, S.; Barbalonga, E.; Rapani, A.; Piovesana, F.; Gregorio, C.; Barbati, G.; Di Lenarda, R.; Stacchi, C. Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study. J. Clin. Med. 2019, 8, 1168. https://doi.org/10.3390/jcm8081168
Lombardi T, Berton F, Salgarello S, Barbalonga E, Rapani A, Piovesana F, Gregorio C, Barbati G, Di Lenarda R, Stacchi C. Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study. Journal of Clinical Medicine. 2019; 8(8):1168. https://doi.org/10.3390/jcm8081168
Chicago/Turabian StyleLombardi, Teresa, Federico Berton, Stefano Salgarello, Erika Barbalonga, Antonio Rapani, Francesca Piovesana, Caterina Gregorio, Giulia Barbati, Roberto Di Lenarda, and Claudio Stacchi. 2019. "Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study" Journal of Clinical Medicine 8, no. 8: 1168. https://doi.org/10.3390/jcm8081168