National Temporal Trend Analysis of Infective Endocarditis among Patients Infected with HIV in Spain (1997–2014): A Retrospective Study


Abstract
:1. Introduction
2. Objective
3. Materials and Methods
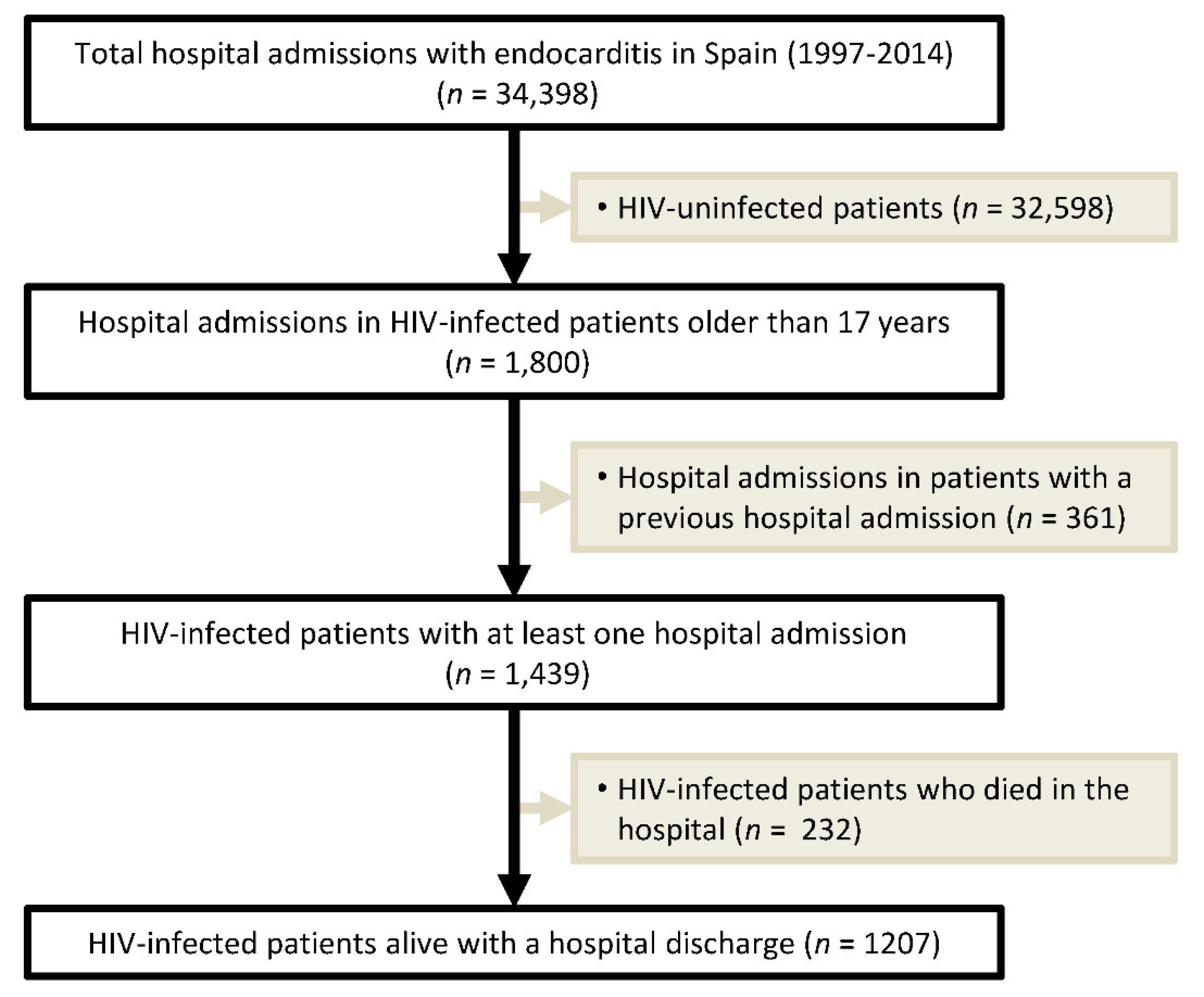
3.1. Study Population
3.2. Ethics Statement
3.3. Study Variables and Statistical Analysis
4. Results
4.1. Characteristics of the Study Population
4.2. Epidemiological Trends of Infective Endocarditis
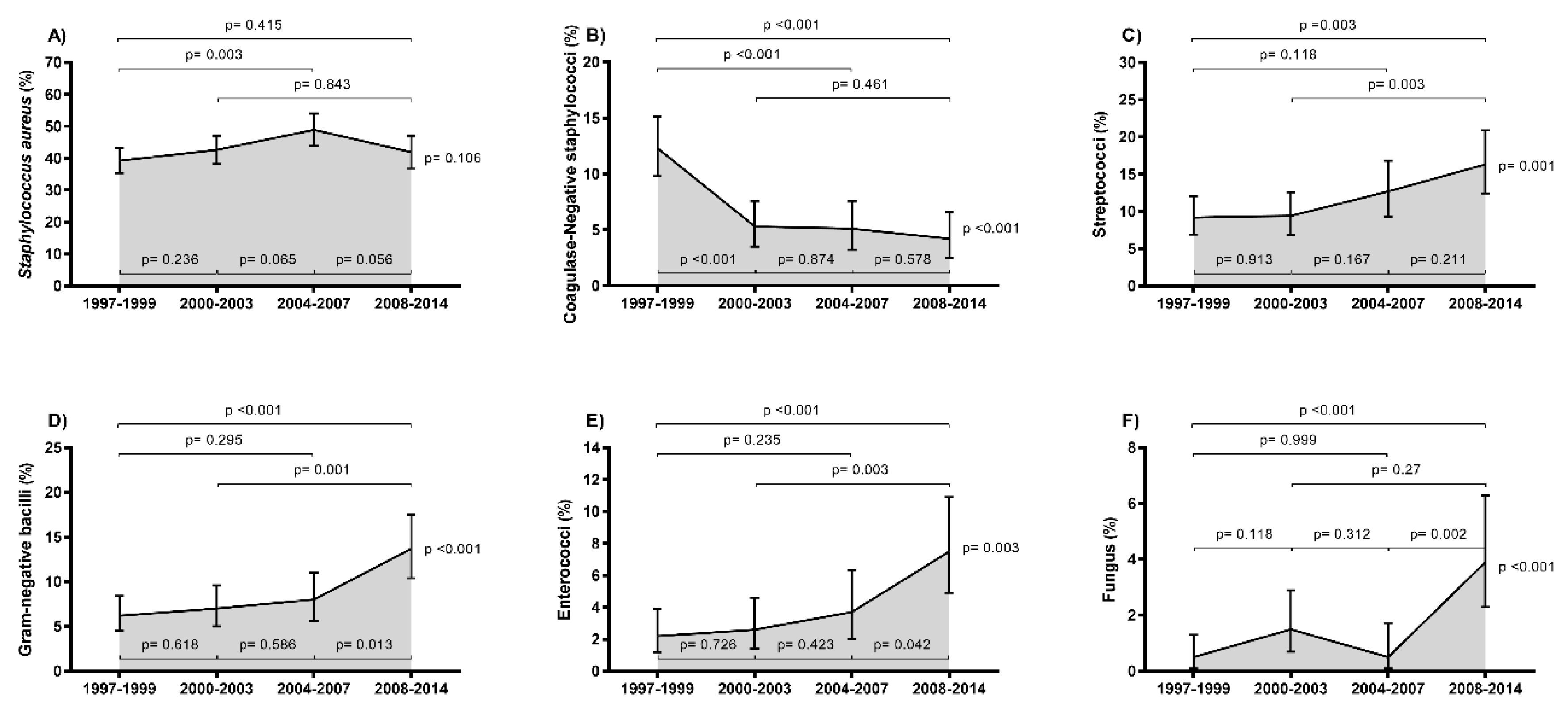
4.3. Epidemiological Trends of IE-Related Microorganisms
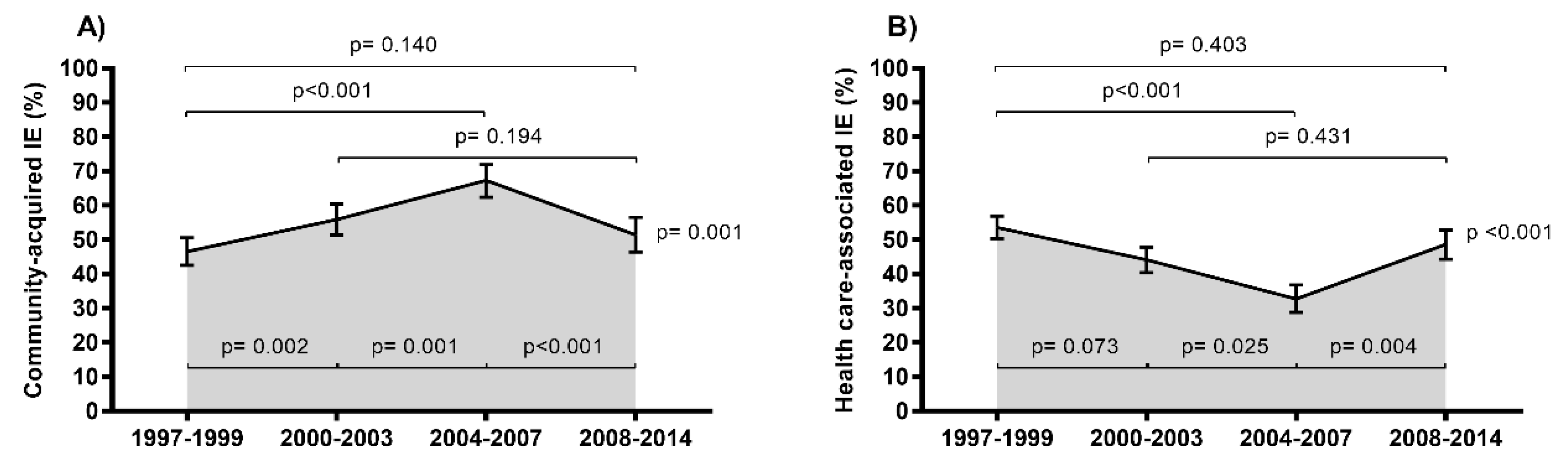
4.4. Epidemiological Trends of IE According to Mode of Acquisition
5. Discussion
6. Study Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Holland, T.L.; Baddour, L.M.; Bayer, A.S.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr. Infective endocarditis. Nat. Rev. Dis. Primers 2016, 2, 16059. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Hidalgo, N.; Almirante, B. Infective endocarditis in the xxi century: Epidemiological, therapeutic, and prognosis changes. Enferm. Infecc. Microbiol. Clin. 2012, 30, 394–406. [Google Scholar] [PubMed]
- Olmos, C.; Vilacosta, I.; Fernandez-Perez, C.; Bernal, J.L.; Ferrera, C.; Garcia-Arribas, D.; Perez-Garcia, C.N.; San Roman, J.A.; Maroto, L.; Macaya, C.; et al. The evolving nature of infective endocarditis in spain: A population-based study (2003 to 2014). J. Am. Coll. Cardiol. 2017, 70, 2795–2804. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; von Bardeleben, R.S.; Ostad, M.A.; Hobohm, L.; Munzel, T.; Konstantinides, S.; Lankeit, M. Temporal trends in the prevalence of infective endocarditis in germany between 2005 and 2014. Am. J. Cardiol. 2017, 119, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Erichsen, P.; Gislason, G.H.; Bruun, N.E. The increasing incidence of infective endocarditis in denmark, 1994-2011. Eur. J. Intern. Med. 2016, 35, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Dayer, M.J.; Jones, S.; Prendergast, B.; Baddour, L.M.; Lockhart, P.B.; Thornhill, M.H. Incidence of infective endocarditis in england, 2000–2013: A secular trend, interrupted time-series analysis. Lancet 2015, 385, 1219–1228. [Google Scholar] [CrossRef]
- Fedeli, U.; Schievano, E.; Buonfrate, D.; Pellizzer, G.; Spolaore, P. Increasing incidence and mortality of infective endocarditis: A population-based study through a record-linkage system. BMC Infect. Dis. 2011, 11, 48. [Google Scholar] [CrossRef] [PubMed]
- Joffre, J.; Dumas, G.; Aegerter, P.; Dubee, V.; Bige, N.; Preda, G.; Baudel, J.L.; Maury, E.; Guidet, B.; Ait-Oufella, H.; et al. Epidemiology of infective endocarditis in french intensive care units over the 1997–2014 period-from cub-rea network. Crit. Care 2019, 23, 143. [Google Scholar] [CrossRef]
- Deeks, S.G.; Overbaugh, J.; Phillips, A.; Buchbinder, S. Hiv infection. Nat. Rev. Dis. Primers 2015, 1, 15035. [Google Scholar] [CrossRef]
- Branas, F.; Azcoaga, A.; Garcia Ontiveros, M.; Antela, A. Chronicity, ageing and multimorbidity. Enferm. Infecc. Microbiol. Clin. 2018, 36 (Suppl. 1), 15–18. [Google Scholar]
- Bloch, M. Frailty in people living with hiv. AIDS Res. Ther. 2018, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, L.; Tatarelli, P.; Di Biagio, A. Bloodstream infections in hiv-infected patients. Virulence 2016, 7, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Ribera, E.; Miro, J.M.; Cortes, E.; Cruceta, A.; Merce, J.; Marco, F.; Planes, A.; Pare, J.C.; Moreno, A.; Ocana, I.; et al. Influence of human immunodeficiency virus 1 infection and degree of immunosuppression in the clinical characteristics and outcome of infective endocarditis in intravenous drug users. Arch. Intern. Med. 1998, 158, 2043–2050. [Google Scholar] [CrossRef] [PubMed]
- Mocroft, A.; Youle, M.; Phillips, A.N.; Halai, R.; Easterbrook, P.; Johnson, M.A.; Gazzard, B. The incidence of aids-defining illnesses in 4883 patients with human immunodeficiency virus infection. Royal free/chelsea and westminster hospitals collaborative group. Arch. Intern. Med. 1998, 158, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Mocroft, A.; Furrer, H.J.; Miro, J.M.; Reiss, P.; Mussini, C.; Kirk, O.; Abgrall, S.; Ayayi, S.; Bartmeyer, B.; Braun, D.; et al. The incidence of aids-defining illnesses at a current cd4 count >/= 200 cells/mul in the post-combination antiretroviral therapy era. Clin. Infect. Dis. 2013, 57, 1038–1047. [Google Scholar] [CrossRef]
- Gebo, K.A.; Burkey, M.D.; Lucas, G.M.; Moore, R.D.; Wilson, L.E. Incidence of, risk factors for, clinical presentation, and 1-year outcomes of infective endocarditis in an urban hiv cohort. J. Acquir. Immune Defic. Syndr. 2006, 43, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad Consumo y Bienestar Social. Sistema de Información de Atención Especializada (Siae). Available online: Https://www.Mscbs.Gob.Es/estadestudios/estadisticas/cmbdhome.Htm (accessed on 3 July 2019).
- Alvaro-Meca, A.; Palomares-Sancho, I.; Diaz, A.; Resino, R.; De Miguel, A.G.; Resino, S. Pneumocystis pneumonia in hiv-positive patients in spain: Epidemiology and environmental risk factors. J. Int. AIDS Soc. 2015, 18, 19906. [Google Scholar] [CrossRef]
- Alvaro-Meca, A.; Berenguer, J.; Diaz, A.; Micheloud, D.; Aldamiz-Echevarria, T.; Fanciulli, C.; Resino, S. Stroke in hiv-infected individuals with and without hcv coinfection in spain in the combination antiretroviral therapy era. PLoS ONE 2017, 12, e0179493. [Google Scholar] [CrossRef]
- Rockville (MD): Agency for Healthcare Research and Quality (US). Healthcare Cost and Utilization Project (hcup) Statistical Briefs. Available online: Https://www.Ncbi.Nlm.Nih.Gov/books/nbk367628/table/sb202.T4/ (accessed on 3 August 2019).
- Díez, M.; Díaz, A.; Herrando, I.; Cornejo, A. Hospital Survey of Patients with Hiv/Aids; Results 2014; Analysis of the evolution 2000–2014; Carlos III Health Institute/National Plan on AIDS: Madrid, Spain, 2015; pp. 1–39. [Google Scholar]
- Berenguer, J.; Alvarez-Pellicer, J.; Martin, P.M.; Lopez-Aldeguer, J.; Von-Wichmann, M.A.; Quereda, C.; Mallolas, J.; Sanz, J.; Tural, C.; Bellon, J.M.; et al. Sustained virological response to interferon plus ribavirin reduces liver-related complications and mortality in patients coinfected with human immunodeficiency virus and hepatitis c virus. Hepatology 2009, 50, 407–413. [Google Scholar] [CrossRef]
- Berenguer, J.; Rodriguez-Castellano, E.; Carrero, A.; Von Wichmann, M.A.; Montero, M.; Galindo, M.J.; Mallolas, J.; Crespo, M.; Tellez, M.J.; Quereda, C.; et al. Eradication of hepatitis c virus and non-liver-related non-acquired immune deficiency syndrome-related events in human immunodeficiency virus/hepatitis c virus coinfection. Hepatology 2017, 66, 344–356. [Google Scholar] [CrossRef]
- Thornton, A.C.; Jose, S.; Bhagani, S.; Chadwick, D.; Dunn, D.; Gilson, R.; Main, J.; Nelson, M.; Rodger, A.; Taylor, C.; et al. Hepatitis b, hepatitis c, and mortality among hiv-positive individuals. AIDS 2017, 31, 2525–2532. [Google Scholar] [CrossRef] [PubMed]
- Nikolopoulos, G.K.; Paraskevis, D.; Hatzitheodorou, E.; Moschidis, Z.; Sypsa, V.; Zavitsanos, X.; Kalapothaki, V.; Hatzakis, A. Impact of hepatitis b virus infection on the progression of aids and mortality in hiv-infected individuals: A cohort study and meta-analysis. Clin. Infect. Dis. 2009, 48, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Alvaro-Meca, A.; Rodriguez-Gijon, L.; Diaz, A.; Gil, A.; Resino, S. Incidence and mortality of tuberculosis disease in spain between 1997 and 2010: Impact of human immunodeficiency virus (hiv) status. J. Infect. 2014, 68, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Diez, M.; Diaz, A.; Garriga, C.; Pons, M.; Ten, A.; Marcos, H.; Gutierrez, G.; Moreno, S.; Gonzalez-Garcia, J.; Barrios, A.; et al. A low-cost, sustainable, second generation system for surveillance of people living with hiv in spain: 10-year trends in behavioural and clinical indicators, 2002 to 2011. Euro Surveill. 2014, 19, 20805. [Google Scholar] [CrossRef] [PubMed]
- El-Sadr, W.M.; Lundgren, J.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.; Burman, W.; Clumeck, N.; Cohen, C.J.; et al. Cd4+ count-guided interruption of antiretroviral treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [PubMed]
- Tumbarello, M.; Tacconelli, E.; Donati, K.G.; Citton, R.; Leone, F.; Spanu, T.; Cauda, R. Hiv-associated bacteremia: How it has changed in the highly active antiretroviral therapy (haart) era. J. Acquir. Immune Defic. Syndr. 2000, 23, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Madeddu, G.; Monforte, A.D.; Girardi, E.; Di Biagio, A.; Lo Caputo, S.; Piolini, R.; Marchetti, G.; Pellizzer, G.; Giacometti, A.; Galli, L.; et al. Cd4 cell count and the risk of infective and non-infective serious non-aids events in hiv-positive persons seen for care in italy. J. Int. AIDS Soc. 2014, 17, 19509. [Google Scholar] [CrossRef]
- Kanters, S.; Vitoria, M.; Doherty, M.; Socias, M.E.; Ford, N.; Forrest, J.I.; Popoff, E.; Bansback, N.; Nsanzimana, S.; Thorlund, K.; et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of hiv infection: A systematic review and network meta-analysis. Lancet HIV 2016, 3, e510–e520. [Google Scholar] [CrossRef]
- Iacob, S.A.; Iacob, D.G.; Jugulete, G. Improving the adherence to antiretroviral therapy, a difficult but essential task for a successful hiv treatment-clinical points of view and practical considerations. Front. Pharmacol. 2017, 8, 831. [Google Scholar] [CrossRef]
- Tsabedze, N.; Vachiat, A.; Zachariah, D.; Manga, P. A new face of cardiac emergencies: Human immunodeficiency virus-related cardiac disease. Cardiol. Clin. 2018, 36, 161–170. [Google Scholar] [CrossRef]
- Vogkou, C.T.; Vlachogiannis, N.I.; Palaiodimos, L.; Kousoulis, A.A. The causative agents in infective endocarditis: A systematic review comprising 33,214 cases. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1227–1245. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Calendar Periods | |||||
|---|---|---|---|---|---|---|
| 1997–1999 | 2000–2003 | 2004–2007 | 2008–2014 | p-Value | ||
| Number of patients | 1800 | 594 | 474 | 376 | 358 | |
| Male | 1494 (83%) | 496 (83.5%) | 398 (84.3%) | 302 (80.3%) | 298 (83.2%) | 0.454 |
| Age, years | ||||||
| <30 | 413 (22.9%) | 251 (42.3%) | 86 (18.2%) | 45 (12%) | 31 (8.7%) | <0.001 |
| 30–34 | 405 (22.5%) | 159 (26.8%) | 136 (28.8%) | 68 (18.1%) | 42 (11.7%) | <0.001 |
| 35–39 | 439 (24.4%) | 116 (19.5%) | 135 (28.6%) | 118 (31.4%) | 70 (19.6%) | 0.301 |
| 40–44 | 302 (16.8%) | 50 (8.4%) | 72 (15.3%) | 101 (26.9%) | 79 (22.1%) | <0.001 |
| >45 | 241 (13.4%) | 18 (3%) | 43 (9.1%) | 44 (11.7%) | 136 (38%) | <0.001 |
| Substances of abuse | ||||||
| Drugs | 386 (21.4%) | 73 (12.3%) | 91 (19.3%) | 110 (29.3%) | 112 (31.3%) | <0.001 |
| Alcohol | 16 (0.9%) | 2 (0.3%) | 3 (0.6%) | 5 (1.3%) | 6 (1.7%) | 0.003 |
| Tobacco | 358 (19.9%) | 56 (9.4%) | 84 (17.8%) | 105 (27.9%) | 113 (31.6%) | <0.001 |
| Comorbidities | ||||||
| Diabetes | 25 (1.4%) | 1 (0.2%) | 7 (1.5%) | 5 (1.3%) | 12 (3.4%) | <0.001 |
| Hypertension | 25 (1.4%) | 1 (0.2%) | 5 (1.1%) | 4 (1.1%) | 15 (4.2%) | <0.001 |
| Coronary artery disease | 15 (0.8%) | 1 (0.2%) | 2 (0.4%) | 6 (1.6%) | 6 (1.7%) | 0.004 |
| Peripheral vascular disease | 51 (2.8%) | 9 (1.5%) | 15 (3.2%) | 19 (5.1%) | 8 (2.2%) | 0.148 |
| Cerebrovascular Disease | 25 (1.4%) | 5 (0.8%) | 6 (1.3%) | 10 (2.7%) | 4 (1.1%) | 0.317 |
| Cancer | 16 (0.9%) | 4 (0.7%) | 4 (0.8%) | 2 (0.5%) | 6 (1.7%) | 0.256 |
| Liver disease | 186 (10.3%) | 31 (5.2%) | 33 (7%) | 61 (16.2%) | 61 (17%) | <0.001 |
| Chronic obstructive pulmonary disease | 25 (1.4%) | 0 (0%) | 4 (0.8%) | 9 (2.4%) | 12 (3.4%) | <0.001 |
| Chronic kidney disease | 20 (1.1%) | 0 (0%) | 0 (0%) | 0 (0%) | 20 (5.6%) | <0.001 |
| Coinfections | ||||||
| Mycobacteria | 51 (2.8%) | 22 (3.7%) | 14 (3%) | 6 (1.6%) | 9 (2.5%) | <0.001 |
| Pneumocystis | 29 (1.6%) | 7 (1.2%) | 10 (2.1%) | 8 (2.1%) | 4 (1.1%) | 0.804 |
| Hepatitis B | 151 (8.4%) | 24 (4%) | 54 (11.4%) | 36 (9.6%) | 37 (10.3%) | <0.001 |
| Hepatitis C | 421 (40.1%) | 86 (14.5%) | 185 (39.2%) | 234 (62.2%) | 216 (60.3%) | <0.001 |
| Predisposing factors | ||||||
| Congenital heart disease | 8 (0.4%) | 1 (0.2%) | 1 (0.2%) | - | 6 (1.7%) | 0.008 |
| Valve surgery | 75 (4.3%) | 21 (2.5%) | 15 (3.2%) | 16 (4.3%) | 23 (6.4%) | 0.029 |
| Infection of cardiac device or implant | 32 (1.8%) | 4 (0.7%) | 7 (1.5%) | 8 (2.1%) | 13 (3.6%) | <0.001 |
| History of pacemaker or defibrillator placement | 13 (0.7%) | 2 (0.3%) | 3 (0.6%) | 1 (0.3%) | 7 (2%) | 0.025 |
| History of prosthetic valve replacement | 98 (5.8%) | 25 (4.2%) | 24 (5.1%) | 19 (5.1%) | 30 (8.4%) | 0.009 |
| Receiving intravenous therapy or home care | 53 (3%) | 7 (1.2%) | 13 (2.8%) | 16 (4.3%) | 17 (4.7%) | <0.001 |
| Hemodialysis dependent | 31 (1.7%) | 4 (0.7%) | 5 (1.1%) | 4 (1.1%) | 18 (5%) | <0.001 |
| Urgent admission | 1593 (88.5%) | 524 (88.2%) | 429 (90.9%) | 331 (88%) | 309 (86.3%) | 0.618 |
| Surgical conditions | 200 (11.1%) | 65 (10.9%) | 65 (13.8%) | 42 (11.2%) | 28 (7.8%) | 0.162 |
| Number of organ failures | ||||||
| 0 | 1528 (84.9%) | 527 (88.7%) | 409 (86.7%) | 305 (81.1%) | 287 (80.2%) | <0.001 |
| 1 | 228 (12.7%) | 62 (10.4%) | 53 (11.2%) | 56 (14.9%) | 57 (15.9%) | 0.034 |
| ≥2 | 44 (2.9%) | 5 (0.9%) | 10 (2.4%) | 15 (4.9%) | 14 (4.9%) | 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Moreno, M.F.; Ryan, P.; Alvaro-Meca, A.; Valencia, J.; Tamayo, E.; Resino, S. National Temporal Trend Analysis of Infective Endocarditis among Patients Infected with HIV in Spain (1997–2014): A Retrospective Study. J. Clin. Med. 2019, 8, 1167. https://doi.org/10.3390/jcm8081167
Muñoz-Moreno MF, Ryan P, Alvaro-Meca A, Valencia J, Tamayo E, Resino S. National Temporal Trend Analysis of Infective Endocarditis among Patients Infected with HIV in Spain (1997–2014): A Retrospective Study. Journal of Clinical Medicine. 2019; 8(8):1167. https://doi.org/10.3390/jcm8081167
Chicago/Turabian StyleMuñoz-Moreno, Maria Fe, Pablo Ryan, Alejandro Alvaro-Meca, Jorge Valencia, Eduardo Tamayo, and Salvador Resino. 2019. "National Temporal Trend Analysis of Infective Endocarditis among Patients Infected with HIV in Spain (1997–2014): A Retrospective Study" Journal of Clinical Medicine 8, no. 8: 1167. https://doi.org/10.3390/jcm8081167