1. Introduction
Antiphospholipid syndrome (APS) is a rare systemic autoimmune disorder characterized by vascular thrombosis of large, medium or small vessels, pregnancy morbidity and persistently positive antiphospholipid antibodies (aPL), including lupus anticoagulant, anticardiolipin antibodies and/or anti–β2-glycoprotein I antibodies [
1]. These antibodies may be detected individually or in combinations of two or three (double- or triple-positive aPL, respectively). APS may occur in its primary form (primary APS, PAPS) or in correlation with other autoimmune diseases, mainly systemic lupus erythematosus (SLE/APS) [
2].
Heart involvement is one of the major complications in APS, including valve and ischemic heart disease [
3,
4,
5]. In a multi-center European cohort of 1000 patients with APS, heart valve disease—mostly valve thickening and/or vegetation—was observed in 30% of patients, while ischemic heart disease manifesting mainly as myocardial infarction (MI), was demonstrated in 5.5% of patients [
2]. MI was the most common cause of death after bacterial infections among patients with APS, referring to 19% of deaths in a 5-year follow-up period [
2]. Other types of heart disease have also been reported in APS, including coronary vasospasm, known as variant (Prinzmetal’s) angina and syndrome X [
6,
7], myocardial ischemia associated with thrombotic cardiac microvasculopathy [
8], and endomyocardial fibrosis due to coronary microcirculation defects [
9].
Cardiovascular magnetic resonance imaging (CMR) is a non-invasive, non-ionizing radiation imaging modality that can assess cardiac geometry and function, myocardial perfusion and fibrosis [
10,
11]. Only one previous study used CMR in APS that showed a significantly higher prevalence of occult myocardial fibrosis associated with microvascular disease, expressed as late gadolinium enhancement (LGE), in 27 patients with APS compared to 81 healthy controls [
12]. Using exercise or pharmacological stress with adenosine (stress CMR), a three- to four-fold increase in myocardial blood flow (MBF) can occur in healthy individuals. The ratio of maximum stress MBF after adenosine use to baseline rest is defined as a myocardial perfusion reserve index (MPRI) (10). The MPRI indicates the functional severity of a coronary lesion, and is of substantial additive value because an anatomic coronary stenosis does not necessarily correspond to a reduction of coronary blood flow. MPRI can distinguish between normal subjects and patients with coronary artery disease (CAD) of either macrovascular or microvascular etiology (lesions in epicardial coronary arteries or micro-circulation defects, respectively) [
13,
14,
15].
Previous stress CMR studies by our group and others have demonstrated perfusion abnormalities by means of MPRI in patients with cardiac syndrome X [
16], Raynaud’s phenomenon [
17] and SLE [
18], with a much higher sensitivity than conventional imaging modalities. The CE-MARC study showed also the superiority of CMR over single photon emission tomography (SPECT) for the detection of myocardial ischemia and fibrosis [
19]. No comparison between APS patients and healthy controls has been carried out to date with regard to stress CMR findings [
20].
Our aim was to examine myocardial perfusion defects using stress CMR in patients with PAPS and SLE/APS without known CAD, in comparison with age- and sex-matched healthy controls. We also evaluated potential associations between CMR findings and APS-related and classic CVD risk factors and coronary angiography findings.
3. Results
Forty four patients with APS (22 with PAPS, 22 with SLE-APS) were included in the study (all Caucasian, 64% female, mean age: 44 ± 13 years, median disease duration: 12.0 (5.5, 21.0). One to one age- and sex-matching of 44 healthy controls without any history of cardiac disease was performed (mean age: 44 ± 11 years, 64% female). Baseline characteristics of all APS patients, and comparisons between those with PAPS and SLE/APS, are presented in
Table 1. Patients with PAPS had a significantly higher prevalence of a previous stroke of non-atherosclerotic origin [5 (23%) vs. 0 (0%)
p = 0.018] and recurrent thrombosis [12 (55%) vs. 5 (23%)
p = 0.030], compared to SLE/APS patients. Additionally, PAPS patients with detectable TnT (above the 99th percentile upper reference limit of 13.9 ng/L) had significantly higher hs-TnT levels compared to those with SLE/APS and detectable TnT [19.5 (7.0–36.0) vs. 6.7 (4.3–9.0),
p = 0.040], but the proportion of patients with hs-TnT below the detection limit did not differ significantly between the two groups [15 (68%) vs. 12 (55%),
p = 0.35]. The median MPRI in the entire APS cohort was 1.48 (0.9, 1.9).
Descriptive statistics and comparisons between the CMR indices of APS patients and their matched controls are presented in
Table 2. The LV volumes and ejection fractions did not differ significantly between the two groups. However, APS patients had a significantly lower median LV mass compared to matched controls [81.0 (65.5–98.5) vs. 121.5 (112.0–140.0),
p < 0.001]. Median RVEDV and RVESV were also lower in APS patients compared to controls, but only RVEDV reached statistical significance [RVEDV: 109.0 (84.0–126.5) vs. 125.0 (120.0–150.0),
p < 0.001; RVESV 38.5 (29.0–48.5) vs. 45.0 (40.0–48.0),
p = 0.057]. There was a trend for higher median RVEF in APS patients compared to controls, but this also did not reach statistical significance (
p = 0.079).
Median MPRI was significantly lower in APS patients compared to healthy controls [1.48 (0.9–1.9) vs. 2.7 (2.2–3.2),
p < 0.001]. Sixteen (36%) APS patients had visible areas of myocardial scar, expressed as LGE, compared to none of the healthy controls (
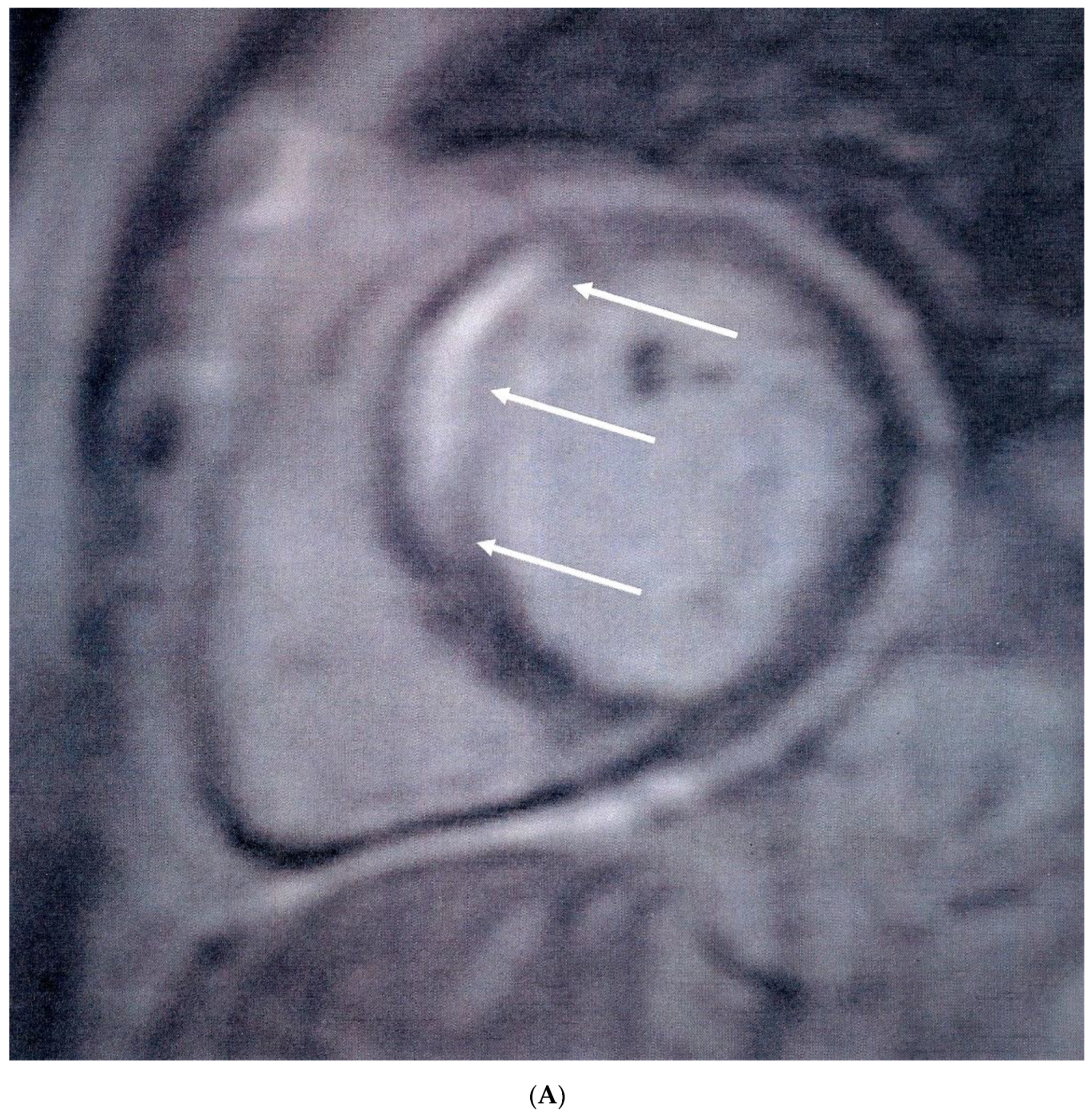
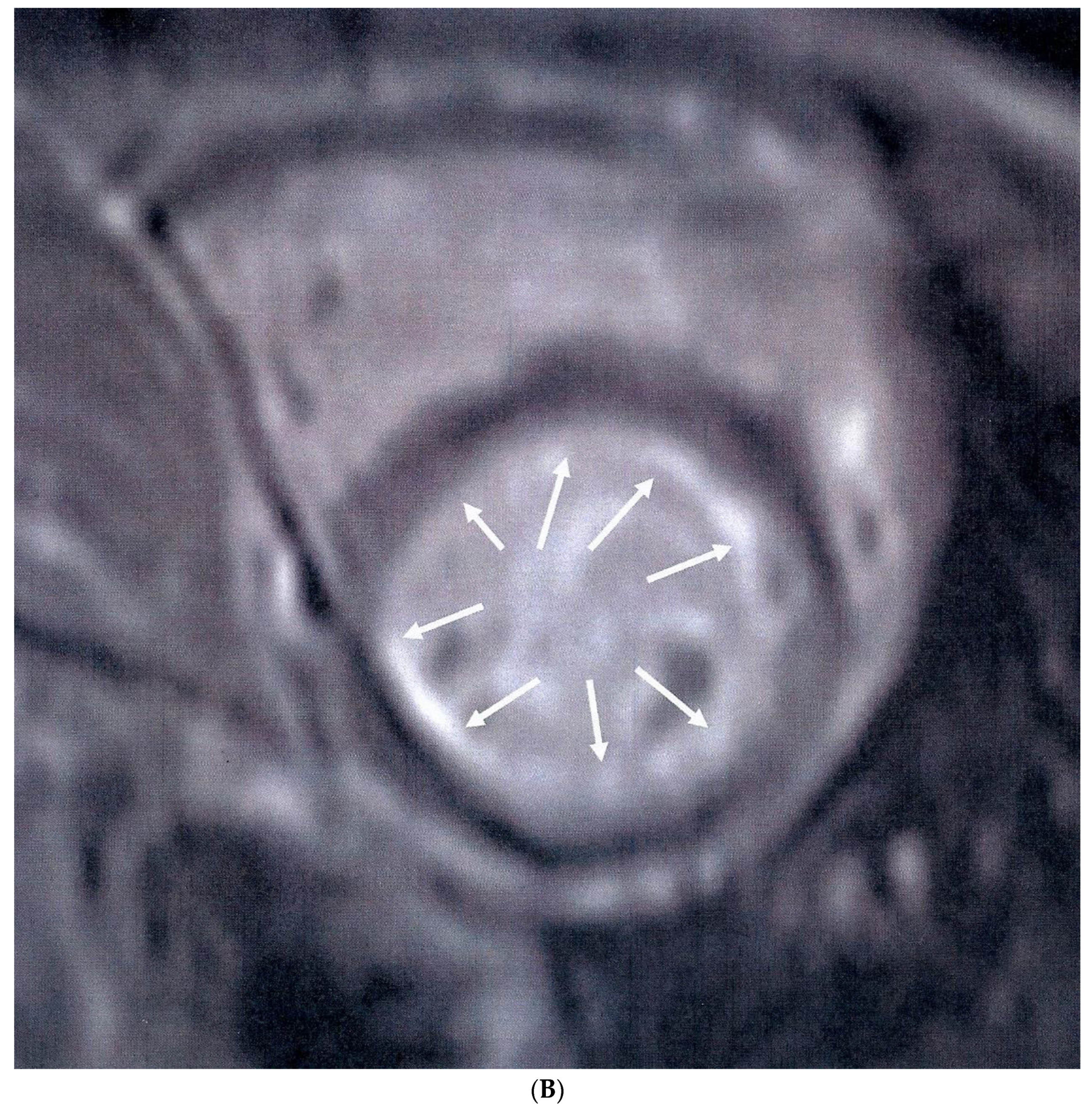
p < 0.001). Myocardial scar following the distribution of coronary arteries was identified in nine (20%) patients (five in the anteroseptal and four in the inferolateral LV wall) (
Figure 1A), while diffuse subendocardial fibrosis (DSF) (
Figure 1B) was identified in seven (16%) patients. In patients with a positive LGE, the median LGE values expressed as percentage of LV mass were 4.5 (3.5–7.5). Coronary angiography was performed in 12 of the 16 APS patients with positive LGE, with macrovascular (obstructive) CAD identified only in two patients, one of which subsequently underwent angioplasty of the left anterior descending artery. Three of 10 patients with otherwise normal coronary angiography findings had abnormal LVEF values (<55%) and concomitant low MPRI values below the median of the APS group (<1.48).
When comparing patients with MPRI above and below the median value of the APS group (
Table 3), no significant differences were identified in any demographic, clinical, laboratory and CMR characteristics, with the exception of obstetric APS and LVEF. The former was significantly less prevalent in patients with higher MPRI values [3 (15%) vs. 8 (33%),
p = 0.029], and the latter was significantly higher in patients with higher MPRI values [61.5 (58.5, 65.0) vs. 64.5 (62.5, 68.0),
p = 0.041], albeit still largely within normal limits (>55%). Additionally, more male patients had a lower MPRI, but this did not reach statistical significance [11 (46%) vs. 5 (75%),
p = 0.153]. Finally, there was a trend for higher MPRI values in patients receiving treatment with corticosteroids compared to those not treated with corticosteroids, but this did not reach any statistical significance [9 (45%) vs. 5 (21%),
p = 0.087]. A similar non-significant trend for higher MPRI was identified in patients treated with acetylsalicylic acid (ASA, Aspirin 100 mg daily) [12 (50%) vs. 5 (25%),
p = 0.09]. No association with hydroxychloroquine use, or hsCRP and hsTnT levels was detected. Of the aforementioned variables, those with a
p-value < 0.1 were included in a multivariable linear regression model for predicting MPRI values. Obstetric APS was replaced with female gender, as it would preclude the analysis of male patients. However, this did not lead to any statistically significant results (
Table 4). No significant associations were also found between LGE and APS characteristics, classic CVD risk factors, or the hsCRP and hsTnT levels, in both descriptive (
Table 5) and multivariate analysis.
At the twelve month follow-up, three patients (6.8%) experienced CAD complications (1 MI, and 2 unstable angina), importantly those with the lowest MPRI values (0.48, 0.56 and 0.58, respectively). However, meaningful statistical analyses could not be performed due to small numbers.
4. Discussion
This is the first study to our knowledge that evaluated the presence of silent myocardial ischemia and fibrosis by stress CMR in patients with APS. The most striking finding of our study is the detection of highly-reduced MPRI compared with age- and sex-matched healthy controls, irrespective of the presence of LGE. Myocardial fibrosis, expressed as LGE, was detected in one third of APS patients, of which only two patients had abnormal coronary angiography findings. These findings demonstrate that even in asymptomatic APS patients without evidence of fibrosis or macrovascular CAD detected by coronary angiography, silent myocardial ischemia may exist.
We also identified for the first time a significantly reduced LV mass in patients with APS compared to controls. Although it may be argued that the athletic activities followed by the healthy controls in our study might lead to LV mass increase, the actual difference between the groups is larger than what might reasonably be explained by exercise-induced LV hypertrophy alone [
28]. On the other hand, little is known about myocardial mass changes preceding clinically overt cardiac involvement. According to currently published literature, reduced LV mass has been demonstrated in patients with rheumatoid arthritis, and was considered a predisposing factor for developing future heart failure [
29]. Nevertheless, evidence is lacking about which factors can influence LV mass in APS apart from hemodynamics.
Myocardial perfusion defects in APS patients without prior CAD were previously examined by three studies using contrast echocardiography and scintigraphy with radionuclides [
30], SPECT [
31] and N-ammonia PET [
32], respectively. Perfusion abnormalities were detected in 30%, 57.7% and 38.8% of 11, 26, and 18 patients tested, respectively. The limitations of these studies were the small number of included patients, the lack of comparison groups, and the use of imaging modalities of inferior diagnostic performance for myocardial perfusion assessment compared to CMR [
14,
22]. The only study that used CMR in APS showed a significantly higher prevalence of silent myocardial fibrosis compared to healthy controls [
12]. No previous study examined silent myocardial ischemia using stress CMR imaging.
Our findings have important clinical implications for stratifying patients with APS at risk for heart disease. The early detection of reduced MPRI can be either due to macro- or micro-vascular CAD. If there is evidence of macro-vascular CAD, presenting as reduced MPRI and/or positive LGE following the distribution of coronary arteries, coronary angiography is indicated with subsequent standard interventional treatment, as needed. Microvascular disease on the other hand, presents as equally reduced MPRI in all myocardial territories with/or without DSF. In our study, we identified only two patients with macrovascular CAD, with the majority having microvascular CAD instead. Next to the aforementioned implications of low MPRI for microvascular CAD, the assessment of myocardial scar in asymptomatic APS patients has also important clinical implications for macrovascular CAD.
Firstly, it carries a prognostic value for the development of future arrhythmia [
33] and/or heart failure [
34] and secondly, it motivates and can justify further investigation with coronary angiography [
34]. Finally, it may prompt initiation of specific medication use including ACE-inhibitors, β-adrenoreceptor blockers or aspirin [
35].
These findings, in addition to the development of CAD events over a 12-month follow-up in three APS patients with the lowest MPRI at CMR, have also important therapeutic implications in APS. Given that almost all patients with APS were on adequate treatment with vitamin K antagonists, this finding raises questions about the presumed efficacy of currently employed anticoagulation strategies (as monotherapy) in criteria and non-criteria APS manifestations [
36,
37], and the potential need for additional cardioprotective treatment in patients with reduced MPRI [
20]. In diabetic patients with abnormal MPRI without obstructive CAD, the use of antianginal agents was shown to improve microvascular ischemia [
38], however, these effects in APS should be independently investigated in well-designed prospective studies. Lifestyle modification and aggressive monitoring and management of classic CVD risk factors are included in the general measures for the management of APS in adults [
39,
40].
Interestingly, no significant associations were detected in our study between abnormal MPRI or LGE and APS clinical and laboratory characteristics or traditional CVD risk factors. A previous study [
12] showed a trend between myocardial scarring and APS features, such as disease duration and positivity for anti-β2-glycoprotein I antibodies, however, these associations did not reach statistical significance. In addition, we found no association between reduced MPRI and hs-TnT or hs-CRP levels. In a recent study of SLE patients [
41], hs-TnT was significantly associated with myocardial edema detected by T2 mapping that was not evaluated by our stress CMR protocol. Patients receiving Aspirin treatment and those on corticosteroids tended to have higher MPRI values, but these trends did not reach statistical significance. However, inferences about these associations cannot be accurately drawn due to the relatively small number of our study population.
In addition to adenosine stress CMR use for the detection of silent perfusion abnormalities in APS, other strengths of the study are the comparison of CMR indices with coronary angiography findings in patients with abnormal LGE, and the 12-month follow-up of patients for CAD events. Our study has also some limitations. The relatively small number of patients might have precluded the identification of significant associations between MPRI and APS-related or classic CVD risk factors. Furthermore, novel CMR indices for the detection of diffuse myocardial edema and fibrosis (T1, T2 mapping and extracellular volume fraction quantification) [
20] were not available in our department at the time of the CMR examination. In addition, coronary angiography was performed only in patients with an LGE presence. It could thus be argued that an unidentified macrovascular obstructive component in the coronary circulation might also be at work, given that microvascular disease is not the sole process leading to MPRI reductions without concomitant fibrosis.
In conclusion, silent myocardial ischemia and myocardial fibrosis are common in APS, independent of APS-related and classic CVD risk factors, hs-CRP and hs-TnT levels or coronary angiography findings. Our results support the diagnostic value of the CMR examination for the detection of silent micro- or macro-vascular CAD in APS. Early identification of ischemic heart lesions by CMR may motivate further cardiac investigation and an early initiation of cardioprotective treatment. In addition, our findings raise questions about the efficacy of currently-used therapeutic approaches for the prevention of CAD in APS, underlining the need for a re-evaluation of current practices by future studies.





{kind=link}
{kind=link}