Efficacy and Feasibility of Salvage Re-Irradiation with CyberKnife for In-Field Neck Lymph Node Recurrence: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. Treatment
2.3. Follow-Up Evaluations and Patient Data
2.4. Statistical Analysis
2.5. Ethics Approval and Consent to Participate
3. Results
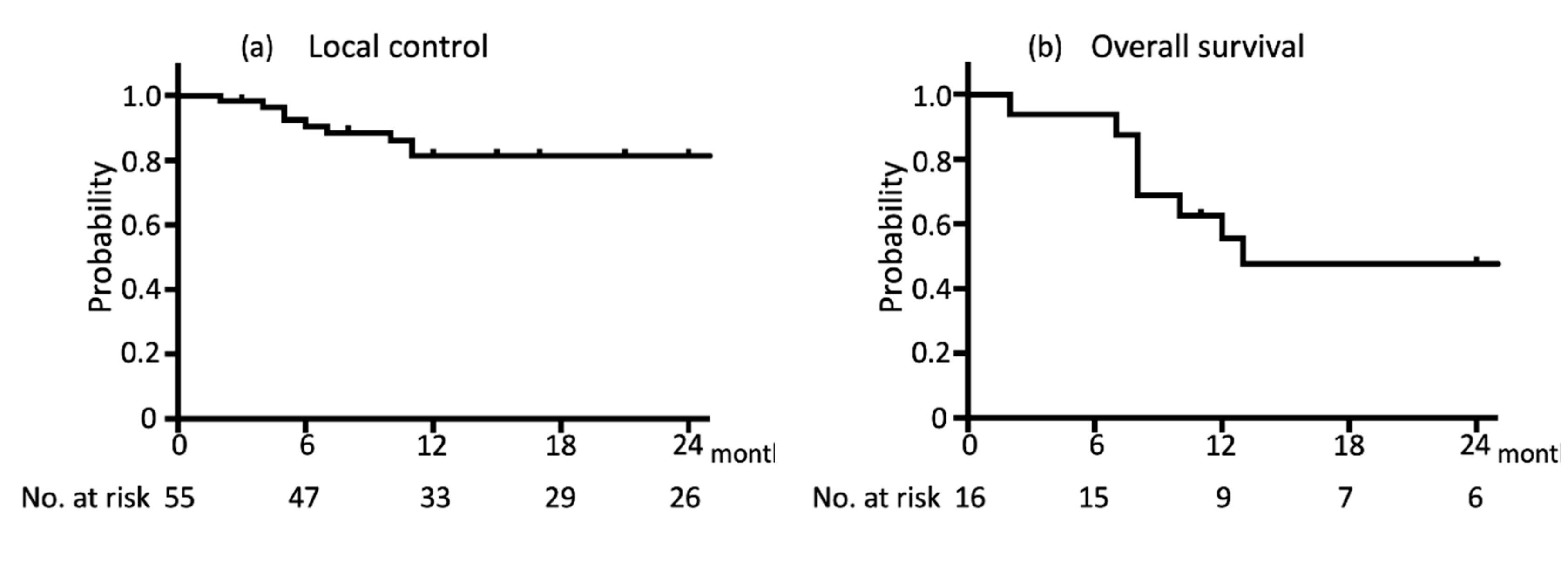
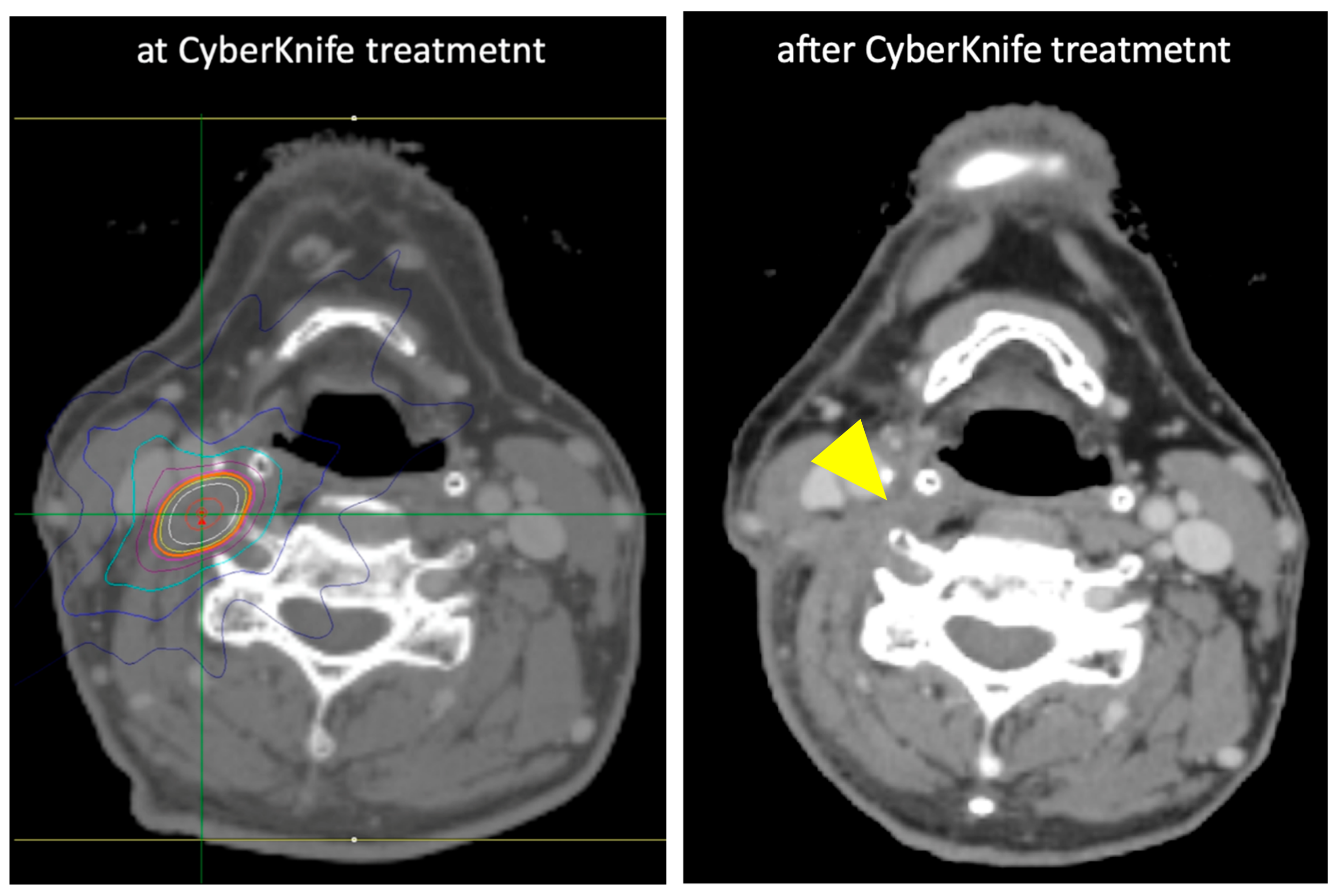
3.1. Tumor Response and LC after Treatment
3.2. Adverse Effects
3.3. Dose–Volume Histogram
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Cooper, J.S.; Porter, K.; Mallin, K.; Hoffman, H.T.; Weber, R.S.; Ang, K.K.; Gay, E.G.; Langer, C.J. National Cancer Database report on cancer of the head and neck: 10-Year update. Head Neck 2009, 31, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Benasso, M.; Bonelli, L.; Numico, G.; Corvo, R.; Sanguineti, G.; Rosso, R.; Vitale, V.; Merlano, M. Treatment with cisplatin and fluorouracil alternating with radiation favourably affects prognosis of inoperable squamous cell carcinoma of the head and neck: Results of a multivariate analysis on 273 patients. Ann. Oncol. 1997, 8, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Browman, G.P.; Hodson, D.I.; Mackenzie, R.J.; Bestic, N.; Zuraw, L.; Hodson, D.I.; Mackenzie, R.J.; Bestic, N.; Zuraw, L. Cancer Care Ontario practice guideline initiative head and neck Cancer disease site group. Choosing a concomitant chemotherapy and radiotherapy regimen for squamous cell head and neck cancer: A systematic review of the published literature with subgroup analysis. Head Neck 2001, 23, 579–589. [Google Scholar] [PubMed]
- Merlano, M.; Benasso, M.; Corvo, R.; Rosso, R.; Vitale, V.; Blengio, F.; Numico, G.; Margarino, G.; Bonelli, L.; Santi, L. Five-year update of a randomized trial of alternating radiotherapy and chemotherapy compared with radiotherapy alone in treatment of unresectable squamous cell carcinoma of the head and neck. J. Natl. Cancer Inst. 1996, 88, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Zakotnik, B.; Smid, L.; Budihna, M.; Lesnicar, H.; Soba, E.; Furlan, L.; Zargi, M. Concomitant radiotherapy with mitomycin C and bleomycin compared with radiotherapy alone in inoperable head and neck cancer: Final report. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 1121–1127. [Google Scholar] [CrossRef]
- Pignon, J.P.; Bourhis, J.; Domenge, C.; Designe, L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: Three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet 2000, 355, 949–955. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maitre, A.; Maillard, E.; Bourhis, J.; Group M-NC. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiol. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef]
- Haddad, R.; O’Neill, A.; Rabinowits, G.; Tishler, R.; Khuri, F.; Adkins, D.; Clark, J.; Sarlis, N.; Lorch, J.; Beitler, J.J.; et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 257–264. [Google Scholar] [CrossRef]
- Dawson, L.A.; Anzai, Y.; Marsh, L.; Martel, M.K.; Paulino, A.; Ship, J.A.; Eisbruch, A. Patterns of local-regional recurrence following parotid-sparing conformal and segmental intensity-modulated radiotherapy for head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1117–1126. [Google Scholar] [CrossRef]
- Temam, S.; Pape, E.; Janot, F.; Wibault, P.; Julieron, M.; Lusinchi, A.; Mamelle, G.; Marandas, P.; Luboinski, B.; Bourhis, J. Salvage surgery after failure of very accelerated radiotherapy in advanced head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1078–1083. [Google Scholar] [CrossRef]
- Liu, M.; Zhao, K.; Chen, Y.; Jiang, G.L. Evaluation of the value of ENI in radiotherapy for cervical and upper thoracic esophageal cancer: A retrospective analysis. Radiat. Oncol. 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Mabanta, S.R.; Mendenhall, W.M.; Stringer, S.P.; Cassisi, N.J. Salvage treatment for neck recurrence after irradiation alone for head and neck squamous cell carcinoma with clinically positive neck nodes. Head Neck 1999, 21, 591–594. [Google Scholar] [CrossRef]
- Hoebers, F.; Heemsbergen, W.; Moor, S.; Lopez, M.; Klop, M.; Tesselaar, M.; Rasch, C. Reirradiation for head-and-neck cancer: Delicate balance between effectiveness and toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e111–e118. [Google Scholar] [CrossRef] [PubMed]
- Langendijk, J.A.; Kasperts, N.; Leemans, C.R.; Doornaert, P.; Slotman, B.J. A phase II study of primary reirradiation in squamous cell carcinoma of head and neck. Radiotherapy and oncology. J. Eur. Soc. Ther. Radiol. Oncol. 2006, 78, 306–312. [Google Scholar] [CrossRef]
- Langer, C.J.; Harris, J.; Horwitz, E.M.; Nicolaou, N.; Kies, M.; Curran, W.; Wong, S.; Ang, K. Phase II study of low-dose paclitaxel and cisplatin in combination with split-course concomitant twice-daily reirradiation in recurrent squamous cell carcinoma of the head and neck: Results of Radiation Therapy Oncology Group Protocol 9911. J. Clin. Oncol. 2007, 25, 4800–4805. [Google Scholar] [CrossRef]
- Spencer, S.A.; Harris, J.; Wheeler, R.H.; Machtay, M.; Schultz, C.; Spanos, W.; Rotman, M.; Meredith, R.; Ang, K.K. Final report of RTOG 9610, a multi-institutional trial of reirradiation and chemotherapy for unresectable recurrent squamous cell carcinoma of the head and neck. Head Neck 2008, 30, 281–288. [Google Scholar] [CrossRef]
- Jacobs, C.; Lyman, G.; Velezgarcia, E.; Sridhar, K.S.; Knight, W.; Hochster, H.; Goodnough, L.T.; Mortimer, J.E.; Einhorn, L.H.; Schacter, L.; et al. A Phase-III Randomized Study Comparing Cisplatin and Fluorouracil as Single Agents and in Combination for Advanced Squamous-Cell Carcinoma of the Head and Neck. J. Clin. Oncol. 1992, 10, 257–263. [Google Scholar] [CrossRef]
- Jacobs, C.; Meyers, F.; Hendrickson, C.; Kohler, M.; Carter, S. A randomized phase III study of cisplatin with or without methotrexate for recurrent squamous cell carcinoma of the head and neck. A Northern California Oncology Group study. Cancer 1983, 51, 1563–1569. [Google Scholar] [CrossRef]
- Higginson, D.S.; Morris, D.E.; Jones, E.L.; Clarke-Pearson, D.; Varia, M.A. Stereotactic body radiotherapy (SBRT): Technological innovation and application in gynecologic oncology. Gynecol. Oncol. 2011, 120, 404–412. [Google Scholar] [CrossRef]
- Soltys, S.G.; Adler, J.R.; Lipani, J.D.; Jackson, P.S.; Choi, C.Y.; Puataweepong, P.; White, S.; Gibbs, I.C.; Chang, S.D. Stereotactic radiosurgery of the postoperative resection cavity for brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 187–193. [Google Scholar] [CrossRef]
- Van der Voort van Zyp, N.C.; Prevost, J.B.; Hoogeman, M.S.; Praag, J.; van der Holt, B.; Levendag, P.C.; van Klaveren, R.J.; Pattynama, P.; Nuyttens, J.J. Stereotactic radiotherapy with real-time tumor tracking for non-small cell lung cancer: Clinical outcome. Radiotherapy and oncology. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 91, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, M.; Ozyigit, G.; Yazici, G.; Dogan, A.; Yildiz, F.; Zorlu, F.; Gürkaynak, M.; Gullu, I.H.; Hosal, S.; Akyol, F. Salvage reirradiaton with stereotactic body radiotherapy for locally recurrent head-and-neck tumors. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Heron, D.E.; Ferris, R.L.; Karamouzis, M.; Andrade, R.S.; Deeb, E.L.; Burton, S.; Gooding, W.E.; Branstetter, B.F.; Mountz, J.M.; Johnson, J.T.; et al. Stereotactic body radiotherapy for recurrent squamous cell carcinoma of the head and neck: Results of a phase I dose-escalation trial. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Roh, K.W.; Jang, J.S.; Kim, M.S.; Sun, D.I.; Kim, B.S.; Jung, S.L.; Kang, J.H.; Yoo, E.J.; Yoon, S.C.; Jang, H.S.; et al. Fractionated stereotactic radiotherapy as reirradiation for locally recurrent head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1348–1355. [Google Scholar] [CrossRef]
- Rwigema, J.C.; Heron, D.E.; Ferris, R.L.; Gibson, M.; Quinn, A.; Yang, Y.; Ozhasoglu, C.; Burton, S. Fractionated stereotactic body radiation therapy in the treatment of previously-irradiated recurrent head and neck carcinoma: Updated report of the University of Pittsburgh experience. Am. J. Clin. Oncol. 2010, 33, 286–293. [Google Scholar] [CrossRef]
- Siddiqui, F.; Patel, M.; Khan, M.; McLean, S.; Dragovic, J.; Jin, J.Y.; Movsas, B.; Ryu, S. Stereotactic body radiation therapy for primary, recurrent, and metastatic tumors in the head-and-neck region. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1047–1053. [Google Scholar] [CrossRef]
- Unger, K.R.; Lominska, C.E.; Deeken, J.F.; Davidson, B.J.; Newkirk, K.A.; Gagnon, G.J.; Hwang, J.; Slack, R.S.; Noone, A.M.; Harter, K.W. Fractionated stereotactic radiosurgery for reirradiation of head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1411–1419. [Google Scholar] [CrossRef]
- Salama, J.K.; Vokes, E.E.; Chmura, S.J.; Milano, M.T.; Kao, J.; Stenson, K.M.; Witt, M.E.; Haraf, D.J. Long-term outcome of concurrent chemotherapy and reirradiation for recurrent and second primary head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 382–391. [Google Scholar] [CrossRef]
- Wakatsuki, M.; Ohno, T.; Kato, S.; Ando, K.; Noda, S.E.; Kiyohara, H.; Shibuya, K.; Karasawa, K.; Kamada, T.; Nakano, T. Impact of boost irradiation on pelvic lymph node control in patients with cervical cancer. J. Radiat. Res. 2014, 55, 139–145. [Google Scholar] [CrossRef]
- Yamazaki, H.; Ogita, M.; Himei, K.; Nakamura, S.; Suzuki, G.; Yoshida, K.; Kotsuma, T.; Yoshioka, Y. Reirradiation using robotic image-guided stereotactic radiotherapy of recurrent head and neck cancer. J. Radiat. Res. 2016, 57, 288–293. [Google Scholar] [CrossRef]
- Yamazaki, H.; Ogita, M.; Himei, K.; Nakamura, S.; Kotsuma, T.; Yoshida, K.; Yoshioka, Y. Carotid blowout syndrome in pharyngeal cancer patients treated by hypofractionated stereotactic re-irradiation using CyberKnife: A multi-institutional matched-cohort analysis. Radiotherapy and oncology. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 115, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Yazici, G.; Sanlı, T.Y.; Cengiz, M.; Yuce, D.; Gultekin, M.; Hurmuz, P.; Yıldız, F.; Zorlu, F.; Akyol, F.; Gurkaynak, M.; et al. A simple strategy to decrease fatal carotid blowout syndrome after stereotactic body reirradiaton for recurrent head and neck cancers. Radiotherapy and oncology. J. Eur. Soc. Ther. Radiol. Oncol. 2013, 8, 242. [Google Scholar]
- NCCN Guidelines. 2019. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx#head-and-neck (accessed on 5 November 2019).
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Shiba, S.; Okonogi, N.; Kato, S.; Wakatsuki, M.; Kobayashi, D.; Kiyohara, H.; Ohno, T.; Karasawa, K.; Nakano, T.; Kamada, T. Clinical Impact of Re-irradiation with Carbon-ion Radiotherapy for Lymph Node Recurrence of Gynecological Cancers. Anticancer Res. 2017, 37, 5577–5583. [Google Scholar] [CrossRef] [PubMed]
- Eekers, D.B.P.; Roelofs, E.; Jelen, U.; Kirk, M.; Granzier, M.; Ammazzalorso, F.; Ahn, P.H.; Janssens, G.O.R.J.; Hoebers, F.J.P.; Friedmann, T.; et al. Benefit of particle therapy in re-irradiation of head and neck patients. Results of a multicentric in silico ROCOCO trial. Radiotherapy and oncology. J. Eur. Soc. Ther. Radiol. Oncol. 2016, 121, 387–394. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Strata | Patients (n = 16) | (%) | Lymph Node (n = 55) | (%) |
|---|---|---|---|---|---|
| Age | 60 (45–72) | ||||
| Gender | Female | 3 | 18.7 | 15 | 27.3 |
| Male | 13 | 81.3 | 40 | 72.7 | |
| Primary site | Nasopharynx | 3 | 18.7 | 17 | 30.9 |
| Oropharynx | 3 | 18.7 | 3 | 5.5 | |
| Hypopharynx | 5 | 31.3 | 5 | 9.1 | |
| Buccal mucosal | 1 | 6.3 | 13 | 23.6 | |
| Tongue | 2 | 12.5 | 2 | 3.6 | |
| Laryngeal | 2 | 12.5 | 15 | 27.3 | |
| Surgical history | Yes | 7 | 43.7 | 33 | 60 |
| No | 9 | 56.3 | 22 | 40 | |
| Ulceration | Yes | 3 | 18.7 | 4 | 7.3 |
| No | 13 | 81.3 | 51 | 92.7 | |
| Tumor target volume (median) | (cm3) | 1.2 (0.05–91) | |||
| Prescribed dose of CyberKnife (median) | (Gy) | 20 (18–36) | |||
| Number of fractions (median) | 1 (1–6) | ||||
| EQD2 (median) | [Gy (α/β = 10)] | 50 (40–58) | |||
| maximum dose (median) | (Gy) | 31 (22–41) | |||
| Treatment interval between primary RT and CyberKnife (median) | (months) | 25 (6–69) | |||
| Previous prescribed dose (median) | (Gy) | 68 (50–70) | |||
| Previous no. of fractions (median) | 34 (25–35) | ||||
| Cumulative EQD2 (median) | [Gy (α/β = 10)] | 116 (92–120) |
| Variable | Strata | n | Median Follow-Up Period (Months) | 1-Year LC | Hazard Ratio | p-Value |
|---|---|---|---|---|---|---|
| Age, years | ≤60 | 29 | 41 | 78.5 | 1.5 | 0.51 |
| >60 | 26 | 11 | 85.5 | 0.6 | ||
| Gender | Male | 40 | 15 | 77.0 | 1.7 | 0.43 |
| Female | 15 | 41 | 92.9 | 0.6 | ||
| Primary site | Nasopharynx | 17 | 41 | 81.3 | NA | 0.24 |
| Buccal mucosal | 13 | 17 | 100 | |||
| Laryngeal | 15 | 37 | 85.1 | |||
| others | 10 | 9 | 50.6 | |||
| Previous surgery | Yes | 33 | 21 | 89.1 | 0.2 | 0.059 |
| No | 22 | 15 | 70.3 | 4.0 | ||
| Ulceration | Yes | 4 | 6 | 80.7 | 0.3 | 0.54 |
| No | 51 | 24 | 100 | 2.9 | ||
| Tumor volume | ≤1.0 cm3 | 25 | 32 | 95.8 | 0.2 | 0.0061 |
| >1.0 cm3 | 30 | 10 | 65.9 | 5.8 | ||
| Prescribed dose of CyberKnife (EQD2) | <50 Gy | 7 | 11 | 62.5 | 2.0 | 0.49 |
| ≥50 Gy | 48 | 23 | 83.8 | 0.5 | ||
| Treatment interval | ≤25 months | 28 | 32 | 79.6 | 1.7 | 0.41 |
| >25 months | 27 | 15 | 83.5 | 0.6 |
| Adverse Events | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 |
|---|---|---|---|---|---|
| pharyngitis | 0 | 2 | 0 | 0 | 0 |
| dermatitis | 1 | 1 | 0 | 0 | 0 |
| anorexia | 1 | 0 | 0 | 0 | 0 |
| injury to carotid artery | 0 | 0 | 0 | 0 | 1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, D.; Sato, H.; Saitoh, J.-i.; Oike, T.; Nakajima, A.; Noda, S.-e.; Kato, S.; Iwanaga, M.; Shimizu, T.; Nakano, T. Efficacy and Feasibility of Salvage Re-Irradiation with CyberKnife for In-Field Neck Lymph Node Recurrence: A Retrospective Study. J. Clin. Med. 2019, 8, 1911. https://doi.org/10.3390/jcm8111911
Kobayashi D, Sato H, Saitoh J-i, Oike T, Nakajima A, Noda S-e, Kato S, Iwanaga M, Shimizu T, Nakano T. Efficacy and Feasibility of Salvage Re-Irradiation with CyberKnife for In-Field Neck Lymph Node Recurrence: A Retrospective Study. Journal of Clinical Medicine. 2019; 8(11):1911. https://doi.org/10.3390/jcm8111911
Chicago/Turabian StyleKobayashi, Daijiro, Hiro Sato, Jun-ichi Saitoh, Takahiro Oike, Atsushi Nakajima, Shin-ei Noda, Shingo Kato, Mototaro Iwanaga, Tsuneo Shimizu, and Takashi Nakano. 2019. "Efficacy and Feasibility of Salvage Re-Irradiation with CyberKnife for In-Field Neck Lymph Node Recurrence: A Retrospective Study" Journal of Clinical Medicine 8, no. 11: 1911. https://doi.org/10.3390/jcm8111911