Effects of Widespread Inotrope Use in Acute Heart Failure Patients

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Endpoints and Definitions
2.2. Statistical Analyses
3. Results
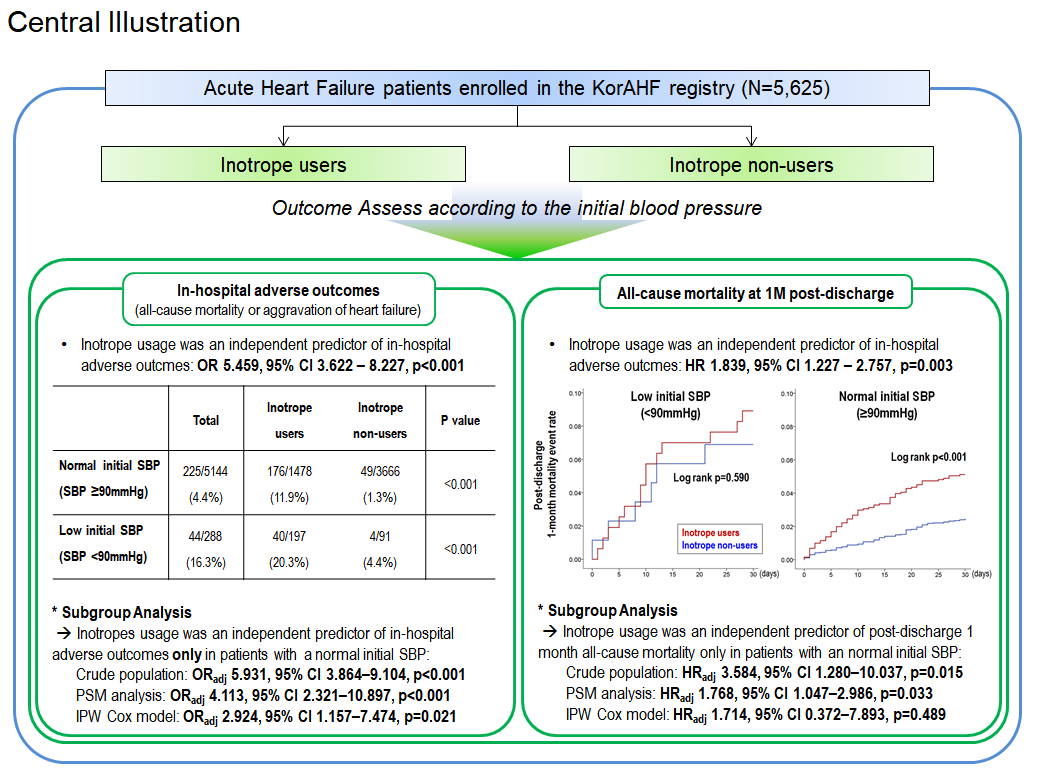
3.1. In-Hospital Clinical Events
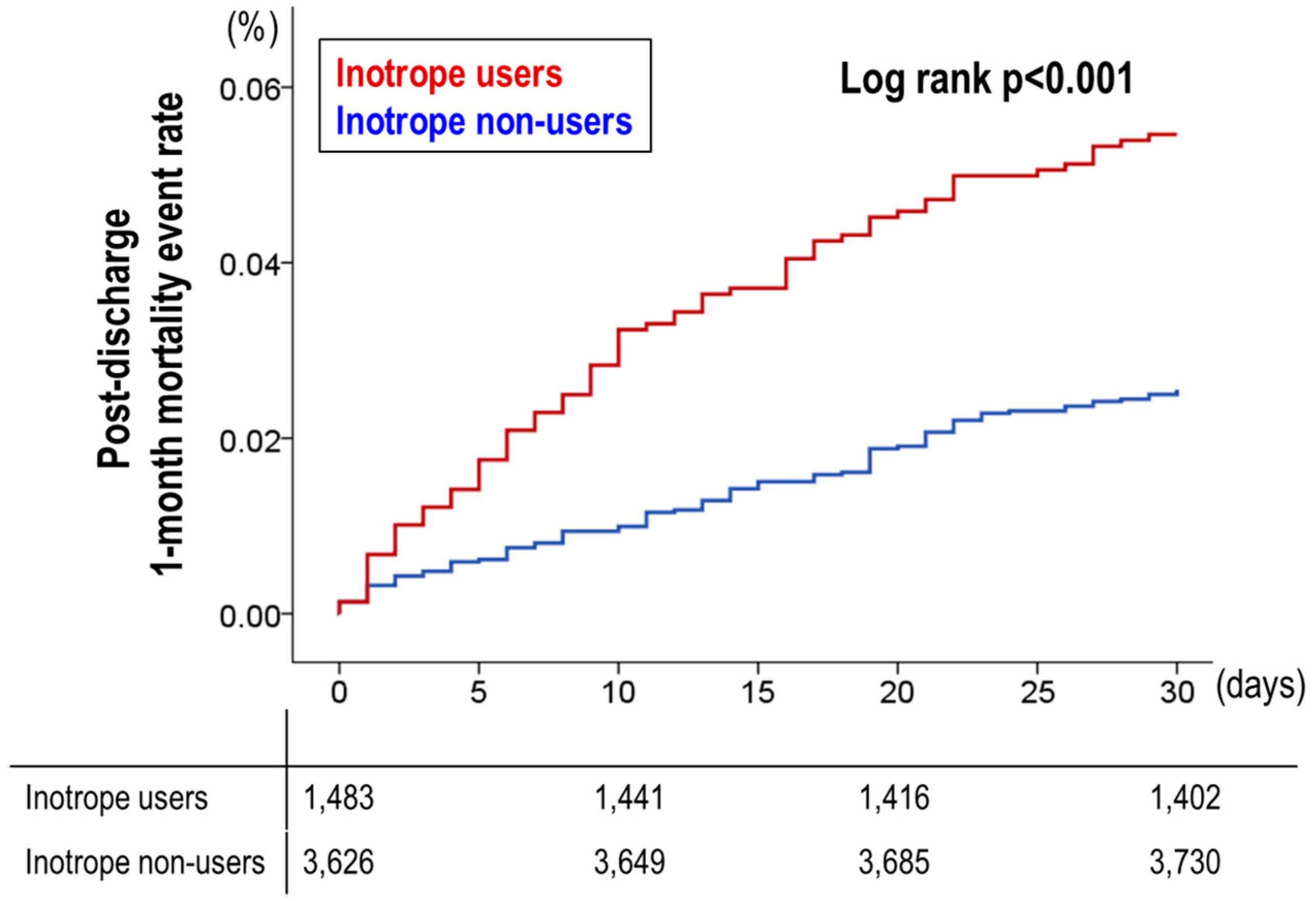
3.2. Post-Discharge 1-Month Mortality
3.3. Propensity Score Matched Population
4. Discussion
4.1. Inotrope Use in Acute HF
4.2. Hazardous Effect of Inotropes in Acute HF Patients
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC) developed with the special contribution of the heart failure association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the american college of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 2013, 128, e240–e327. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Alburikan, K.; Metra, M.; Rodgers, J.E. Acute decompensated heart failure update. Curr. Cardiol. Rev. 2015, 11, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Zsilinszka, R.; Mentz, R.J.; DeVore, A.D.; Eapen, Z.J.; Pang, P.S.; Hernandez, A.F. Acute heart failure: Alternatives to hospitalization. JACC Heart Fail. 2017, 5, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Thackray, S.; Easthaugh, J.; Freemantle, N.; Cleland, J.G. The effectiveness and relative effectiveness of intravenous inotropic drugs acting through the adrenergic pathway in patients with heart failure-a meta-regression analysis. Eur. J. Heart Fail. 2002, 4, 515–529. [Google Scholar] [CrossRef] [Green Version]
- Abraham, W.T.; Adams, K.F.; Fonarow, G.C.; Costanzo, M.R.; Berkowitz, R.L.; LeJemtel, T.H.; Cheng, M.L.; Wynne, J.; ADHERE Scientific Advisory Committee and Investigators; ADHERE Study Group. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: An analysis from the acute decompensated heart failure national registry (adhere). J. Am. Coll. Cardiol. 2005, 46, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Parissis, J.; Porcher, R.; Gayat, E.; Nikolaou, M.; Boas, F.V.; Delgado, J.F.; Follath, F. Short-term survival by treatment among patients hospitalized with acute heart failure: The global alarm-hf registry using propensity scoring methods. Intensive Care Med. 2011, 37, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; et al. Clinical characteristics and outcome of acute heart failure in Korea: Results from the Korean acute heart failure registry (korahf). Korean Circ. J. 2017, 47, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.L.; Schwartzman, D.S.; Salama, G. Mode of death prevention by serelaxin. J. Am. Coll. Cardiol. 2015, 66, 98–99. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Voors, A.A.; Ponikowski, P.; Pang, P.S.; Greenberg, B.H.; Filippatos, G.; Felker, G.M.; Davison, B.A.; Cotter, G.; Gimpelewicz, C.; et al. Serelaxin in addition to standard therapy in acute heart failure: Rationale and design of the relax-ahf-2 study. Eur. J. Heart Fail. 2017, 19, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Cerlinskaite, K.; Javanainen, T.; Cinotti, R.; Mebazaa, A. Global Research on Acute Conditions Team -modi(GREAT) Network. Acute heart failure management. Korean Circ. J. 2018, 48, 463–480. [Google Scholar] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the american college of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Lee, K.L.; Bull, D.A.; Redfield, M.M.; Stevenson, L.W.; Goldsmith, S.R.; LeWinter, M.M.; Deswal, A.; Rouleau, J.L.; Ofili, E.O.; et al. Diuretic strategies in patients with acute decompensated heart failure. N. Engl. J. Med. 2011, 364, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Ellison, D.H.; Felker, G.M. Diuretic treatment in heart failure. N. Engl. J. Med. 2018, 378, 684–685. [Google Scholar] [CrossRef] [PubMed]
- Cuffe, M.S.; Califf, R.M.; Adams, K.F., Jr.; Benza, R.; Bourge, R.; Colucci, W.S.; Massie, B.M.; O’Connor, C.M.; Pina, I.; Quigg, R.; et al. Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure, I. Short-term intravenous milrinone for acute exacerbation of chronic heart failure: A randomized controlled trial. JAMA 2002, 287, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.C.; Zhu, D.M.; Shan, Y.X. Dobutamine therapy is associated with worse clinical outcomes compared with nesiritide therapy for acute decompensated heart failure: A systematic review and meta-analysis. Am. J. Cardiovasc. Drugs. 2015, 15, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Mortara, A.; Oliva, F.; Metra, M.; Carbonieri, E.; Di Lenarda, A.; Gorini, M.; Midi, P.; Senni, M.; Urso, R.; Lucci, D.; et al. Treatment with inotropes and related prognosis in acute heart failure: Contemporary data from the Italian network on heart failure (IN-HF) outcome registry. J. Heart Lung Transplant. 2014, 33, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Nizamic, T.; Murad, M.H.; Allen, L.A.; McIlvennan, C.K.; Wordingham, S.E.; Matlock, D.D.; Dunlay, S.M. Ambulatory inotrope infusions in advanced heart failure: A systematic review and meta-analysis. JACC Heart Fail. 2018, 6, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Motiejunaite, J.; Gayat, E.; Crespo-Leiro, M.G.; Lund, L.H.; Maggioni, A.P.; Chioncel, O.; Akiyama, E.; Harjola, V.P.; Seferovic, P.; et al. Investigators ESCHFL-TR. Long-term safety of intravenous cardiovascular agents in acute heart failure: Results from the european society of cardiology heart failure long-term registry. Eur. J. Heart Fail. 2018, 20, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.; Rhee, J.; Chaudhari, V.; Rosenzweig, A. The role of exercise in cardiac aging: From physiology to molecular mechanisms. Circ. Res. 2016, 118, 279–295. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Holmes, J.; Krum, H.; Altman, D.G.; Manzano, L.; Cleland, J.G.; Lip, G.Y.; Coats, A.J.; Andersson, B.; Kirchhof, P.; et al. Efficacy of beta blockers in patients with heart failure plus atrial fibrillation: An individual-patient data meta-analysis. Lancet 2014, 384, 2235–2243. [Google Scholar] [CrossRef]
- Prijic, S.; Buchhorn, R. Mechanisms of beta-blockers action in patients with heart failure. Rev. Recent Clin. Trials 2014, 9, 58–60. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Population (n = 5471) | Inotrope Users (n = 1703) | Inotrope Non-Users (n = 3768) | p Value | |
|---|---|---|---|---|
| Sex (male) | 2919 (53.4%) | 1024 (60.1%) | 1895 (50.3%) | <0.001 |
| Age (years old) | 68.6 ± 14.4 | 66.8 ± 14.8 | 69.4 ± 14.2 | <0.001 |
| BMI (kg/m2) | 23.3 ± 3.9 | 22.9 ± 3.8 | 23.5 ± 3.9 | <0.001 |
| LVEF (%) | 37.3 ± 15.5 | 33.0 ± 14.6 | 39.2 ± 15.5 | <0.001 |
| Risk factors | ||||
| HTN, n (%) | 2211 (40.4%) | 791 (46.4%) | 1420 (37.7%) | <0.001 |
| DM, n (%) | 3518 (64.3%) | 1053 (61.8%) | 2465 (65.4%) | 0.010 |
| Smoking, % * | 17.9/21.1/61.1 | 20.3/21.8/57.9 | 16.8/20.7/62.5 | 0.002 |
| Previous MI, n (%) | 909 (16.6%) | 308 (18.1%) | 601 (16.0%) | 0.051 |
| Previous PCI, n (%) | 931 (17.0%) | 318 (18.7%) | 613 (16.3%) | 0.030 |
| Previous CABG, n (%) | 287 (5.2%) | 113 (6.6%) | 174 (4.6%) | 0.002 |
| COPD, n (%) | 602 (11.0%) | 199 (11.7%) | 403 (10.7%) | 0.280 |
| CRF, n (%) | 791 (14.5%) | 277 (16.3%) | 514 (13.6%) | 0.011 |
| Previous CVA, n (%) | 833 (15.2%) | 237 (13.9%) | 596 (15.8%) | 0.069 |
| Valve disease, n (%) | 769 (14.1%) | 295 (17.3%) | 474 (12.6%) | <0.001 |
| Atrial fibrillation, n (%) | 1850 (33.8%) | 465 (27.3%) | 1385 (36.8%) | <0.001 |
| Heart failure Etiology | ||||
| Ischemic heart disease | 2096 (38.3%) | 768 (45.1%) | 1328 (35.2%) | <0.001 |
| Valvular heart disease | 763 (13.9%) | 289 (17.0%) | 474 (12.6%) | <0.001 |
| Congenital heart disease | 50 (0.9%) | 17 (1.0%) | 33 (0.9%) | 0.659 |
| Cardiomyopathy | 1163 (21.3%) | 374 (22.0%) | 789 (20.9%) | 0.392 |
| Hypertension | 216 (3.9%) | 24 (1.4%) | 192 (5.1%) | <0.001 |
| Myocarditis | 75 (1.4%) | 44 (2.6%) | 31 (0.8%) | <0.001 |
| Infiltrative disease † | 69 (1.3%) | 13 (0.8%) | 56 (1.5%) | 0.027 |
| Tachycardia related disease # | 586 (10.7%) | 69 (4.1%) | 517 (13.7%) | <0.001 |
| Thyroid related disease $ | 29 (0.5%) | 4 (0.2%) | 25 (0.7%) | 0.043 |
| Toxic related disease‡ | 58 (1.1%) | 19 (1.1%) | 39 (1.0%) | 0.787 |
| NYHA at admission, (%) ** | 15.2/36.6/48.2 | 11.1/33.0/55.9 | 17.1/38.2/44.7 | <0.001 |
| Initial SBP (mmHg) | 131 ± 30 | 121 ± 30 | 136 ± 30 | <0.001 |
| Initial DBP (mmHg) | 79 ± 19 | 74 ± 18 | 81 ± 19 | <0.001 |
| Initial HR | 93 ± 26 | 93 ± 25 | 93 ± 26 | 0.432 |
| Laboratory analysis | ||||
| WBC (109/L) | 8710 ± 3960 | 9480 ± 4620 | 8360 ± 3560 | <0.001 |
| Hb (g/dL) | 12.4 ± 3.0 | 12.4 ± 2.3 | 12.4 ± 2.3 | 0.465 |
| Platelet (109/L) | 211 ± 89 | 204 ± 89 | 215 ± 88 | <0.001 |
| Total cholesterol (mg/dL) | 152 ± 43 | 148 ± 43 | 154 ± 43 | <0.001 |
| Triglyceride (mg/dL) | 100 ± 59 | 98 ± 64 | 101 ± 57 | 0.193 |
| HDL (mg/dL) | 41 ± 14 | 39 ± 14 | 42 ± 14 | <0.001 |
| LDL (mg/dL) | 107 ± 55 | 104 ± 56 | 108 ± 55 | 0.059 |
| Na (mEq/L) | 138 ± 5 | 137 ± 5 | 138 ± 4 | <0.001 |
| Uric acid (mg/dL) | 7.0 ± 2.9 | 7.4 ± 3.0 | 6.9 ± 2.8 | <0.001 |
| BUN (mg/dL) | 26 ± 16 | 29 ± 19 | 25 ± 15 | <0.001 |
| Creatinine (mg/dL) | 1.49 ± 1.49 | 1.62 ± 1.60 | 1.43 ± 1.43 | <0.001 |
| Glucose (mg/dL) | 156 ± 77 | 166 ± 86 | 151 ± 73 | <0.001 |
| CRP (mg/L) | 2.36 ± 4.25 | 3.15 ± 5.33 | 2.00 ± 3.60 | <0.001 |
| BNP (pg/mL) | 1341 ± 1304 | 1571 ± 1454 | 1243 ± 1223 | <0.001 |
| NTproBNP (pg/mL) | 9327 ± 10846 | 11762 ± 12089 | 8232 ± 10051 | <0.001 |
| Total | Inotrope Users | Inotrope Non-Users | p Value | |
|---|---|---|---|---|
| Total population | ||||
| Primary endpoint | 280/5471 (5.1%) | 227/1703 (13.3%) | 53/3768 (1.4%) | <0.001 |
| Mortality | 258/5471 (4.7%) | 220/1703 (12.9%) | 38/3768 (1.0%) | <0.001 |
| Cardiac death | 197/5471 (3.6%) | 173/1703 (10.2%) | 24/3768 (0.6%) | <0.001 |
| Normal initial SBP (SBP ≥ 90 mmHg) | ||||
| Primary endpoint | 225/5144 (4.4%) | 176/1478 (11.9%) | 49/3666 (1.3%) | <0.001 |
| Mortality | 203/5144 (3.9%) | 169/1478 (11.4%) | 34/3666 (0.9%) | <0.001 |
| Cardiac death | 153/5144 (3.0%) | 130/1478 (8.8%) | 23/3666 (0.6%) | <0.001 |
| Low initial SBP (SBP < 90 mmHg) | ||||
| Primary endpoint | 44/288 (16.3%) | 40/197 (20.3%) | 4/91 (4.4%) | <0.001 |
| Mortality | 44/288 (15.3%) | 40/197 (20.3%) | 4/91 (4.4%) | <0.001 |
| Cardiac death | 34/288 (11.8%) | 33/197 (16.8%) | 1/91 (1.1%) | <0.001 |
| HFrEF (EF ≤ 40%) | ||||
| Primary endpoint | 179/3198 (6.0%) | 150/1167 (12.9%) | 29/2031 (1.4%) | <0.001 |
| Mortality | 161/3198 (5.0%) | 143/1167 (12.3%) | 18/2031 (0.9%) | <0.001 |
| Cardiac death | 132/3198 (4.1%) | 119/1167 (10.2%) | 13/2031 (0.6%) | <0.001 |
| HFmrEF (40% < EF < 50%) | ||||
| Primary endpoint | 24/750 (3.2%) | 18/181 (9.9%) | 6/569 (1.1%) | <0.001 |
| Mortality | 23/750 (3.1%) | 18/181 (9.9%) | 5/569 (0.9%) | <0.001 |
| Cardiac death | 16/750 (2.1%) | 12/181 (6.6%) | 4/569 (0.7%) | <0.001 |
| HFpEF (EF ≥ 50%) | ||||
| Primary endpoint | 41/1284 (3.2%) | 29/266 (10.9%) | 12/1018 (1.2%) | <0.001 |
| Mortality | 39/1284 (3.0%) | 29/266 (10.9%) | 10/1018 (1.0%) | <0.001 |
| Cardiac death | 22/1284 (7.1%) | 19/266 (7.1%) | 3/1018 (0.3%) | <0.001 |
| Odds Ratio | 95% CI | p | |
|---|---|---|---|
| Old age (>70 years old) | 2.877 | 1.908–4.340 | <0.001 |
| Low BMI (<25 kg/m2) | 1.587 | 1.009–2.498 | 0.046 |
| Chronic renal failure | 2.254 | 1.331–3.816 | 0.002 |
| LVEF (≤40%) | 1.715 | 1.111–2.647 | 0.015 |
| Uric Acid > 7 mg/dL | 1.689 | 1.182–2.413 | 0.004 |
| CRP > 0.5 mg/dL | 2.636 | 1.689–4.112 | <0.001 |
| Renal replacement therapy during admission | 10.657 | 6.763–16.794 | <0.001 |
| Inotrope usage | 5.459 | 3.622–8.227 | <0.001 |
| Total | Inotrope Users | Inotrope Non-Users | p Value | |
|---|---|---|---|---|
| 1-month mortality | 176/5213 (3.4%) | 81/1483 (5.5%) | 95/3730 (2.5%) | <0.001 |
| Subgroup—by initial SBP | ||||
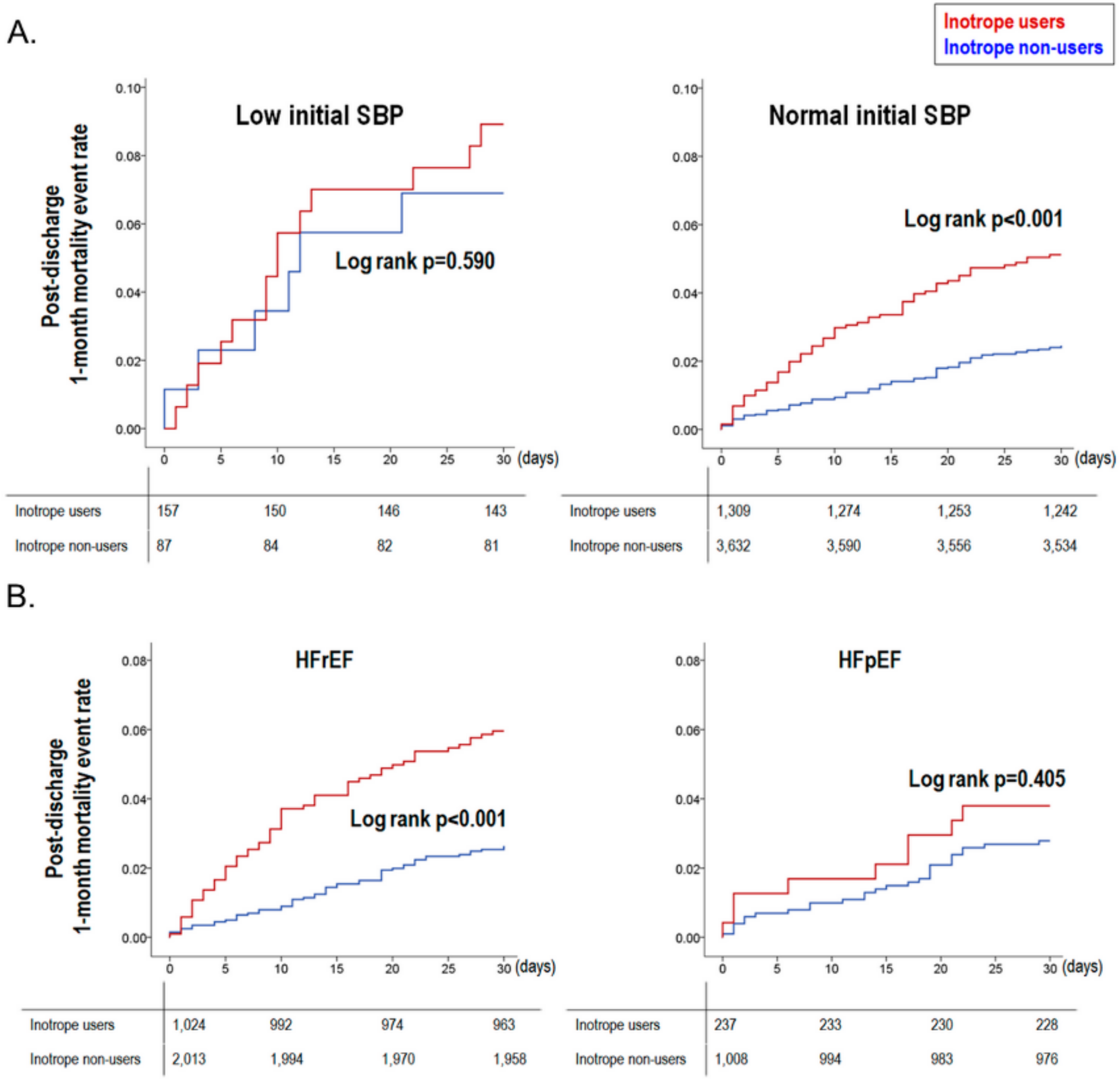
| Low Initial SBP | 20/244 (8.2%) | 14/157 (8.9%) | 6/87 (6.9%) | 0.582 |
| Normal Initial SBP | 156/4941 (3.2%) | 67/1309 (5.1%) | 89/3632 (2.5%) | <0.001 |
| Subgroup—by LV systolic function | ||||
| HFrEF | 114/3037 (3.8%) | 61/1024 (6.0%) | 53/2013 (2.6%) | <0.001 |
| HRmrEF | 17/727 (2.3%) | 5/163 (3.1%) | 12/564 (2.1%) | 0.484 |
| HFpEF | 37/1245 (3.0%) | 9/237 (3.8%) | 28/1008 (2.8%) | 0.406 |
| Hazard Ratio | 95% CI | p | |
|---|---|---|---|
| Old age (>70 years old) | 2.809 | 1.739–4.539 | <0.001 |
| Hyponatremia | 1.572 | 1.048–2.358 | 0.029 |
| Uric Acid > 7 mg/dL | 1.542 | 1.052–2.260 | 0.026 |
| High CRP | 1.817 | 1.153–2.863 | 0.010 |
| Renal replacement therapy during admission | 2.653 | 1.487–4.734 | 0.001 |
| Inotrope usage | 1.891 | 1.264–2.829 | 0.002 |
| Inotrope Users (n = 989) | Inotrope Non-Users (n = 989) | Standardized Mean Difference | p Value | |
|---|---|---|---|---|
| Sex (male) | 566 (57.2%) | 583 (58.9%) | 3.2% | 0.439 |
| Age (years old) | 65.6 ± 15.2 | 67.2 ± 14.5 | 10.7% | 0.014 |
| BMI (kg/m2) | 23.1 ± 3.7 | 23.1 ± 3.7 | 0.5% | 0.732 |
| LVEF (%) | 34.3 ± 15.0 | 32.8 ± 12.9 | 10.5% | 0.020 |
| Risk factors | ||||
| HTN, n (%) | 560 (56.6%) | 523 (52.9%) | 7.7% | 0.095 |
| DM, n (%) | 371 (37.5%) | 369 (37.3%) | 0.4% | 0.926 |
| Smoking, % * | 18.8/21.8/59.4 | 20.4/21.1/58.4 | 2.1% | 0.656 |
| Previous MI, n (%) | 166 (16.8%) | 161 (16.3%) | 1.4% | 0.762 |
| Previous PCI, n (%) | 168 (17.0%) | 180 (18.2%) | 3.3% | 0.479 |
| Previous CABG, n (%) | 68 (6.9%) | 64 (6.5%) | 1.7% | 0.719 |
| COPD, n (%) | 118 (11.9%) | 90 (9.1%) | 9.1% | 0.048 |
| CRF, n (%) | 152 (15.4%) | 118 (11.9%) | 9.9% | 0.031 |
| Initial SBP | 126 ± 29 | 133 ± 30 | 23.7% | <0.001 |
| Initial DBP | 76 ± 18 | 81 ± 20 | 26.3% | <0.001 |
| Initial HR | 93 ± 24 | 94 ± 25 | 4.1% | 0.290 |
| Valve disease, n (%) | 160 (16.2%) | 150 (15.2%) | 2.9% | 0.536 |
| Previous CVA, n (%) | 135 (13.7%) | 145 (14.7%) | 3.0% | 0.513 |
| Atrial fibrillation, n (%) | 269 (27.2%) | 251 (25.4%) | 4.2% | 0.358 |
| Laboratory analysis | ||||
| WBC (109/L) | 9010±4040 | 8680 ± 3790 | 8.4% | 0.059 |
| Hb (g/dL) | 12.4 ± 2.3 | 12.6 ± 2.3 | 8.7% | 0.036 |
| Platelet (109/L) | 209 ± 93 | 210 ± 80 | 1.2% | 0.976 |
| Na (m Eq/L) | 137± 5 | 137 ± 5 | 4.0% | 0.368 |
| Uric acid (mg/dL) | 7.3 ± 2.8 | 7.1 ± 3.5 | 6.3% | 0.076 |
| Creatinine (mg/dL) | 1.54 ± 1.48 | 1.35 ± 1.16 | 14.3% | 0.001 |
| Glucose (mg/dL) | 163 ± 80 | 156 ± 75 | 7.7% | 0.029 |
| CRP (mg/L) | 2.64 ± 4.59 | 2.26 ± 3.86 | 9.0% | 0.044 |
| Clinical events | ||||
| In-hospital adverse outcomes | 7.9% (78/989) | 1.9% (19/989) | NA | <0.001 |
| 1-month mortality | 4.2% (39/921) | 2.6% (25/974) | NA | 0.045 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.; Cho, H.-J.; Lee, H.-Y.; Lee, S.; Park, S.K.; Lee, S.E.; Kim, J.-J.; Jeon, E.-S.; Chae, S.C.; Baek, S.H.; et al. Effects of Widespread Inotrope Use in Acute Heart Failure Patients. J. Clin. Med. 2018, 7, 368. https://doi.org/10.3390/jcm7100368
Kang J, Cho H-J, Lee H-Y, Lee S, Park SK, Lee SE, Kim J-J, Jeon E-S, Chae SC, Baek SH, et al. Effects of Widespread Inotrope Use in Acute Heart Failure Patients. Journal of Clinical Medicine. 2018; 7(10):368. https://doi.org/10.3390/jcm7100368
Chicago/Turabian StyleKang, Jeehoon, Hyun-Jai Cho, Hae-Young Lee, Sangjun Lee, Sue K. Park, Sang Eun Lee, Jae-Joong Kim, Eun-Seok Jeon, Shung Chull Chae, Sang Hong Baek, and et al. 2018. "Effects of Widespread Inotrope Use in Acute Heart Failure Patients" Journal of Clinical Medicine 7, no. 10: 368. https://doi.org/10.3390/jcm7100368