Impaired Executive Functioning of Sexual Assault Survivors with Acute Stress Disorder

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Assessments
2.2.1. PTSD Symptom Scale-Self Report (PSS-SR)
2.2.2. Korean Beck Depression Inventory-II (BDI-II)
2.2.3. Korean Beck Anxiety Inventory (BAI)
2.2.4. Korean State Trait Anger Expression Inventory (STAXI)
2.2.5. Korean Wechsler Adult Intelligence Scale–Fourth Edition (K-WAIS–IV)
2.2.6. Cambridge Neuropsychological Test Automated Battery (CANTAB)
- Intra-Extra Dimensional Set Shift (IED): This test of rule acquisition and reversal, which is a computerized version of the Wisconsin Card Sorting Test, was used to assess cognitive flexibility/set-shift. Participants were required to pay attention to a reinforced stimulus (shapes: intra-dimensional shift) and subsequently shift to a previously irrelevant stimulus (lines: extra-dimensional shift). The test assessed participants’ ability to learn in a total of nine stages.
- Stockings of Cambridge (SOC): A variant of the classic Tower of London task, SOC was used to assess spatial planning. Participants were asked to mimic a display pattern with as few moves as possible. In the trial with the highest difficulty, participants have to move five times to solve the problem.
- Spatial Span (SSP): A visuospatial version of the digit span test, SSP was used to assess attention/working memory. Participants were instructed to mimic sequential flashing boxes in the order presented.
- Stop Signal Task (SST): This stop-signal response-inhibition test was used to assess the ability to inhibit a prepotent response. Participants were instructed to hit a press-pad as quickly and accurately as possible when an image of an arrow was shown, but to avoid hitting the pad when a beep was heard with the arrow.
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Group Differences in the ASD and HC Groups
3.1.1. Demographic and Clinical Characteristics
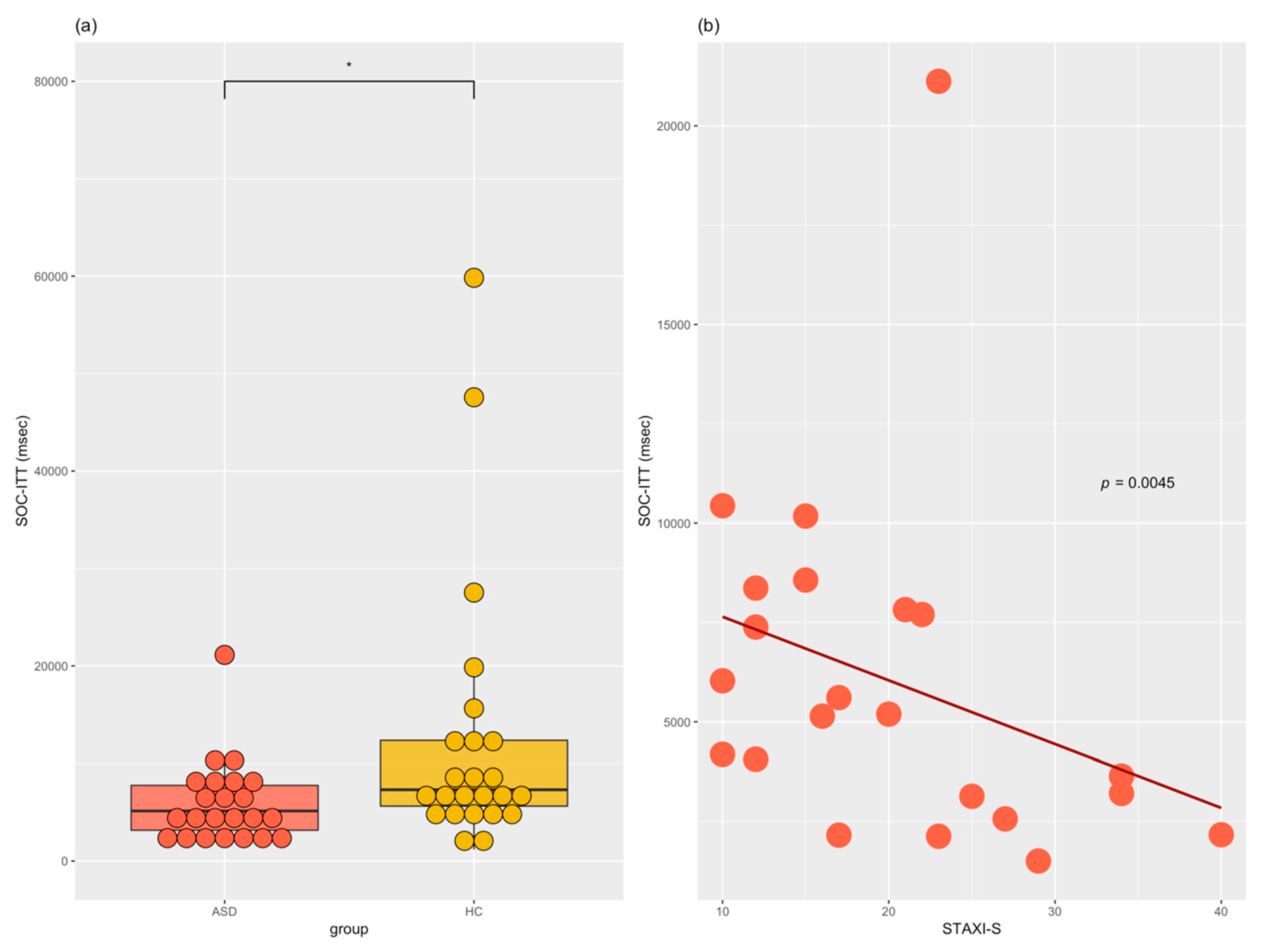
3.1.2. Executive Functioning
3.2. Relationship among Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic stress disorder in the national comorbidity survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- National Center for Post Traumatic Stress Disorder. Available online: https://www.ptsd.va.gov/professional/PTSD-overview/epidemiological-facts-ptsd.asp (accessed on 3 September 2018).
- Creamer, M.; Burgess, P.; McFarlane, A.C. Post-traumatic stress disorder: Findings from the australian national survey of mental health and well-being. Psychol. Med. 2001, 31, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Rothbaum, B.O.; Foa, E.B.; Riggs, D.S.; Murdock, T.; Walsh, W. A prospective examination of post-traumatic stress disorder in rape victims. J. Trauma. Stress 1992, 5, 455–475. [Google Scholar] [CrossRef]
- Burgess, A.W.; Holmstrom, L.L. Rape trauma syndrome. Am. J. Psychiatry 1974, 131, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Tannura, T.A. Rape trauma syndrome. Am. J. Sex Educ. 2014, 9, 247–256. [Google Scholar] [CrossRef]
- Brown, A.L.; Testa, M.; Messman-Moore, T.L. Psychological consequences of sexual victimization resulting from force, incapacitation, or verbal coercion. Violence Against Women 2009, 15, 898–919. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.P.; Murad, M.H.; Paras, M.L.; Colbenson, K.M.; Sattler, A.L.; Goranson, E.N.; Elamin, M.B.; Seime, R.J.; Shinozaki, G.; Prokop, L.J. Sexual abuse and lifetime diagnosis of psychiatric disorders: Systematic review and meta-analysis. Mayo Clin. Proc. 2010, 85, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A. Acute stress disorder as a predictor of posttraumatic stress disorder: A systematic review. J. Clin. Psychiatry 2011, 72, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.P.; VanElzakker, M.B.; Shin, L.M. Emotion and cognition interactions in PTSD: A review of neurocognitive and neuroimaging studies. Front. Integr. Neurosci. 2012, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.C.; Berntsen, D.; Bohni, M.K. A memory-based model of posttraumatic stress disorder: Evaluating basic assumptions underlying the PTSD diagnosis. Psychol. Rev. 2008, 115, 985–1011. [Google Scholar] [CrossRef] [PubMed]
- Hull, A.M. Neuroimaging findings in post-traumatic stress disorder: Systematic review. Br. J. Psychiatry 2002, 181, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Elzinga, B.M.; Bremner, J.D. Are the neural substrates of memory the final common pathway in posttraumatic stress disorder (PTSD)? J. Affect. Disord. 2002, 70, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Hayes, J.P.; LaBar, K.S.; McCarthy, G.; Selgrade, E.; Nasser, J.; Dolcos, F.; Morey, R.A. Reduced hippocampal and amygdala activity predicts memory distortions for trauma reminders in combat-related PTSD. J. Psychiatr. Res. 2011, 45, 660–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polak, A.R.; Witteveen, A.B.; Reitsma, J.B.; Olff, M. The role of executive function in posttraumatic stress disorder: A systematic review. J. Affect. Disord. 2012, 141, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Aupperle, R.L.; Melrose, A.J.; Stein, M.B.; Paulus, M.P. Executive function and PTSD: Disengaging from trauma. Neuropharmacology 2012, 62, 686–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, M.A.; Langlais, P.J.; Delis, D.; Cohen, R.A. Attentional dysfunction associated with posttraumatic stress disorder among rape survivors. Clin. Neuropsychol. 2000, 14, 7–12. [Google Scholar] [CrossRef]
- Koso, M.; Hansen, S. Executive function and memory in posttraumatic stress disorder: A study of bosnian war veterans. Eur. Psychiatry 2006, 21, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Vasterling, J.J.; Duke, L.M.; Brailey, K.; Constans, J.I.; Allain, A.N., Jr.; Sutker, P.B. Attention, learning, and memory performances and intellectual resources in vietnam veterans: Ptsd and no disorder comparisons. Neuropsychology 2002, 16, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.L.; Shin, L.M.; Phelps, E.A. Neurocircuitry models of posttraumatic stress disorder and extinction: Human neuroimaging research—Past, present, and future. Biol. Psychiatry 2006, 60, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Felmingham, K.L.; Kemp, A.H.; Barton, M.; Peduto, A.S.; Rennie, C.; Gordon, E.; Williams, L.M. Neural networks of information processing in posttraumatic stress disorder: A functional magnetic resonance imaging study. Biol. Psychiatry 2005, 58, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Brandes, D.; Ben-Schachar, G.; Gilboa, A.; Bonne, O.; Freedman, S.; Shalev, A.Y. Ptsd symptoms and cognitive performance in recent trauma survivors. Psychiatry Res. 2002, 110, 231–238. [Google Scholar] [CrossRef]
- LaGarde, G.; Doyon, J.; Brunet, A. Memory and executive dysfunctions associated with acute posttraumatic stress disorder. Psychiatry Res. 2010, 177, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Quidé, Y.; Cléry, H.; Andersson, F.; Descriaud, C.; Saint-Martin, P.; Barantin, L.; Gissot, V.; Carrey, L.B.M.; Osterreicher, S.; Dufour-Rainfray, D. Neurocognitive, emotional and neuroendocrine correlates of exposure to sexual assault in women. J. Psychiatry Neurosci. 2018, 43, 170116–170124. [Google Scholar] [CrossRef] [PubMed]
- Arffa, S. The relationship of intelligence to executive function and non-executive function measures in a sample of average, above average, and gifted youth. Arch. Clin. Neuropsychol. 2007, 22, 969–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajilchi, B.; Nejati, V. Executive functions in students with depression, anxiety, and stress symptoms. Basic Clin. Neurosci. 2017, 8, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Fossati, P.; Ergis, A.; Allilaire, J. Executive functioning in unipolar depression: A review. Encephale 2002, 28, 97–107. [Google Scholar] [PubMed]
- Hergueta, T.; Baker, R.; Dunbar, G.C. The mini-international neuropsychiatric interview (MINI): The development and validation of a structured diagnostic psychiatric interview for dsm-ivand icd-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Yoo, S.-W.; Kim, Y.-S.; Noh, J.-S.; Oh, K.-S.; Kim, C.-H.; NamKoong, K.; Chae, J.-H.; Lee, G.-C.; Jeon, S.-I.; Min, K.-J. Validity of Korean version of the mini-international neuropsychiatric interview. Anxiety Mood 2006, 2, 50–55. [Google Scholar]
- Foa, E.B.; Riggs, D.S.; Dancu, C.V.; Rothbaum, B.O. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J. Trauma. Stress 1993, 6, 459–473. [Google Scholar] [CrossRef]
- Foa, E.B.; Yadin, E. Assessment and diagnosis of posttraumatic stress disorder. Psychiatr. Times 2011, 28, 63–65. [Google Scholar]
- Kim, R.S. Structure of Posttraumatic Stress Disorder Symptom: Reclassification of Symptom; Catholic University: Seoul, Korea, 2007. [Google Scholar]
- Scher, C.D.; McCreary, D.R.; Asmundson, G.J.; Resick, P.A. The structure of post-traumatic stress disorder symptoms in three female trauma samples: A comparison of interview and self-report measures. J. Anxiety Disord. 2008, 22, 1137–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Lee, E.; Hwang, S.; Hong, S. Korean-Beck Depression Inventory-II; Korea Psychology Corporation: Daegu, Korea, 2014. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Kim, J.; Lee, E.; Hwang, S.; Hong, S. Korean-Beck Anxiety Inventory; Korea Psychology Corporation: Daegu, Korea, 2014. [Google Scholar]
- Steer, R.A.; Beck, A.T. Beck Anxiety Inventory. In Evaluating Stress: A Book of Resources; Zalaquett, C.P., Wood, R.J., Eds.; Scarecrow Education: Lanham, MD, USA, 1997; pp. 23–40. [Google Scholar]
- Chon, K.-K.; Hahn, D.-W.; Lee, C.-H.; Spielberger, C. Korean adaptation of the state-trait anger expression inventory: Anger and blood pressure. Korean J. Health Psychol. 1997, 2, 60–78. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait Anger Expression Inventory (STAXI); Psychological Assessment Resources: Odessa, FL, USA, 1988. [Google Scholar]
- Hwang, S.; Kim, J.; Park, G.; Chey, J.; Hong, S. K-WAIS-IV Administration and Scoring Manual; Korea Psychology Corporation: Daegu, Korea, 2012. [Google Scholar]
- Wechsler, D. Wechsler Adult Intelligence Scale (WAIS–IV), 4th ed.; The Psychological Corporation: San Antonio, TX, USA, 2008. [Google Scholar]
- Yeom, T.; Park, Y.; Oh, K.; Kim, J.; Lee, Y. Korean Wechsler Adult Intelligence Scale (K-WAIS) Manual; Handbook Guidence: Seoul, Korea, 1992. [Google Scholar]
- Robbins, T.W.; James, M.; Owen, A.M.; Sahakian, B.J.; Lawrence, A.D.; McInnes, L.; Rabbitt, P.M. A study of performance on tests from the cantab battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers: Implications for theories of executive functioning and cognitive aging. J. Int. Neuropsychol. Soc. 1998, 4, 474–490. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar]
- Arnsten, A.F. Stress signalling pathways that impair prefrontal cortex structure and function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechtel, P.; Pizzagalli, D.A. Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology 2011, 214, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, A.F.; Goldman-Rakic, P.S. Noise stress impairs prefrontal cortical cognitive function in monkeys: Evidence for a hyperdopaminergic mechanism. Arch. Gen. Psychiatry 1998, 55, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.L.; Arnsten, A.F.; Jentsch, J.D.; Roth, R.H. Dopamine and spatial working memory in rats and monkeys: Pharmacological reversal of stress-induced impairment. J. Neurosci. 1996, 16, 7768–7775. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Hermans, E.J.; van Marle, H.J.; Luo, J.; Fernández, G. Acute psychological stress reduces working memory-related activity in the dorsolateral prefrontal cortex. Biol. Psychiatry 2009, 66, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Kohn, N.; Hermans, E.J.; Fernández, G. Cognitive benefit and cost of acute stress is differentially modulated by individual brain state. Soc. Cogn. Affect. Neurosci. 2017, 12, 1179–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiGangi, J.A.; Gomez, D.; Mendoza, L.; Jason, L.A.; Keys, C.B.; Koenen, K.C. Pretrauma risk factors for posttraumatic stress disorder: A systematic review of the literature. Clin. Psychol. Rev. 2013, 33, 728–744. [Google Scholar] [CrossRef] [PubMed]
- Olff, M.; Polak, A.R.; Witteveen, A.B.; Denys, D. Executive function in posttraumatic stress disorder (PTSD) and the influence of comorbid depression. Neurobiol. Learn. Mem. 2014, 112, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Kotler, M.; Iancu, I.; Efroni, R.; Amir, M. Anger, impulsivity, social support, and suicide risk in patients with posttraumatic stress disorder. J. Nerv. Ment. Dis. 2001, 189, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Glass, D.C.; Reim, B.; Singer, J.E. Behavioral consequences of adaptation to controllable and uncontrollable noise. J. Exp. Soc. Psychol. 1971, 7, 244–257. [Google Scholar] [CrossRef]
- Schuitevoerder, S.; Rosen, J.W.; Twamley, E.W.; Ayers, C.R.; Sones, H.; Lohr, J.B.; Goetter, E.M.; Fonzo, G.A.; Holloway, K.J.; Thorp, S.R. A meta-analysis of cognitive functioning in older adults with PTSD. J. Anxiety Disord. 2013, 27, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Mohlman, J.; Gorman, J.M. The role of executive functioning in CBT: A pilot study with anxious older adults. Behav. Res. Ther. 2005, 43, 447–465. [Google Scholar] [CrossRef] [PubMed]
- Olff, M. Sex and gender differences in post-traumatic stress disorder: An update. Eur. J. Psychotraumatol. 2017, 8, 1351204. [Google Scholar] [CrossRef]
- Harned, M.S.; Ormerod, A.J.; Palmieri, P.A.; Collinsworth, L.L.; Reed, M. Sexual assault and other types of sexual harassment by workplace personnel: A comparison of antecedents and consequences. J. Occup. Health Psychol. 2002, 7, 174–188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ASD (n = 27) | HC (n = 25) | Wald X2 | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | F | p | |
| Age (years) | 27.76 | 10.78 | 28.03 | 6.57 | 0.01 | 0.914 |
| Education (years) | 13.83 | 2.78 | 15.72 | 2.49 | 6.14 | 0.0132 * |
| IQ | 103.71 | 16.19 | 113.24 | 8.37 | 6.58 1 | 0.0138 * |
| Vocabulary | 11.71 | 2.90 | 12.68 | 2.17 | 1.66 1 | 0.2040 |
| BDI-II | 27.64 | 12.45 | 6.64 | 4.4 | 63.28 | <0.0001 *** |
| BAI | 28.36 | 15.2 | 2.84 | 3.05 | 67.76 | <0.0001 *** |
| STAXI-S | 20.32 | 8.44 | 10.72 | 1.14 | 54.72 | <0.0001 *** |
| STAXI-T | 18.96 | 5.78 | 17.88 | 5.04 | 0.50 | 0.4801 |
| PSS-SR-total | 37.2 | 9.27 | - | - | - | - |
| PSS-SR-reexperience | 10.36 | 2.91 | - | - | - | - |
| PSS-SR-avoidance | 4.92 | 1.38 | - | - | - | - |
| PSS-SR-numbing | 10.16 | 4.26 | - | - | - | - |
| PSS-SR-hyperarousal | 11.76 | 2.74 | - | - | - | - |
| PSS-SR-dysphoria | 16.88 | 5.25 | - | - | - | - |
| ASD (n = 23) | NC (n = 25) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Wald X2 | p | p a | p b | |
| IED-TE | 20.52 | 12.89 | 15.96 | 10.49 | 13.72 | 0.0002 *** | 0.0182 * | 0.0228 * |
| IED-TT | 83.70 | 20.21 | 77.92 | 17.54 | 1.13 | 0.2881 | 0.5623 | 0.6094 |
| SOC-ITT (msec) | 5929.26 | 4245.15 5 | 12,623.36 | 13,989.06 | 7.42 | 0.0064 * | 0.0199 * | 0.0508 |
| SOC-PS | 7.78 | 2.13 | 9.16 | 1.68 | 5.95 | 0.0148 * | 0.4733 | 0.2262 |
| SSP-SL | 6.96 | 1.94 | 7.76 | 1.27 | 2.79 | 0.0948 | 0.3137 | 0.6396 |
| SSP-TE | 13.22 | 8.71 | 10.8 | 7.49 | 5.85 | 0.0068 * | 0.0013 ** | 0.0066 *** |
| SST-PSS | 0.52 | 0.14 | 0.62 | 0.15 | 5.34 | 0.0209 * | 0.1636 | 0.0520 |
| SST-RT (msec) | 517.06 | 207.86 | 698.77 | 234.25 | 7.76 | 0.0053 ** | 0.0191 * | 0.0066 ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.M.; Choi, J.-S.; Lee, J.S.; Lee, J.-Y.; Lee, S.; Jung, H.Y. Impaired Executive Functioning of Sexual Assault Survivors with Acute Stress Disorder. J. Clin. Med. 2018, 7, 362. https://doi.org/10.3390/jcm7100362
Park SM, Choi J-S, Lee JS, Lee J-Y, Lee S, Jung HY. Impaired Executive Functioning of Sexual Assault Survivors with Acute Stress Disorder. Journal of Clinical Medicine. 2018; 7(10):362. https://doi.org/10.3390/jcm7100362
Chicago/Turabian StylePark, Su Mi, Jung-Seok Choi, Ji Sun Lee, Jun-Young Lee, Saerom Lee, and Hee Yeon Jung. 2018. "Impaired Executive Functioning of Sexual Assault Survivors with Acute Stress Disorder" Journal of Clinical Medicine 7, no. 10: 362. https://doi.org/10.3390/jcm7100362