Addressing Opioid-Related Chemical Coping in Long-Term Opioid Therapy for Chronic Noncancer Pain: A Multicenter, Observational, Cross-Sectional Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
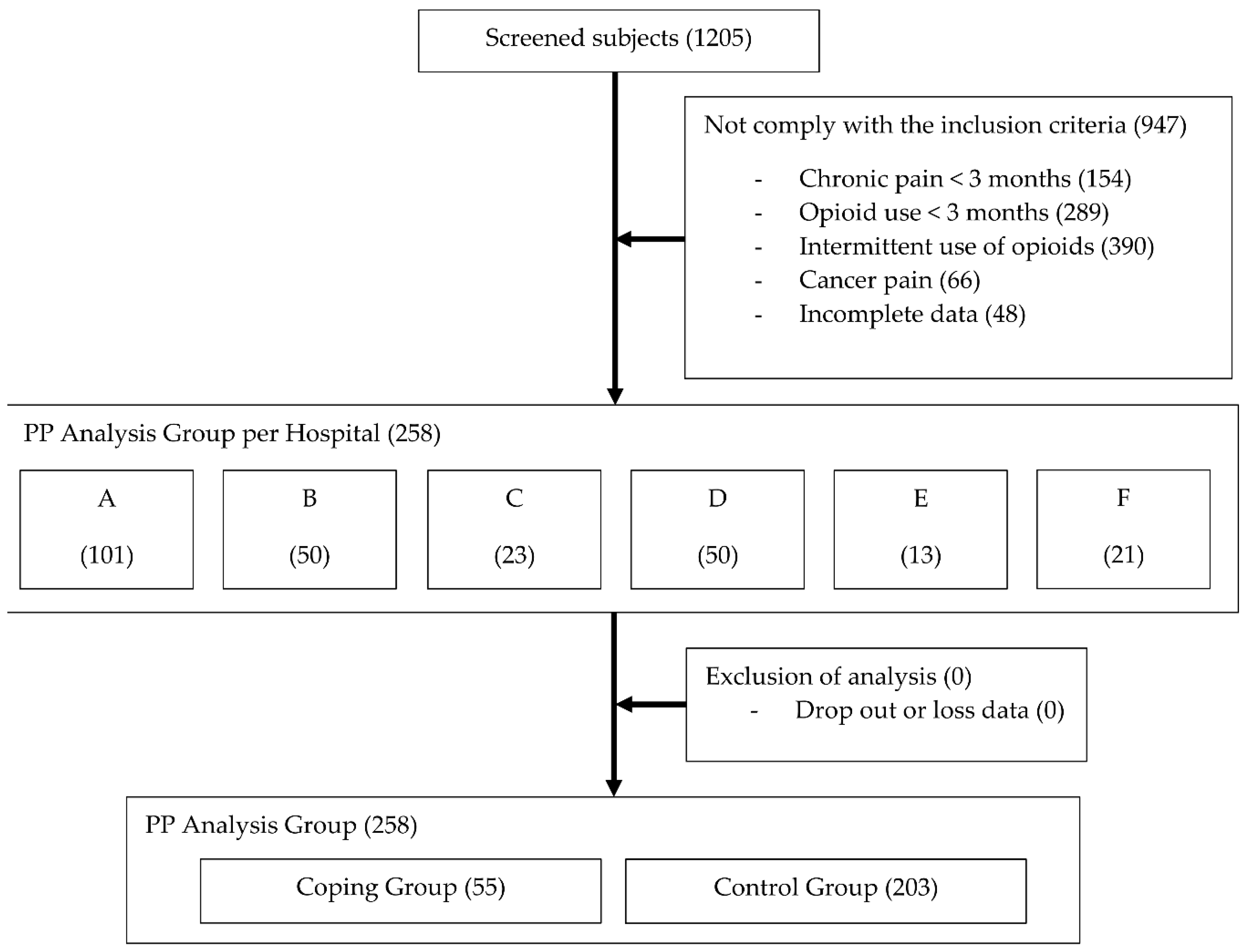
2.1. Study Participants
2.2. Evaluation of Opioid-Related Chemical Coping
2.3. Outcome Measurements
2.4. Sample Size Calculation and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brennan, F.; Cousins, M.J. Pain Relief as a Human Right. Pain Clin. Updat. 2004, 12, 1–4. [Google Scholar]
- Centers for Disease Control and Prevention. Opioid Prescribing 2017. Available online: https://www.cdc.gov/vitalsigns/opioids/index.html (accessed on 12 May 2018).
- Krnic, D.; Anic-Matic, A.; Dosenovic, S.; Draganic, P.; Zezelic, S.; Puljak, L. National consumption of opioid and nonopioid analgesics in Croatia: 2007–2013. Ther. Clin. Risk Manag. 2015, 11, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Pain & Policy Studies Group. Opioid Consumption Data 2017. Available online: http://www.painpolicy.wisc.edu/opioid-consumption-data (accessed on 11 May 2018).
- Duthey, B.; Scholten, W. Adequacy of opioid analgesic consumption at country, global, and regional levels in 2010, its relationship with development level, and changes compared with 2006. J. Pain Symptom Manag. 2014, 47, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Le Merrer, J.; Becker, J.A.; Befort, K.; Kieffer, B.L. Reward processing by the opioid system in the brain. Physiol. Rev. 2009, 89, 1379–1412. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2015, 162, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.S.; Park, C.K.; Cho, K.J.; Choi, K.H.; Kim, J.H.; Kim, S.B.; Kuh, S.U.; Lee, J.C.; Lee, J.H.; Lee, K.Y.; et al. A Nationwide Retrospective Study of Opioid Management Patterns in 2,468 Patients with Spinal Pain in Korea. Asian Spine J. 2016, 10, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Krebs, E.E.; Gravely, A.; Nugent, S.; Jensen, A.C.; DeRonne, B.; Goldsmith, E.S.; Kroenke, K.; Bair, M.J.; Noorbaloochi, S. Effect of Opioid vs. Nonopioid Medications on Pain-Related Function in Patients with Chronic Back Pain or Hip or Knee Osteoarthritis Pain: The SPACE Randomized Clinical Trial. JAMA 2018, 319, 872–882. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Prescription of Long-Acting Opioids and Mortality in Patients with Chronic Noncancer Pain. JAMA 2016, 315, 2415–2423. [Google Scholar] [CrossRef] [PubMed]
- Kirsh, K.L.; Jass, C.; Bennett, D.S.; Hagen, J.E.; Passik, S.D. Initial development of a survey tool to detect issues of chemical coping in chronic pain patients. Palliat. Support. Care 2007, 5, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.H.; Hui, D.; Bruera, E. A Pilot Study to Define Chemical Coping in Cancer Patients Using the Delphi Method. J. Palliat. Med. 2015, 18, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Koob, G.F.; McLellan, A.T. Neurobiologic Advances from the Brain Disease Model of Addiction. N. Engl. J. Med. 2016, 374, 363–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruera, E.; Schoeller, T.; Wenk, R.; MacEachern, T.; Marcelino, S.; Hanson, J.; Suarez-Almazor, M. A prospective multicenter assessment of the Edmonton staging system for cancer pain. J. Pain Symptom Manag. 1995, 10, 348–355. [Google Scholar] [CrossRef]
- Nikulina, V.; Guarino, H.; Acosta, M.C.; Marsch, L.A.; Syckes, C.; Moore, S.K.; Portenoy, R.K.; Cruciani, R.A.; Turk, D.C.; Rosenblum, A. Patient vs. provider reports of aberrant medication-taking behavior among opioid-treated patients with chronic pain who report misusing opioid medication. Pain 2016, 157, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, E. Assessment and management of chemical coping in patients with cancer. J. Clin. Oncol. 2014, 32, 1734–1738. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.H.; Tanco, K.; Park, J.C.; Wong, A.; Seo, L.; Liu, D.; Chisholm, G.; Williams, J.; Hui, D.; Bruera, E. Frequency, Predictors, and Medical Record Documentation of Chemical Coping Among Advanced Cancer Patients. Oncologist 2015, 20, 692–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voon, P.; Karamouzian, M.; Kerr, T. Chronic pain and opioid misuse: A review of reviews. Subst. Abuse Treat Prev. Policy 2017, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- Vowles, K.E.; McEntee, M.L.; Julnes, P.S.; Frohe, T.; Ney, J.P.; van der Goes, D.N. Rates of opioid misuse, abuse, and addiction in chronic pain: A systematic review and data synthesis. Pain 2015, 156, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Green, C.R.; Anderson, K.O.; Baker, T.A.; Campbell, L.C.; Decker, S.; Fillingim, R.B.; Kalauokalani, D.A.; Lasch, K.E.; Myers, C.; Tait, R.C.; et al. The unequal burden of pain: Confronting racial and ethnic disparities in pain. Pain Med. 2003, 4, 277–294. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Cheville, A. Management of Chronic Pain in the Aftermath of the Opioid Backlash. JAMA 2017, 317, 2365–2366. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J. The supply chain of medicinal controlled substances: Addressing the Achilles heel of drug diversion. J. Pain Palliat. Care Pharmacother. 2012, 26, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.J.; Logan, J.E.; Toblin, R.L.; Kaplan, J.A.; Kraner, J.C.; Bixler, D.; Crosby, A.E.; Paulozzi, L.J. Patterns of abuse among unintentional pharmaceutical overdose fatalities. JAMA 2008, 300, 2613–2620. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, T.; Christrup, L.L.; Drewes, A.M.; Fallon, M.T.; Kress, H.G.; McQuay, H.J.; Mikus, G.; Morlion., B.J.; Perez-Cajaraville, J.; Pogatzki-Zahn, E.; et al. European Pain Federation position paper on appropriate opioid use in chronic pain management. Eur. J. Pain 2017, 21, 3–19. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; p. 541. ISBN 13:978-0890425558. [Google Scholar]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- National Center for Injury Prevention and Control. CDC Compilation of Benzodiazepines, Muscle Relaxants, Stimulants, Zolpidem, and Opioid Analgesics with Oral Morphine Milligram Equivalent Conversion Factors; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016; Grant No. 2010-DG-BX-K088; Available online: http://www.pdmpassist.org/pdf/BJA_performance_measure_aid_MME_conversion.pdf (accessed on 11 May 2018).
- Brown, R.L.; Rounds, L.A. Conjoint screening questionnaires for alcohol and other drug abuse: Criterion validity in a primary care practice. Wis. Med. J. 1995, 94, 135–140. [Google Scholar] [PubMed]
- Yun, Y.H.; Mendoza, T.R.; Heo, D.S.; Yoo, T.; Heo, B.Y.; Park, H.A.; Shin, H.C.; Wang, X.S.; Cleeland, C.S. Development of a cancer pain assessment tool in Korea: A validation study of a Korean version of the brief pain inventory. Oncology 2004, 66, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Won, C.W.; Rho, Y.G.; SunWoo, D.; Lee, Y.S. The Validity and Reliability of Korean Instrumental Activities of Daily Living (K-IADL) Scale. J. Korean Geriatr. Soc. 2002, 6, 273–280. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, H.; Bolton, J. Assessing the clinical significance of change scores recorded on subjective outcome measures. J. Manip. Physiol. Ther. 2004, 27, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Jovey, R.D. Opioids, pain, and addiction–practical strategies. Br. J. Pain 2012, 6, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.M.; Mendoza, T.R.; Sit, L.; Passik, S.; Scher, H.I.; Cleeland, C.; Basch, E. The Brief Pain Inventory and its “pain at its worst in the last 24 h” item: Clinical trial endpoint considerations. Pain Med. 2010, 11, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.F. The hospital anxiety and depression scale. Occup. Med. 2014, 64, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.J.; Choi, S.H.; Lee, B.H.; Kwon, J.C.; Na, D.L.; Han, S.H. The Reliability and Validity of the Korean Instrumental Activities of Daily Living (K-IADL). J. Korean Neurol. Assoc. 2002, 20, 8–14. [Google Scholar]
- Jung, Y.E.; Min, J.A.; Shin, A.Y.; Han, S.Y.; Lee, K.U.; Kim, T.S.; Park, J.E.; Choi, S.W.; Lee, S.H.; Choi, K.S.; et al. The Korean version of the Connor-Davidson Resilience Scale: An extended validation. Stress Health 2012, 28, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Coon, C.D.; Cappelleri, J.C. Interpreting Change in Scores on Patient-Reported Outcome Instruments. Ther. Innov. Regul. Sci. 2015, 50, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edlund, M.J.; Martin, B.C.; Fan, M.Y.; Devries, A.; Braden, J.B.; Sullivan, M.D. Risks for opioid abuse and dependence among recipients of chronic opioid therapy: Results from the TROUP study. Drug Alcohol Depend. 2010, 112, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014; HHS Publication No. (SMA) 14-4863. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.pdf (accessed on 27 March 2018).
- Schnohr, C.; Hojbjerre, L.; Riegels, M.; Ledet, L.; Larsen, T.; Schultz-Larsen, K.; Petersen, L.; Prescott, E.; Grønbaek, M. Does educational level influence the effects of smoking, alcohol, physical activity, and obesity on mortality? A prospective population study. Scand. J. Public Health 2004, 32, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.D.; Scherrer, J.F.; Lynskey, M.T.; Agrawal, A.; Duncan, A.E.; Haber, J.R.; Heath, A.C.; Bucholz, K.K. Associations of alcohol, nicotine, cannabis, and drug use/dependence with educational attainment: Evidence from cotwin-control analyses. Alcohol Clin. Exp. Res. 2012, 36, 1412–1420. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-operation and Development (OECD). Education at a Glance 2017: OECD Indicators; OECD Publishing: Paris, France, 2017; Available online: https://read.oecd-ilibrary.org/education/education-at-a-glance-2017_eag-2017-en#page8 (accessed on 7 May 2018).
- Morasco, B.J.; Lovejoy, T.I.; Dobscha, S.K. The Relationship between PTSD and Chronic Pain: Mediating Role of Coping Strategies and Depression. Pain 2013, 154, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Pope, H.G. The concept of affective spectrum disorder: Relationship to fibromyalgia and other syndromes of chronic fatigue and chronic muscle pain. Baillière’s Clin. Rheumatol. 1994, 8, 839–856. [Google Scholar] [CrossRef]
- Crabtree, D.; Ganty, P. Common functional pain syndromes. BJA Educ. 2016, 16, 334–340. [Google Scholar] [CrossRef]
- Cheatle, M.D.; Gallagher, R.M. Chronic pain and comorbid mood and substance use disorders: A biopsychosocial treatment approach. Curr. Psychiatry Rep. 2006, 8, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, J.A.; Rukstalis, M.; Hoffman, S.N.; Han, J.J.; Erlich, P.M.; Gerhard, G.S.; Stewart, W.F. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction 2010, 105, 1776–1782. [Google Scholar] [CrossRef] [PubMed]
- Vietri, J.; Joshi, A.V.; Barsdorf, A.I.; Mardekian, J. Prescription opioid abuse and tampering in the United States: Results of a self-report survey. Pain Med. 2014, 15, 2064–2074. [Google Scholar] [CrossRef] [PubMed]
- Markou, A.; Kosten, T.R.; Koob, G.F. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998, 18, 135–174. [Google Scholar] [CrossRef]
- Verdam, M.G.E.; Oort, F.J.; Sprangers, M.A.G. Item bias detection in the Hospital Anxiety and Depression Scale using structural equation modeling: Comparison with other item bias detection methods. Qual. Life Res. 2017, 26, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Witkiewitz, K.; Vowles, K.E. Alcohol and Opioid Use, Co-Use, and Chronic Pain in the Context of the Opioid Epidemic: A Critical Review. Alcohol Clin. Exp. Res. 2018, 42, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Dunn, K.M.; Saunders, K.W.; Rutter, C.M.; Banta-Green, C.J.; Merrill, J.O.; Sullivan, M.D.; Weisner, C.M.; Silverberg, M.J.; Campbell, C.I.; Psaty, B.M.; et al. Opioid prescriptions for chronic pain and overdose: A cohort study. Ann. Intern. Med. 2010, 152, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.; Mamdani, M.M.; Dhalla, I.A.; Paterson, J.M.; Juurlink, D.N. Opioid dose and drug-related mortality in patients with nonmalignant pain. Arch. Intern. Med. 2011, 171, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, N.; Funk, M.J.; Proescholdbell, S.; Hirsch, A.; Ribisl, K.M.; Marshall, S. Cohort Study of the Impact of High-Dose Opioid Analgesics on Overdose Mortality. Pain Med. 2016, 17, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.G.; Messina, J.; Xie, F.; Rathmell, J. Long-term safety and tolerability of fentanyl buccal tablet for the treatment of breakthrough pain in opioid-tolerant patients with chronic pain: An 18-month study. J. Pain Symptom Manag. 2010, 40, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.K.; Bennett, D.S.; Rauck, R.; Simon, S.; Taylor, D.; Brennan, M.; Shoemaker, S. Prevalence and characteristics of breakthrough pain in opioid-treated patients with chronic noncancer pain. J. Pain 2006, 7, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Smith, H. A Comprehensive Review of Rapid-Onset Opioids for Breakthrough Pain. CNS Drugs 2012, 26, 509–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granata, R.; Bossi, P.; Bertulli, R.; Saita, L. Rapid-onset opioids for the treatment of breakthrough cancer pain: Two cases of drug abuse. Pain Med. 2014, 15, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Passik, S.D.; Messina, J.; Golsorkhi, A.; Xie, F. Aberrant Drug-Related Behavior Observed During Clinical Studies Involving Patients Taking Chronic Opioid Therapy for Persistent Pain and Fentanyl Buccal Tablet for Breakthrough Pain. J. Pain Symptom Manag. 2011, 41, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.H.; Tanco, K.; Hui, D.; Reddy, A.; Bruera, E. Chemical coping versus pseudoaddiction in patients with cancer pain. Palliat. Support. Care 2014, 12, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.A.; Shortreed, S.M.; Saunders, K.W.; LeResche, L.; Von Korff, M. Association of levels of opioid use with pain and activity interference among patients initiating chronic opioid therapy: A longitudinal study. Pain 2016, 157, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Voon, P.; Buxton, J.A.; Wood, E.; Montaner, J.S.; Kerr, T. Dose-response relationship between functional pain interference and nonmedical analgesic use: Findings from a nationally representative Canadian survey. Can. J. Pain 2018, 2, 103–112. [Google Scholar] [CrossRef]
- Jacobs, M.S. Psychological Factors Influencing Chronic Pain and the Impact of Litigation. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 135–141. [Google Scholar] [CrossRef]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Eccleston, C.; Morley, S.J.; Williams, A.C. Psychological approaches to chronic pain management: Evidence and challenges. Br. J. Anaesth. 2013, 111, 59–63. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Turk, D.C. Behavioral and Cognitive–Behavioral Treatment for Chronic Pain: Outcome, Predictors of Outcome, and Treatment Process. Spine (Phila Pa 1976) 2002, 27, 2564–2573. [Google Scholar] [CrossRef]
- Lee, C.S.; Kim, D.; Park, S.Y.; Lee, C.S.; Kim, Y.C.; Moon, J.Y. Usefulness of the Korean Version of the CAGE-Adapted to Include Drugs Combined with Clinical Predictors to Screen for Opioid-related Aberrant Behavior. Anesth. Analg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.S.; Shim, J.Y.; Choi, Y.S.; Kim, D.Y.; Hwang, I.G.; Baek, S.K.; Shin, J.Y.; Lee, J.; Lee, C.G. Physician’s Attitude toward Treating Breakthrough Cancer Pain in Korea. Korean J. Hosp. Palliat. Care 2017, 20, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Levy, B.; Paulozzi, L.; Mack, K.A.; Jones, C.M. Trends in Opioid Analgesic–Prescribing Rates by Specialty, U.S., 2007–2012. Am. J. Prev. Med. 2015, 49, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N.; Sheehan, K.A.; Scanlan, E.; Matthews, M.; Ross, E.L. Beliefs and attitudes about opioid prescribing and chronic pain management: Survey of primary care providers. J. Opioid Manag. 2014, 10, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Webster, F.; Bremner, S.; Oosenbrug, E.; Durant, S.; McCartney, C.J.; Katz, J. From Opiophobia to Overprescribing: A Critical Scoping Review of Medical Education Training for Chronic Pain. Pain Med. 2017, 18, 1467–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, J.; Radbruch, L.; Torode, J.; Cherny, N.I. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Asia: A report from the Global Opioid Policy Initiative (GOPI). Ann. Oncol. 2013, 24 (Suppl. 11), xi24–xi32. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.I. Drug Control Policy in Korea. Vancouver, British Columbia, Canada: International Centre for Criminal Law Reform and Criminal Justice Policy 2014. Available online: http://www.tcm-intl.com/public/data/%E6%B3%95%E5%BE%8B%E6%B3%95%E8%A7%84/%E5%9B%BD%E9%99%85/%E9%9F%A9%E5%9B%BD/Drug%20Control%20Policy%20in%20Korea.pdf (accessed on 12 May 2018).
- Feng, L.Y.; Yu, W.J.; Chang, W.T.; Han, E.; Chung, H.; Li, J.H. Comparison of illegal drug use pattern in Taiwan and Korea from 2006 to 2014. Subst. Abuse Treat. Prev. Policy 2016, 11, 34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1. Please read carefully the definition of opioid-related chemical coping: “Opioid-related chemical coping is the use of opioids to cope with emotional distress characterized by inappropriate and/or excessive opioid use” [12]. | |
| 2. The following are aberrant behaviors related to chemical coping with opioids. Please mark all the behaviors which you believe the patient presents: | |
| Behavior | Check |
| |
| Variable | Overall (n = 258) | Control (n = 203) | Coping * (n = 55) | p-Value |
|---|---|---|---|---|
| Gender, n (%) Male Female | 153 (59.3) 105 (40.7) | 120 (59.1) 83 (40.9) | 33 (60.0) 22 (40.0) | 0.905 |
| Age, mean ± SD, years | 52.89 ± 3.36 | 53.79 ± 13.54 | 48.58 ± 12.25 | 0.038 |
| Ethnicity, n (%), Asian | 258 (100) | 203 (78.7) | 55 (21.3) | - |
| BMI, mean ± SD, kg/m2 | 24.81 ± 4.03 | 24.89 ± 3.87 | 24.51 ± 4.58 | 0.544 |
| Marital status, n (%) Married Single Divorced/Widowed | 64 (24.9) 185 (72.0) 8 (3.1) | 50 (24.8) 146 (72.3) 6 (3.0) | 14 (25.5) 39 (70.9) 2 (3.6) | 0.960 |
| Education level, n (%) <high school ≥high school | 58 (22.6) 200 (77.5) | 53 (26.1) 150 (73.9) | 5 (9.1) 50 (90.9) | 0.007 |
| Employment status, n (%) Unemployed (students and housewives included) Employed | 192 (75.6) 62 (24.4) | 152 (75.6) 49 (24.4) | 40 (75.5) 13 (24.5) | 0.982 |
| Religion, n (%) No Yes | 130 (50.6) 127 (49.4) | 106 (52.5) 96 (47.5) | 24 (43.6) 31 (56.4) | 0.245 |
| Chronicity of pain, mean ± SD, months | 74.55 ± 64.25 | 73.23 ± 66.09 | 79.44 ± 57.23 | 0.526 |
| NRS, mean ± SD, points Initial Current Absolute change p-value of absolute change Percent change | 7.38 ± 1.61 6.55 ± 2.09 −0.83 ± 2.29 <0.001 −8.6 ± 32.3 | 7.37 ± 1.54 6.51 ± 2.10 −0.89 ± 2.41 <0.001 −8.9 ± 22.1 | 7.43 ± 1.89 6.86 ± 2.07 −0.58 ± 1.74 0.048 −8.5 ± 34.4 | 0.730 0.309 0.364 0.936 † |
| Etiology of pain, n (%) Trauma Surgery Degenerative Disease Combined Idiopathic | 128 (49.6) 51 (19.8) 15 (5.8) 73 (26.7) 1 (0.4) 9 (3.5) | 96 (47.3) 43 (21.2) 10 (4.9) 56 (28.1) 1 (0.5) 6 (3.0) | 32 (58.2) 8 (14.5) 5 (9.1) 17 (32.7) 0 (0.0) 3 (5.5) | 0.152 0.273 0.325 ‡ 0.236 1 0.407 ‡ |
| Location of pain, n (%) Head and Neck Chest or Abdomen Back Extremities Others§ or unknown | 42 (16.3) 35 (13.6) 102 (39.5) 197 (76.4) 20 (7.8) | 27 (13.3) 24 (11.8) 77 (37.9) 155 (76.4) 15 (7.4) | 15 (27.3) 11 (20.0) 25 (45.5) 42 (76.4) 5 (9.1) | 0.013 0.116 0.311 0.999 0.776 |
| Type of pain, n (%) Nociceptive Neuropathic Functional Mixed | 36 (14.0) 197 (76.4) 15 (5.8) 27 (10.5) | 29 (14.3) 160 (78.8) 5 (2.5) 17 (8.4) | 7 (12.7) 37 (67.3) 10 (18.2) 10 (18.2) | 0.767 0.074 <0.001 ‡ 0.035 |
| Substance abuse history within 1 year, n (%) Yes Tobacco Alcohol Medication Illicit drugs Multiple | 79 (30.6) 62 (24.0) 19 (7.4) 6 (2.3) 0 (0.0) 1 (0.4) | 52 (25.6) 46 (22.7) 8 (3.9) 1 (0.5) 0 (0.0) 1 (0.5) | 27 (49.1) 16 (29.1) 11 (20.0) 5 (9.1) 0 (0.0) 0 (0.0) | 0.001 0.322 <0.001 <0.001 - 1.00 ‡ |
| Taken prescription drugs with alcohol within 1 year, n (%) | 29 (11.2) | 17 (8.5) | 12 (22.6) | 0.002 |
| Concurrent psychopathology, n (%) Yes Depression Anxiety PTSD Bipolar disorder Others | 120 (46.5) 84 (32.6) 25 (9.7) 52 (20.2) 6 (2.3) 22 (8.5) | 86 (42.4) 56 (27.6) 19 (9.4) 37 (18.2) 4 (2.0) 18 (8.9) | 34 (61.8) 28 (50.9) 6 (10.9) 15 (27.3) 2 (3.6) 4 (7.3) | 0.008 0.001 0.73 0.138 0.611 ‡ 1.00 ‡ |
| Secondary morbid gain, n (%) Miss work or studies Avoid military duty Ongoing litigation | 42 (53.1) 43 (16.7) | 30 (83.3) 46 (22.8) 28 (13.9) | 12 (92.3) 7 (13.0) 15 (27.8) | 0.658 0.157 0.010 |
| Suicidal ideation, n (%) | 172 (66.7) | 132 (65.3) | 40 (75.5) | 0.161 |
| Variable | Overall (n = 258) | Control (n = 203) | Coping * (n = 55) | p-Value |
|---|---|---|---|---|
| Duration of opioids, mean ± SD, months >12 months, n (%) | 16.34 ± 31.08 65 (25.2) | 15.90 ± 28.76 51 (25.1) | 17.85 ± 38.25 14 (25.5) | 0.722 0.747 |
| Opioid types, n (%) Long-acting Oral long-acting Transdermal patch Short-acting Oral short-acting Rapid onset fentanyl Intravenous | 231 (89.5) 213 (82.6) 85 (32.9) 145 (56.2) 141 (54.7) 15 (5.8) 12 (4.7) | 184 (90.6) 170 (83.7) 63 (31.0) 109 (53.7) 107 (52.7) 7 (3.4) 6 (3.0) | 47 (85.5) 43 (78.2) 22 (40.0) 36 (65.5) 34 (61.8) 8 (14.5) 6 (10.9) | 0.265 0.335 0.210 0.119 0.229 0.005 0.023 |
| MEDD, mean ± SD, mg/day ≥100 mg/day, n (%) ≥200 mg/day, n (%) | 129 ± 220 95 (36.8) 34 (13.2) | 119 ± 227 68 (33.5) 20 (9.9) | 169 ± 186 27 (49.1) 14 (25.5) | 0.006 † 0.033 0.002 |
| Number of visits per year to the opioid provider, mean ± SD | 22.77 ± 30.71 | 19.07 ± 18.86 | 36.35 ± 53.93 | 0.023 |
| ER visits seeking opioids, n (%) | 24 (9.3) | 9 (4.4) | 15 (27.3) | <0.001 |
| First opioid provider, n (%) Family doctor General physician Surgeon ER physician Pain physician Others ‡ Unknown | 2 (0.8) 6 (2.3) 20 (7.8) 2 (0.8) 209 (81.0) 18 (7.0) 1 (0.4) | 1 (0.5) 5 (2.5) 13 (6.4) 2 (1.0) 166 (81.8) 15 (7.4) 1 (0.5) | 1 (1.8) 1 (1.8) 7 (12.7) 0 (0.0) 43 (78.2) 3 (5.5) 0 (0.0) | 0.702 0.609 0.778 0.120 0.460 0.547 0.617 0.602 |
| Benzodiazepines, n (%) | 120 (46.5) | 95 (46.8) | 25 (45.5) | 0.859 |
| Non-opioid medications, n (%) Antidepressants Anticonvulsants Topical agents | 134 (51.9) 182 (70.5) 33 (12.8) | 107(55.4) 149 (77.2) 24 (12.4) | 27 (51.9) 33 (64.7) 9 (17.6) | 0.651 0.068 0.333 |
| Physical therapy, n (%) | 32 (12.4) | 28 (3.9) | 4 (7.4) | 0.203 |
| Variable | Overall (n = 258) | Control (n = 203) | Coping * (n = 55) | p-Value |
|---|---|---|---|---|
| CAGE-AID, n (%) Negative Positive (≥1 positive) | 79 (30.6) 179 (69.4) | 68 (33.5) 135 (66.5) | 11 (20.0) 44 (80.0) | 0.106 0.054 |
| PCS, mean ± SD, points ≥30 points, n (%) | 34.22 ± 12.27 170 (65.9) | 34.14 ± 12.33 134 (66.0) | 34.51 ± 12.18 36 (65.5) | 0.843 0.939 |
| BPI-SF, mean ± SD, points Worst NRS NRS on average NRS right now Pain relief (%) Pain interference General activity Mood Walking ability Normal work Relations with other people Sleep Enjoyment of life | 8.12 ± 1.97 6.63 ± 2.05 6.37 ± 2.36 48.44 ± 23.47 6.47 ± 2.48 6.59 ± 2.53 5.85 ± 3.14 6.38 ± 2.75 6.04 ± 3.26 6.29 ± 3.09 6.78 ± 3.00 | 7.95 ± 2.06 6.53 ± 2.05 6.29 ± 2.30 49.79 ± 22.39 6.31 ± 2.53 6.39 ± 2.56 5.77 ± 3.14 6.22 ± 2.79 5.88 ± 3.28 6.06 ± 3.12 6.66 ± 3.03 | 8.75 ± 1.42 6.98 ± 2.04 6.67 ± 2.58 43.45 ± 26.75 7.07 ± 2.20 7.35 ± 2.27 6.15 ± 3.15 6.96 ± 2.55 6.62 ± 3.15 7.15 ± 2.85 7.22 ± 2.85 | 0.001 0.152 0.288 0.112 0.043 0.013 0.437 0.076 0.137 0.021 0.221 |
| K-IADL, mean ± SD, points Percentage | 7.46 ± 7.18 64.01 ± 74.55 | 6.96 ± 6.90 58.28 ± 73.74 | 9.31 ± 7.90 85.18 ± 74.35 | 0.031 0.017 |
| PGIC, n (%), better | 108 (41.9) | 89 (43.8) | 19 (34.5) | 0.215 |
| Satisfaction scale, † Satisfied, n (%) Unsatisfied, n (%) | 190 (73.6) 68 (26.4) | 159 (78.3) 44 (21.7) | 31 (56.4) 24 (43.6) | 0.002 |
| HADS Anxiety, mean ± SD, points ≥11 (abnormal), n (%) Depression, mean ± SD, points ≥11 (abnormal), n (%) | 10.88 ± 4.99 125 (48.4) 11.76 ± 4.71 160 (62.0) | 10.72 ± 4.80 96 (47.3) 11.74 ± 4.35 127 (62.6) | 11.45 ± 5.66 29 (52.7) 11.80 ± 5.91 33 (60.0) | 0.381 0.474 0.938 0.728 |
| ISI, mean ± SD, points ≥15 (moderate-severe), n (%) ≥22 (severe), n (%) | 16.83 ± 7.63 162 (62.8) 88 (34.1) | 16.61 ± 7.62 124 (61.1) 66 (32.5) | 17.62 ± 7.66 38 (69.1) 22 (40.0) | 0.386 0.276 0.299 |
| K-CD-RISC, mean ± SD, points | 67.95 ± 22.06 | 68.77 ± 22.24 | 64.91 ± 21.30 | 0.250 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castañeda, A.M.; Lee, C.-S.; Kim, Y.-C.; Lee, D.; Moon, J.Y. Addressing Opioid-Related Chemical Coping in Long-Term Opioid Therapy for Chronic Noncancer Pain: A Multicenter, Observational, Cross-Sectional Study. J. Clin. Med. 2018, 7, 354. https://doi.org/10.3390/jcm7100354
Castañeda AM, Lee C-S, Kim Y-C, Lee D, Moon JY. Addressing Opioid-Related Chemical Coping in Long-Term Opioid Therapy for Chronic Noncancer Pain: A Multicenter, Observational, Cross-Sectional Study. Journal of Clinical Medicine. 2018; 7(10):354. https://doi.org/10.3390/jcm7100354
Chicago/Turabian StyleCastañeda, Anyela Marcela, Chang-Soon Lee, Yong-Chul Kim, Dasom Lee, and Jee Youn Moon. 2018. "Addressing Opioid-Related Chemical Coping in Long-Term Opioid Therapy for Chronic Noncancer Pain: A Multicenter, Observational, Cross-Sectional Study" Journal of Clinical Medicine 7, no. 10: 354. https://doi.org/10.3390/jcm7100354