Deep vs. Awake Extubation and LMA Removal in Terms of Airway Complications in Pediatric Patients Undergoing Anesthesia: A Systemic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
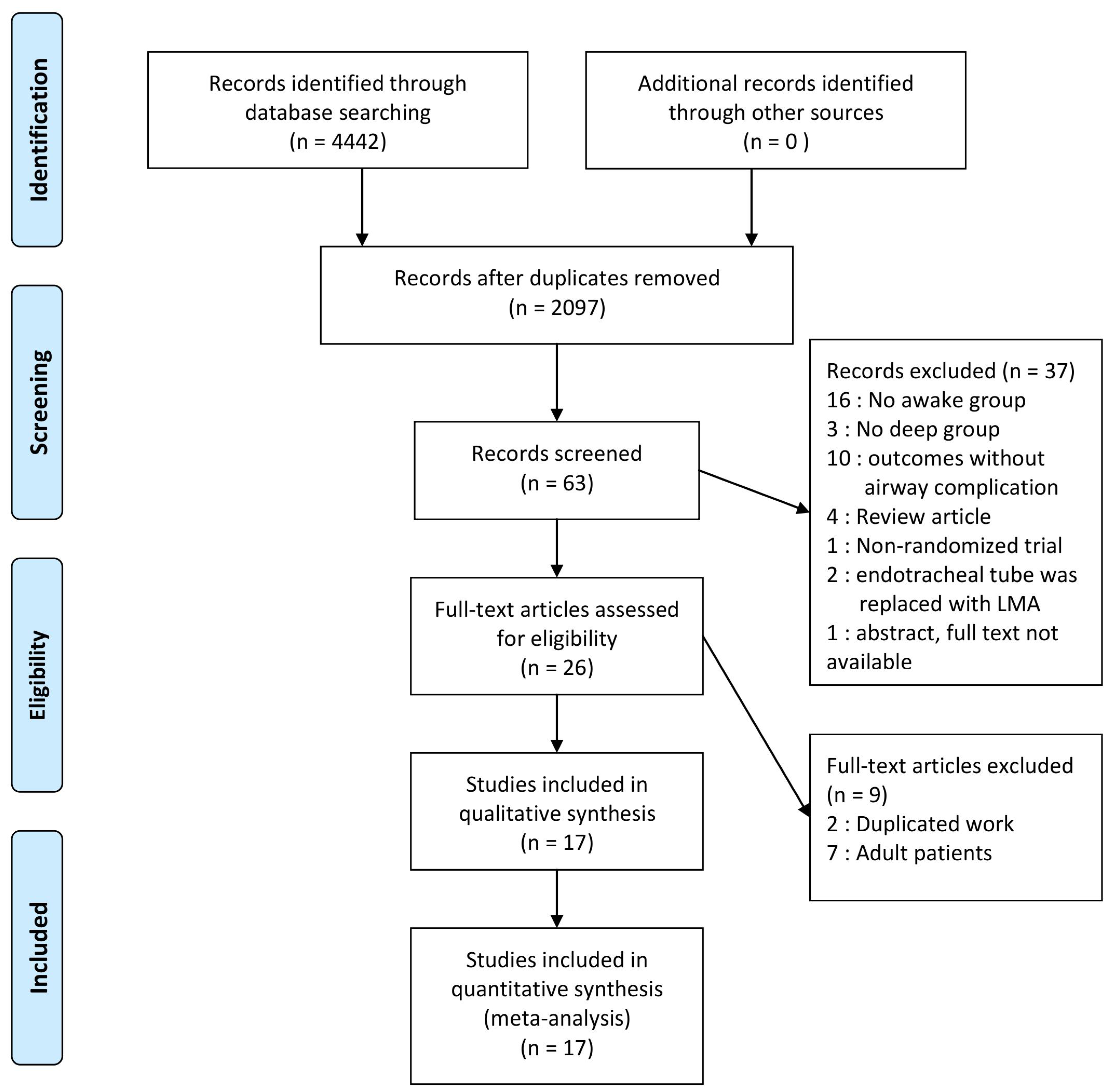
2.1. Data Sources and Search Strategy (Literature Search)
2.2. Study Selection (Trial Selection and Methodological Assessment)
2.3. Data Collection (Data Extraction)
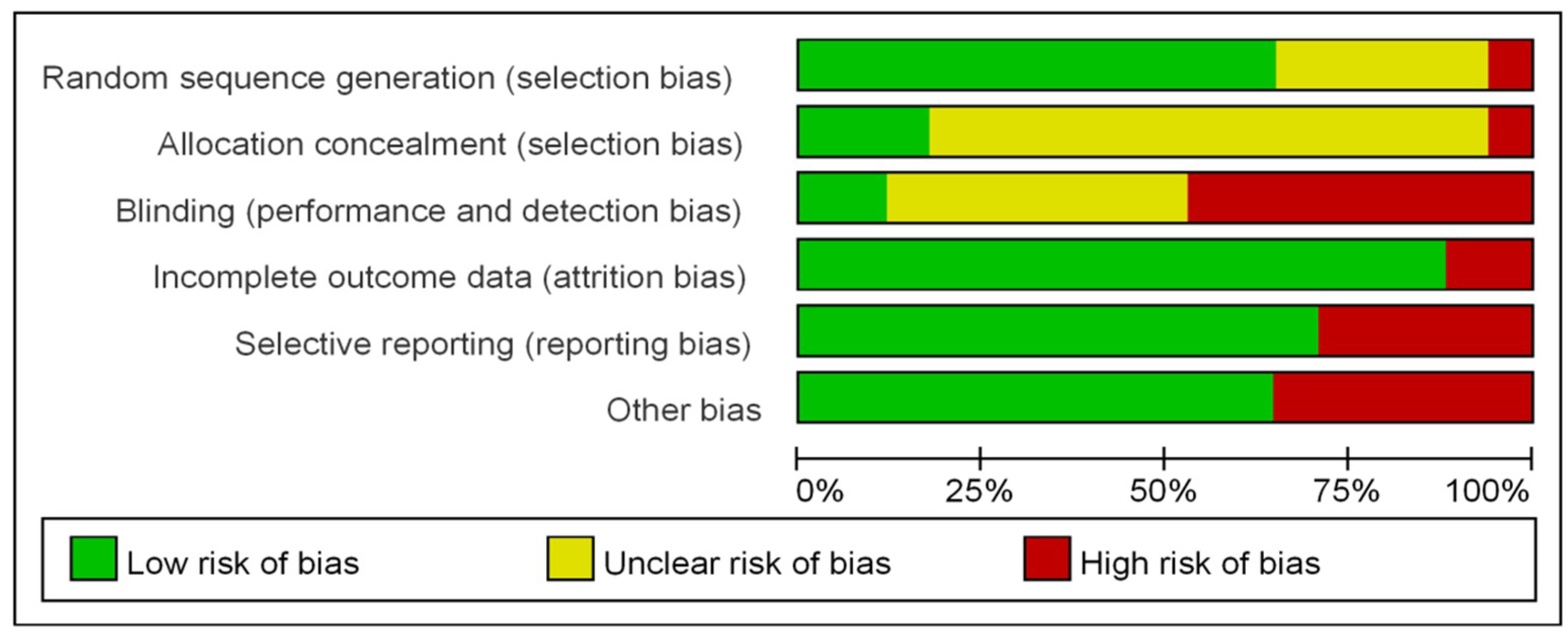
2.4. Methodological Quality and Risk of Bias Assessment
2.5. Outcomes Assessed
2.6. Data Synthesis and Statistical Analyses (Meta-Analysis)
2.7. Predefined Sources of Heterogeneity
3. Results
3.1. Characteristics of Trials and Patients
3.2. Methodological Quality and Risk of Bias (Risk of Bias Assessment)
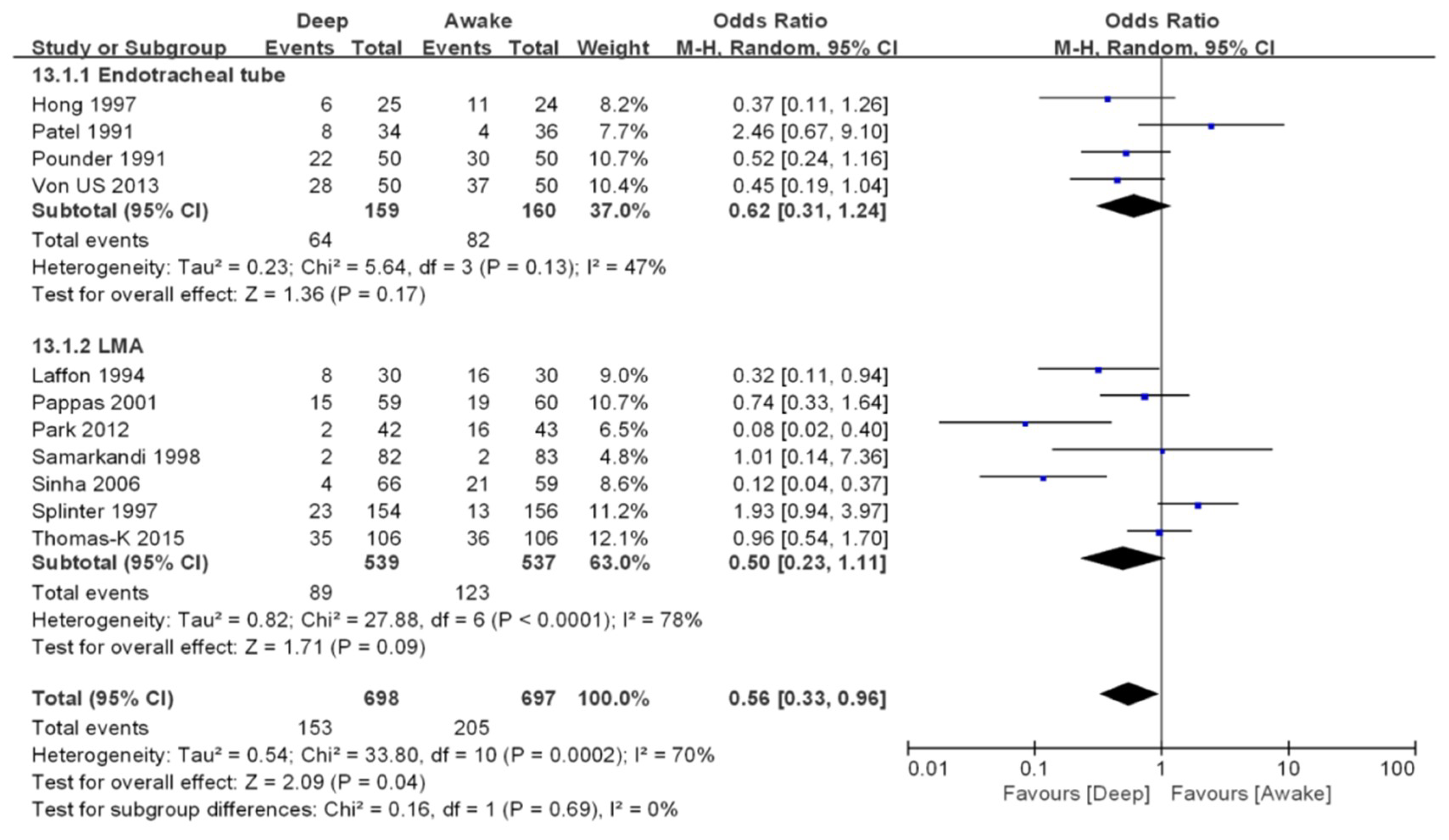
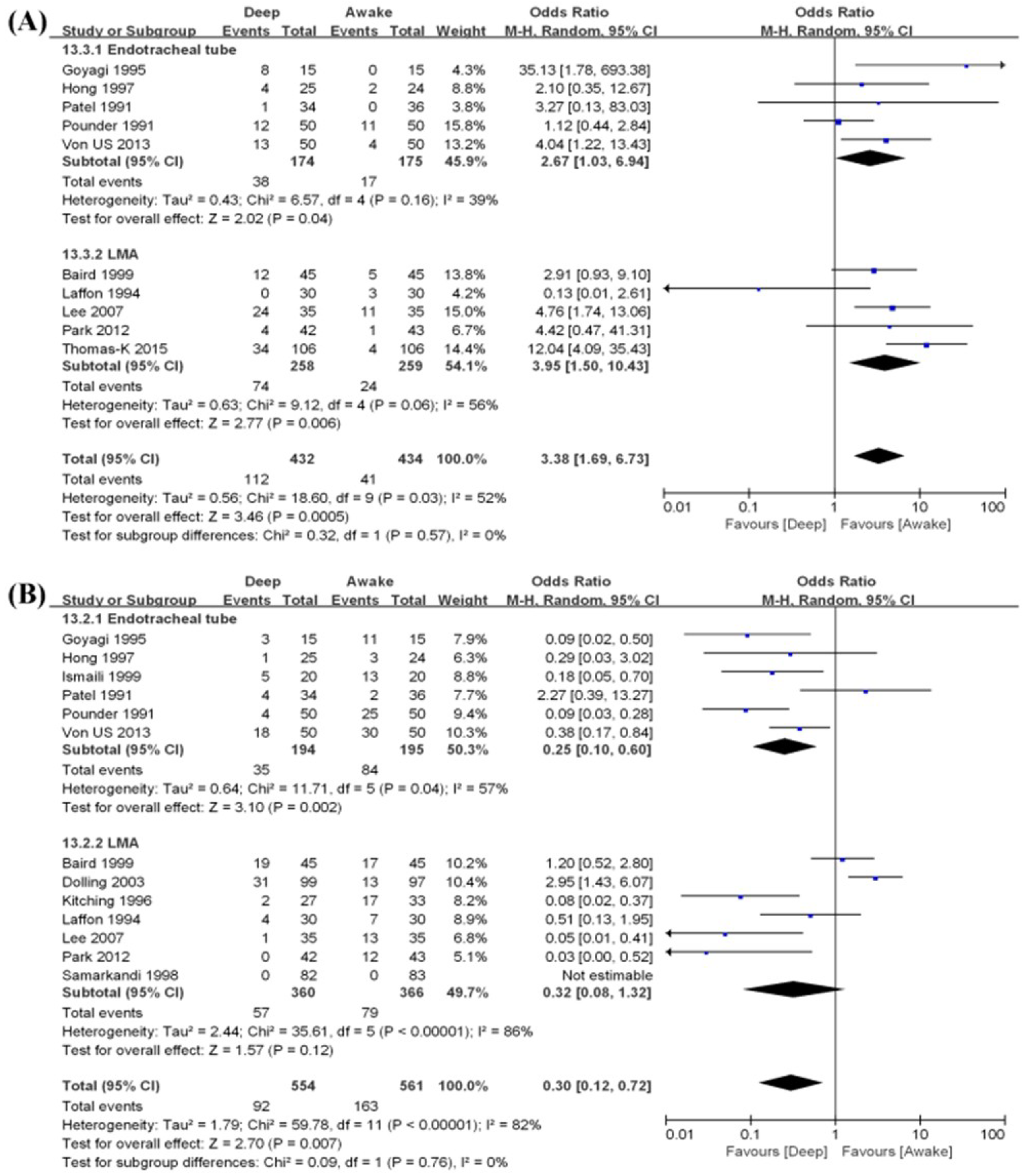
3.3. Outcome Synthesis
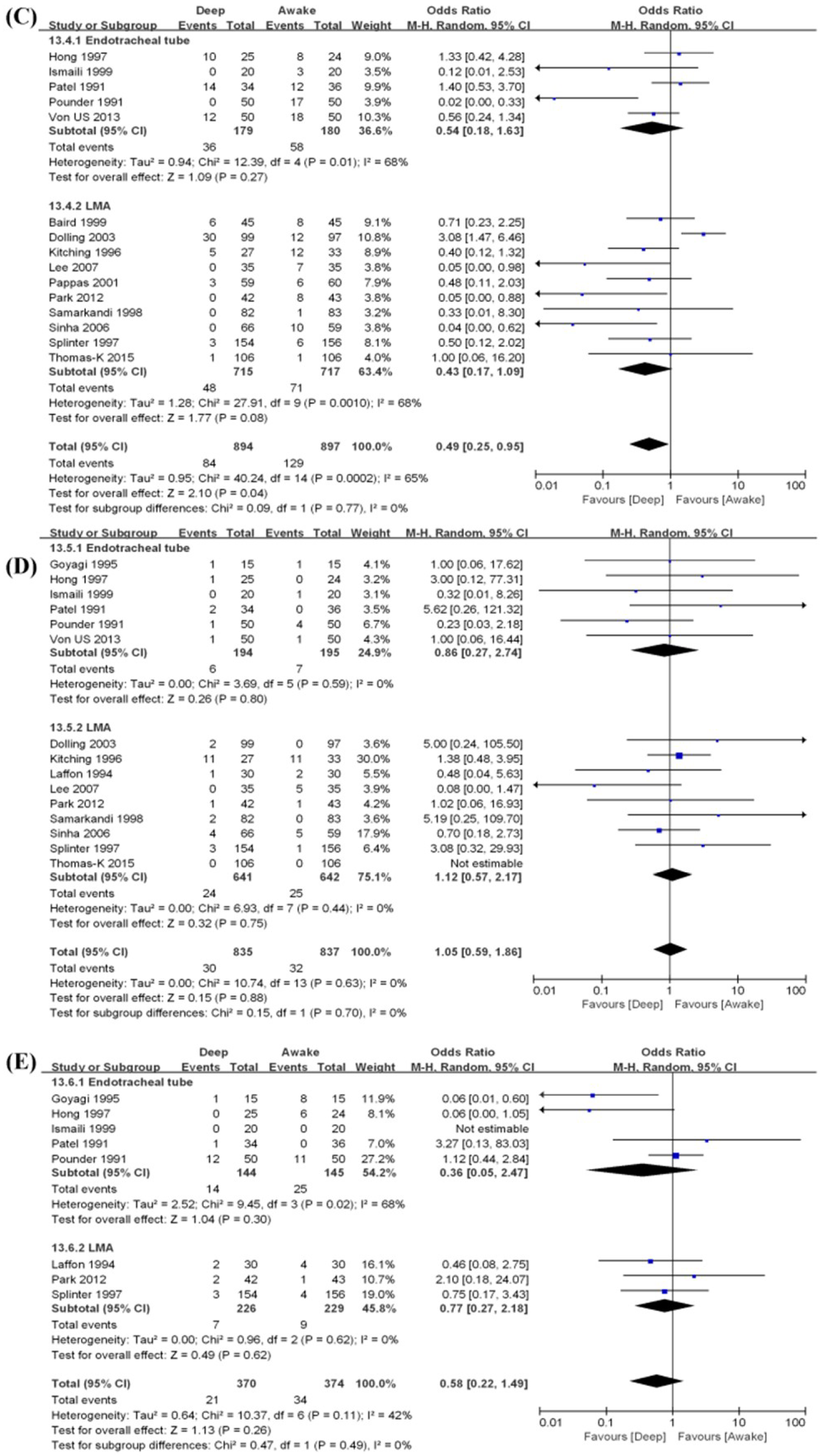
3.4. Subgroup Analysis
Endotracheal Tube vs. Laryngeal Mask Airway (LMA)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stone, D.J.; Gal, T.J. Airway management. In Miller’s Anesthesia, 4th ed.; Churchill Livingstone: New York, NY, USA, 1994; pp. 1403–1436. [Google Scholar]
- Von Ungern-Sternberg, B.S.; Boda, K.; Chambers, N.A.; Rebmann, C.; Johnson, C.; Sly, P.D.; Habre, W. Risk Assessment for Respiratory Complications in Paediatric Anaesthesia: A Prospective Cohort Study. Lancet 2010, 376, 773–783. [Google Scholar] [CrossRef]
- Mc Donnell, C. Interventions guided by analysis of quality indicators decrease the frequency of laryngospasm during pediatric anesthesia. Paediatr. Anaesth. 2013, 23, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Orestes, M.I.; Lander, L.; Verghese, S.; Shah, R.K. Incidence of laryngospasm and bronchospasm in pediatric adenotonsillectomy. Laryngoscope 2012, 122, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Kanaya, A.; Kuratani, N.; Nakata, Y.; Yamauchi, M. Factors affecting extubation time following pediatric ambulatory surgery: An analysis using electronic anesthesia records from an academic university hospital. JA Clin. Rep. 2017, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Brain, A.I.J. The Intavent Laryngeal Mask: Instruction Manual, 2nd ed; Brain Medical Limited: Henley-on-Thames, England, UK, 1993. [Google Scholar]
- Dolling, S.; Anders, N.R.; Rolfe, S.E. A comparison of deep vs. awake removal of the laryngeal mask airway in paediatric dental daycase surgery. A randomised controlled trial. Anaesthesia 2003, 58, 1224–1228. [Google Scholar] [PubMed]
- Nunez, J.; Nunez, J.; Hughes, J.; Wareham, K.; Asai, T. Timing of removal of the laryngeal mask airway. Anaesthesia 1998, 53, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitching, A.J.; Walpole, A.R.; Blogg, C.E. Removal of the laryngeal mask airway in children: Anaesthetized compared with awake. Br. J. Anaesth. 1996, 76, 874–876. [Google Scholar] [CrossRef] [PubMed]
- Varughese, A.; McCulloch, D.; Lewis, M.; Stokes, M. Removal of laryngeal mask airway (LMA) in children: Awake or deep? Anesthesiology 1994, 81. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.I.; Hannallah, R.S.; Norden, J.; Casey, W.F.; Verghese, S.T. Emergence airway complications in children: A comparison of tracheal extubation in awake and deeply anesthetized patients. Anesth. Analg. 1991, 73, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Pounder, D.R.; Blackstock, D.; Steward, D.J. Tracheal extubation in children: Halothane versus isoflurane, anesthetized versus awake. Anesthesiology 1991, 74, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Laffon, M.; Plaud, B.; Dubousset, A.M.; Ben Haj’Hmida, R.; Ecoffey, C. Removal of laryngeal mask airway: Airway complications in children, anaesthetized versus awake. Paediatr. Anesth. 1994, 4, 35–37. [Google Scholar] [CrossRef]
- Goyagi, T.; Kihara, S.; Harukuni, I.; Sato, S. Comparison of airway complications on tracheal extubation in deeply sevoflurane anesthetized versus awake children. Masui 1995, 44, 1242–1245. [Google Scholar] [PubMed]
- Hong, J.Y.; Han, S.J.; Kil, H.K.; Kim, W.O. Airway—Related Complications and SpO2 Changes of Deeply Anesthetized Versus Awake Extubation in Children. Korean J. Anesthesiol. 1997, 32, 384–389. [Google Scholar] [CrossRef]
- Splinter, W.M.; Reid, C.W. Removal of the laryngeal mask airway in children: Deep anesthesia versus awake. J. Clin. Anesth. 1997, 9, 4–7. [Google Scholar] [CrossRef]
- Samarkandi, A. Awake removal of the laryngeal mask airway is safe in paediatric patients. Can. J. Anaesth. 1998, 45, 150–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baird, M.; Mayor, A.; Goodwin, A. Removal of the laryngeal mask airway: Factors affecting the incidence of post-operative adverse respiratory events in 300 patients. Eur. J. Anaesthesiol. 1999, 16, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Ismaili, M.H.; Faroudy, M.; Kabbaj, S.; Maazouzi, W. Tracheal extubation of children after ophthalmologic surgery: Halothane vs. oxygen. Cah. Anesthesiol. 1999, 47, 391–393. [Google Scholar]
- Pappas, A.L.; Sukhani, R.; Lurie, J.; Pawlowski, J.; Sawicki, K.; Corsino, A. Severity of airway hyperreactivity associated with laryngeal mask airway removal: Correlation with volatile anesthetic choice and depth of anesthesia. J. Clin. Anesth. 2001, 13, 498–503. [Google Scholar] [CrossRef]
- Sinha, A.; Sood, J. Safe removal of LMA in children–at what BIS? Paediatr. Anaesth. 2006, 16, 1144–1147. [Google Scholar] [PubMed]
- Lee, J.; Kim, J.; Kim, S.; Kim, C.; Yoon, T.; Kim, H. Removal of the laryngeal tube in children: Anaesthetized compared with awake. Br. J. Anaesth. 2007, 98, 802–805. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Kim, K.J.; Oh, J.T.; Choi, E.K.; Lee, J.R. A randomized controlled trial comparing Laryngeal Mask Airway removal during adequate anesthesia and after awakening in children aged 2 to 6 years. J. Clin. Anesth. 2012, 24, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Von Ungern-Sternberg, B.S.; Davies, K.; Hegarty, M.; Erb, T.O.; Habre, W. The effect of deep vs. awake extubation on respiratory complications in high-risk children undergoing adenotonsillectomy: A randomised controlled trial. Eur J. Anaesthesiol. 2013, 30, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Kattappurathu, G.; Kasisomayajula, A.; Short, J. Best position and depth of anaesthesia for laryngeal mask airway removal in children: A randomised controlled trial. Eur. J. Anaesthesiol. 2015, 32, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Peat, J.K.; Gray, E.J.; Mellis, C.M.; Leeder, S.R.; Woolcock, A.J. Differences in airway responsiveness between children and adults living in the same environment: An epidemiological study in two regions of New South Wales. Eur. Respir. J. 1994, 7, 1805–1813. [Google Scholar] [CrossRef] [PubMed]
- Baijal, R.G.; Bidani, S.A.; Minard, C.G.; Watcha, M.F. Perioperative respiratory complications following awake and deep extubation in children undergoing adenotonsillectomy. Paediatr. Anaesth. 2015, 25, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Mathew, P.J.; Mathew, J.L. Early versus late removal of the laryngeal mask airway (LMA) for general anaesthesia. Cochrane Database Syst. Rev. 2015, 8. [Google Scholar] [CrossRef] [PubMed]
- Visvanathan, T.; Kluger, M.T.; Webb, R.K.; Westhorpe, R.N. Crisis management during anaesthesia: Laryngospasm. Qual. Saf. Health Care 2005, 14, e3. [Google Scholar] [CrossRef] [PubMed]
- Olsson, G.L.; Hallen, B. Laryngospasm during anaesthesia. A computer-aided incidence study in 136,929 patients. Acta Anaesthesiol. Scand. 1984, 28, 567–575. [Google Scholar] [PubMed]
- Tsui, B.C.; Wagner, A.; Cave, D.; Elliott, C.; El-Hakim, H.; Malherbe, S. The incidence of laryngospasm with a “no touch” extubation technique after tonsillectomy and adenoidectomy. Anesth. Analg. 2004, 98, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Soliman, I.E.; Patel, R.I.; Ehrenpreis, M.B.; Hannallah, R.S. Recovery scores do not correlate with postoperative hypoxemia in children. Anesth. Analg. 1988, 67, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.L.R.; Vital, R.B.; Lira, C.C.S.; Magro, I.B.; Sato, P.T.S.; Lima, L.H.N.; Braz, L.G.; Modolo, N.S.P. Laryngeal Mask Airway Versus Other Airway Devices for Anesthesia in Children With an Upper Respiratory Tract Infection: A Systematic Review and Meta-analysis of Respiratory Complications. Anesth. Analg. 2018, 127, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Guler, G.; Akin, A.; Tosun, Z.; Eskitascoglu, E.; Mizrak, A.; Boyaci, A. Single-dose dexmedetomidine attenuates airway and circulatory reflexes during extubation. Acta Anaesthesiol. Scand. 2005, 49, 1088–1091. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, R.K.; Rajan, S.; Paul, J.; Kumar, L. Respiratory and hemodynamic outcomes following exchange extubation with laryngeal mask airway as compared to traditional awake extubation. Anesth. Essays Res. 2016, 10, 212–217. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Nomber of Patients (Deep/Awake) | Language | Age (year) | Weight (kg) | Airway Device | Anesthetics | Neuromuscular Blockade | Type of Surgery | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Deep | Awake | Deep | Awake | ||||||||
| Baird | 1999 [20] | 90 (45/45) | English | 7.0 | 7.8 | 26.9 | 28.5 | LMA | Inhalational | No | Not mentioned |
| Dolling | 2003 [7] | 196 (99/97) | English | 5 | 5 | 22 | 21 | LMA | Inhalational | No | Dental surgery |
| Goyagi | 1995 [16] | 30 (15/15) | Japanese | 5.2 | 5.6 | 21.7 | 22.1 | ETT | Inhalational | No | T/A, ventilation tube, or herniotomy |
| Hong | 1997 [17] | 49 (25/24) | Korean | 6.4 | 5.8 | 22.4 | 20.8 | ETT | Inhalational | pancuronium | T/A |
| Ismaili | 1999 [21] | 40 (20/20) | French | 5.9 | 5.7 | 22.1 | 22.6 | ETT | Inhalational | No or vecuronium | Ophthalmic surgery |
| Kitching | 1996 [9] | 60 (27/33) | English | Not mentioned | Not mentioned | LMA | Inhalational | No | Urogenital or lower limb plastic surgery | ||
| Laffon | 1994 [15] | 60 (30/30) | English | 0.5 | 0.5 | 18 | 19 | LMA | Inhalational | No | Minor urologic or lower abdominal surgery |
| Lee | 2007 [24] | 70 (35/35) | English | 4 | 3 | 16.8 | 17.8 | LMA | Inhalational | No | Urologic, orthopedic or plastic surgery |
| Pappas | 2001 [22] | 119 (59/60) | English | 3.3 | 2.9 | 21.5 | 15 | LMA | Inhalational | No | Infra-umbilical surgery |
| Park | 2012 [25] | 85 (42/43) | English | 4.2 | 3.9 | 16.2 | 15.9 | LMA | Inhalational | No | Inguinal hernia repair or hydrocelectomy |
| Patel | 1991 [13] | 70 (34/36) | English | 4.7 | 4.0 | 18.4 | 17.0 | ETT | Inhalational | succinylcholine | Strabismus or T/A |
| Pounder | 1991 [14] | 100 (50/50) | English | 2.4 | 2.2 | 13.5 | 13 | ETT | Inhalational | succinylcholine | Minor urologic or abdominal herniotomy |
| Samarkandi | 1998 [19] | 165 (82/83) | English | 3.7 | 3.6 | 15.6 | 15.4 | LMA | Inhalational | No | Lower limb or perineal surgery |
| Sinha | 2006 [23] | 125 (66/59) | English | 2.6 | 2.7 | 10.6 | 11.0 | LMA | Inhalational | No | Herniotomy, orchiopexy, or lower limb plastic surgery |
| Splinter | 1997 [18] | 310 (154/156) | English | 6.1 | 6.9 | 24 | 28 | LMA | Inhalational | No | Not mentioned |
| Thomas-K | 2015 [27] | 212 (106/106) | English | 7.7 | 6.8 | Not mentioned (Only BMI) | LMA | Inhalational | No | Pediatric, orthopedic, ophthalmic or plastic surgery | |
| Von US | 2013 [26] | 100 (50/50) | English | 4 | 5 | 18 | 20 | ETT | Inhalational | Yes, but not mentioned which was used | T/A |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koo, C.-H.; Lee, S.Y.; Chung, S.H.; Ryu, J.-H. Deep vs. Awake Extubation and LMA Removal in Terms of Airway Complications in Pediatric Patients Undergoing Anesthesia: A Systemic Review and Meta-Analysis. J. Clin. Med. 2018, 7, 353. https://doi.org/10.3390/jcm7100353
Koo C-H, Lee SY, Chung SH, Ryu J-H. Deep vs. Awake Extubation and LMA Removal in Terms of Airway Complications in Pediatric Patients Undergoing Anesthesia: A Systemic Review and Meta-Analysis. Journal of Clinical Medicine. 2018; 7(10):353. https://doi.org/10.3390/jcm7100353
Chicago/Turabian StyleKoo, Chang-Hoon, Sun Young Lee, Seung Hyun Chung, and Jung-Hee Ryu. 2018. "Deep vs. Awake Extubation and LMA Removal in Terms of Airway Complications in Pediatric Patients Undergoing Anesthesia: A Systemic Review and Meta-Analysis" Journal of Clinical Medicine 7, no. 10: 353. https://doi.org/10.3390/jcm7100353