
Gender Differences in Patients with Gastric Adenocarcinoma
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Pathological Classification
2.3. Clinical Staging
2.4. Statistical Analysis
3. Results
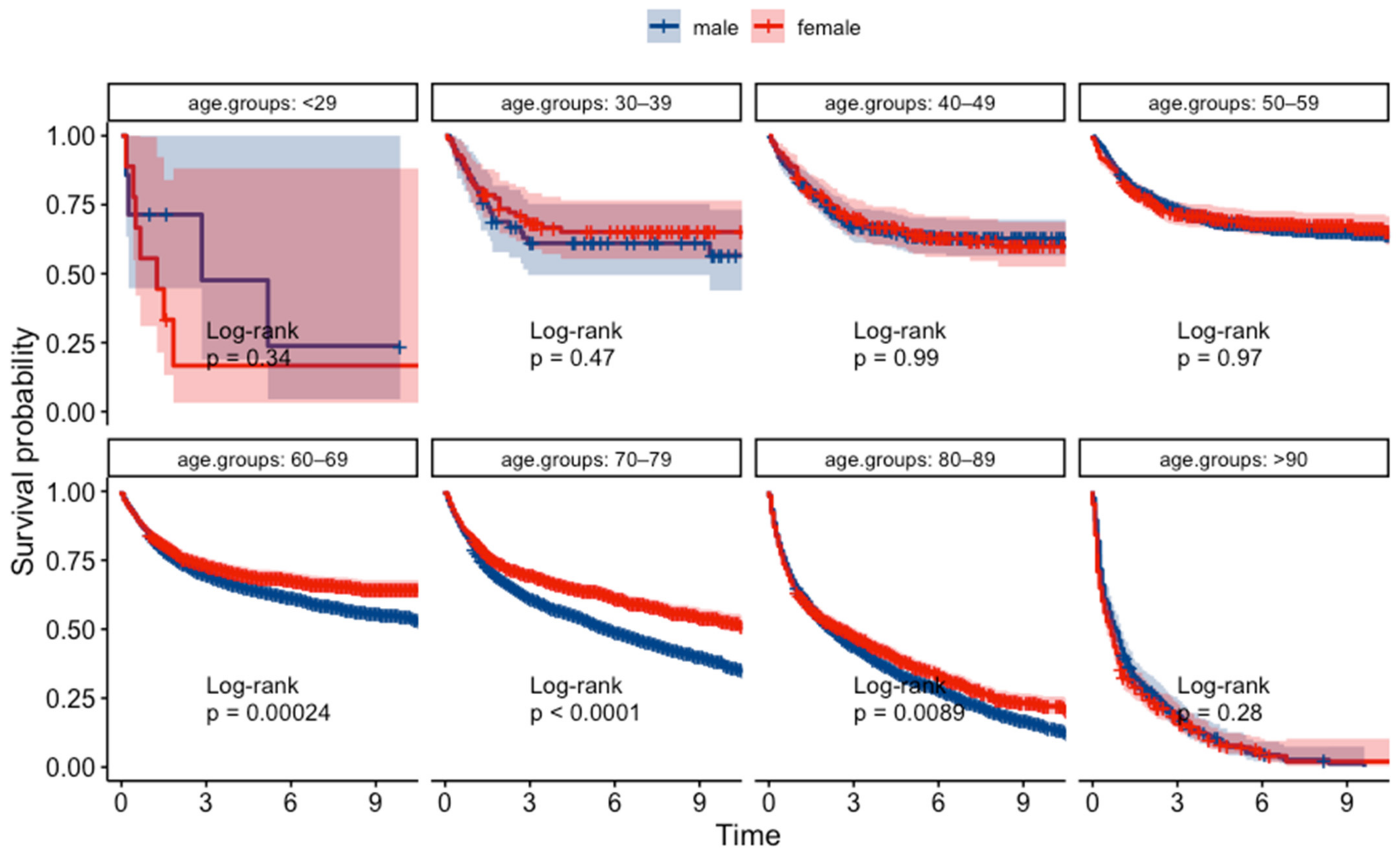
3.1. Gender Differences in Age of Onset
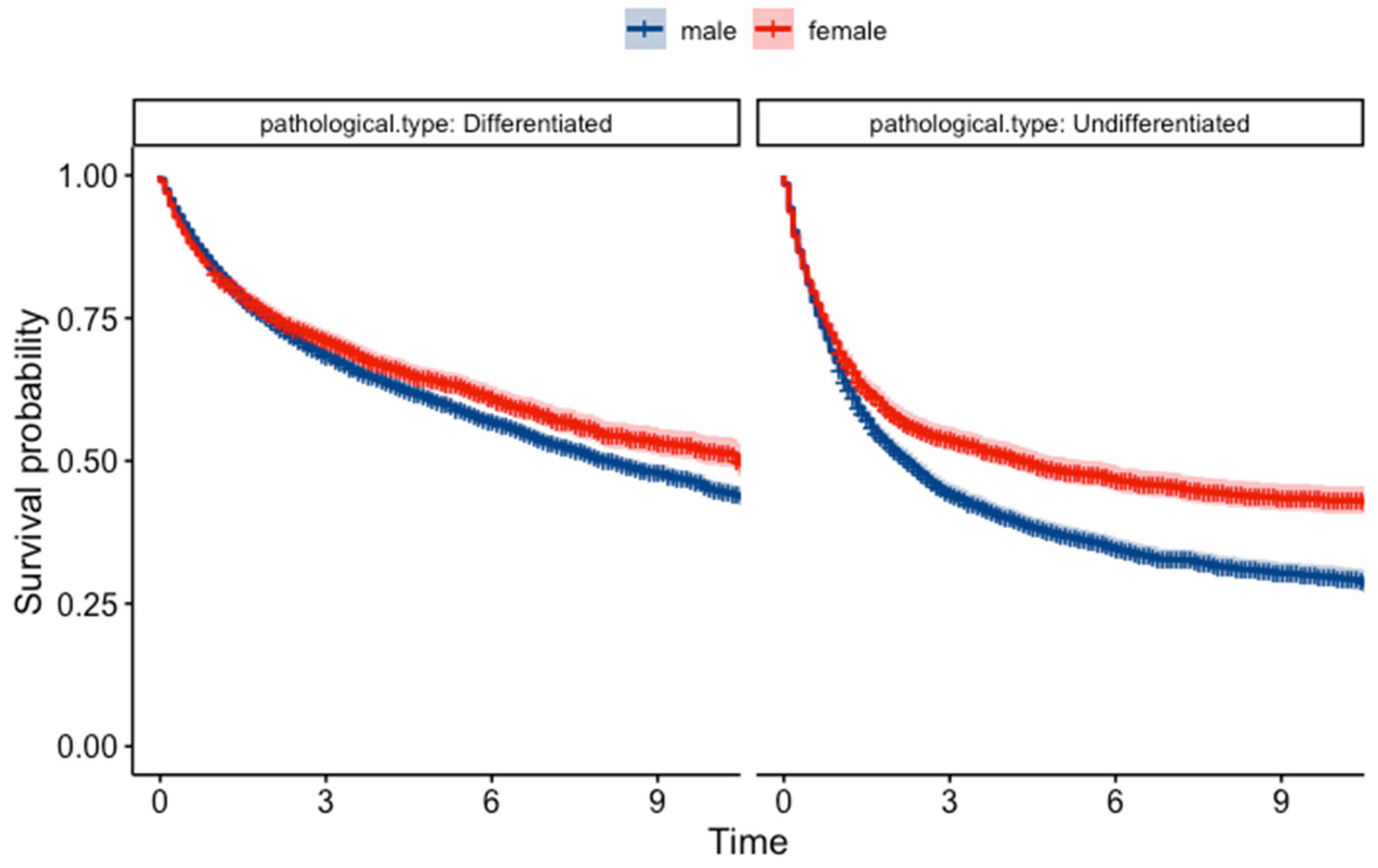
3.2. Gender Differences in Pathological Type
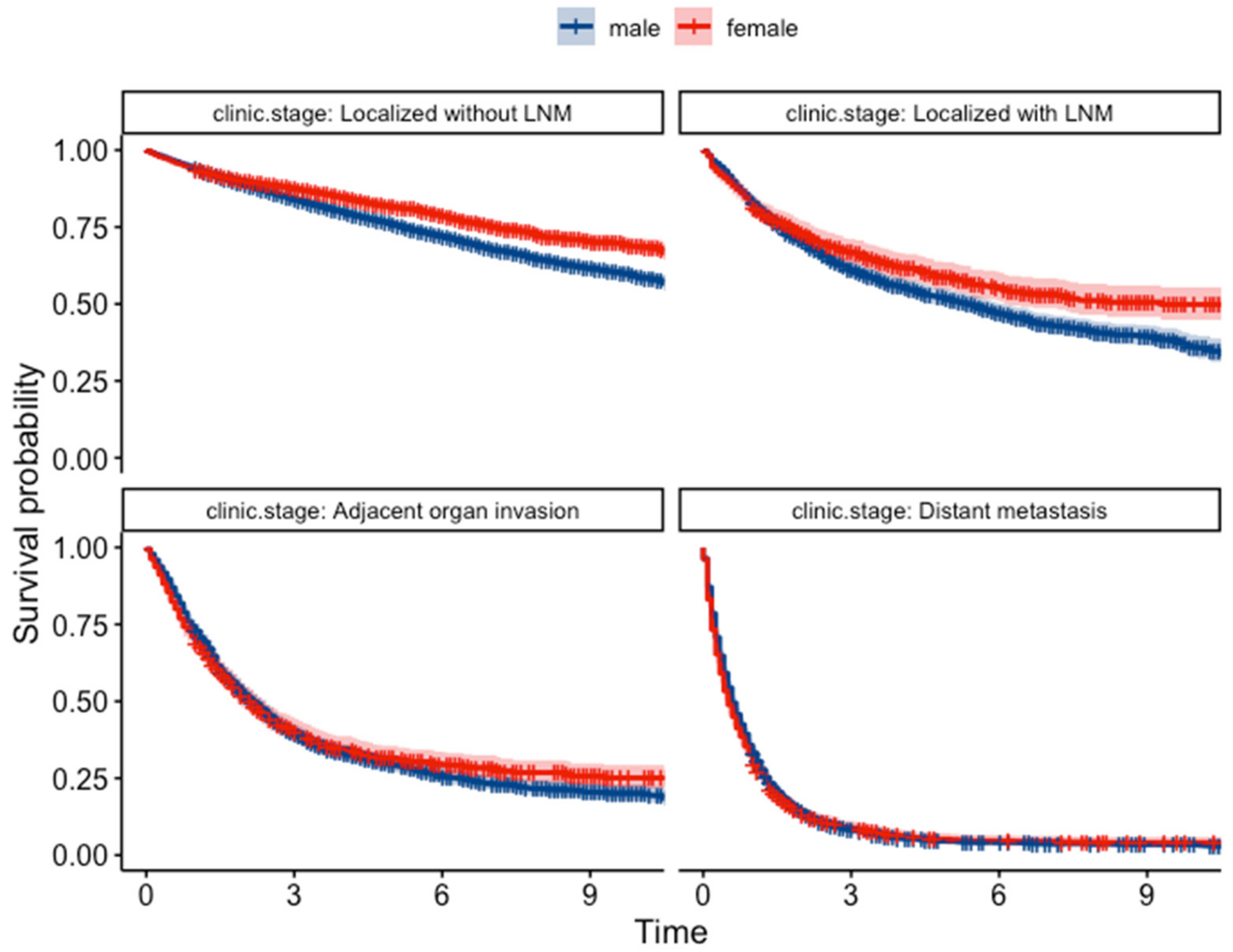
3.3. Gender Differences in Type of Presentation and Clinical Staging
3.4. Gender Difference in Survival Rate
3.5. Prognostic Factors
4. Discussion
Meaning of the Study
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fuchs, C.S.; Mayer, R.J. Gastric Carcinoma. N. Engl. J. Med. 1995, 333, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Center for Cancer Control and Information Services. National Cancer Center Japan. Cancer Registry and Statistics. Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/5_stomach.html (accessed on 14 April 2024).
- Bozzetti, F.; Bonfanti, G.; Morabito, A.; Bufalino, R.; Menotti, V.; Andreola, S.; Doci, R.; Gennari, L. A multifactorial approach for the prognosis of patients with carcinoma of the stomach after curative resection. Surg. Gynecol. Obs. 1986, 162, 229–234. [Google Scholar]
- Korenaga, D.; Haraguchi, M.; Okamura, T.; Baba, H.; Saito, A.; Sugimachi, K. DNA ploidy and tumor invasion in human gastric cancer. Histopathologic differentiation. Arch. Surg. 1989, 124, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Ito, Y.; Ioka, A.; Tanaka, M.; Tsukuma, H. Gender differences in stomach cancer survival in Osaka, Japan: Analyses using relative survival model. Jpn. J. Clin. Oncol. 2009, 39, 690–694. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Chandanos, E.; Lagergren, J. Oestrogen and the enigmatic male predominance of gastric cancer. Eur. J. Cancer 2008, 44, 2397–2403. [Google Scholar] [CrossRef]
- Kim, H.G.; Ghu, H.D.; Yun, S.K.; Ryu, S.Y.; Kim, D.Y. Clinicopathological features of female gastric carcinoma patients with curative resection: Comparison with male patients. Chonnam Med. J. 2012, 48, 86–90. [Google Scholar] [CrossRef]
- Sugano, H.; Nakamura, K.; Kato, Y. Pathological studies of human gastric cancer. Acta Pathol. Jpn. 1982, 32 (Suppl. S2), 329–347. [Google Scholar]
- Luan, X.; Niu, P.; Wang, W.; Zhao, L.; Zhang, X.; Zhao, D.; Chen, Y. Sex Disparity in Patients with Gastric Cancer: A Systematic Review and Meta-Analysis. J. Oncol. 2022, 2022, 1269435. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhao, Q. The Demographic Characteristics of Histological Types of Gastric Cancer with Gender, Age, and Tumor Location. J. Gastrointest. Cancer 2009, 40, 98–100. [Google Scholar] [CrossRef]
- Sipponen, P.; Correa, P. Delayed rise in incidence of gastric cancer in females results in unique sex ratio (M/F) pattern: Etiologic hypothesis. Gastric Cancer 2002, 5, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, H.; Iwanaga, T.; Koyama, H.; Taniguchi, H. Effect of sex hormones on the experimental induction of cancer in rat stomach—A preliminary study. Digestion 1982, 23, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, A.; Kojima, N.; Andoh, T.; Matsukura, N.; Yoshiyasu, M.; Tanaka, N.; Ohkawa, K.; Shirota, A.; Asano, G.; Hayashi, K. Hormone receptors in gastric cancer. Eur. J. Cancer Clin. Oncol. 1983, 19, 687–689. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Chow, W.H.; Gao, Y.T.; Shu, X.O.; Ji, B.T.; Yang, G.; Lubin, J.H.; Li, H.L.; Rothman, N.; Zheng, W.; et al. Menstrual and reproductive factors and gastric cancer risk in a large prospective study of women. Gut 2007, 56, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, M.; Ye, W.; Rubio, C.; Lagergren, J. Estrogen and risk of gastric cancer: A protective effect in a nationwide cohort study of patients with prostate cancer in Sweden. Cancer Epidemiol. Biomark. Prev. 2004, 13, 2203–2207. [Google Scholar] [CrossRef]
- Maguire, A.; Porta, M.; Sanz-Anquela, J.M.; Ruano, I.; Malats, N.; Piñol, J.L. Sex as a prognostic factor in gastric cancer. Eur. J. Cancer 1996, 32a, 1303–1309. [Google Scholar] [CrossRef]
- Hsu, L.W.; Huang, K.H.; Chen, M.H.; Fang, W.L.; Chao, Y.; Lo, S.S.; Li, A.F.; Wu, C.W.; Shyr, Y.M. Genetic alterations in gastric cancer patients according to sex. Aging 2020, 13, 376–388. [Google Scholar] [CrossRef]
- Quaas, A.; Pamuk, A.; Klein, S.; Quantius, J.; Rehkaemper, J.; Barutcu, A.G.; Rueschoff, J.; Zander, T.; Gebauer, F.; Hillmer, A.; et al. Sex-specific prognostic effect of CD66b-positive tumor-infiltrating neutrophils (TANs) in gastric and esophageal adenocarcinoma. Gastric Cancer 2021, 24, 1213–1226. [Google Scholar] [CrossRef]
- Kohlruss, M.; Ott, K.; Grosser, B.; Jesinghaus, M.; Slotta-Huspenina, J.; Novotny, A.; Hapfelmeier, A.; Schmidt, T.; Gaida, M.M.; Weichert, W.; et al. Sexual Difference Matters: Females with High Microsatellite Instability Show Increased Survival after Neoadjuvant Chemotherapy in Gastric Cancer. Cancers 2021, 13, 1048. [Google Scholar] [CrossRef] [PubMed]
- Bando, E.; Kojima, N.; Kawamura, T.; Takahashi, S.; Fukushima, N.; Yonemura, Y. Prognostic value of age and sex in early gastric cancer. Br. J. Surg. 2004, 91, 1197–1201. [Google Scholar] [CrossRef] [PubMed]
- Schafmayer, C.; Jürgens, G.; Jürgens, I.; Klomp, H.J.; Fändrich, F.; Kahlke, V. [Long-term survival of curatively operated gastric cancer: Influence of the gender and splenectomy]. Zentralbl Chir. 2007, 132, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare of Japan. Handbook of Health and Wel-Fare Statistics 2022; Life Expectancy by Sex and Specified Ages, by Year; Ministry of Health, Labour and Welfare of Japan: Tokyo, Japan, 2022. Available online: https://www.mhlw.go.jp/english/database/db-hh/1-2.html (accessed on 6 March 2024).
- Camargo, M.C.; Goto, Y.; Zabaleta, J.; Morgan, D.R.; Correa, P.; Rabkin, C.S. Sex hormones, hormonal interventions, and gastric cancer risk: A meta-analysis. Cancer Epidemiol. Biomark. Prev. 2012, 21, 20–38. [Google Scholar] [CrossRef]
- Wang, Z.; Butler, L.M.; Wu, A.H.; Koh, W.P.; Jin, A.; Wang, R.; Yuan, J.M. Reproductive factors, hormone use and gastric cancer risk: The Singapore Chinese Health Study. Int. J. Cancer 2016, 138, 2837–2845. [Google Scholar] [CrossRef]
- Green, J.; Roddam, A.; Pirie, K.; Kirichek, O.; Reeves, G.; Beral, V. Reproductive factors and risk of oesophageal and gastric cancer in the Million Women Study cohort. Br. J. Cancer 2012, 106, 210–216. [Google Scholar] [CrossRef]
- Kang, S.; Park, M.; Cho, J.Y.; Ahn, S.J.; Yoon, C.; Kim, S.G.; Cho, S.-J. Tumorigenic mechanisms of estrogen and Helicobacter pylori cytotoxin-associated gene A in estrogen receptor α-positive diffuse-type gastric adenocarcinoma. Gastric Cancer 2022, 25, 678–696. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, K.M.; Lee, S.Y.; Jung, J. Estrogen aggravates tumor growth in a diffuse gastric cancer xenograft model. Pathol. Oncol. Res. 2021, 27, 622733. [Google Scholar] [CrossRef]
- Matsui, M.; Kojima, O.; Kawakami, S.; Uehara, Y.; Takahashi, T. The prognosis of patients with gastric cancer possessing sex hormone receptors. Surg. Today 1992, 22, 421–425. [Google Scholar] [CrossRef]
- Al-Marhoon, M.S.; Nunn, S.; Soames, R.W. The association between cagA+ H. pylori infection and distal gastric cancer: A proposed model. Dig. Dis. Sci. 2004, 49, 1116–1122. [Google Scholar] [CrossRef]
- Al-Marhoon, M.S.; Nunn, S.; Soames, R.W. cagA+ Helicobacter pylori induces greater levels of prostaglandin E2 than cagA−strains. Prostaglandins Other Lipid Mediat. 2004, 73, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Seoane, A.; Bessa, X.; Balleste, B.; O’Callaghan, E.; Panadès, A.; Alameda, F.; Navarro, S.; Gallén, M.; Andreu, M.; Bory, F. Helicobacter pylori and gastric cancer: Relationship with histological subtype and tumor location. Gastroenterol. Y Hepatol. 2005, 28, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Gong, E.J.; Lee, J.Y.; Bae, S.E.; Park, Y.S.; Choi, K.D.; Song, H.J.; Lee, G.H.; Jung, H.-Y.; Jeong, W.J.; Cheon, G.J. Characteristics of non-cardia gastric cancer with a high serum anti-Helicobacter pylori IgG titer and its association with diffuse-type histology. PLoS ONE 2018, 13, e0195264. [Google Scholar] [CrossRef] [PubMed]
- Gunma Prefecture General Affairs Department Statistics Division. Gunma Prefecture Statistical Information Provision System. Available online: https://toukei.pref.gunma.jp/nbj/ (accessed on 14 April 2024).
- Statistics Bureau of Japan. Population Estimates(as of 1 October 2022).Nationwide: Population by Age (Each Age) and Gender. Available online: https://www.stat.go.jp/data/jinsui/2022np/index.html (accessed on 14 April 2024).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | p-Value | |
|---|---|---|---|
| The number of the patients | 13,093 (71) | 5343 (29) | |
| Age (years) | 71.8 (±10.1) | 72.6 (±12.5) | <0.001 |
| Tumor location | <0.001 | ||
| Cardia | 1359 (10.4) | 374 (7) | |
| Fundus | 586 (4.5) | 190 (3.6) | |
| Body | 5803 (44.3) | 2362 (44.2) | |
| Antrum | 4171 (31.9) | 1962 (36.7) | |
| Unknown | 1174 (9) | 455 (8.5) | |
| Type of presentation | <0.001 | ||
| Health checkup | 3929 (30) | 1409 (26.4) | |
| Accidental discovery | 3114 (23.8) | 1199 (22.4) | |
| Others | 1620 (12.4) | 735 (13.7) | |
| Unknown | 4430 (33.8) | 2000 (37.4) | |
| Pathology classification | <0.001 | ||
| Differentiated | 8681 (66.3) | 2802 (52.4) | |
| Undifferentiated | 3449 (26.3) | 2113 (39.5) | |
| Unknown | 963 (7.4) | 428 (8) | |
| Clinical Stage | <0.001 | ||
| Localized without LNM | 7151 (54.6) | 2827 (52.9) | |
| Localized with LNM | 1389 (10.6) | 531 (9.9) | |
| Adjacent organ invasion | 1342 (10.2) | 671 (12.6) | |
| Distant metastasis | 2273 (17.4) | 903 (16.9) | |
| Unknown | 938 (7.2) | 411 (7.7) |
| 5-Year OS (95% CI) | MST (Months) (95% CI) | p-Value | ||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Log-Rank | Generalized Wilcoxon | |
| Overall | 52.6 (51.7–53.5) | 55.3 (53.9–56.7) | 69 (65.2–72.8) | 86 (76.4–95.6) | 0.0018 | 0.756 |
| Pathology Classification | ||||||
| Differentiated | 60.7 (59.6–61.9) | 64.2 (62.3–66.2) | 97 (91.6–102.4) | 126 (114.1–137.9) | 0.0025 | 0.097 |
| Undifferentiated | 37.3 (35.6–39.1) | 48.5 (46.3–50.7) | 27 (24.6–29.3) | 53 (40.6–65.4) | <0.001 | <0.001 |
| Clinical Stage | ||||||
| Localized without LNM | 76.3 (75.2–77.4) | 81.7 (80.2–83.3) | 142 (–) | – | <0.001 | <0.001 |
| Localized with LNM | 51.81 (49.0–54.8) | 58.88 (54.6–63.6) | 65 (56.6–73.4) | 111 (78.5–143.5) | 0.0026 | 0.084 |
| Adjacent organ invasion | 29.68 (27.2–32.4) | 31.6 (28.1–35.6) | 26 (23.8–28.2) | 25 (22.0–27.9) | 0.55 | 0.433 |
| Distant metastasis | 4.45 (3.59–5.51) | 5.23 (3.85–7.11) | 7 (6.5–7.5) | 6 (5.3–6.7) | 0.179 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xing, Y.; Hosaka, H.; Moki, F.; Tomaru, S.; Itoi, Y.; Sato, K.; Hashimoto, Y.; Tanaka, H.; Kuribayashi, S.; Takeuchi, Y.; et al. Gender Differences in Patients with Gastric Adenocarcinoma. J. Clin. Med. 2024, 13, 2524. https://doi.org/10.3390/jcm13092524
Xing Y, Hosaka H, Moki F, Tomaru S, Itoi Y, Sato K, Hashimoto Y, Tanaka H, Kuribayashi S, Takeuchi Y, et al. Gender Differences in Patients with Gastric Adenocarcinoma. Journal of Clinical Medicine. 2024; 13(9):2524. https://doi.org/10.3390/jcm13092524
Chicago/Turabian StyleXing, Yujin, Hiroko Hosaka, Fumitaka Moki, Shota Tomaru, Yuki Itoi, Keigo Sato, Yu Hashimoto, Hirohito Tanaka, Shiko Kuribayashi, Yoji Takeuchi, and et al. 2024. "Gender Differences in Patients with Gastric Adenocarcinoma" Journal of Clinical Medicine 13, no. 9: 2524. https://doi.org/10.3390/jcm13092524