
An OCT-A Analysis of the Importance of Intermediate Capillary Plexus in Diabetic Retinopathy: A Brief Review

Abstract
:1. Introduction


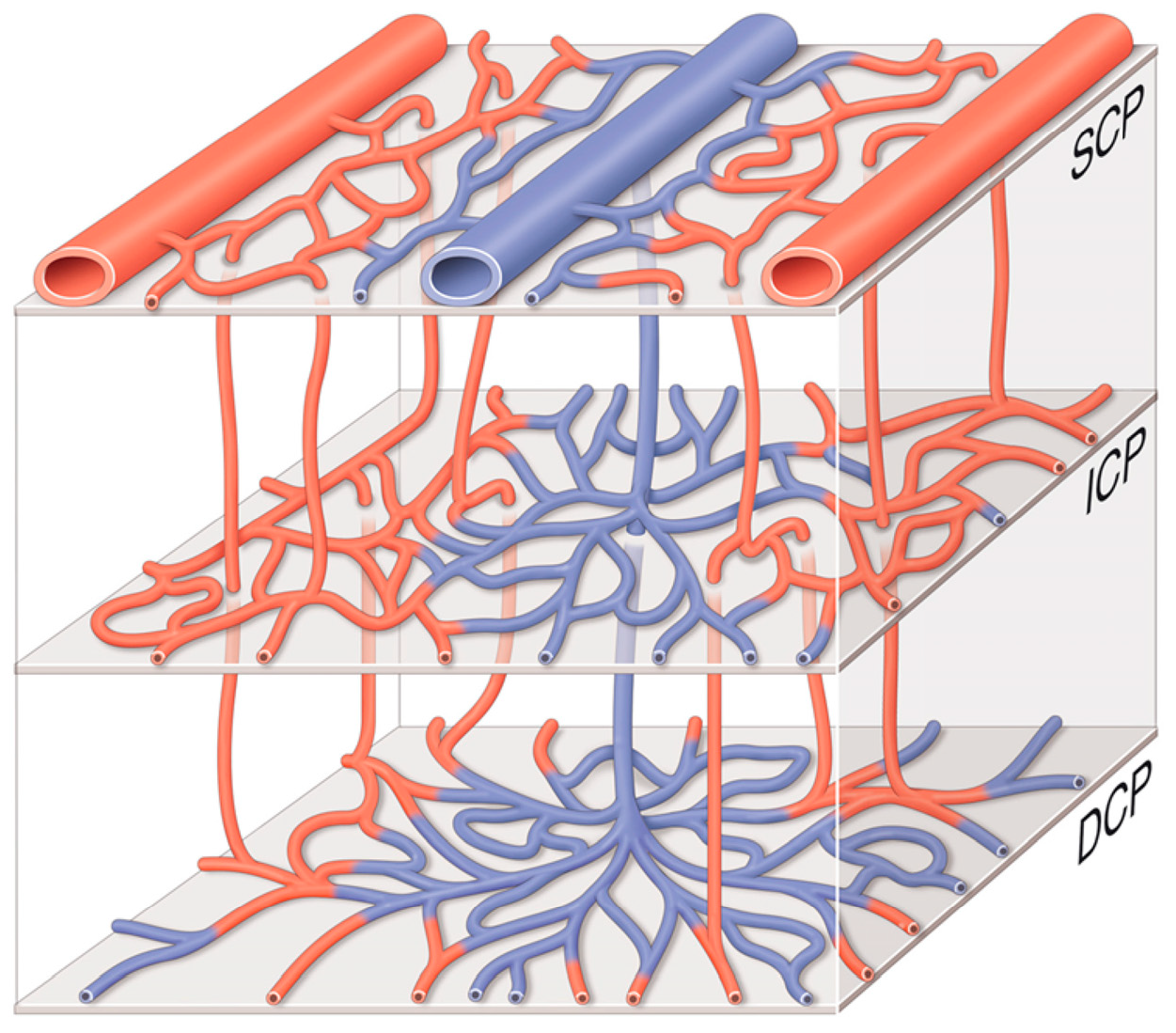
2. The Intermediate Capillary Plexus
3. OCT-A Image of the ICP
4. ICP and Diabetic Retinopathy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Provis, J.M. Development of t he primate retinal vasculature. Prog. Retin. Eye Res. 2001, 20, 799–821. [Google Scholar] [CrossRef]
- Lavia, C.; Mecê, P.; Nassisi, M.; Bonnin, S.; Marie-Louise, J.; Couturier, A.; Erginay, A.; Tadayoni, R.; Gaudric, A. Retinal Capillary Plexus Pattern and Density from Fovea to Periphery Measured in Healthy Eyes with Swept-Source Optical Coherence Tomography Angiography. Sci. Rep. 2020, 10, 1474. [Google Scholar] [CrossRef] [PubMed]
- His, W. Abbildungen über das Gefässystem der Menschliden Ntetzhaut und derjenigen des Kaninchens. Arch F Anat U Entwickelungsg 1880, 5, 224–231. [Google Scholar]
- Flocks, M.; Miller, J.; Chao, P. Retinal Circulation time with the Aid of Fundus Cinephotography. Am. J. Ophthalmol. 1959, 48, 3–6. [Google Scholar] [CrossRef]
- Spaide, R.F.; Klancnik, J.M.; Cooney, M.J. Retinal Vascular Layers Imaged by Fluorescein Angiography and Optical Coherence Tomography Angiography. JAMA Ophthalmol. 2015, 133, 45. [Google Scholar] [CrossRef] [PubMed]
- Weinhaus, R.S.; Burke, J.M.; Delori, F.C.; Snodderly, D.M. Comparison of fluorescein angiography with microvascular anatomy of macaque retinas. Exp. Eye Res. 1995, 61, 1–16. [Google Scholar] [CrossRef]
- Campbell, J.P.; Zhang, M.; Hwang, T.S.; Bailey, S.T.; Wilson, D.J.; Jia, Y.; Huang, D. Detailed Vascular Anatomy of the Human Retina by Projection-Resolved Optical Coherence Tomography Angiography. Sci. Rep. 2017, 7, 42201. [Google Scholar] [CrossRef]
- Couturier, A.; Mané, V.; Bonnin, S.; Erginay, A.; Massin, P.; Gaudric, A.; Tadayoni, R. Capillary plexus anomalies in diabetic retinopathy on optical coherence tomography angiography. Retina 2015, 35, 2384–2391. [Google Scholar] [CrossRef]
- Garrity, S.T.; Paques, M.; Gaudric, A.; Freund, K.B.; Sarraf, D. Considerations in the Understanding of Venous Outflow in the Retinal Capillary Plexus. Retina 2017, 37, 1809–1812. [Google Scholar] [CrossRef]
- Antonetti, D.A.; Klein, R.; Gardner, T.W. Diabetic Retinopathy. N. Engl. J. Med. 2012, 366, 1227–1239. [Google Scholar] [CrossRef]
- Khan, A.; Petropoulos, I.N.; Ponirakis, G.; Malik, R.A. Visual complications in diabetes mellitus: Beyond retinopathy. Diabet Med. 2017, 34, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Jampol, L.M.; Glassman, A.R.; Sun, J. Evaluation and Care of Patients with Diabetic Retinopathy. N. Engl. J. Med. 2020, 382, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef]
- Ashraf, M.; Sampani, K.; Clermont, A.; Abu-Qamar, O.; Rhee, J.; Silva, P.S.; Aiello, L.P.; Sun, J.K. Vascular Density of Deep, Intermediate and Superficial Vascular Plexuses Are Differentially Affected by Diabetic Retinopathy Severity. Investig. Ophthalmol. Vis. Sci. 2020, 61, 53. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Tang, F.; Wong, R.; Lok, J.; Szeto, S.K.H.; Chan, J.C.K.; Tham, C.C.; Ng, D.S.; Cheung, C.Y. OCT Angiography Metrics Predict Progression of Diabetic Retinopathy and Development of Diabetic Macular Edema. Ophthalmology 2019, 126, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Moult, E.M.; Zangwill, L.M.; Weinreb, R.N.; Fujimoto, J.G. Geometric Perfusion Deficits: A Novel OCT Angiography Biomarker for Diabetic Retinopathy Based on Oxygen Diffusion. Am. J. Ophthalmol. 2021, 222, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Nesper, P.L.; Ong, J.X.; Fawzi, A.A. Deep Capillary Geometric Perfusion Deficits on OCT Angiography Detect Clinically Referable Eyes with Diabetic Retinopathy. Ophthalmol. Retin. 2022, 6, 1194–1205. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.C.; Nesper, P.L.; Roberts, P.K.; Moharram, G.A.; Chai, H.; Liu, L.; Jampol, L.M.; Fawzi, A.A. Importance of Considering the Middle Capillary Plexus on OCT Angiography in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2167. [Google Scholar] [CrossRef]
- Midena, E.; Torresin, T.; Longhin, E.; Midena, G.; Pilotto, E.; Frizziero, L. Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk. JCM 2021, 10, 4035. [Google Scholar] [CrossRef]
- Usui, Y.; Westenskow, P.D.; Kurihara, T.; Aguilar, E.; Sakimoto, S.; Paris, L.P.; Wittgrove, C.; Feitelberg, D.; Friedlander, M.S.; Moreno, S.K.; et al. Neurovascular crosstalk between interneurons and capillaries is required for vision. J. Clin. Investig. 2015, 125, 2335–2346. [Google Scholar] [CrossRef]
- Hormel, T.T.; Jia, Y.; Jian, Y.; Hwang, T.S.; Bailey, S.T.; Pennesi, M.E.; Wilson, D.J.; Morrison, J.C.; Huang, D. Plexus-specific retinal vascular anatomy and pathologies as seen by projection-resolved optical coherence tomographic angiography. Prog. Retin. Eye Res. 2021, 80, 100878. [Google Scholar] [CrossRef] [PubMed]
- Pitale, P.M.; Shen, G.; Sigireddi, R.R.; Polo-Prieto, M.; Park, Y.H.; Gibson, S.E.; Westenskow, P.D.; Channa, R.; Frankfort, B.J. Selective vulnerability of the intermediate retinal capillary plexus precedes retinal ganglion cell loss in ocular hypertension. Front. Cell Neurosci. 2022, 16, 1073786. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.S.; Cavallerano, J.D.; Haddad, N.M.N.; Kwak, H.; Dyer, K.H.; Omar, A.F.; Shikari, H.; Sun, J.K.; Aiello, L.P. Peripheral Lesions Identified on Ultrawide Field Imaging Predict Increased Risk of Diabetic Retinopathy Progression over 4 Years. Ophthalmology 2015, 122, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Koustenis, A.; Harris, A.; Gross, J.; Januleviciene, I.; Shah, A.; Siesky, B. Optical coherence tomography angiography: An overview of the technology and an assessment of applications for clinical research. Br. J. Ophthalmol. 2017, 101, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Bailey, S.T.; Hwang, T.S.; McClintic, S.M.; Gao, S.S.; Pennesi, M.E.; Flaxel, C.J.; Lauer, A.K.; Wilson, D.J.; Hornegger, J.; et al. Quantitative optical coherence tomography angiography of vascular abnormalities in the living human eye. Proc. Natl. Acad. Sci. USA 2015, 112, E2395–E2402. [Google Scholar] [CrossRef] [PubMed]
- Tokayer, J.; Jia, Y.; Dhalla, A.H.; Huang, D. Blood flow velocity quantification using split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Biomed. Opt. Express 2013, 4, 1909–1924. [Google Scholar] [CrossRef] [PubMed]
- Garrity, S.T.; Iafe, N.A.; Phasukkijwatana, N.; Chen, X.; Sarraf, D. Quantitative Analysis of Three Distinct Retinal Capillary Plexuses in Healthy Eyes Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis Sci. 2017, 58, 5548–5555. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Hormel, T.T.; Wang, J.; Guo, Y.; Bailey, S.T.; Hwang, T.S.; Jia, Y. An Open-Source Deep Learning Network for Reconstruction of High-Resolution OCT Angiograms of Retinal Intermediate and Deep Capillary Plexuses. Trans. Vis. Sci. Tech. 2021, 10, 13. [Google Scholar] [CrossRef]
- Dadkhah, A.; Jiao, S. Integrating photoacoustic microscopy, optical coherence tomography, OCT angiography, and fluorescence microscopy for multimodal imaging. Exp. Biol. Med. 2020, 245, 342–347. [Google Scholar] [CrossRef]
- Tucker-Schwartz, J.M.; Lapierre-Landry, M.; Patil, C.A.; Skala, M.C. Photothermal optical lock-in optical coherence tomography for in vivo imaging. Biomed. Opt. Express 2015, 6, 2268–2282. [Google Scholar] [CrossRef]
- Moore, J.; Bagley, S.; Ireland, G.; McLeod, D.; Boulton, M.E. Three dimensional analysis of microaneurysms in the human diabetic retina. J. Anat. 1999, 194 Pt 1, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Waheed, N.K.; Moult, E.M.; Adhi, M.; Lee, B.; De Carlo, T.; Jayaraman, V.; Baumal, C.R.; Duker, J.S.; Fujimoto, J.G. Ultrahigh speed swept source optical coherence tomography angiography of retinal and choriocapillaris alterations in diabetic patients with and without retinopathy. Retina 2017, 37, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Hwang, T.S.; Dongye, C.; Wilson, D.J.; Huang, D.; Jia, Y. Automated Quantification of Nonperfusion in Three Retinal Plexuses Using Projection-Resolved Optical Coherence Tomography Angiography in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5101–5106. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.X.; Fawzi, A.A. Perspectives on diabetic retinopathy from advanced retinal vascular imaging. Eye 2022, 36, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Garhöfer, G.; Chua, J.; Tan, B.; Wong, D.; Schmidl, D.; Schmetterer, L. Retinal Neurovascular Coupling in Diabetes. J. Clin. Med. 2020, 9, 2829. [Google Scholar] [CrossRef] [PubMed]
- You, Q.S.; Wang, J.; Guo, Y.; Pi, S.; Flaxel, C.J.; Bailey, S.T.; Huang, D.; Jia, Y.; Hwang, T.S. Optical Coherence Tomography Angiography Avascular Area Association with 1-Year Treatment Requirement and Disease Progression in Diabetic Retinopathy. Am. J. Ophthalmol. 2020, 217, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Luu, C.D.; Szental, J.A.; Lee, S.Y.; Lavanya, R.; Wong, T.Y. Correlation between Retinal Oscillatory Potentials and Retinal Vascular Caliber in Type 2 Diabetes. Investig. Ophthalmol. Vis. Sci. 2010, 51, 482. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Palmieri, M.; Viggiano, P.; Ferro, G.; Mastropasqua, R. Photoreceptor damage in diabetic choroidopathy. Retina 2020, 40, 1062–1069. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Neuroretinal Anatomic Layers | Vascular Nomenclature Correspondence | |
|---|---|---|
| NFL | RPCP | SVC |
| GCL | SCP | |
| IPL | ||
| ICP | DVC | |
| INL | ||
| OPL | ||
| DCP | ||
| ONL | ||
| Avascular Layers | ||
| PR | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haddad, C.; Baleine, M.; Motulsky, E. An OCT-A Analysis of the Importance of Intermediate Capillary Plexus in Diabetic Retinopathy: A Brief Review. J. Clin. Med. 2024, 13, 2516. https://doi.org/10.3390/jcm13092516
Haddad C, Baleine M, Motulsky E. An OCT-A Analysis of the Importance of Intermediate Capillary Plexus in Diabetic Retinopathy: A Brief Review. Journal of Clinical Medicine. 2024; 13(9):2516. https://doi.org/10.3390/jcm13092516
Chicago/Turabian StyleHaddad, Charbel, Manon Baleine, and Elie Motulsky. 2024. "An OCT-A Analysis of the Importance of Intermediate Capillary Plexus in Diabetic Retinopathy: A Brief Review" Journal of Clinical Medicine 13, no. 9: 2516. https://doi.org/10.3390/jcm13092516