

The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience


Abstract
:1. Introduction
2. Methodology
2.1. Patients
2.2. Ethical Aspects
2.3. Outcomes of the Study
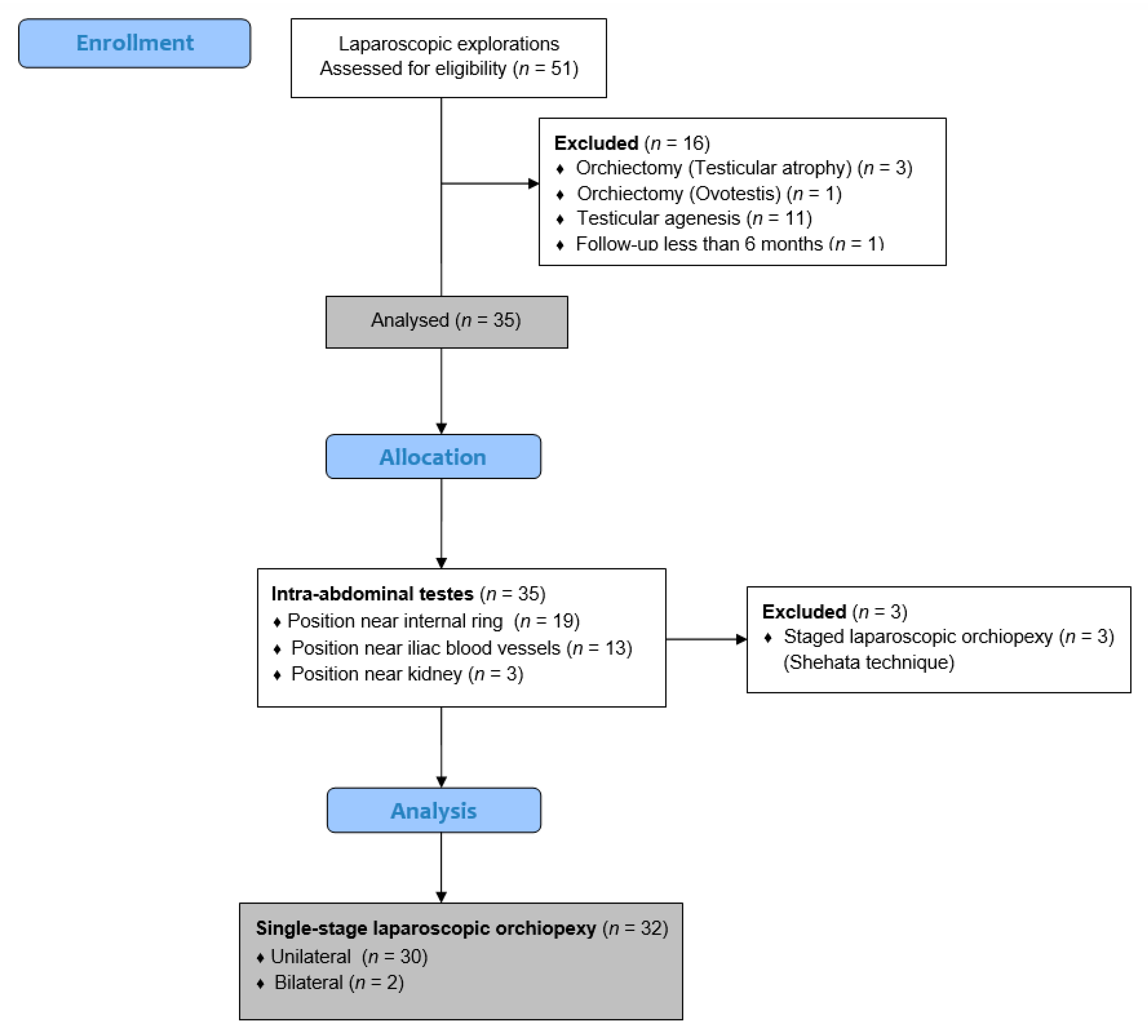
2.4. Study Design
2.5. Surgical Technique
2.6. Postoperative Protocol and Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Clinical Data of the Patients with Intra-Abdominal Cryptorchid Testes
3.2. Intraoperative Findings and Clinical Outcomes of the Intra-Abdominal Testes
3.3. Comparison of Testicular Volume before and Six Months after Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodprasert, W.; Virtanen, H.E.; Mäkelä, J.-A.; Toppari, J. Hypogonadism and cryptorchidism. Front. Endocrinol. 2020, 10, 906. [Google Scholar] [CrossRef] [PubMed]
- Morizawa, Y.; Aoki, K.; Fukui, S.; Tomizawa, M.; Shimizu, T.; Onishi, K.; Hori, S.; Gotoh, D.; Nakai, Y.; Miyake, M.; et al. Assessment of diagnostic accuracy for cryptorchidism and risk factors for delayed orchidopexy. Int. J. Urol. 2023, 31, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Neumann, C.; Jukic, M. An unusual presentation of testicular torsion in children: A single-centre retrospective study. Can. J. Urol. 2019, 26, 10026–10032. [Google Scholar] [PubMed]
- Pogorelić, Z.; Jurić, I.; Biočić, M.; Furlan, D.; Budimir, D.; Todorić, J.; Milunović, K.P. Management of testicular rupture after blunt trauma in children. Pediatr. Surg. Int. 2011, 27, 885–889. [Google Scholar] [CrossRef]
- Elder, J.S. Surgical management of the undescended testis: Recent advances and controversies. Eur. J. Pediatr. Surg. 2016, 26, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Thorup, J.; Hildorf, S.; Hildorf, A.E.; Baastrup, J.M.; Mamsen, L.S.; Andersen, C.Y.; Olsen, T.E.; Cortes, D. The fate of germ cells in cryptorchid testis. Front. Endocrinol. 2024, 14, 1305428. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.; FRCSC for the Canadian Association of Pediatric Surgeon Evidence-Based Resource; Wayne, C.; Nasr, A. Ideal timing of orchiopexy: A systematic review. Pediatr. Surg. Int. 2013, 30, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Gates, R.L.; Shelton, J.; A Diefenbach, K.; Arnold, M.; Peter, S.D.S.; Renaud, E.J.; Slidell, M.B.; Sømme, S.; Valusek, P.; Villalona, G.A.; et al. Management of the undescended testis in children: An American Pediatric Surgical Association outcomes and evidence based practice committee systematic review. J. Pediatr. Surg. 2022, 57, 1293–1308. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Li, G.; Chen, H.; Wang, J.; Li, S. Laparoscopic orchiopexy of palpable undescended testes_ experience of a single tertiary institution with over 773 cases. BMC Pediatr. 2020, 20, 124. [Google Scholar] [CrossRef]
- Anand, S.; Krishnan, N.; Pogorelić, Z. Utility of laparoscopic approach of orchiopexy for palpable cryptorchidism: A systematic review and meta-analysis. Children 2021, 8, 677. [Google Scholar] [CrossRef]
- Shehata, S.; Hadziselimovic, F.; Khater, D.; Kotb, M. The Management of intraabdominal testis: A survey of the World Federation of Associations of Pediatric Surgeons (WOFAPS) Practices. Front. Pediatr. 2022, 10, 928069. [Google Scholar] [CrossRef] [PubMed]
- Al Hindi, S.; Khalaf, Z. The outcome of laparoscopic assisted orchidopexy in very young children: A single hospital experience. J. Pediatr. Urol. 2021, 17, 536.e1–536.e7. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.; McIntosh, J.; Murphy, J.P.; Gatti, J. Laparoscopic orchiopexy for intra-abdominal testes—A single institution review. J. Laparoendosc. Adv. Surg. Tech. 2013, 23, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Papparella, A.; De Rosa, L.; Noviello, C. Laparoscopic Fowler-Stephens orchidopexy for intra-abdominal cryptorchid testis: A single institution experience. Pediatr. Medica Chir. 2021, 42. [Google Scholar] [CrossRef] [PubMed]
- Shehata, S.; Shalaby, R.; Ismail, M.; Abouheba, M.; Elrouby, A. Staged laparoscopic traction-orchiopexy for intraabdominal testis (Shehata technique). J. Pediatr. Surg. 2016, 51, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Zhao, X.; Zhang, C.; Yu, K.; Fang, E.; Zhou, X.; Yuan, J.; Li, N. Compared outcomes of high-level cryptorchidism managed by Fowler-Stephens orchiopexy versus the Shehata technique: A systematic review and meta-analysis. J. Pediatr. Urol. 2023, 19, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Jukić, M.; Biuk, I.; Pogorelić, Z. The incidence and causes of unplanned reoperations as a quality indicator in pediatric surgery. Children 2022, 9, 106. [Google Scholar] [CrossRef] [PubMed]
- Jukić, M.; Antišić, J.; Pogorelić, Z. Incidence and causes of 30-day readmission rate from discharge as an indicator of quality care in pediatric surgery. Acta Chir. Belg. 2023, 123, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Huang, W.J.S.; Chen, K. Measurement of testicular volume in smaller testes: How accurate is the conventional orchidometer? J. Androl. 2009, 30, 685–689. [Google Scholar] [CrossRef] [PubMed]
- E Mau, E.; Leonard, M.P. Practical approach to evaluating testicular status in infants and children. Can. Fam. Physician 2017, 63, 432–435. [Google Scholar]
- Wayne, C.; The Canadian Association of Paediatric Surgeons Evidence-Based Resource; Chan, E.; Nasr, A. What is the ideal surgical approach for intra-abdominal testes? A systematic review. Pediatr. Surg. Int. 2015, 31, 327–338. [Google Scholar] [CrossRef]
- Bawazir, O.A.; Maghrabi, A.M. A comparative study between two techniques of laparoscopic orchiopexy for intra-abdominal testis. Indian J. Urol. 2021, 37, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Vallone, G.; Settimi, A.; Sabin, M.A.G.; Amici, G.; Cusano, T. Laparoscopic orchiopexy without division of the spermatic vessels: Can it be considered the procedure of choice in cases of intraabdominal testis? Surg. Endosc. 2000, 14, 658–660. [Google Scholar] [CrossRef]
- Docimo, S.G. The results of surgical therapy for cryptorchidism: A literature review and analysis. J. Urol. 1995, 154, 1148–1152. [Google Scholar] [CrossRef]
- Jordan, G.H. Editorial: Will laparoscopic orchiopexy replace open surgery for the nonpalpable undescended testis? J. Urol. 1997, 158, 1956. [Google Scholar] [CrossRef] [PubMed]
- Samadi, A.A.; Palmer, L.S.; Franco, I. Laparoscopic orchiopexy: Report of 203 cases with review of diagnosis, operative technique, and lessons learned. J. Endourol. 2003, 17, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.; Docimo, S.; Surer, I.; Peters, C.; Cisek, L.; Diamond, D.; Caldamone, A.; Koyle, M.; Strand, W.; Moore, R.; et al. A multi-institutional analysis of laparoscopic orchidopexy. BJU Int. 2001, 87, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.; Palmer, L.; Franco, I. Laparoscopic orchidopexy: A review of a large clinical series. BJU Int. 2001, 87, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Moursy, E.E.; Gamal, W.; Hussein, M.M. Laparoscopic orchiopexy for non-palpable testes: Outcome of two techniques. J. Pediatr. Urol. 2011, 7, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Alzahem, A. Laparoscopy-assisted orchiopexy versus laparoscopic two-stage fowler stephens orchiopexy for nonpalpable testes: Comparative study. Urol. Ann. 2013, 5, 110–114. [Google Scholar] [CrossRef]
- Todorić, D.; Stanišić, L.; Meštrović, J.; Jurić, I.; Pogorelić, Z.; Milunović, K.P.; Šušnjar, T.; Todorić, J.; Furlan, D.; Budimir, D. Update on management of undescended testes. Pediatr. Croat. 2015, 59 (Suppl. S1), 109–115. [Google Scholar]
- Sato, Y.; Kirihana, Y.; Meguro, S.; Tanji, R.; Onagi, A.; Honda-Takinami, R.; Matsuoka, K.; Hoshi, S.; Hata, J.; Akaihata, H.; et al. Evaluation of testicular stiffness in boys with unilateral cryptorchidism after orchiopexy by ultrasound strain elastography. Fukushima J. Med. Sci. 2024. [Google Scholar] [CrossRef]
- Van Der Plas, E.M.; Zijp, G.W.; Froeling, F.M.; Van Der Voort-Doedens, L.M.; Vries, A.M.-D.; Goede, J.; Hack, W.W. Long-term testicular volume after orchiopexy at diagnosis of acquired undescended testis. J. Urol. 2013, 190, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, M.P.E.; Barceló, F.Y.; Egaña, P.-J.L. The undescended testis in children and adolescents part 2: Evaluation and therapeutic approach. Pediatr. Surg. Int. 2022, 38, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.D.; Acevedo, A.M.; Bayne, A.; Austin, J.; Seideman, C. Factors associated with delay in undescended testis referral. J. Pediatr. Urol. 2019, 15, 380.e1–380.e6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Demographic characteristics | |
| Age (months) | 10 (9, 13) |
| <12 months | 24 (75) |
| 12–24 months | 6 (18.8) |
| 24–36 months | 1 (3.1) |
| 36–48 months | 1 (3.1) |
| >48 months | 0 (0) |
| Height (cm) | 84.5 (81, 86) |
| Weight (kg) | 10 (9, 12) |
| BMI (kg/m2) | 14.9 (13.4, 15.6) |
| Clinical data of patients | |
| Lateralization | |
| Right | 14 (43.8) |
| Left | 16 (50) |
| Bilateral | 2 (6.2) |
| Associated anomalies | 7 (21.9) |
| Cardiac abnormalities | 3 (9.4) |
| Hematological abnormalities | 1 (3.1) |
| Metabolic abnormalities | 1 (3.1) |
| Down syndrome | 2 (6.3) |
| Variables | Values |
|---|---|
| Intraoperative findings | |
| Normal testis | 24 (70.6) |
| Hypotrophic testis | 10 (29.4) |
| Atrophic testis | 0 (0) |
| Intra-abdominal position of the testis | |
| Near the internal ring | 19 (55.9) |
| Near the iliac blood vessels | 15 (44.1) |
| Near the kidney | 0 (0) |
| Duration of surgery (min) | 37.5 (33, 42.5) |
| Length of hospital stay (days) | 1 (1, 1) |
| Complications | |
| Wound infection | 1 (2.8) |
| Testicular atrophy | 2 (5.5) |
| Higher position in the scrotum | 3 (8.3) |
| Follow-up (months) | 35 (19, 60.5) |
| Reoperation | 0 (0) |
| ReAd | 0 (0) |
| uROR | 0 (0) |
| Before Surgery | Six Months after Surgery | p * | |
|---|---|---|---|
| Testicular length (mm) | 13.5 (12, 15) | 14 (11.5, 16) | 0.313 |
| Testicular width (mm) | 7 (7, 8) | 8 (7, 8) | 0.158 |
| Testicular volume (mL) | 0.31 (0.28, 0.43) | 0.40 (0.33, 0.53) | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pogorelić, Z.; Šitum, J.; Barić, T.; Šitum, M. The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience. J. Clin. Med. 2024, 13, 2045. https://doi.org/10.3390/jcm13072045
Pogorelić Z, Šitum J, Barić T, Šitum M. The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience. Journal of Clinical Medicine. 2024; 13(7):2045. https://doi.org/10.3390/jcm13072045
Chicago/Turabian StylePogorelić, Zenon, Josipa Šitum, Tomislav Barić, and Marijan Šitum. 2024. "The Safety and Effectiveness of Single-Stage, Vessel-Preserving, Laparoscopic Orchiopexy for Intra-Abdominal Testes in Pediatric Patients: A 10-Year Single-Center Experience" Journal of Clinical Medicine 13, no. 7: 2045. https://doi.org/10.3390/jcm13072045