
The Functional Implications of Transanal Irrigation: Insights from Pathophysiology and Clinical Studies of Neurogenic Bowel Dysfunction
Abstract
:1. Introduction
2. Neuroanatomy and Physiology of Functional Defecation
2.1. Somatic and Autonomic Nervous Systems and Enteric Nervous System
2.2. Four Phases of Defecation
3. Pathophysiology of Neurogenic Bowel
3.1. Hyper-Reflexic Bowel and Impact on Defecation
3.2. Hyporeflexic Bowel and Impact on Defecation
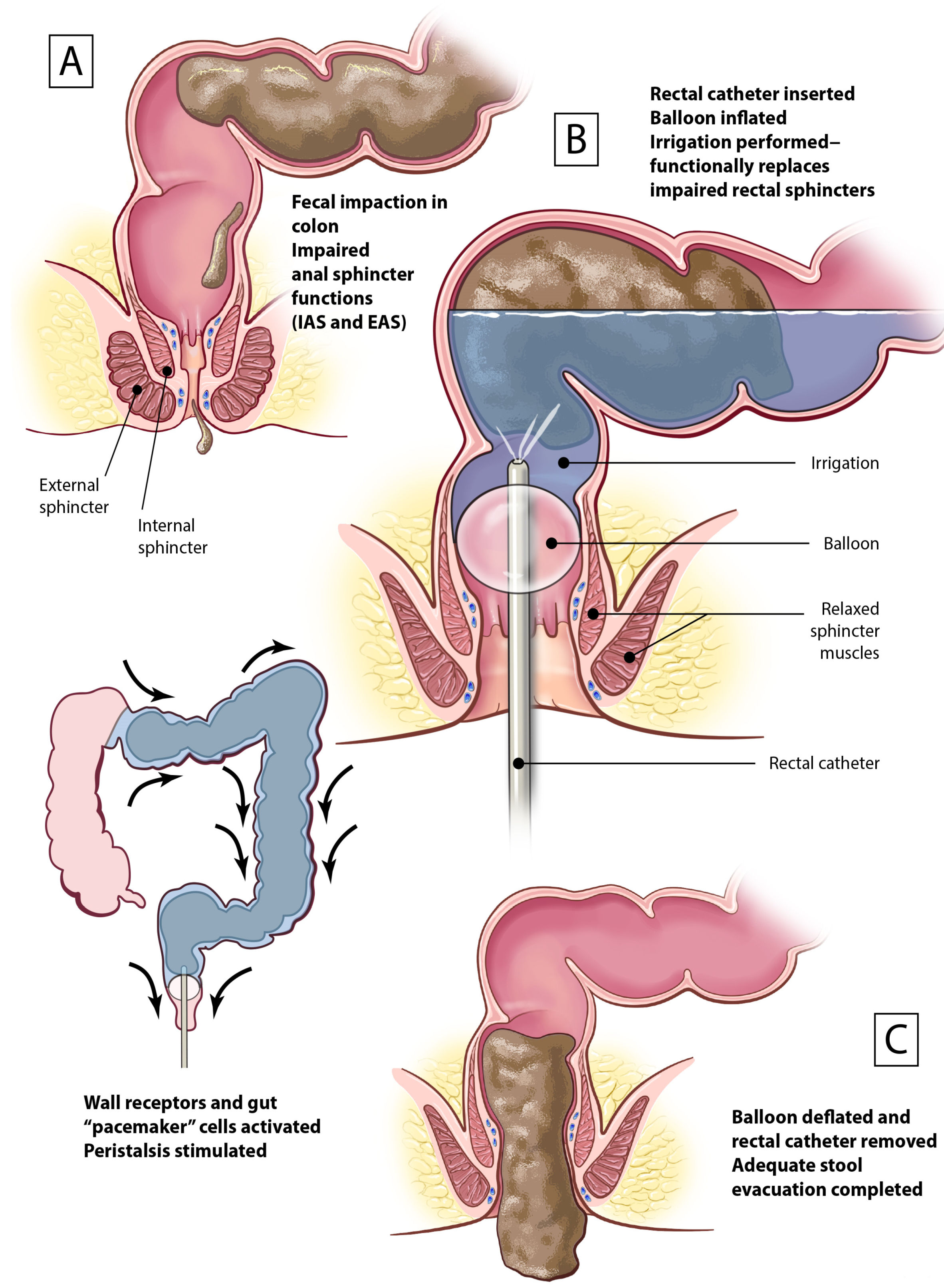
4. The Role of TAI in Managing NBD
Proposed MOA of TAI in Triggering Effective Evacuation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glickman, S.; Kamm, M.A. Bowel dysfunction in spinal-cord-injury patients. Lancet 1996, 347, 1651–1653. [Google Scholar] [CrossRef]
- Krogh, K.; Nielsen, J.; Djurhuus, J.C.; Mosdal, C.; Sabroe, S.; Laurberg, S. Colorectal function in patients with spinal cord lesions. Dis. Colon Rectum 1997, 40, 1233–1239. [Google Scholar] [CrossRef]
- Colachis, S.C., 3rd. Autonomic hyperreflexia with spinal cord injury. J. Am. Paraplegia Soc. 1992, 15, 171–186. [Google Scholar] [CrossRef]
- Emmanuel, A. Managing neurogenic bowel dysfunction. Clin. Rehabil. 2010, 24, 483–488. [Google Scholar] [CrossRef]
- Bloemen-Vrencken, J.H.; Post, M.W.; Hendriks, J.M.; De Reus, E.C.; De Witte, L.P. Health problems of persons with spinal cord injury living in the Netherlands. Disabil. Rehabil. 2005, 27, 1381–1389. [Google Scholar] [CrossRef]
- Middleton, J.W.; Lim, K.; Taylor, L.; Soden, R.; Rutkowski, S. Patterns of morbidity and rehospitalisation following spinal cord injury. Spinal Cord 2004, 42, 359–367. [Google Scholar] [CrossRef]
- Preziosi, G.; Gordon-Dixon, A.; Emmanuel, A. Neurogenic bowel dysfunction in patients with multiple sclerosis: Prevalence, impact, and management strategies. Degener. Neurol. Neuromuscul. Dis. 2018, 8, 79–90. [Google Scholar] [CrossRef]
- Gulick, E.E. Neurogenic Bowel Dysfunction Over the Course of Multiple Sclerosis: A Review. Int. J. MS Care 2022, 24, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Starowicz, J.; Cassidy, C.; Brunton, L. Health Concerns of Adolescents and Adults With Spina Bifida. Front. Neurol. 2021, 12, 745814. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, T.L.; Bowel and Bladder Workshop Participants; de Groat, W.; Eisner, K.; Emmanuel, A.; French, J.; Grill, W.; Kennelly, M.J.; Krassioukov, A.; Santacruz, B.G.; et al. Translating promising strategies for bowel and bladder management in spinal cord injury. Exp. Neurol. 2018, 306, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Beierwaltes, P.S.; Chinarian, J.L.; Munoz, S.; Suson, K.D. Using a Decision Tree to Guide Bowel Management in Spina Bifida. J. Pediatr. Nurs. 2019, 47, 68–72. [Google Scholar] [CrossRef]
- Kurze, I.; Geng, V.; Bothig, R. Guideline for the management of neurogenic bowel dysfunction in spinal cord injury/disease. Spinal Cord 2022, 60, 435–443. [Google Scholar] [CrossRef]
- Rodriguez, G.M.; Gater, D.R. Neurogenic Bowel and Management after Spinal Cord Injury: A Narrative Review. J. Pers. Med. 2022, 12, 1141. [Google Scholar] [CrossRef]
- Magnuson, F.S.; Christensen, P.; Krassioukov, A.; Rodriguez, G.; Emmanuel, A.; Kirshblum, S.; Krogh, K. Neurogenic Bowel Dysfunction in Patients with Spinal Cord Injury and Multiple Sclerosis-An Updated and Simplified Treatment Algorithm. J. Clin. Med. 2023, 12, 6971. [Google Scholar] [CrossRef]
- Johns, J.; Krogh, K.; Rodriguez, G.M.; Eng, J.; Haller, E.; Heinen, M.; Laredo, R.; Longo, W.; Montero-Colon, W.; Korsten, M. Management of Neurogenic Bowel Dysfunction in Adults after Spinal Cord Injury. J. Spinal Cord Med. 2021, 44, 442–510. [Google Scholar] [CrossRef]
- Dietz, N.; Sarpong, K.; Ugiliweneza, B.; Wang, D.; Aslan, S.S.; Castillo, C.; Boakye, M.; Herrity, A.N. Longitudinal Trends and Prevalence of Bowel Management in Individuals With Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 53–67. [Google Scholar] [CrossRef]
- Rupp, R.; Biering-Sorensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey-Md, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Wecht, J.M.; Krassioukov, A.V.; Alexander, M.; Handrakis, J.P.; McKenna, S.L.; Kennelly, M.; Trbovich, M.; Biering-Sorensen, F.; Burns, S.; Elliott, S.L.; et al. International Standards to document Autonomic Function following SCI (ISAFSCI): Second Edition. Top. Spinal Cord Inj. Rehabil. 2021, 27, 23–49. [Google Scholar] [CrossRef] [PubMed]
- Beierwaltes, P.; Church, P.; Gordon, T.; Ambartsumyan, L. Bowel function and care: Guidelines for the care of people with spina bifida. J. Pediatr. Rehabil. Med. 2020, 13, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, A.V.; Krogh, K.; Bazzocchi, G.; Leroi, A.M.; Bremers, A.; Leder, D.; van Kuppevelt, D.; Mosiello, G.; Vogel, M.; Perrouin-Verbe, B.; et al. Consensus review of best practice of transanal irrigation in adults. Spinal Cord 2013, 51, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Page, A.J.; Li, H. Chapter 13—Gastrointestinal mechanosensory function in health and disease. In Mechanobiology in Health and Disease; Verbruggen, S.W., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 377–414. [Google Scholar]
- Huizinga, J.D.; Hussain, A.; Chen, J.H. Interstitial cells of Cajal and human colon motility in health and disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 321, G552–G575. [Google Scholar] [CrossRef]
- Camilleri, M. Gastrointestinal motility disorders in neurologic disease. J. Clin. Investig. 2021, 131, e143771. [Google Scholar] [CrossRef] [PubMed]
- den Braber-Ymker, M.; Lammens, M.; van Putten, M.J.; Nagtegaal, I.D. The enteric nervous system and the musculature of the colon are altered in patients with spina bifida and spinal cord injury. Virchows Arch. 2017, 470, 175–184. [Google Scholar] [CrossRef]
- Hou, S.; Rabchevsky, A.G. Autonomic consequences of spinal cord injury. Compr. Physiol. 2014, 4, 1419–1453. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A.; Sadiq, N.M. Physiology, Gastrointestinal Nervous Control; StatPearls: Treasure Island, FL, USA, 2024. [Google Scholar]
- Christensen, J.; Rick, G.A. Distribution of myelinated nerves in ascending nerves and myenteric plexus of cat colon. Am. J. Anat. 1987, 178, 250–258. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Holmes, E.; Kinross, J.; Burcelin, R.; Gibson, G.; Jia, W.; Pettersson, S. Host-gut microbiota metabolic interactions. Science 2012, 336, 1262–1267. [Google Scholar] [CrossRef]
- Lemann, M.; Flourie, B.; Picon, L.; Coffin, B.; Jian, R.; Rambaud, J.C. Motor activity recorded in the unprepared colon of healthy humans. Gut 1995, 37, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.K.; Park, K.J.; Hennig, G.W. Colonic migrating motor complexes, high amplitude propagating contractions, neural reflexes and the importance of neuronal and mucosal serotonin. J. Neurogastroenterol. Motil. 2014, 20, 423–446. [Google Scholar] [CrossRef]
- Rao, S.S.; Welcher, K. Periodic rectal motor activity: The intrinsic colonic gatekeeper? Am. J. Gastroenterol. 1996, 91, 890–897. [Google Scholar]
- Lin, A.Y.; Du, P.; Dinning, P.G.; Arkwright, J.W.; Kamp, J.P.; Cheng, L.K.; Bissett, I.P.; O’Grady, G. High-resolution anatomic correlation of cyclic motor patterns in the human colon: Evidence of a rectosigmoid brake. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G508–G515. [Google Scholar] [CrossRef]
- Nandhra, G.K.; Mark, E.B.; Di Tanna, G.L.; Haase, A.M.; Poulsen, J.; Christodoulides, S.; Kung, V.; Klinge, M.W.; Knudsen, K.; Borghammer, P.; et al. Normative values for region-specific colonic and gastrointestinal transit times in 111 healthy volunteers using the 3D-Transit electromagnet tracking system: Influence of age, gender, and body mass index. Neurogastroenterol. Motil. 2020, 32, e13734. [Google Scholar] [CrossRef]
- Proano, M.; Camilleri, M.; Phillips, S.F.; Brown, M.L.; Thomforde, G.M. Transit of solids through the human colon: Regional quantification in the unprepared bowel. Am. J. Physiol. 1990, 258, G856–G862. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.M.; Read, N.W.; Prior, A.; Daly, J.A.; Cheah, S.K.; Grundy, D. Sensory and motor responses to rectal distention vary according to rate and pattern of balloon inflation. Gastroenterology 1990, 99, 1008–1015. [Google Scholar] [CrossRef]
- Schuster, M.M.; Hendrix, T.R.; Mendeloff, A.I. The internal anal sphincter response: Manometric studies on its normal physiology, neural pathways, and alteration in bowel disorders. J. Clin. Investig. 1963, 42, 196–207. [Google Scholar] [CrossRef]
- Nullens, S.; Nelsen, T.; Camilleri, M.; Burton, D.; Eckert, D.; Iturrino, J.; Vazquez-Roque, M.; Zinsmeister, A.R. Regional colon transit in patients with dys-synergic defaecation or slow transit in patients with constipation. Gut 2012, 61, 1132–1139. [Google Scholar] [CrossRef]
- Krogh, K.; Mosdal, C.; Gregersen, H.; Laurberg, S. Rectal wall properties in patients with acute and chronic spinal cord lesions. Dis. Colon Rectum 2002, 45, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Lynch, A.C.; Frizelle, F.A. Colorectal motility and defecation after spinal cord injury in humans. Prog. Brain Res. 2006, 152, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Mosiello, G.; Safder, S.; Marshall, D.; Rolle, U.; Benninga, M.A. Neurogenic Bowel Dysfunction in Children and Adolescents. J. Clin. Med. 2021, 10, 1669. [Google Scholar] [CrossRef]
- Krogh, K.; Mosdal, C.; Laurberg, S. Gastrointestinal and segmental colonic transit times in patients with acute and chronic spinal cord lesions. Spinal Cord 2000, 38, 615–621. [Google Scholar] [CrossRef]
- Velde, S.V.; Pratte, L.; Verhelst, H.; Meersschaut, V.; Herregods, N.; Van Winckel, M.; Van Biervliet, S. Colon transit time and anorectal manometry in children and young adults with spina bifida. Int. J. Colorectal Dis. 2013, 28, 1547–1553. [Google Scholar] [CrossRef]
- Jost, W.H.; Schrank, B. Defecatory disorders in de novo Parkinsonians—colonic transit and electromyogram of the external anal sphincter. Wien. Klin. Wochenschr. 1998, 110, 535–537. [Google Scholar] [PubMed]
- Sakakibara, R.; Odaka, T.; Uchiyama, T.; Liu, R.; Asahina, M.; Yamaguchi, K.; Yamaguchi, T.; Yamanishi, T.; Hattori, T. Colonic transit time, sphincter EMG, and rectoanal videomanometry in multiple system atrophy. Mov. Disord. 2004, 19, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, P.T.; Vollebregt, P.F.; Knowles, C.H.; Lunniss, P.J.; Dinning, P.G.; Scott, S.M. Understanding the physiology of human defaecation and disorders of continence and evacuation. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 751–769. [Google Scholar] [CrossRef] [PubMed]
- Lynch, A.C.; Anthony, A.; Dobbs, B.R.; Frizelle, F.A. Anorectal physiology following spinal cord injury. Spinal Cord. 2000, 38, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Lunniss, P.J.; Gladman, M.A.; Hetzer, F.H.; Williams, N.S.; Scott, S.M. Risk factors in acquired faecal incontinence. J. R. Soc. Med. 2004, 97, 111–116. [Google Scholar] [CrossRef]
- Yates, A. Transanal irrigation: Is it the magic intervention for bowel management in individuals with bowel dysfunction? Br. J. Nurs. 2020, 29, 393–398. [Google Scholar] [CrossRef]
- Mekhael, M.; Kristensen, H.O.; Larsen, H.M.; Juul, T.; Emmanuel, A.; Krogh, K.; Christensen, P. Transanal Irrigation for Neurogenic Bowel Disease, Low Anterior Resection Syndrome, Faecal Incontinence and Chronic Constipation: A Systematic Review. J. Clin. Med. 2021, 10, 753. [Google Scholar] [CrossRef]
- Christensen, P.; Krogh, K. Transanal irrigation for disordered defecation: A systematic review. Scand. J. Gastroenterol. 2010, 45, 517–527. [Google Scholar] [CrossRef]
- Christensen, P.; Bazzocchi, G.; Coggrave, M.; Abel, R.; Hultling, C.; Krogh, K.; Media, S.; Laurberg, S. A randomized, controlled trial of transanal irrigation versus conservative bowel management in spinal cord-injured patients. Gastroenterology 2006, 131, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Krogh, K.; Christensen, P.; Sabroe, S.; Laurberg, S. Neurogenic bowel dysfunction score. Spinal Cord 2006, 44, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Lee, B.S.; Lee, J.E.; Shin, H.I. Application of transanal irrigation for patients with spinal cord injury in South Korea: A 6-month follow-up study. Spinal Cord 2013, 51, 389–394. [Google Scholar] [CrossRef]
- Preziosi, G.; Gosling, J.; Raeburn, A.; Storrie, J.; Panicker, J.; Emmanuel, A. Transanal irrigation for bowel symptoms in patients with multiple sclerosis. Dis. Colon. Rectum 2012, 55, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Brochard, C.; Peyronnet, B.; Hascoet, J.; Olivier, R.; Manunta, A.; Jezequel, M.; Alimi, Q.; Ropert, A.; Neunlist, M.; Bouguen, G.; et al. Defecation disorders in Spina Bifida: Realistic goals and best therapeutic approaches. Neurourol. Urodyn. 2019, 38, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Brochard, C.; Jezequel, M.; Blanchard-Dauphin, A.; Kerdraon, J.; Perrouin-Verbe, B.; Leroi, A.M.; Reymann, J.M.; Peyronnet, B.; Morçet, J.; Siproudhis, L. Transanal irrigation is a better choice for bowel dysfunction in adults with Spina bifida: A randomised controlled trial. Colorectal Dis. 2023, 25, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S.; Wallwork, S.; Soni, B.M. Transanal irrigation with Peristeen in neurogenic bowel dysfunction: Audit of impact on symptoms and quality of life. Gastrointest. Nurs. 2020, 18, 27–34. [Google Scholar] [CrossRef]
- Teng, M.; Miget, G.; Moutounaick, M.; Kervinio, F.; Charlanes, A.; Chesnel, C.; Breton, F.L.; Amarenco, G. Transanal Irrigation for Neurogenic Bowel Dysfunction in Multiple Sclerosis: A Retrospective Study. J. Neurogastroenterol. Motil. 2022, 28, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Del Popolo, G.; Mosiello, G.; Pilati, C.; Lamartina, M.; Battaglino, F.; Buffa, P.; Redaelli, T.; Lamberti, G.; Menarini, M.; Di Benedetto, P.; et al. Treatment of neurogenic bowel dysfunction using transanal irrigation: A multicenter Italian study. Spinal Cord 2008, 46, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Hamonet-Torny, J.; Bordes, J.; Daviet, J.C.; Dalmay, F.; Joslin, F.; Salle, J.Y. Long-term transanal irrigation’s continuation at home. Preliminary study. Ann. Phys. Rehabil. Med. 2013, 56, 134–142. [Google Scholar] [CrossRef]
- Boman, E.; Nylander, M.; Oja, J.; Olofsson, B. Transanal Irrigation for People With Neurogenic Bowel Dysfunction: An Integrative Literature Review. Gastroenterol. Nurs. 2022, 45, 211–230. [Google Scholar] [CrossRef]
- Christensen, P.; Krogh, K.; Perrouin-Verbe, B.; Leder, D.; Bazzocchi, G.; Petersen Jakobsen, B.; Emmanuel, A.V. Global audit on bowel perforations related to transanal irrigation. Tech. Coloproctol. 2016, 20, 109–115. [Google Scholar] [CrossRef]
- Faaborg, P.M.; Christensen, P.; Kvitsau, B.; Buntzen, S.; Laurberg, S.; Krogh, K. Long-term outcome and safety of transanal colonic irrigation for neurogenic bowel dysfunction. Spinal Cord 2009, 47, 545–549. [Google Scholar] [CrossRef]
- Bildstein, C.; Melchior, C.; Gourcerol, G.; Boueyre, E.; Bridoux, V.; Verin, E.; Leroi, A.M. Predictive factors for compliance with transanal irrigation for the treatment of defecation disorders. World J. Gastroenterol. 2017, 23, 2029–2036. [Google Scholar] [CrossRef]
- Ethans, K.; Smith, K.; Khandelwal, A.; Nankar, M.; Shea, J.; Casey, A. Transanal irrigation bowel routine for people with Cauda Equina Syndrome. J. Spinal Cord Med. 2022, 47, 263–269. [Google Scholar] [CrossRef]
- Christensen, P.; Olsen, N.; Krogh, K.; Bacher, T.; Laurberg, S. Scintigraphic assessment of retrograde colonic washout in fecal incontinence and constipation. Dis. Colon Rectum 2003, 46, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Knowles, C.H.; Dinning, P.; Scott, S.M.; Swash, M.; de Wachter, S. New concepts in the pathophysiology of fecal incontinence. Ann. Laparosc. Endosc. Surg. 2022, 7, 15. [Google Scholar] [CrossRef]
- Metcalf, A.M.; Phillips, S.F.; Zinsmeister, A.R.; MacCarty, R.L.; Beart, R.W.; Wolff, B.G. Simplified assessment of segmental colonic transit. Gastroenterology 1987, 92, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Ascanelli, S.; Bombardini, C.; Chimisso, L.; Carcoforo, P.; Turroni, S.; D’Amico, F.; Caniati, M.L.; Baldi, E.; Tugnoli, V.; Morotti, C.; et al. Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study. Mult. Scler. J. Exp. Transl. Clin. 2022, 8, 20552173221109771. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Scale | TAI Group Scores | Conservative Treatment Group Scores | p-Value |
|---|---|---|---|
| Cleveland Clinic Constipation * | 10.3 | 13.2 | 0.0016 |
| St. Mark’s Fecal Incontinence * | 5.0 | 7.3 | 0.015 |
| NBD Score * | 10.4 | 13.3 | 0.048 |
| Quality of life | 6.3 | 4.2 | 0.00009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez, G.; Kirshblum, S.; Thao, M.; McArthur, M.; Camilleri, M. The Functional Implications of Transanal Irrigation: Insights from Pathophysiology and Clinical Studies of Neurogenic Bowel Dysfunction. J. Clin. Med. 2024, 13, 1527. https://doi.org/10.3390/jcm13061527
Rodriguez G, Kirshblum S, Thao M, McArthur M, Camilleri M. The Functional Implications of Transanal Irrigation: Insights from Pathophysiology and Clinical Studies of Neurogenic Bowel Dysfunction. Journal of Clinical Medicine. 2024; 13(6):1527. https://doi.org/10.3390/jcm13061527
Chicago/Turabian StyleRodriguez, Gianna, Steven Kirshblum, Mai Thao, Mackenzie McArthur, and Michael Camilleri. 2024. "The Functional Implications of Transanal Irrigation: Insights from Pathophysiology and Clinical Studies of Neurogenic Bowel Dysfunction" Journal of Clinical Medicine 13, no. 6: 1527. https://doi.org/10.3390/jcm13061527