
Laparoscopic Treatment of Perforated Peptic Ulcer: A Propensity Score-Matched Comparison of Interrupted Stitches Repair versus Knotless Barbed Suture
 ,
on behalf of the IGo-GIPS Study Group
,
on behalf of the IGo-GIPS Study Group
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Settings and Protocol
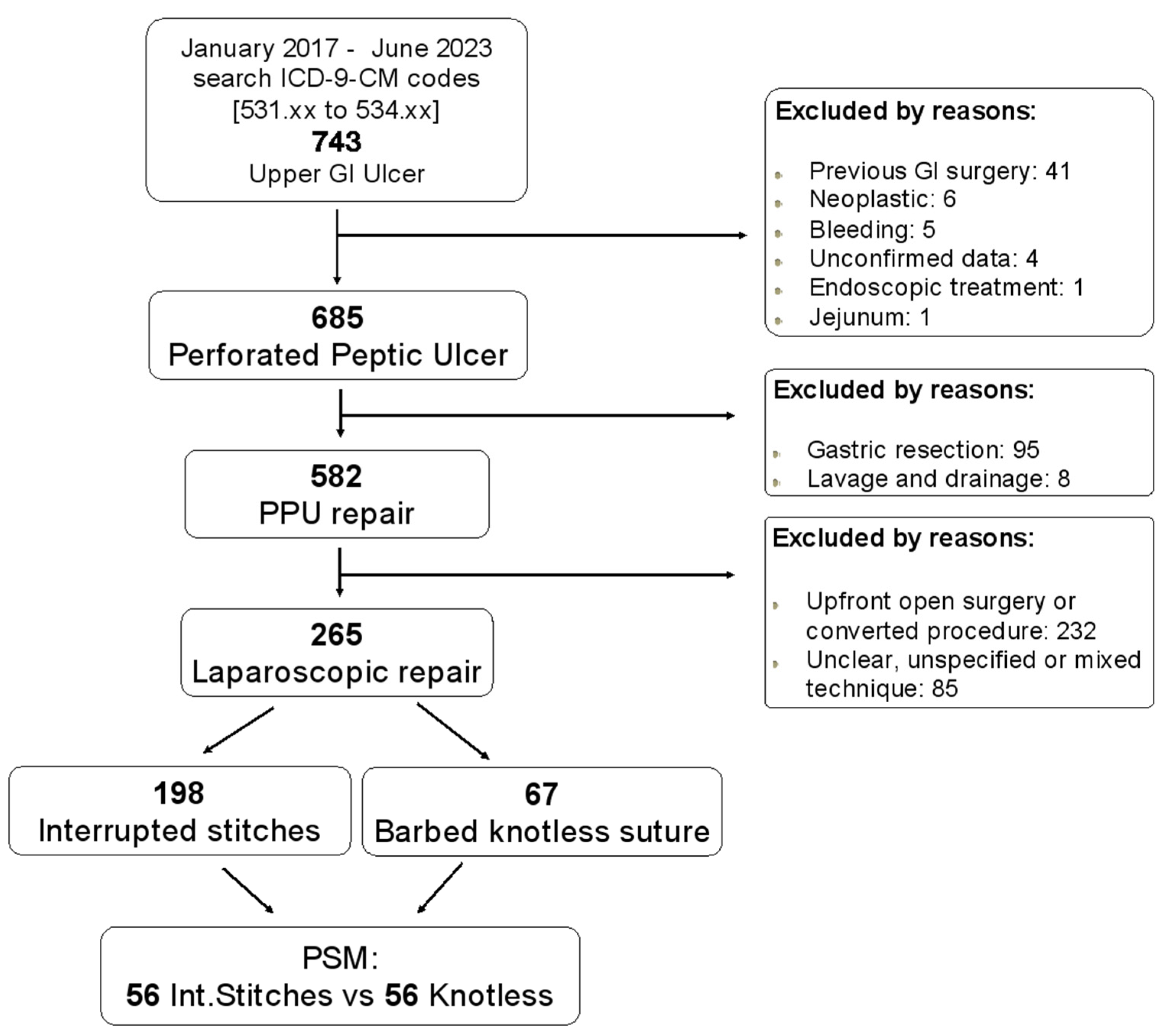
2.2. Inclusion and Exclusion Criteria and Collected Data Confirmation
2.3. Patients’ Characteristics, Preoperative Variables and Objectives of This Study
3. Statistical Analysis
4. Results
4.1. Entire Series
4.2. Comparison before PSM
4.3. Comparison after PSM

{kind=link}
| Entire Cohort 265 (%) | IStiS 198 (%) | KnotS 67 (%) | p Value | |
|---|---|---|---|---|
| Gender, male n. (%) | 144 (54.3) | 109 (55.1) | 35 (52.2) | 0.690 |
| Mean age, (range) | 60.6 ± 16.8 (18–92) | 59.9 ± 17.1 (18–92) | 62.4 ± 16.0 (29–91) | 0.291 |
| BMI | 25.2 ± 4.6 | 25.4 ± 4.7 | 24.7 ± 4.5 | 0.342 |
| ASA ≥ 3 | 123 (46.4) | 92 (46.5) | 31 (46.3) | 0.978 |
| Site | 0.848 | |||
| Gastric prepyloric | 116 (43.8) | 86 (43.4) | 30 (44.8) | |
| Duodenal bulb | 149 (56.2) | 112 (56.6) | 37 (55.2) | |
| Size (mm) | 7.7 ± 2.6 | 7.8 ± 2.6 | 7.7 ± 2.6 | 0.750 |
| Surgical procedure | ||||
| Simple suture | 17 (6.4) | 12 (6.1) | 5 (7.5) | |
| Suture plus omental patch | 239 (90.2) | 179 (90.4) | 60 (89.5) | |
| Graham omentopexy | 9 (3.4) | 7 (3.5) | 2 (3.0) | |
| Operating time (minutes) | 91.7 ± 41.2 | 92.0 ± 41.6 | 90.8 ± 40.1 | 0.832 |
| Hemoglobin | 13.7 ± 2.5 | 13.7 ± 2.3 | 13.5 ± 3.0 | 0.604 |
| WBC | 13.5 ± 5.6 | 13.3 ± 5.4 | 13.9 ± 6.0 | 0.417 |
| PLT | 279.7 ± 89.2 | 281.4 ± 91.4 | 274.7 ± 83.0 | 0.598 |
| Glycemia | 139.9 ± 46.0 | 140.0 ± 49.1 | 139.6 ± 35.9 | 0.948 |
| Creatinine | 1.1 ± 0.8 | 1.0 ± 0.6 | 1.3 ± 1.1 | 0.007 |
| INR | 1.2 ± 0.5 | 1.2 ± 0.5 | 1.2 ± 0.6 | 0.538 |
| Lactate (mmol/L) | 2.8 ± 0.1 | 2.7 ± 0.1 | 2.9 ± 0.2 | 0.403 |
| C-Reactive Protein | 6.5 ± 6.9 | 6.6 ± 7.2 | 6.2 ± 6.0 | 0.707 |
| BOEY score | 1.2 ± 0.9 | 1.2 ± 1.0 | 1.3 ± 1.0 | 0.383 |
| Mannheim Peritonitis Index (MPI) | 17.1 ± 7.8 | 17.2 ± 8.1 | 17.0 ± 6.7 | 0.866 |
| Pulp Score | 4.3 ± 3.0 | 4.2 ± 3.0 | 4.4 ± 3.1 | 0.717 |
| SIRS | 1.3 ± 1.0 | 1.3 ± 0.9 | 1.4 ± 1.0 | 0.418 |
| qSOFA | 0.29 ± 0.03 | 0.28 ± 0.03 | 0.31 ± 0.08 | 0.685 |
| Shock Index | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.958 |
| Age–Shock Index | 42.3 ± 19.1 | 41.7 ± 18.4 | 44.2 ± 21.2 | 0.354 |
| CACI | 2.62 ± 2.29 | 2.46 ± 2.25 | 3.10 ± 2.36 | 0.049 |
| CACI ≥ 6 | 32 (12.1) | 21 (10.6) | 11 (16.4) | 0.207 |
| EmSFI | 2.86 ± 1.29 | 2.75 ± 1.18 | 3.17 ± 1.53 | 0.021 |
| 5-Item frailty Index | 0.12 ± 0.16 | 0.11 ± 0.14 | 0.17 ± 0.19 | 0.004 |
| Frailty yes (5-mFI ≥ 0.4) | 35 (13.2) | 22 (11.1) | 13 (19.4) | 0.083 |
| LOS (days) | 10.5 ± 10.7 | 10.3 ± 10.8 | 11.3 ± 10.4 | 0.518 |
| Morbidity | 69 (28.9) | 46 (25.7) | 23 (38.3) | 0.062 |
| Clavien–Dindo I–II | 46 (17.4) | 32 (16.2) | 14 (20.9) | 0.377 |
| Clavien–Dindo III | 14 (5.3) | 8 (4.0) | 6 (9.0) | 0.126 |
| Clavien–Dindo IV | 10 (3.8) | 7 (3.5) | 3 (4.5) | 0.717 |
| CCI (Comprehensive Complication Index 0–100) | 47.35 ± 34.59 | 48.97 ± 35.12 | 43.84 ± 33.74 | 0.504 |
| CCI (Comprehensive Complication Index ≥8) | 17.05 ± 30.70 | 16.18 ± 30.51 | 19.63 ± 31.35 | 0.428 |
| Mortality | 26 (9.8) | 19 (9.6) | 7 (10.5) | 0.815 |
| Before Propensity Score Matching | p Value | After Propensity Score Matching | p Value | |||
|---|---|---|---|---|---|---|
| IStiS 198 (%) | KnotS 67 (%) | IStiS 56 (%) | KnotS 56 (%) | |||
| Age, year | 59.9 ± 17.1 | 62.4 ± 16.0 | 0.291 | 63.6 ± 15.1 | 62.5 ± 15.3 | 0.715 |
| Male sex n (%) | 109 (55.1) | 35 (52.2) | 0.690 | 30 (53.6) | 30 (53.6) | 1.000 |
| BMI, kg/m2 | 25.4 ± 4.7 | 24.7 ± 4.5 | 0.342 | 25.2 ± 5.8 | 24.4 ± 4.7 | 0.441 |
| ASA ≥ 3 | 92 (46.5) | 31 (46.3) | 0.978 | 23 (41.1) | 24 (42.9) | 0.251 |
| Lactate (mmol/L) | 2.7 ± 0.1 | 2.9 ± 0.2 | 0.403 | 2.5 ± 0.2 | 2.8 ± 0.2 | 0.374 |
| Glycemia | 140.0 ± 49.1 | 139.6 ± 35.9 | 0.948 | 148.8 ± 62.1 | 141.8 ± 35.5 | 0.470 |
| Creatinine | 1.0 ± 0.6 | 1.3 ± 1.1 | 0.007 | 1.0 ± 0.4 | 1.1 ± 0.8 | 0.301 |
| INR | 1.2 ± 0.5 | 1.2 ± 0.6 | 0.538 | 1.3 ± 0.5 | 1.2 ± 0.6 | 0.899 |
| Hemoglobin (g/dL) | 13.7 ± 2.3 | 13.5 ± 3.0 | 0.604 | 13.5 ± 2.4 | 13.9 ± 2.3 | 0.304 |
| WBC (109/L) | 13.3 ± 5.4 | 13.9 ± 6.0 | 0.417 | 13.4 ± 5.2 | 13.6 ± 6.2 | 0.828 |
| PLT | 281.4 ± 91.4 | 274.7 ± 83.0 | 0.598 | 289.9 ± 108.8 | 274.9 ± 83.5 | 0.413 |
| C-Reactive Protein (mg/L) | 6.6 ± 7.2 | 6.2 ± 6.0 | 0.707 | 6.1 ± 6.8 | 6.1 ± 6.2 | 0.976 |
| CACI | 2.46 ± 2.25 | 3.10 ± 2.36 | 0.049 | 2.78 ± 1.96 | 2.73 ± 2.09 | 0.889 |
| CACI ≥ 6 | 21 (10.6) | 11 (16.4) | 0.207 | 4 (7.1) | 5 (8.9) | 1.000 |
| Shock Index | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.958 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.676 |
| Age-Shock Index | 41.7 ± 18.4 | 44.2 ± 21.2 | 0.354 | 45.0 ± 17.6 | 43.3 ± 17.9 | 0.611 |
| SIRS | 1.3 ± 0.9 | 1.4 ± 1.0 | 0.418 | 1.4 ± 1.0 | 1.3 ± 1.0 | 0.852 |
| qSofa | 0.28 ± 0.03 | 0.31 ± 0.08 | 0.685 | 0.30 ± 0.07 | 0.26 ± 0.08 | 0.745 |
| EmSFI | 2.75 ± 1.18 | 3.17 ± 1.53 | 0.021 | 2.82 ± 0.79 | 2.89 ± 1.02 | 0.679 |
| 5-Item frailty Index | 0.11 ± 0.14 | 0.17 ± 0.19 | 0.004 | 0.12 ± 0.13 | 0.14 ± 0.16 | 0.601 |
| Frailty yes (5-mFI ≥ 0.4) | 22 (11.1) | 13 (19.4) | 0.083 | 3 (5.4) | 7 (12.5) | 0.321 |
| Before Propensity Score Matching | p Value | After Propensity Score Matching | p Value | |||
|---|---|---|---|---|---|---|
| IStiS 198 (%) | KnotS 67 (%) | IStiS 56 (%) | KnotS 56 (%) | |||
| Operative time (min), mean ± SD | 92.0 ± 41.6 | 90.8 ± 40.1 | 0.832 | 87.9 ± 39.7 | 92.8 ± 42.6 | 0.537 |
| Site | 0.848 | 0.131 | ||||
| Gastric prepyloric | 86 (43.4) | 30 (44.8) | 32 (57.1) | 24 (42.9) | ||
| Duodenal bulb | 112 (56.6) | 37 (55.2) | 24 (42.9) | 32 (57.1) | ||
| Ulcer size (mm), mean ± SD | 7.8 ± 2.6 | 7.7 ± 2.6 | 0.750 | 7.6 ± 2.4 | 7.8 ± 2.7 | 0.756 |
| Boey Score | 1.2 ± 1.0 | 1.3 ± 1.0 | 0.383 | 1.2 ± 1.0 | 1.2 ± 0.9 | 0.774 |
| Mannheim Peritonitis Index (MPI) | 17.2 ± 8.1 | 17.0 ± 6.7 | 0.866 | 17.1 ± 7.3 | 16.8 ± 6.9 | 0.842 |
| Pulp score | 4.2 ± 3.0 | 4.4 ± 3.1 | 0.717 | 4.5 ± 2.7 | 4.2 ± 2.9 | 0.569 |
| Leak | 12 (6.1) | 5 (7.5) | 0.773 | 2 (3.6) | 3 (5.4) | 1.000 |
| 30 days morbidity (Clavien–Dindo I–IV) (n, %) | 46 (25.7) | 23 (38.3) | 0.062 | 12 (24.0) | 17 (32.7) | 0.331 |
| Clavien–Dindo I–II | 32 (16.2) | 14 (20.9) | 0.377 | 10 (17.9) | 11 (19.6) | 0.809 |
| Clavien–Dindo III | 8 (4.0) | 6 (9.0) | 0.126 | 3 (5.4) | 6 (10.7) | 0.489 |
| Clavien–Dindo IV | 7 (3.5) | 3 (4.5) | 0.717 | - | - | |
| CCI (Comprehensive Complication Index 0–100) | 48.97 ± 35.12 | 43.84 ± 33.74 | 0.504 | 48.88 ± 38.35 | 38.68 ± 32.68 | 0.375 |
| CCI (Comprehensive Complication Index ≥8) | 16.18 ± 30.51 | 19.63 ± 31.35 | 0.428 | 16.09 ± 31.32 | 14.50 ± 27.30 | 0.776 |
| Length Hospital Stay (days, median) | 10.3 ± 10.8 | 11.3 ± 10.4 | 0.518 | 9.4 ± 8.1 | 10.8 ± 10.6 | 0.465 |
| Postoperative 30-day mortality, n (%) | 19 (9.6) | 7 (10.5) | 0.815 | 6 (10.7) | 4 (7.1) | 0.742 |
5. Discussion
6. Limitations and Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. List of Italian Group for Gastro-Intestinal Surgery Postoperative Surveillance (IGo-GIPS)
References
- Lanas, A.; Chan, F.K.L. Peptic ulcer disease. Lancet 2017, 390, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Azhari, H.; King, J.A.; Coward, S.; Windsor, J.W.; Ma, C.; Shah, S.C.; Ng, S.C.; Mak, J.W.; Kotze, P.G.; Ben-Horin, S.; et al. The Global Incidence of Peptic Ulcer Disease Is Decreasing Since the Turn of the 21st Century: A Study of the Organisation for Economic Co-Operation and Development (OECD). Am. J. Gastroenterol. 2022, 117, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Dadfar, A.; Edna, T.-H. Epidemiology of perforating peptic ulcer: A population-based retrospective study over 40 years. World J. Gastroenterol. 2020, 26, 5302–5313. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.H.; McLean, R.C.; McCallum, I.; Perren, D.; Phillips, A.W. An evaluation of the epidemiology, management and outcomes for perforated peptic ulcers across the North of England over 15 years: A retrospective cohort study. Int. J. Surg. 2019, 64, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Sivaram, P.; Sreekumar, A. Preoperative factors influencing mortality and morbidity in peptic ulcer perforation. Eur. J. Trauma Emerg. Surg. 2018, 44, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Mansoor, T.; Rab, A.Z.; Rizvi, S.A.A. Risk factors influencing postoperative outcome in patients with perforated peptic ulcer: A prospective cohort study. Eur. J. Trauma Emerg. Surg. 2022, 48, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Lanas, A.; García-Rodríguez, L.A.; Polo-Tomás, M.; Ponce, M.; Quintero, E.; Perez-Aisa, M.A.; Gisbert, J.P.; Bujanda, L.; Castro, M.; Muñoz, M.; et al. The changing face of hospitalisation due to gastrointestinal bleeding and perforation. Aliment. Pharmacol. Ther. 2011, 33, 585–591. [Google Scholar] [CrossRef]
- Kubosawa, Y.; Mori, H.; Kinoshita, S.; Nakazato, Y.; Fujimoto, A.; Kikuchi, M.; Nishizawa, T.; Suzuki, M.; Suzuki, H. Changes of gastric ulcer bleeding in the metropolitan area of Japan. World J. Gastroenterol. 2019, 25, 6342–6353. [Google Scholar] [CrossRef]
- Leow, A.H.; Lim, Y.; Liew, W.; Goh, K. Time trends in upper gastrointestinal diseases and Helicobacter pylori infection in a multiracial Asian population—A 20-year experience over three time periods. Aliment. Pharmacol. Ther. 2016, 43, 831–837. [Google Scholar] [CrossRef]
- Nagata, N.; Niikura, R.; Sekine, K.; Sakurai, T.; Shimbo, T.; Kishida, Y.; Tanaka, S.; Aoki, T.; Okubo, H.; Watanabe, K.; et al. Risk of peptic ulcer bleeding associated with Helicobacter pylori infection, nonsteroidal anti-inflammatory drugs, low-dose aspirin, and antihypertensive drugs: A case-control study. J. Gastroenterol. Hepatol. 2015, 30, 292–298. [Google Scholar] [CrossRef]
- Nagasue, T.; Nakamura, S.; Kochi, S.; Kurahara, K.; Yaita, H.; Kawasaki, K.; Fuchigami, T. Time Trends of the Impact of Helicobacter pylori Infection and Nonsteroidal Anti-Inflammatory Drugs on Peptic Ulcer Bleeding in Japanese Patients. Digestion 2015, 91, 37–41. [Google Scholar] [CrossRef]
- Boey, J.M.; Choi, S.K.Y.F.; Alagaratnam, T.T.F.; Poon, A.F. Risk stratification in perforated duodenal ulcers. A prospective validation of predictive factors. Ann. Surg. 1987, 205, 22–26. [Google Scholar] [CrossRef]
- Buck, D.L.; Vester-Andersen, M.; Møller, M.H. Surgical delay is a critical determinant of survival in perforated peptic ulcer. Br. J. Surg. 2013, 100, 1045–1049. [Google Scholar] [CrossRef]
- Mouret, P.; François, Y.; Vignal, J.; Bartht, X.; Lombard-Platet, R. Laparoscopic treatment of perforated peptic ulcer. Br. J. Surg. 1990, 77, 1006. [Google Scholar] [CrossRef]
- Coe, P.O.; Lee, M.J.; Boyd-Carson, H.M.; Lockwood, S.F.; Saha, A. Open Versus Laparoscopic Repair of Perforated Peptic Ulcer Disease: A Propensity-matched Study of the National Emergency Laparotomy Audit. Ann. Surg. 2022, 275, 928–932. [Google Scholar] [CrossRef] [PubMed]
- Leusink, A.; Markar, S.R.; Wiggins, T.; Mackenzie, H.; Faiz, O.; Hanna, G.B. Laparoscopic surgery for perforated peptic ulcer: An English national population-based cohort study. Surg. Endosc. 2018, 32, 3783–3788. [Google Scholar] [CrossRef] [PubMed]
- Fransvea, P.; Costa, G.; Lepre, L.; Podda, M.; Giordano, A.; Bellanova, G.; Agresta, F.; Marini, P.; Sganga, G. Laparoscopic Repair of Perforated Peptic Ulcer in the Elderly: An Interim Analysis of the FRAILESEL Italian Multicenter Prospective Cohort Study. Surg. Laparosc. Endosc. Percutaneous Tech. 2020, 31, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Nemecek, E.; Negrin, L.; Beran, C.; Nemecek, R.; Hollinsky, C. The application of the V-Loc closure device for gastrointestinal sutures: A preliminary study. Surg. Endosc. 2013, 27, 3830–3834. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-W.; Song, S.; Jee, Y.S. Duet laparoscopic repair with knotless barbed sutures for treatment of perforated peptic ulcer: Reality in general surgery with lacking of manpower. Ann. Transl. Med. 2021, 9, 311. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.-C.; Lee, C.-H.; Soong, R.-S.; Chen, Y.-C. A simple and effective technique for laparoscopic gastrorrhaphy: Modified Graham’s patch with barbed suture. BMC Surg. 2023, 23, 295. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; Fransvea, P.; Lepre, L.; Liotta, G.; Mazzoni, G.; Biloslavo, A.; Bianchi, V.; Costa, A.; Sganga, G.; Agresta, F.; et al. Perforated peptic ulcer (PPU) treatment: An Italian nationwide propensity score-matched cohort study investigating laparoscopic vs open approach. Surg. Endosc. 2023, 37, 5137–5149. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; Fransvea, P.; Puccioni, C.; Giovinazzo, F.; Carannante, F.; Bianco, G.; Catamero, A.; Masciana, G.; Miacci, V.; Caricato, M.; et al. Gastro-intestinal emergency surgery: Evaluation of morbidity and mortality. Protocol of a prospective, multicenter study in Italy for evaluating the burden of abdominal emergency surgery in different age groups. (The GESEMM study). Front. Surg. 2022, 9, 927044. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, G.; Chapman, M. Primary closure versus Graham patch omentopexy in perforated peptic ulcer: A systematic review and meta-analysis. Surgeon 2022, 20, e61–e67. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit. Care Med. 1992, 20, 864–874. [Google Scholar] [CrossRef]
- Costa, G.; Massa, G.; ERASO (Elderly Risk Assessment for Surgical Outcome); Collaborative Study Group. Frailty and emergency surgery in the elderly: Protocol of a prospective, multicenter study in Italy for evaluating perioperative outcome (The FRAILESEL Study). Updat. Surg. 2018, 70, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Chimukangara, M.; Helm, M.C.; Frelich, M.J.; Bosler, M.E.; Rein, L.E.; Szabo, A.; Gould, J.C. A 5-item frailty index based on NSQIP data correlates with outcomes following paraesophageal hernia repair. Surg. Endosc. 2017, 31, 2509–2519. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The comprehensive complication index: A novel continuous scale to measure surgical morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef]
- Lonjon, G.; Boutron, I.; Trinquart, L.; Ahmad, N.; Aim, F.; Nizard, R.; Ravaud, P. Comparison of Treatment Effect Estimates From Prospective Nonrandomized Studies With Propensity Score Analysis and Randomized Controlled Trials of Surgical Procedures. Ann. Surg. 2014, 259, 18–25. [Google Scholar] [CrossRef]
- Chung, K.T.; Shelat, V.G. Perforated peptic ulcer—An update. World J. Gastrointest. Surg. 2017, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Agresta, F.; on behalf of the Joined Italian Surgical Societies Working Group; Campanile, F.C.; Podda, M.; Cillara, N.; Pernazza, G.; Giaccaglia, V.; Ciccoritti, L.; Ioia, G.; Mandalà, S.; et al. Current status of laparoscopy for acute abdomen in Italy: A critical appraisal of 2012 clinical guidelines from two consecutive nationwide surveys with analysis of 271,323 cases over 5 years. Surg. Endosc. 2017, 31, 1785–1795. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.; Sousa, H.S.; Gonçalves, D.; da Costa, E.L.; Pinho, A.C.; Barbosa, E.; Barbosa, J. Surgery for Perforated Peptic Ulcer: Is Laparoscopy a New Paradigm? Minim. Invasive Surg. 2021, 2021, 8828091. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; the ERASO (Elderly Risk Assessment and Surgical Outcome) Collaborative Study Group; Fransvea, P.; Podda, M.; Pisanu, A.; Carrano, F.M.; Iossa, A.; Balducci, G.; Agresta, F. The use of emergency laparoscopy for acute abdomen in the elderly: The FRAILESEL Italian Multicenter Prospective Cohort Study. Updat. Surg. 2020, 72, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Mohamedahmed, A.Y.Y.; Albendary, M.; Patel, K.; Ayeni, A.A.; Zaman, S.; Zaman, O.; Ibrahim, R.; Mobarak, D. Comparison of Omental Patch Closure Versus Simple Closure for Laparoscopic Repair of Perforated Peptic Ulcer: A Systematic Review and Meta-Analysis. Am. Surg. 2022, 89, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, A.E.; Morales, C.H.; Villegas, M.I. Laparoscopic repair for perforated peptic ulcer disease. Cochrane Database Syst. Rev. 2005, CD004778. [Google Scholar] [CrossRef]
- Tarasconi, A.; Coccolini, F.; Biffl, W.L.; Tomasoni, M.; Ansaloni, L.; Picetti, E.; Molfino, S.; Shelat, V.; Cimbanassi, S.; Weber, D.G.; et al. Perforated and bleeding peptic ulcer: WSES guidelines. World J. Emerg. Surg. 2020, 15, 1–24. [Google Scholar] [CrossRef]
- Rowlands, B.C.; King, P.A. Immediate Partial Gastrectomy for Perforated Peptic Ulcer. Br. Med. J. 1955, 1, 1254–1256. [Google Scholar] [CrossRef]
- Qvist, G. Vagotomy and Pyloroplasty in the treatment of Peptic Ulcer. Br. J. Clin. Pract. 1964, 19, 235–238. [Google Scholar] [CrossRef]
- Kraft, R.O.; Fry, W.J.; Ransom, H.K. Vagotomy and Pyloroplasty in the Care of Patients with Gastric Ulcer. Arch. Surg. 1966, 92, 456–462. [Google Scholar] [CrossRef]
- Cellan-Jones, C.J. A rapid method of treatment in perforated duodenal ulcer. BMJ 1929, 1, 1076–1077. [Google Scholar] [CrossRef]
- Graham, R. The treatment of perforated duodenal ulcers. Surg. Gynec. Obstet. 1937, 64, 235–238. [Google Scholar]
- Ates, M.; Sevil, S.; Bakircioglu, E.; Colak, C. Laparoscopic Repair of Peptic Ulcer Perforation Without Omental Patch Versus Conventional Open Repair. J. Laparoendosc. Adv. Surg. Tech. A 2007, 17, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.; Wu, S.; Huang, H.; Yeh, C.; Huang, J.; Hsieh, C. Laparoscopic Simple Closure Alone is Adequate for Low Risk Patients with Perforated Peptic Ulcer. Mol. Med. 2011, 35, 1873–1878. [Google Scholar] [CrossRef] [PubMed]
- Ellatif, M.A.; Salama, A.; Elezaby, A.; El-Kaffas, H.; Hassan, A.; Magdy, A.; Abdallah, E.; El-Morsy, G. Laparoscopic repair of perforated peptic ulcer: Patch versus simple closure. Int. J. Surg. 2013, 11, 948–951. [Google Scholar] [CrossRef]
- Wang, Y.; Hsieh, C.; Lo, H.; Su, L. Sutureless Onlay Omental Patch for the Laparoscopic Repair of Perforated Peptic Ulcers. Mol. Med. 2014, 38, 1917–1921. [Google Scholar] [CrossRef]
- Lin, B.-C.; Liao, C.-H.; Wang, S.-Y.; Hwang, T.-L. Laparoscopic repair of perforated peptic ulcer: Simple closure versus omentopexy. J. Surg. Res. 2017, 220, 341–345. [Google Scholar] [CrossRef]
- Odisho, T.; Shahait, A.A.; Sharza, J.; Ali, A.A. Outcomes of laparoscopic modified Cellan-Jones repair versus open repair for perforated peptic ulcer at a community hospital. Surg. Endosc. 2023, 37, 715–722. [Google Scholar] [CrossRef]
- Jang, S.H.; Jung, Y.K.; Choi, S.J.; Ha, T.K. Postoperative mechanical small bowel obstruction induced by V-Loc barbed absorbable suture after laparoscopic distal gastrectomy. Ann. Surg. Treat. Res. 2017, 92, 380–382. [Google Scholar] [CrossRef]
- Sakata, S.; Kabir, S.; Petersen, D.; Doudle, M.; Stevenson, A.R.L. Are we burying our heads in the sand? Preventing small bowel obstruction from the V-loc® suture in laparoscopic ventral rectopexy. Color. Dis. 2015, 17, O180–O183. [Google Scholar] [CrossRef]
- Tyner, R.P.; Clifton, G.T.; Fenton, S.J. Hand-sewn gastrojejunostomy using knotless unidirectional barbed absorbable suture during laparoscopic gastric bypass. Surg. Endosc. 2013, 27, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- De Blasi, V.; Facy, O.; Goergen, M.; Poulain, V.; De Magistris, L.; Azagra, J.S. Barbed Versus Usual Suture for Closure of the Gastrojejunal Anastomosis in Laparoscopic Gastric Bypass: A Comparative Trial. Obes. Surg. 2013, 23, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Lund, S.; Chauhan, K.K.; Zietlow, J.; Stephens, D.; Zietlow, S.; Strajina, V.; Turay, D.; Zielinski, M. Risk Factors for Gastrointestinal Leak after Perforated Peptic Ulcer Disease Operative Repair. Am. Surg. 2021, 87, 1879–1885. [Google Scholar] [CrossRef] [PubMed]
- Dogra, P.; Kaushik, R.; Singh, S.; Bhardwaj, S. Risk factors for leak after omentopexy for duodenal ulcer perforations. Eur. J. Trauma Emerg. Surg. 2022, 49, 1163–1167. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, G.; Garbarino, G.M.; Lepre, L.; Liotta, G.; Mazzoni, G.; Gabrieli, A.; Costa, A.; Podda, M.; Sganga, G.; Fransvea, P., on behalf of the IGo-GIPS Study Group. Laparoscopic Treatment of Perforated Peptic Ulcer: A Propensity Score-Matched Comparison of Interrupted Stitches Repair versus Knotless Barbed Suture. J. Clin. Med. 2024, 13, 1242. https://doi.org/10.3390/jcm13051242
Costa G, Garbarino GM, Lepre L, Liotta G, Mazzoni G, Gabrieli A, Costa A, Podda M, Sganga G, Fransvea P on behalf of the IGo-GIPS Study Group. Laparoscopic Treatment of Perforated Peptic Ulcer: A Propensity Score-Matched Comparison of Interrupted Stitches Repair versus Knotless Barbed Suture. Journal of Clinical Medicine. 2024; 13(5):1242. https://doi.org/10.3390/jcm13051242
Chicago/Turabian StyleCosta, Gianluca, Giovanni Maria Garbarino, Luca Lepre, Gianluca Liotta, Gianluca Mazzoni, Alice Gabrieli, Alessandro Costa, Mauro Podda, Gabriele Sganga, and Pietro Fransvea on behalf of the IGo-GIPS Study Group. 2024. "Laparoscopic Treatment of Perforated Peptic Ulcer: A Propensity Score-Matched Comparison of Interrupted Stitches Repair versus Knotless Barbed Suture" Journal of Clinical Medicine 13, no. 5: 1242. https://doi.org/10.3390/jcm13051242