
Myocardial Injury after Non-Cardiac Surgery in Patients Who Underwent Open Repair for Abdominal Aortic Aneurysm: A Retrospective Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
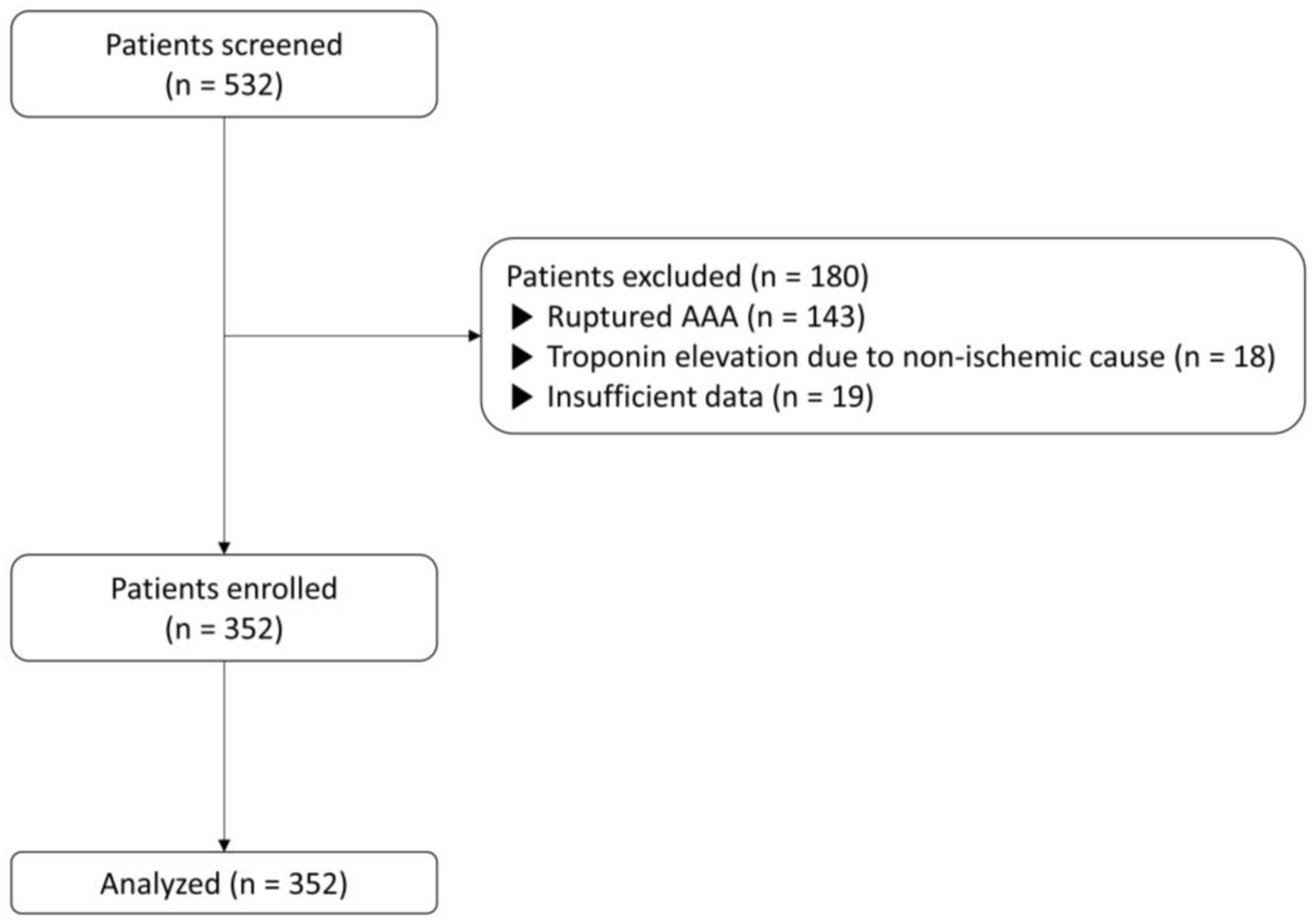
2.1. Study Population
2.2. Data Collection
2.3. Surgical Procedure
2.4. Perioperative Assessment Protocol
2.5. Definition of MINS
2.6. Study Endpoints
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greenhalgh, R. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (evar trial 1), 30-day operative mortality results: Randomised controlled trial. Lancet 2004, 364, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.W.; Hickey, G.L.; Grayson, A.D.; Mitchell, D.C.; McCollum, C.N. National risk prediction model for elective abdominal aortic aneurysm repair. Br. J. Surg. 2013, 100, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.W.; Grayson, A.D.; Mitchell, D.C.; McCollum, C.N. Evaluation of five risk prediction models for elective abdominal aortic aneurysm repair using the uk national vascular database. Br. J. Surg. 2012, 99, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Theissen, A. Enhanced recovery after elective surgery. A revolution that reduces post-operative morbidity and mortality. J. Visc. Surg. 2020, 157, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Biccard, B.M.; Sigamani, A.; Xavier, D.; Chan, M.T.V.; Srinathan, S.K.; Walsh, M.; Abraham, V.; Pearse, R.; Wang, C.Y.; et al. Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2017, 317, 1642–1651. [Google Scholar] [PubMed]
- Devereaux, P.J.; Chan, M.T.; Alonso-Coello, P.; Walsh, M.; Berwanger, O.; Villar, J.C.; Wang, C.Y.; Garutti, R.I.; Jacka, M.J.; Sigamani, A.; et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012, 307, 2295–2304. [Google Scholar]
- Puelacher, C.; Buse, G.L.; Seeberger, D.; Sazgary, L.; Marbot, S.; Lampart, A.; Espinola, J.; Kindler, C.; Hammerer, A.; Seeberger, E.; et al. Perioperative myocardial injury after noncardiac surgery: Incidence, mortality, and characterization. Circulation 2018, 137, 1221–1232. [Google Scholar] [CrossRef]
- van Waes, J.A.; Nathoe, H.M.; de Graaff, J.C.; Kemperman, H.; de Borst, G.J.; Peelen, L.M.; van Klei, W.A. Myocardial injury after noncardiac surgery and its association with short-term mortality. Circulation 2013, 127, 2264–2271. [Google Scholar] [CrossRef]
- Devereaux, P.; Szczeklik, W. Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur. Heart J. 2020, 41, 3083–3091. [Google Scholar] [CrossRef]
- Ruetzler, K.; Smilowitz, N.R.; Berger, J.S.; Devereaux, P.J.; Maron, B.A.; Newby, L.K.; de Jesus Perez, V.; Sessler, D.I.; Wijeysundera, D.N. Diagnosis and management of patients with myocardial injury after noncardiac surgery: A scientific statement from the american heart association. Circulation 2021, 144, e287–e305. [Google Scholar] [CrossRef]
- Biccard, B.M.; Scott, D.J.A.; Chan, M.T.V.; Archbold, A.; Wang, C.Y.; Sigamani, A.; Urrútia, G.; Cruz, P.; Srinathan, S.K.; Szalay, D.; et al. Myocardial injury after noncardiac surgery (mins) in vascular surgical patients: A prospective observational cohort study. Ann. Surg. 2018, 268, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. Kdigo clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Callaghan, C.J.; Ali, A.A.; Sheikh, A.Y.; Akhtar, A.; Pavlovic, A.; Nouraei, S.A.; Dutka, D.P.; Gaunt, M.E. Perioperative myocardial injury after elective open abdominal aortic aneurysm repair predicts outcome. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 413–419. [Google Scholar] [CrossRef]
- Mannova, J.; Silhart, Z.; Prokes, A.; Sevcik, P. Myocardial injury in patients after an elective abdominal aortic aneurysm repair. Bratisl. Lek. Listy 2013, 114, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Botto, F.; Alonso-Coello, P.; Chan, M.T.; Villar, J.C.; Xavier, D.; Srinathan, S.; Guyatt, G.; Cruz, P.; Graham, M.; Wang, C.Y.; et al. Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014, 120, 564–578. [Google Scholar] [PubMed]
- Smilowitz, N.R.; Redel-Traub, G.; Hausvater, A.; Armanious, A.; Nicholson, J.; Puelacher, C.; Berger, J.S. Myocardial injury after noncardiac surgery: A systematic review and meta-analysis. Cardiol. Rev. 2019, 27, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2019, 16, 225–242. [Google Scholar] [CrossRef]
- Kuivaniemi, H.; Ryer, E.J.; Elmore, J.R.; Tromp, G. Understanding the pathogenesis of abdominal aortic aneurysms. Expert. Rev. Cardiovasc. Ther. 2015, 13, 975–987. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Sessler, D.I. Cardiac complications in patients undergoing major noncardiac surgery. N. Engl. J. Med. 2015, 373, 2258–2269. [Google Scholar] [CrossRef]
- Golledge, J.; Norman, P.E. Atherosclerosis and abdominal aortic aneurysm: Cause, response, or common risk factors? Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1075–1077. [Google Scholar] [CrossRef]
- Singh, K.; Bønaa, K.; Jacobsen, B.; Bjørk, L.; Solberg, S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The tromsø study. Am. J. Epidemiol. 2001, 154, 236–244. [Google Scholar] [CrossRef]
- Sukhija, R.; Aronow, W.S.; Yalamanchili, K.; Sinha, N.; Babu, S. Prevalence of coronary artery disease, lower extremity peripheral arterial disease, and cerebrovascular disease in 110 men with an abdominal aortic aneurysm. Am. J. Cardiol. 2004, 94, 1358–1359. [Google Scholar] [CrossRef] [PubMed]
- Collard, C.D.; Gelman, S. Pathophysiology, clinical manifestations, and prevention of ischemia-reperfusion injury. Anesthesiology 2001, 94, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Katseni, K.; Chalkias, A.; Kotsis, T.; Dafnios, N.; Arapoglou, V.; Kaparos, G.; Logothetis, E.; Iacovidou, N.; Karvouni, E.; Katsenis, K. The effect of perioperative ischemia and reperfusion on multiorgan dysfunction following abdominal aortic aneurysm repair. Biomed. Res. Int. 2015, 2015, 598980. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Dorado, D.; Oliveras, J. Myocardial oedema: A preventable cause of reperfusion injury? Cardiovasc. Res. 1993, 27, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Böttiger, B.W.; Motsch, J.; Böhrer, H.; Böker, T.; Aulmann, M.; Nawroth, P.P.; Martin, E. Activation of blood coagulation after cardiac arrest is not balanced adequately by activation of endogenous fibrinolysis. Circulation 1995, 92, 2572–2578. [Google Scholar] [CrossRef] [PubMed]
- Zammert, M.; Gelman, S. The pathophysiology of aortic cross-clamping. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Meershoek, A.J.A.; Leunissen, T.C.; van Waes, J.A.R.; Klei, W.A.; Huisman, A.; de Groot, M.C.H.; Hoefer, I.E.; van Solinge, W.W.; Moll, F.L.; de Borst, G.J. Reticulated platelets as predictor of myocardial injury and 30 day mortality after non-cardiac surgery. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Khashram, M.; Hider, P.N.; Williman, J.A.; Jones, G.T.; Roake, J.A. Does the diameter of abdominal aortic aneurysm influence late survival following abdominal aortic aneurysm repair? A systematic review and meta-analysis. Vascular 2016, 24, 658–667. [Google Scholar] [CrossRef]
- Loram, L.C.; Themistocleous, A.C.; Fick, L.G.; Kamerman, P.R. The time course of inflammatory cytokine secretion in a rat model of postoperative pain does not coincide with the onset of mechanical hyperalgesia. Can. J. Physiol. Pharmacol. 2007, 85, 613–620. [Google Scholar] [CrossRef]
- Wasko, M.K.; Bobecka-Wesołowska, K.; Tomasiuk, R.; Kowalczewski, J. Measurement of the inflammatory response in the early postoperative period after hip and knee arthroplasty. Clin. Chem. Lab. Med. 2015, 53, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Duceppe, E.; Parlow, J.; MacDonald, P.; Lyons, K.; McMullen, M.; Srinathan, S.; Graham, M.; Tandon, V.; Styles, K.; Bessissow, A.; et al. Canadian cardiovascular society guidelines on perioperative cardiac risk assessment and management for patients who undergo noncardiac surgery. Can. J. Cardiol. 2017, 33, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Marcantonio, E.R.; Mangione, C.M.; Thomas, E.J.; Polanczyk, C.A.; Cook, E.F.; Sugarbaker, D.J.; Donaldson, M.C.; Poss, R.; Ho, K.K. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999, 100, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Hertzer, N.R. Fatal myocardial infarction following abdominal aortic aneurysm resection. Three hundred forty-three patients followed 6–11 years postoperatively. Ann. Surg. 1980, 192, 667. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, S.; Mehilli, J.; Cassese, S.; Hall, T.S.; Abdelhamid, M.; Barbato, E.; De Hert, S.; de Laval, I.; Geisler, T.; Hinterbuchner, L.; et al. 2022 ESC guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery. Eur. Heart J. 2022, 43, 3826–3924. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Xavier, D.; Pogue, J.; Guyatt, G.; Sigamani, A.; Garutti, I.; Leslie, K.; Rao-Melacini, P.; Chrolavicius, S.; Yang, H.; et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study. Ann. Intern. Med. 2011, 154, 523–528. [Google Scholar] [CrossRef]
- Lalka, S.G.; Sawada, S.G.; Dalsing, M.C.; Cikrit, D.F.; Sawchuk, A.P.; Kovacs, R.L.; Segar, D.S.; Ryan, T.; Feigenbaum, H. Dobutamine stress echocardiography as a predictor of cardiac events associated with aortic surgery. J. Vasc. Surg. 1992, 15, 831–842. [Google Scholar] [CrossRef]
- Langan, E.M., III; Youkey, J.R.; Franklin, D.P.; Elmore, J.R.; Costello, J.M.; Nassef, L.A. Dobutamine stress echocardiography for cardiac risk assessment before aortic surgery. J. Vasc. Surg. 1993, 18, 905–913. [Google Scholar] [CrossRef]
- Sigl, M.; Baumann, S.; Könemann, A.S.; Keese, M.; Schwenke, K.; Gerken, A.L.H.; Dürschmied, D.; Rosenkaimer, S. Prognostic value of extended cardiac risk assessment before elective open abdominal aortic surgery. Herz 2023. [Google Scholar] [CrossRef]
- Mertes, H.; Sawada, S.G.; Ryan, T.; Segar, D.S.; Kovacs, R.; Foltz, J.; Feigenbaum, H. Symptoms, adverse effects, and complications associated with dobutamine stress echocardiography. Experience in 1118 patients. Circulation 1993, 88, 15–19. [Google Scholar] [CrossRef]
- Geleijnse, M.L.; Krenning, B.J.; Nemes, A.; van Dalen, B.M.; Soliman, O.I.; Cate, F.J.T.; Schinkel, A.F.; Boersma, E.; Simoons, M.L. Incidence, pathophysiology, and treatment of complications during dobutamine-atropine stress echocardiography. Circulation 2010, 121, 1756–1767. [Google Scholar] [CrossRef]
- Columbo, J.A.; Demsas, F.; Wanken, Z.J.; Suckow, B.D.; Beach, J.M.; Henkin, S.; Goodney, P.P.; Stone, D.H. Stress testing before abdominal aortic aneurysm repair does not lead to a reduction in perioperative cardiac events. J. Vasc. Surg. 2021, 74, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Raux, M.; Godet, G.; Isnard, R.; Mergoni, P.; Goarin, J.-P.; Bertrand, M.; Fleron, M.; Coriat, P.; Riou, B. Low negative predictive value of dobutamine stress echocardiography before abdominal aortic surgery. Br. J. Anaesth. 2006, 97, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Cutler, B.S.; Hendel, R.C.; Leppo, J.A. Dipyridamole-thallium scintigraphy predicts perioperative and long-term survival after major vascular surgery. J. Vasc. Surg. 1992, 15, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Cutler, B.S.; Leppo, J.A. Dipyridamole thallium 201 scintigraphy to detect coronary artery disease before abdominal aortic surgery. J. Vasc. Surg. 1987, 5, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.-F.; Mundler, O.; Bertrand, M.; Vicaut, E.; Barre, E.; Godet, G.; Samama, C.M.; Coriat, P.; Kieffer, E.; Viars, P. Dipyridamole-thallium scintigraphy and gated radionuclide angiography to assess cardiac risk before abdominal aortic surgery. N. Engl. J. Med. 1994, 330, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Kwon, T.W.; Cho, Y.P.; Lee, J.Y.; Park, H.; Han, Y. Preoperative cardiac evaluation by dipyridamole thallium-201 myocardial perfusion scan provides no benefit in patients with abdominal aortic aneurysm. World J. Surg. 2013, 37, 2965–2971. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.D.; Huang, W.C.; Peng, N.J.; Hu, C. Dipyridamole-induced adverse effects in myocardial perfusion scans: Dynamic evaluation. Int. J. Cardiol. Heart Vasc. 2017, 14, 14–19. [Google Scholar] [CrossRef]
- Buse, G.L.; Manns, B.; Lamy, A.; Guyatt, G.; Polanczyk, C.A.; Chan, M.T.V.; Wang, C.Y.; Villar, J.C.; Sigamani, A.; Sessler, D.I.; et al. Troponin t monitoring to detect myocardial injury after noncardiac surgery: A cost-consequence analysis. Can. J. Surg. 2018, 61, 185–194. [Google Scholar] [CrossRef]
- Abbasi, F.; Brown, B.W.; Lamendola, C.; McLaughlin, T.; Reaven, G.M. Relationship between obesity, insulin resistance, and coronary heart disease risk. J. Am. Coll. Cardiol. 2002, 40, 937–943. [Google Scholar] [CrossRef]
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: A 26-year follow-up of participants in the framingham heart study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef]
- Kenchaiah, S.; Evans, J.C.; Levy, D.; Wilson, P.W.; Benjamin, E.J.; Larson, M.G.; Kannel, W.B.; Vasan, R.S. Obesity and the risk of heart failure. N. Engl. J. Med. 2002, 347, 305–313. [Google Scholar] [CrossRef]
- Curtis, J.P.; Selter, J.G.; Wang, Y.; Rathore, S.S.; Jovin, I.S.; Jadbabaie, F.; Kosiborod, M.; Portnay, E.L.; Sokol, S.I.; Bader, F.; et al. The obesity paradox: Body mass index and outcomes in patients with heart failure. Arch. Intern. Med. 2005, 165, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Wawrzeńczyk, A.; Anaszewicz, M.; Wawrzeńczyk, A.; Budzyński, J. Clinical significance of nutritional status in patients with chronic heart failure—A systematic review. Heart Fail. Rev. 2019, 24, 671–700. [Google Scholar] [CrossRef]
- Oreopoulos, A.; Padwal, R.; Norris, C.M.; Mullen, J.C.; Pretorius, V.; Kalantar-Zadeh, K. Effect of obesity on short- and long-term mortality postcoronary revascularization: A meta-analysis. Obesity 2008, 16, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Montori, V.M.; Somers, V.K.; Korinek, J.; Thomas, R.J.; Allison, T.G.; Mookadam, F.; Lopez-Jimenez, F. Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: A systematic review of cohort studies. Lancet 2006, 368, 666–678. [Google Scholar] [CrossRef] [PubMed]
- Niedziela, J.; Hudzik, B.; Niedziela, N.; Gąsior, M.; Gierlotka, M.; Wasilewski, J.; Myrda, K.; Lekston, A.; Poloński, L.; Rozentryt, P. The obesity paradox in acute coronary syndrome: A meta-analysis. Eur. J. Epidemiol. 2014, 29, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Milajerdi, A.; Djafarian, K.; Shab-Bidar, S.; Speakman, J.R. Pre- and post-diagnosis body mass index and heart failure mortality: A dose-response meta-analysis of observational studies reveals greater risk of being underweight than being overweight. Obes. Rev. 2018, 20, 252–261. [Google Scholar] [CrossRef]
- Padwal, R.; McAlister, F.A.; McMurray, J.J.; Cowie, M.R.; Rich, M.; Pocock, S.; Swedberg, K.; Maggioni, A.; Gamble, G.; Ariti, C. The obesity paradox in heart failure patients with preserved versus reduced ejection fraction: A meta-analysis of individual patient data. Int. J. Obes. 2014, 38, 1110–1114. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No MINS (n = 207) | MINS (n = 145) | p-Value | |
|---|---|---|---|
| Sex (female) | 41 (19.8%) | 29 (20.0%) | 0.964 |
| Age (years) | 70 (63, 76) | 76 (69, 80) | <0.001 |
| BMI (kg/m2) | 24.1 (21.9, 26.1) | 22.9 (21.1, 25.2) | 0.026 |
| Smoking | 55 (26.6%) | 31 (21.4%) | 0.265 |
| Hypertension | 144 (69.6%) | 111 (76.6%) | 0.149 |
| Diabetes mellitus | 32 (15.5%) | 22 (15.2%) | 0.941 |
| Cerebrovascular accident | 22 (10.6%) | 21 (14.5%) | 0.277 |
| Coronary artery disease | 45 (21.7%) | 36 (24.8%) | 0.498 |
| Previous PCI | 35 (16.9%) | 25 (17.2%) | 0.935 |
| PAOD | 7 (3.4%) | 5 (3.4%) | >0.999 |
| COPD | 6 (2.9%) | 3 (2.1%) | 0.742 |
| Chronic kidney disease | 7 (3.4%) | 23 (15.9%) | <0.001 |
| ESRD | 0 | 5 (3.4%) | 0.011 |
| Anemia | 73 (35.3%) | 81 (55.9%) | <0.001 |
| AAA size (mm) | 60 (52, 70) | 70 (56, 85) | <0.001 |
| Preoperative medications | |||
| Beta-blockers | 64 (30.9%) | 49 (33.8%) | 0.570 |
| Calcium channel blockers | 80 (38.6%) | 59 (40.7%) | 0.700 |
| RAS inhibitors | 84 (40.6%) | 61 (42.1%) | 0.780 |
| Statins | 95 (45.9%) | 66 (45.5%) | 0.944 |
| Diuretics | 22 (10.6%) | 30 (20.7%) | 0.009 |
| Preoperative laboratory results | |||
| WBC count (/μL) | 6860 (5820, 8690) | 7580 (6115, 9660) | 0.005 |
| Hemoglobin (g/dL) | 13.3 (12.3, 14.3) | 12.3 (10.6, 13.9) | <0.001 |
| Platelet count (/μL) | 207,000 (170,000, 244,000) | 189,000 (151,500, 241,000) | 0.014 |
| C-reactive protein (mg/L) | 1.8 (0.8, 4.8) | 4.6 (1.3, 22.5) | <0.001 |
| BUN (mg/dL) | 16.4 (13.1, 19.9) | 20.2 (16.0, 25.5) | <0.001 |
| Creatinine (mg/dL) | 0.89 (0.75, 1.05) | 1.01 (0.83, 1.38) | <0.001 |
| eGFR (mL/min.1.73 m2) | 85 (69, 93) | 70 (48, 85) | <0.001 |
| Intraoperative data | |||
| Administered fluid (mL) | 2550 (1900, 3400) | 2500 (1900, 3300) | 0.902 |
| Urine output (mL) | 305 (150, 500) | 275 (135, 489) | 0.317 |
| Cell saver (mL) | 226 (132, 423) | 238 (112, 384) | 0.737 |
| Bleeding (mL) | 500 (500, 825) | 500 (500, 925) | 0.604 |
| Operative time (min) | 132 (104, 166) | 136 (105, 173) | 0.659 |
| Anesthesia time (min) | 205 (175, 235) | 195 (170, 235) | 0.413 |
| ACC time (min) | 40 (30, 53) | 40 (30, 50) | 0.257 |
| No MINS (n = 207) | MINS (n = 145) | p-Value | |
|---|---|---|---|
| Hospital stay (day) | 9 (7, 13) | 11 (9, 17) | <0.001 |
| ICU stay (day) | 1 (1, 1) | 1 (1, 3) | <0.001 |
| MV duration (h) | 0 (0, 0) | 0 (0, 4) | <0.001 |
| Cerebrovascular accident | 2 (1.0%) | 1 (0.7%) | >0.999 |
| Acute kidney injury | 40 (19.3%) | 51 (35.2%) | 0.001 |
| Myocardial infarction | 0 | 4 (2.8%) | 0.028 |
| 30-day mortality | 1 (0.5%) | 8 (5.5%) | 0.004 |
| 1-year mortality | 3 (1.4%) | 12 (8.3%) | 0.002 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 1.039 (0.964–1.120) | 0.317 | ||
| BMI (kg/m2) | 0.771 (0.610–0.974) | 0.029 | 0.801 (0.632–1.015) | 0.066 |
| Hypertension | 0.293 (0.077–1.116) | 0.072 | ||
| Diabetes mellitus | 0.684 (0.084–5.582) | 0.723 | ||
| Cerebrovascular accident | 2.105 (0.423–10.476) | 0.364 | ||
| Coronary artery disease | 1.699 (0.415–6.949) | 0.461 | ||
| Chronic kidney disease | 0.000 (-) | 0.998 | ||
| Anemia | 4.667 (0.956–22.792) | 0.057 | ||
| AAA size (mm) | 1.030 (0.998–1.063) | 0.063 | ||
| MINS | 12.029 (1.488–97.260) | 0.020 | 10.440 (1.278–85.274) | 0.029 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 1.037 (0.978–1.100) | 0.220 | ||
| BMI (kg/m2) | 0.781 (0.650–0.938) | 0.008 | 0.787 (0.636–0.974) | 0.028 |
| Hypertension | 0.751 (0.250–2.256) | 0.610 | ||
| Diabetes mellitus | 0.843 (0.185–3.847) | 0.826 | ||
| Cerebrovascular accident | 5.405 (1.821–16.045) | 0.002 | 6.692 (2.037–21.986) | 0.002 |
| Coronary artery disease | 1.228 (0.380–3.965) | 0.731 | ||
| Chronic kidney disease | 2.870 (0.763–10.797) | 0.119 | ||
| Anemia | 3.731 (1.164–11.956) | 0.027 | 2.041 (0.584–7.136) | 0.264 |
| AAA size (mm) | 1.011 (0.982–1.040) | 0.454 | ||
| MINS | 6.135 (1.699–22.152) | 0.006 | 5.189 (1.357–19.844) | 0.016 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 1.061 (1.035–1.089) | <0.001 | 1.052 (1.023–1.081) | <0.001 |
| BMI (kg/m2) | 0.940 (0.879–1.005) | 0.068 | ||
| Hypertension | 1.428 (0.879–2.320) | 0.150 | ||
| Diabetes mellitus | 0.978 (0.542–1.764) | 0.941 | ||
| Cerebrovascular accident | 1.424 (0.751–2.700) | 0.279 | ||
| Coronary artery disease | 1.189 (0.720–1.962) | 0.498 | ||
| Chronic kidney disease | 5.386 (2.244–12.928) | <0.001 | 3.755 (1.471–9.581) | 0.006 |
| Anemia | 2.323 (1.505–3.587) | <0.001 | 1.413 (0.852–2.345) | 0.180 |
| AAA size (mm) | 1.031 (1.017–1.045) | <0.001 | 1.027 (1.013–1.042) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, M.I.; Kim, T.-H.; Yoon, H.J.; Song, S.-W.; Min, N.; Lee, J.; Ham, S.Y. Myocardial Injury after Non-Cardiac Surgery in Patients Who Underwent Open Repair for Abdominal Aortic Aneurysm: A Retrospective Study. J. Clin. Med. 2024, 13, 959. https://doi.org/10.3390/jcm13040959
Bae MI, Kim T-H, Yoon HJ, Song S-W, Min N, Lee J, Ham SY. Myocardial Injury after Non-Cardiac Surgery in Patients Who Underwent Open Repair for Abdominal Aortic Aneurysm: A Retrospective Study. Journal of Clinical Medicine. 2024; 13(4):959. https://doi.org/10.3390/jcm13040959
Chicago/Turabian StyleBae, Myung Il, Tae-Hoon Kim, Hei Jin Yoon, Suk-Won Song, Narhyun Min, Jongyun Lee, and Sung Yeon Ham. 2024. "Myocardial Injury after Non-Cardiac Surgery in Patients Who Underwent Open Repair for Abdominal Aortic Aneurysm: A Retrospective Study" Journal of Clinical Medicine 13, no. 4: 959. https://doi.org/10.3390/jcm13040959