
Benchmarking Hospital Practices and Policies on Intrahospital Neurocritical Care Transport: The Safe-Neuro-Transport Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Institutional Review Board Approval
2.2. Survey of Hospital IHT Practices
2.3. Review of Intrahospital Transport Standard Operating Procedures/Hospital Policies
2.4. Statistical Analysis
3. Results
3.1. Participating Institutions
3.2. Clinical Setting of Participating Hospitals Where Critical Care IHT Is Conducted
Portable CT Scan
3.3. Preparation/Assessment of a Patient before the Initiation of IHT
3.4. Equipment and Monitoring during Critical Care
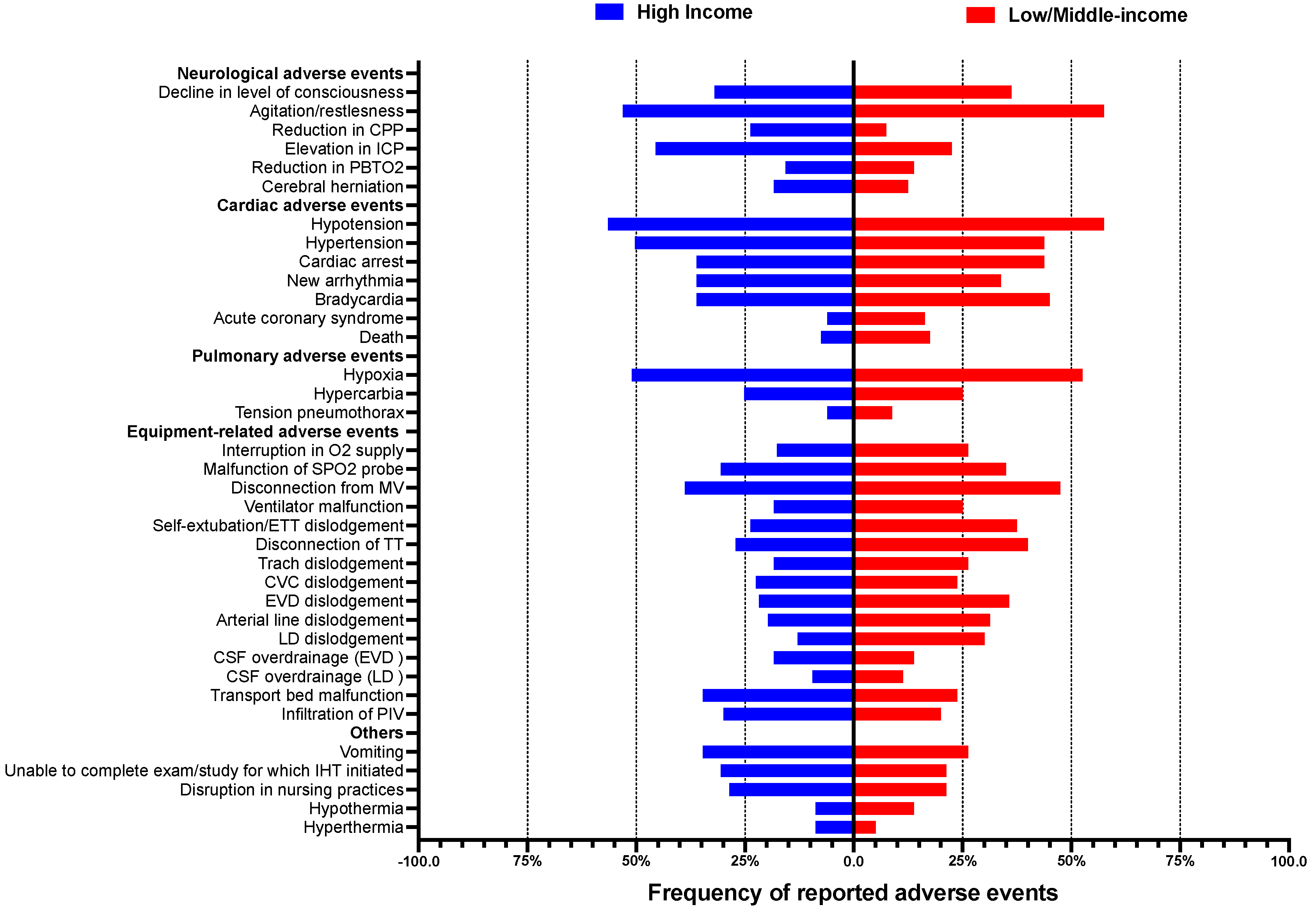
3.5. Reported Neurological and Non-Neurological Adverse Events Occurring during Intrahospital Transport
3.6. Presence of IHT Standard Operating Procedures/Hospital Policies
3.7. Review of IHT SOPs/HPs
3.8. Differences between Country Income Levels and Intrahospital Transport Practices of Critically Ill Patients
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaikittisilpa, N.; Lele, A.V.; Lyons, V.H.; Nair, B.G.; Newman, S.-F.; Blissitt, P.A.; Vavilala, M.S. Risks of Routinely Clamping External Ventricular Drains for Intrahospital Transport in Neurocritically Ill Cerebrovascular Patients. Neurocrit. Care 2017, 26, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Veiga, V.C.; Postalli, N.F.; Alvarisa, T.K.; Travassos, P.P.; Vale, R.T.D.S.; de Oliveira, C.Z.; Rojas, S.S.O. Adverse events during intrahospital transport of critically ill patients in a large hospital. Rev. Bras. Ter. Intensiva 2019, 31, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.M.; Zychowicz, M.E.; Champagne, M.; Thornlow, D.K. Intrahospital Transport of the Critically Ill Adult: A Standardized Evaluation Plan. Dimens. Crit. Care Nurs. 2016, 35, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Lahner, D.; Nikolic, A.; Marhofer, P.; Koinig, H.; Germann, P.; Weinstabl, C.; Krenn, C.G. Incidence of Complications in Intrahospital Transport of Critically Ill Patients--Experience in an Austrian University Hospital. Wien. Klin. Wochenschr. 2007, 119, 412–416. [Google Scholar] [CrossRef]
- Waydhas, C. Intrahospital Transport of Critically Ill Patients. Crit. Care 1999, 3, R83–R89. [Google Scholar] [CrossRef]
- Doring, B.L.; Kerr, M.E.; Lovasik, D.A.; Thayer, T. Factors That Contribute to Complications during Intrahospital Transport of the Critically Ill. J. Neurosci. Nurs. 1999, 31, 80–86. [Google Scholar] [CrossRef]
- Knight, P.H.; Maheshwari, N.; Hussain, J.; Scholl, M.; Hughes, M.; Papadimos, T.J.; Guo, W.A.; Cipolla, J.; Stawicki, S.P.; Latchana, N. Complications during Intrahospital Transport of Critically Ill Patients: Focus on Risk Identification and Prevention. Int. J. Crit. Illn. Inj. Sci. 2015, 5, 256–264. [Google Scholar] [CrossRef]
- Murata, M.; Nakagawa, N.; Kawasaki, T.; Yasuo, S.; Yoshida, T.; Ando, K.; Okamori, S.; Okada, Y. Adverse Events during Intrahospital Transport of Critically Ill Patients: A Systematic Review and Meta-Analysis. Am. J. Emerg. Med. 2022, 52, 13–19. [Google Scholar] [CrossRef]
- Hosmann, A.; Angelmayr, C.; Hopf, A.; Rauscher, S.; Brugger, J.; Ritscher, L.; Bohl, I.; Schnackenburg, P.; Engel, A.; Plöchl, W.; et al. Detrimental Effects of Intrahospital Transport on Cerebral Metabolism in Patients Suffering Severe Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. 2021, 135, 1–8. [Google Scholar] [CrossRef]
- Parmentier-Decrucq, E.; Poissy, J.; Favory, R.; Nseir, S.; Onimus, T.; Guerry, M.-J.; Durocher, A.; Mathieu, D. Adverse Events during Intrahospital Transport of Critically Ill Patients: Incidence and Risk Factors. Ann. Intensive Care 2013, 3, 10. [Google Scholar] [CrossRef]
- Bergman, L.M.; Pettersson, M.E.; Chaboyer, W.P.; Carlström, E.D.; Ringdal, M.L. Safety Hazards during Intrahospital Transport: A Prospective Observational Study. Crit. Care Med. 2017, 45, e1043–e1049. [Google Scholar] [CrossRef] [PubMed]
- Harish, M.M.; Janarthanan, S.; Siddiqui, S.S.; Chaudhary, H.K.; Prabu, N.R.; Divatia, J.V.; Kulkarni, A.P. Complications and Benefits of Intrahospital Transport of Adult Intensive Care Unit Patients. Indian J. Crit. Care Med. 2016, 20, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zhao, Q.; Yang, M.; Xie, X.; Gong, M.; Chen, H. Intrahospital Transport of Critically Ill Patients: A Cross-Sectional Survey of Nurses’ Attitudes and Experiences in Adult Intensive Care Units. J. Adv. Nurs. 2022, 78, 2775–2784. [Google Scholar] [CrossRef]
- Kalisch, B.J.; Kalisch, P.A.; Burns, S.M.; Kocan, M.J.; Prendergast, V. Intrahospital Transport of Neuro ICU Patients. J. Neurosci. Nurs. 1995, 27, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Guidelines Committee of the American College of Critical Care Medicine; Society of Critical Care Medicine and American Association of Critical-Care Nurses Transfer Guidelines Task Force. Guidelines for the Transfer of Critically Ill Patients. Crit. Care Med. 1993, 21, 931–937. [Google Scholar] [CrossRef]
- Warren, J.; Fromm, R.E., Jr.; Orr, R.A.; Rotello, L.C.; Horst, H.M. American College of Critical Care Medicine Guidelines for the Inter- and Intrahospital Transport of Critically Ill Patients. Crit. Care Med. 2004, 32, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Ferdinande, P. Recommendations for intra-hospital transport of the severely head injured patient. Working Group on Neurosurgical Intensive Care of the European Society of Intensive Care Medicine. Intensive Care Med. 1999, 25, 144. [Google Scholar] [CrossRef] [PubMed]
- Fellowships. Available online: http://www.snacc.org/fellowships/ (accessed on 20 July 2022).
- UCNS Fellowship Directory. Available online: https://www.ucns.org/Online/Fellowship_Directory/Online/Fellowship_Directory.aspx?hkey=ca0abd99-aad7-4e31-b735-6baddea75ca2 (accessed on 20 July 2022).
- Lele, A.V.; Wahlster, S.; Alunpipachathai, B.; Awraris Gebrewold, M.; Chou, S.H.-Y.; Crabtree, G.; English, S.; Der-Nigoghossian, C.; Gagnon, D.J.; Kim-Tenser, M.; et al. Perceptions Regarding the SARS-CoV-2 Pandemic’s Impact on Neurocritical Care Delivery: Results from a Global Survey. J. Neurosurg. Anesthesiol. 2022, 34, 209–220. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Thompson, D.M.; Fernald, D.H.; Mold, J.W. Intraclass Correlation Coefficients Typical of Cluster-Randomized Studies: Estimates from the Robert Wood Johnson Prescription for Health Projects. Ann. Fam. Med. 2012, 10, 235–240. [Google Scholar] [CrossRef]
- Barker, N.G. A Practical Introduction to the Bootstrap Using the SAS System. 2005. Available online: https://www.semanticscholar.org/paper/A-Practical-Introduction-to-the-Bootstrap-Using-the-Barker/fbdbad99bdc1b6f235035859a293c17cbffaccef (accessed on 6 December 2022).
- STATA Version 15, Stata Statistical Software; StataCorp LLC: College Station, TX, USA, 2015.
- RStudio. Available online: https://www.rstudio.com/ (accessed on 7 January 2022).
- GraphPad Prism 9 for MacOS; GraphPad Software: San Diego, CA, USA, 2021.
- Kleffmann, J.; Pahl, R.; Deinsberger, W.; Ferbert, A.; Roth, C. Intracranial Pressure Changes during Intrahospital Transports of Neurocritically Ill Patients. Neurocrit. Care 2016, 25, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Peace, K.; Maloney-Wilensky, E.; Frangos, S.; Hujcs, M.; Levine, J.; Kofke, W.A.; Yang, W.; Le Roux, P.D. Portable Head CT Scan and Its Effect on Intracranial Pressure, Cerebral Perfusion Pressure, and Brain Oxygen. J. Neurosurg. 2011, 114, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- LaRovere, K.L.; Brett, M.S.; Tasker, R.C.; Strauss, K.J.; Burns, J.P. Pediatric Critical Nervous System Program Head Computed Tomography Scanning during Pediatric Neurocritical Care: Diagnostic Yield and the Utility of Portable Studies. Neurocrit. Care 2012, 16, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Prabhat, A.M.; Crawford, A.L.; Mazurek, M.H.; Yuen, M.M.; Chavva, I.R.; Ward, A.; Hofmann, W.V., Jr.; Timario, N.; Qualls, S.R.; Helland, J.; et al. Methodology for Low-Field, Portable Magnetic Resonance Neuroimaging at the Bedside. Front. Neurol. 2021, 12, 760321. [Google Scholar] [CrossRef]
- Williams, P.; Karuppiah, S.; Greentree, K.; Darvall, J. A Checklist for Intrahospital Transport of Critically Ill Patients Improves Compliance with Transportation Safety Guidelines. Aust. Crit. Care 2020, 33, 20–24. [Google Scholar] [CrossRef]
- Brunsveld-Reinders, A.H.; Arbous, M.S.; Kuiper, S.G.; de Jonge, E. A Comprehensive Method to Develop a Checklist to Increase Safety of Intra-Hospital Transport of Critically Ill Patients. Crit. Care 2015, 19, 214. [Google Scholar] [CrossRef]
- Hu, Y.; Shi, D.; You, L.; Li, W. Intrahospital Transport of Critically Ill Patients: A Survey of Emergency Nurses. Nurs. Crit. Care 2021, 26, 326–332. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| High-Income Hospital | Low–Middle-Income Hospital | ||
|---|---|---|---|
| n = 246 | n = 103 | n = 143 | |
| Survey Participant Type | |||
| Physicians not in a leadership role | 107 (43.5%) | 43 (41.7%) | 64 (44.8%) |
| Nurse not in a leadership role | 37 (15%) | 30 (20.4%) | 7 (3.8%) |
| Physician in a leadership role (Medical Director) | 73 (29.7%) | 25 (24.3%) | 48 (33.6%) |
| Physician in a leadership role (Program Director) | 26 (8.4%) | 10 (9.7%) | 16 (11.9%) |
| Nurse in a leadership role (ICU Nurse Manager) | 11 (4.5%) | 6 (5.8%) | 5 (3.5%) |
| Advanced Practice Providers | 9 (3.1%) | 4 (3.8%) | 5 (3.5%) |
| Experience at Current Hospital | |||
| ≥5 years | 175 (71.1%) | 74 (42.3%) | 101 (57.7%) |
| <5 years | 71 (28.9%) | 37 (25.2%) | 24 (30%) |
| Hospital Type | |||
| Teaching hospital | 227 (92.3%) | 99 (43.6%) | 128 (56.3%) |
| Comprehensive stroke center | 153 (62.2%) | 90 (58.8%) | 63 (41.2%) |
| Level I trauma center | 94 (38.2%) | 61 (64.9%) | 33 (35.1%) |
| Intensive care unit | |||
| Hospitals with more than one | 197 (80.1%) | 85 (48.2%) | 102 (51.8%) |
| Dedicated neurocritical care unit | 156 (63.4%) | 84 (53.9%) | 72 (46.2%) |
| Presence of IHT SOP/HP | 90 (36.6%) | 44 (42.7%) | 46 (32.2%) |
| Overall (n = 246) | HIC (n = 103) | LMIC (n = 143) | Variation between Country Income Region ICC (95% CI) * | Variation between Country ICC (95% CI) * | |
|---|---|---|---|---|---|
| Vasoactive medication use | 70.60% | 67.40% | 73.80% | 0 (0.00–0.02) | 0.09 (0.00–0.27) |
| Hemodynamic data | 69.85% | 65.90% | 73.80% | 0 (0.00–0.02) | 0.07 (0.00–0.24) |
| Examine equipment necessary | 63.40% | 60.50% | 66.30% | 0 (0.00–0.02) | 0.02 (0.00–0.12) |
| Inspired oxygen setting | 62.90% | 55.80% | 70% | 0 (0.00–0.02) | 0.11 (0.00–0.31) |
| Destination area ready to receive | 61.05% | 55.80% | 66.30% | 0 (0.00–0.01) | 0.06 (0.00–0.20) |
| Identify qualified personnel | 60.95% | 54.40% | 67.50% | 0 (0.00–0.02) | 0.06 (0.00–0.22) |
| Positive end-expiratory pressure settings | 60.15% | 56.50% | 63.80% | 0 (0.00–0.01) | 0.08 (0.00–0.25) |
| Pulse oximetry | 59% | 51% | 67.50% | 0 (0.00–0.02) | 0.06 (0.00–0.23) |
| Transport tolerance/sedation plans | 59% | 53% | 65% | 0 (0.00–0.02) | 0.13 (0.00–0.34) |
| Identify overall risks associated with transport | 54.45% | 47.60% | 61.30% | 0 (0.00–0.02) | 0.18 (0.00–0.38) |
| Interdisciplinary communication | 53.65% | 43.50% | 63.80% | 0 (0.00–0.02) | 0.10 (0.00–0.28) |
| Chest tube status | 52.80% | 45.60% | 60% | 0 (0.00–0.02) | 0.06 (0.00–0.22) |
| Risk stratification (low-/moderate-/high-risk) | 52.25% | 43.50% | 61% | 0 (0.00–0.02) | 0.11 (0.00–0.32) |
| Notify ancillary services of IHT timing | 52.05% | 42.80% | 61.30% | 0 (0.00–0.014) | 0.11 (0.00–0.29) |
| Ventilator settings | 49.85% | 42.20% | 57.50% | 0 (0.00–0.02) | 0.16 (0.00–0.35) |
| Notify the physician accompanying patient | 44.20% | 29.90% | 58.50% | 0.02 (0.00–0.08) | 0.09 (0.00–0.26) |
| Baseline intracranial pressure | 43.20% | 55.10% | 31.30% | 0.08 (0.00–0.19) | 0.18 (0.00–0.41) |
| Peak airway pressure | 43% | 34% | 51.30% | 0 (0.00–0.02) | 0.11 (0.00–0.31) |
| PaO2:FiO2 ratio | 42.55% | 38.80% | 46.30% | 0 (0.00–0.02) | 0.03 (0.00–0.15) |
| Head of bed tolerance for intracranial/cerebral perfusion pressure | 41.95% | 47.60% | 36.30% | 0.09 (0.00–0.22) | 0.10 (0.00–0.29) |
| Indication for IHT | 40.55% | 28.60% | 52.50% | 0 (0.00–0.02) | 0.17 (0.00–0.40) |
| External ventricular drain clamping tolerance | 39.50% | 41.50% | 37.50% | 0.08 (0.00–0.19) | 0.22 (0.00–0.46) |
| Neurological status documentation | 39.05% | 30.60% | 47.50% | 0 (0.00–0.01) | 0.14 (0.00–0.35) |
| Nutrition (NPO status tube feeds) | 38.00% | 27.20% | 48.80% | 0 (0.00–0.03) | 0.07 (0.00–0.24) |
| Neurophysiological monitoring | 36.30% | 38.80% | 33.80% | 0.07 (0.00–0.16) | 0.12 (0.00–0.32) |
| Minute ventilation status | 34.85% | 27.20% | 42.50% | 0 (0.00–0.02) | 0.14 (0.00–0.36) |
| Tracheostomy <7 days | 32.10% | 20.40% | 43.80% | 0.03 (0.00–0.09) | 0.08 (0.00–0.27) |
| Baseline cerebral perfusion pressure | 29.05% | 38.10% | 20% | 0.04 (0.00–0.11) | 0.13 (0.00–0.33) |
| Brain tissue oxygen monitoring | 10.95% | 15.60% | 6.30% | 0.08 (0.00–0.22) | 0.23 (0.00–0.51) |
| Overall | HIC (n = 103) | LMIC (n = 143) | Variation between Country Income Region ICC (95% CI) * | Variation between Country ICC (95% CI) * | |
|---|---|---|---|---|---|
| Pulse oximetry | 93.80% | 89.40% | 98.20% | 0 (0.00–0.01) | 0.14 (0.00–0.35) |
| Ample oxygen source | 89.95% | 87.20% | 92.70% | 0.01 (0.00–0.05) | 0.21 (0.00–0.35) |
| Resuscitation bag | 80.50% | 75.50% | 85.50% | 0 (0.00–0.01) | 0.17 (0.00–0.40) |
| Additional drugs | 70.50% | 62.80% | 78.20% | 0 (0.00–0.02) | 0.09 (0.00–0.27) |
| Resuscitation drugs | 69.80% | 54.20% | 85.40% | 0.01 (0.00–0.04) | 0.19 (0.00–0.41) |
| Transport ventilator | 68.60% | 68.10% | 69.10% | 0.01 (0.00–0.05) | 0.18 (0.00–0.39) |
| Stethoscope | 68.55% | 55.30% | 81.80% | 0.02 (0.00–0.059) | 0.18 (0.00–0.41) |
| Cardiac telemonitoring | 66.85% | 75.50% | 58.20% | 0.09 (0.00–0.24) | 0.20 (0.00–0.04) |
| Endotracheal intubation equipment | 59.65% | 44.70% | 74.60% | 0.03 (0.00–0.09) | 0.30 (0.04–0.56) |
| Manual bag-ventilated | 47.50% | 27.70% | 67.30% | 0.04 (0.00–0.11) | 0.17 (0.00–0.42) |
| Telephone number/pager | 45.45% | 30.90% | 60% | 0 (0.00–0.02) | 0.20 (0.00–0.43) |
| Transport trolley | 42.30% | 26.60% | 58% | 0.03 (0.00–0.08) | 0.25 (0.00–0.05) |
| Intensive care unit ventilator | 38.40% | 27.70% | 49.10% | 0 (0.00–0.02) | 0.23 (0.00–0.05) |
| Defibrillator | 35.50% | 38.30% | 32.70% | 0.02 (0.00–0.09) | 0.16 (0.00–0.38) |
| Elevator key | 34.55% | 30.90% | 38.20% | 0 (0.00–0.02) | 0.17 (0.00–0.39) |
| Intracranial pressure | 32.85% | 45.70% | 20% | 0.06 (0.00–0.18) | 0.28 (0.00–0.55) |
| Portable suction | 29.80% | 28.70% | 30.90% | 0 (0.00–0.02) | 0.15 (0.00–0.38) |
| End-tidal carbon dioxide | 28.60% | 24.50% | 32.70% | 0 (0.00–0.02) | 0.46 (0.07–0.71) |
| Brain tissue oxygenation | 8.60% | 11.70% | 5.50% | Not calculated due to low overall prevalence | Not calculated due to low overall prevalence |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zirpe, K.G.; Alunpipatthanachai, B.; Matin, N.; Gulek, B.G.; Blissitt, P.A.; Palmieri, K.; Rosenblatt, K.; Athiraman, U.; Gollapudy, S.; Theard, M.A.; et al. Benchmarking Hospital Practices and Policies on Intrahospital Neurocritical Care Transport: The Safe-Neuro-Transport Study. J. Clin. Med. 2023, 12, 3183. https://doi.org/10.3390/jcm12093183
Zirpe KG, Alunpipatthanachai B, Matin N, Gulek BG, Blissitt PA, Palmieri K, Rosenblatt K, Athiraman U, Gollapudy S, Theard MA, et al. Benchmarking Hospital Practices and Policies on Intrahospital Neurocritical Care Transport: The Safe-Neuro-Transport Study. Journal of Clinical Medicine. 2023; 12(9):3183. https://doi.org/10.3390/jcm12093183
Chicago/Turabian StyleZirpe, Kapil G., Bhunyawee Alunpipatthanachai, Nassim Matin, Bernice G. Gulek, Patricia A. Blissitt, Katherine Palmieri, Kathryn Rosenblatt, Umeshkumar Athiraman, Suneeta Gollapudy, Marie Angele Theard, and et al. 2023. "Benchmarking Hospital Practices and Policies on Intrahospital Neurocritical Care Transport: The Safe-Neuro-Transport Study" Journal of Clinical Medicine 12, no. 9: 3183. https://doi.org/10.3390/jcm12093183