

Widespread Intra- and Inter-Network Dysconnectivity among Large-Scale Resting State Networks in Schizophrenia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Imaging Data Acquisition and Preprocessing
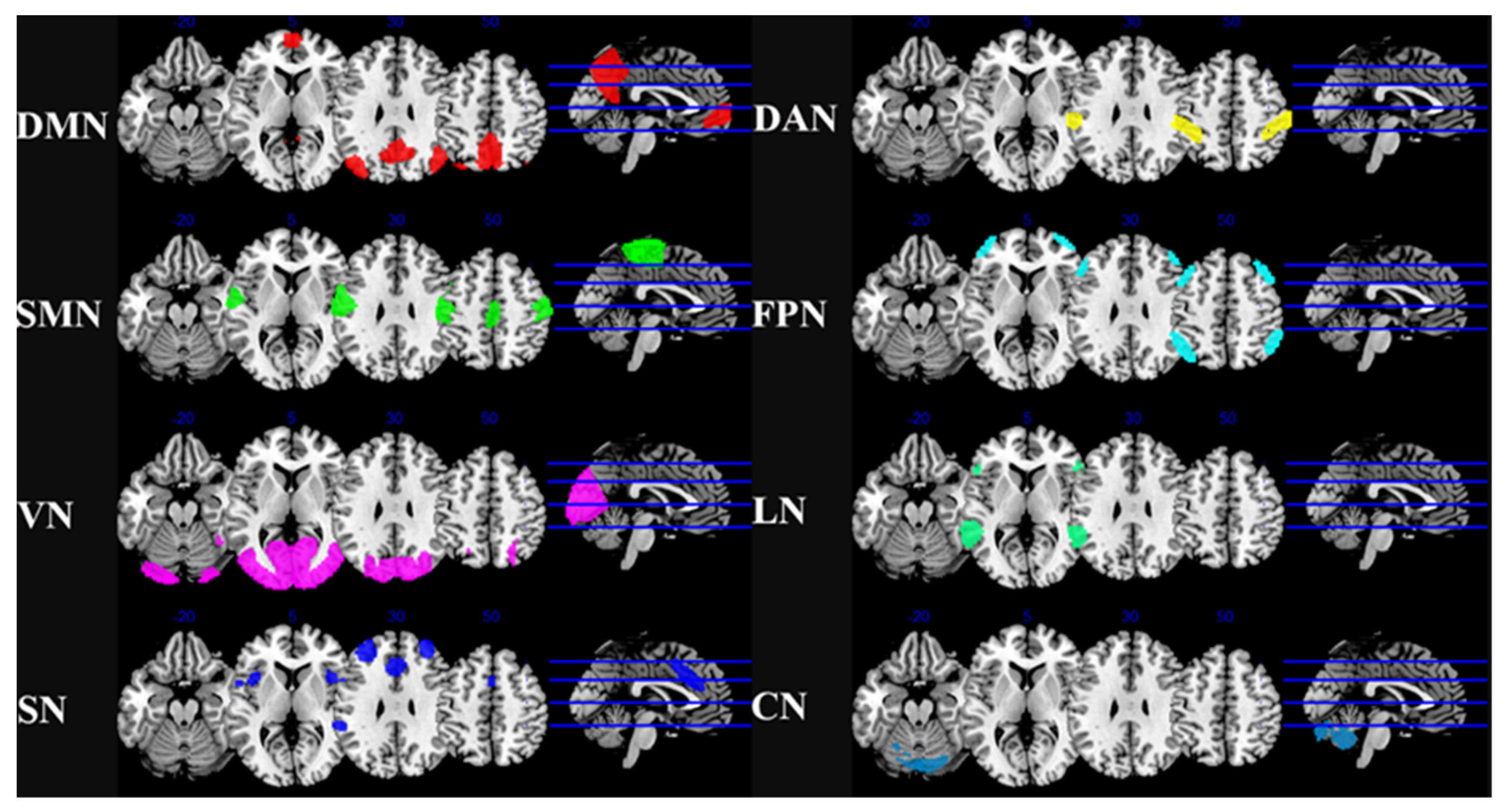
2.4. ROI-to-ROI Whole Brain Functional Connectivity Analysis
2.5. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
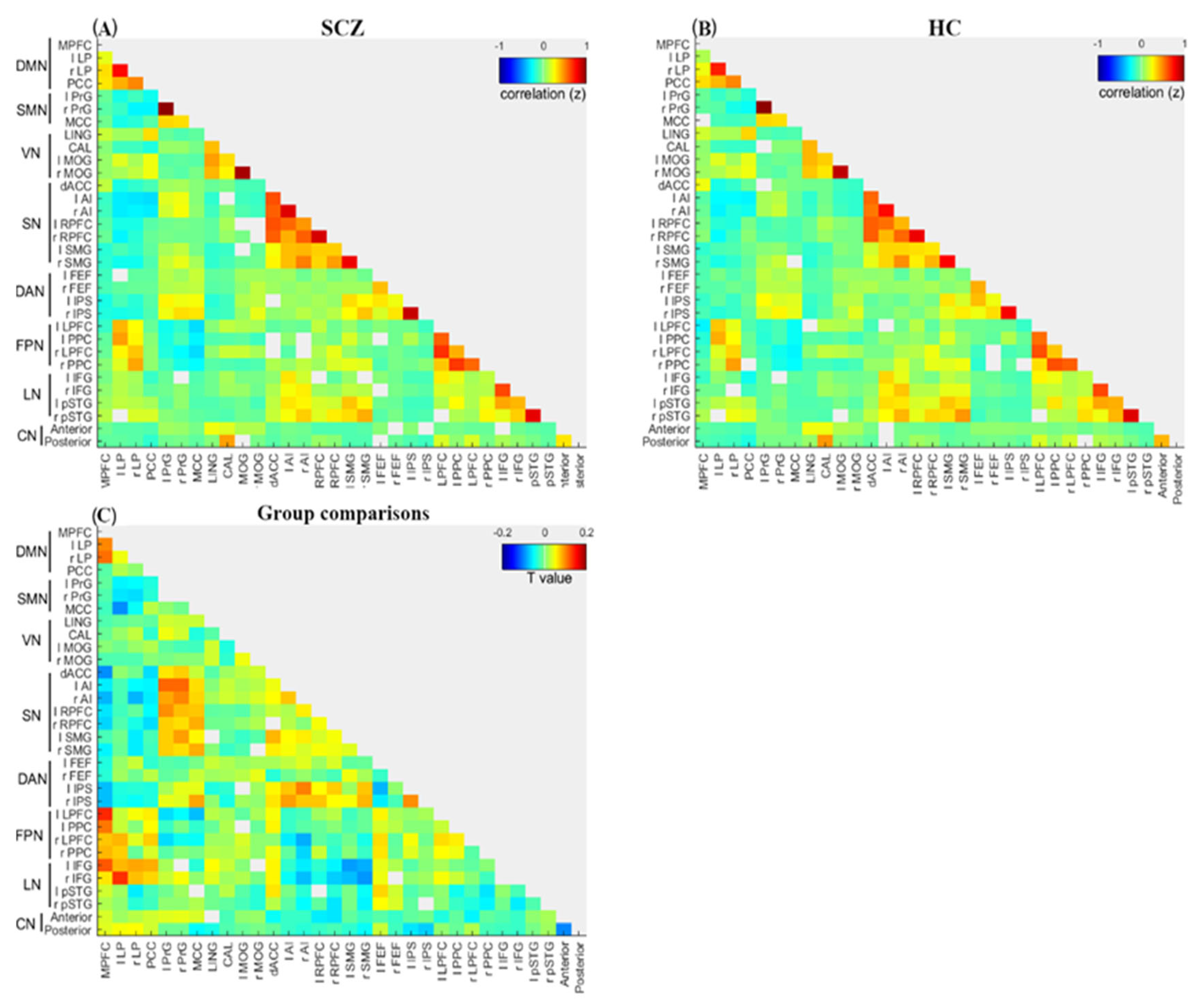
3.2. Overall Characteristics of Intra- and Inter-Network Connectivity
3.2.1. Intra-Network Connectivity
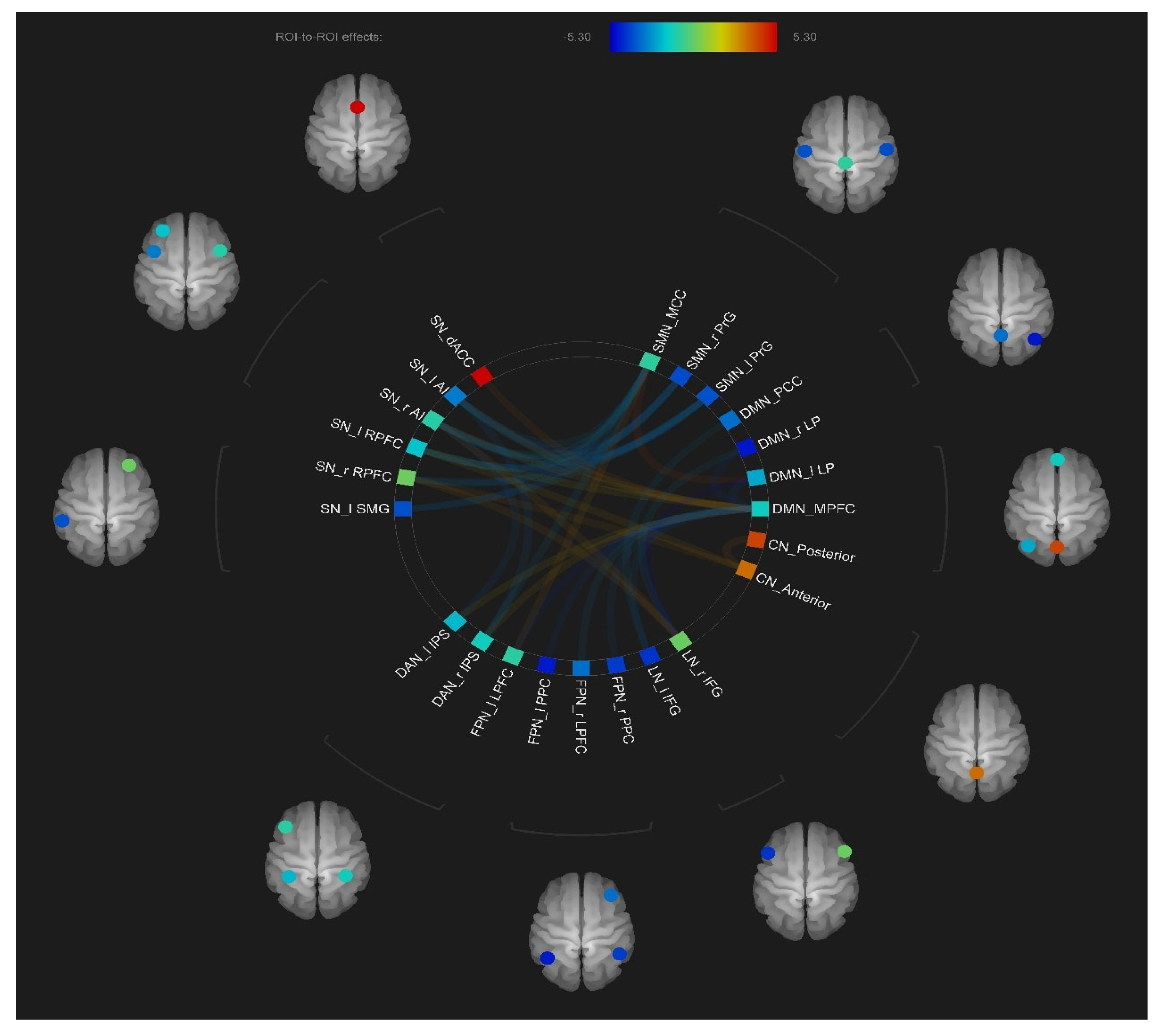
3.2.2. Inter-Network Connectivity
3.3. Relationships between Functional Connectivity Patterns and Clinical Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SCZ | Schizophrenia |
| HC | Healthy control |
| RSN | Resting-state network |
| FC | Functional connectivity |
| ROI | Region of interest |
| DMN | Default mode network |
| SN | Salience network |
| FPN | Frontoparietal network |
| CN | Cerebellar network |
| CEN | Central executive network |
| DAN | Dorsal attention network |
| SMN | Sensorimotor network |
| VN | Visual network |
| PANSS | Positive and Negative Syndrome Scale |
| MPFC | Medial prefrontal cortex |
| LP | Lateral parietal |
| PCC | Posterior cingulate cortex |
| PrG | Precentral gyrus |
| MCC | Middle cingulate cortex |
| dACC | Dorsal Anterior cingulate cortex |
| AI | Anterior insula |
| RPFC | Rostral prefrontal cortex |
| SMG | Supramarginal Gyrus |
| LPFC | Lateral prefrontal cortex |
| PPC | Posterior parietal cortex |
| IFG | Inferior frontal gyrus |
| PSTG | Posterior superior temporal gyrus |
| Anterior | Cerebellar anterior lobules |
| Posterior | Cerebellar posterior lobules |
References
- Insel, T.R. Rethinking Schizophrenia. Nature 2010, 468, 187–193. [Google Scholar] [CrossRef]
- McCutcheon, R.A.; Reis Marques, T.; Howes, O.D. Schizophrenia-An Overview. JAMA Psychiatry 2020, 77, 201–210. [Google Scholar] [CrossRef]
- Friston, K.; Brown, H.R.; Siemerkus, J.; Stephan, K.E. The Dysconnection Hypothesis (2016). Schizophr. Res. 2016, 176, 83–94. [Google Scholar] [CrossRef]
- Jiang, T.; Zhou, Y.; Liu, B.; Liu, Y.; Song, M. Brainnetome-Wide Association Studies in Schizophrenia: The Advances and Future. Neurosci. Biobehav. Rev. 2013, 37, 2818–2835. [Google Scholar] [CrossRef]
- Stephan, K.E.; Friston, K.J.; Frith, C.D. Dysconnection in Schizophrenia: From Abnormal Synaptic Plasticity to Failures of Self-Monitoring. Schizophr. Bull. 2009, 35, 509–527. [Google Scholar] [CrossRef]
- Fornito, A.; Bullmore, E.T. Connectomics: A New Paradigm for Understanding Brain Disease. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2015, 25, 733–748. [Google Scholar] [CrossRef]
- Menon, V. Large-Scale Brain Networks and Psychopathology: A Unifying Triple Network Model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef]
- Meyer-Lindenberg, A. From Maps to Mechanisms through Neuroimaging of Schizophrenia. Nature 2010, 468, 194–202. [Google Scholar] [CrossRef]
- Littow, H.; Huossa, V.; Karjalainen, S.; Jääskeläinen, E.; Haapea, M.; Miettunen, J.; Tervonen, O.; Isohanni, M.; Nikkinen, J.; Veijola, J.; et al. Aberrant Functional Connectivity in the Default Mode and Central Executive Networks in Subjects with Schizophrenia—A Whole-Brain Resting-State ICA Study. Front. Psychiatry 2015, 6, 26. [Google Scholar] [CrossRef]
- Squire, L.R.; Wixted, J.T.; Clark, R.E. Recognition Memory and the Medial Temporal Lobe: A New Perspective. Nat. Rev. Neurosci. 2007, 8, 872–883. [Google Scholar] [CrossRef]
- Bastos-Leite, A.J.; Ridgway, G.R.; Silveira, C.; Norton, A.; Reis, S.; Friston, K.J. Dysconnectivity Within the Default Mode in First-Episode Schizophrenia: A Stochastic Dynamic Causal Modeling Study with Functional Magnetic Resonance Imaging. Schizophr. Bull. 2015, 41, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Wang, J.; Luo, X.; Chen, G.; Huang, H.; Huang, R.; Huang, L.; Wang, Y. Abnormalities of Intrinsic Regional Brain Activity in First-Episode and Chronic Schizophrenia: A Meta-Analysis of Resting-State Functional MRI. J. Psychiatry Neurosci. 2020, 45, 55–68. [Google Scholar] [CrossRef]
- Zhang, Y.; Dai, Z.; Chen, Y.; Sim, K.; Sun, Y.; Yu, R. Altered Intra- and Inter-Hemispheric Functional Dysconnectivity in Schizophrenia. Brain Imaging Behav. 2019, 13, 1220–1235. [Google Scholar] [CrossRef]
- Horwitz, B.; Rowe, J.B. Functional Biomarkers for Neurodegenerative Disorders Based on the Network Paradigm. Prog. Neurobiol. 2011, 95, 505. [Google Scholar] [CrossRef]
- Wu, D.; Jiang, T. Schizophrenia-Related Abnormalities in the Triple Network: A Meta-Analysis of Working Memory Studies. Brain Imaging Behav. 2020, 14, 971–980. [Google Scholar] [CrossRef]
- Liemburg, E.J.; Vercammen, A.; Ter Horst, G.J.; Curcic-Blake, B.; Knegtering, H.; Aleman, A. Abnormal Connectivity between Attentional, Language and Auditory Networks in Schizophrenia. Schizophr. Res. 2012, 135, 15–22. [Google Scholar] [CrossRef]
- Dixon, M.L.; Andrews-Hanna, J.R.; Spreng, R.N.; Irving, Z.C.; Mills, C.; Girn, M.; Christoff, K. Interactions between the Default Network and Dorsal Attention Network Vary across Default Subsystems, Time, and Cognitive States. NeuroImage 2017, 147, 632–649. [Google Scholar] [CrossRef]
- Kaufmann, T.; Skåtun, K.C.; Alnæs, D.; Doan, N.T.; Duff, E.P.; Tønnesen, S.; Roussos, E.; Ueland, T.; Aminoff, S.R.; Lagerberg, T.V.; et al. Disintegration of Sensorimotor Brain Networks in Schizophrenia. Schizophr. Bull. 2015, 41, 1326–1335. [Google Scholar] [CrossRef]
- Schiwy, L.C.; Forlim, C.G.; Fischer, D.J.; Kühn, S.; Becker, M.; Gallinat, J. Aberrant Functional Connectivity within the Salience Network Is Related to Cognitive Deficits and Disorganization in Psychosis. Schizophr. Res. 2022, 246, 103–111. [Google Scholar] [CrossRef]
- Chahine, G.; Richter, A.; Wolter, S.; Goya-Maldonado, R.; Gruber, O. Disruptions in the Left Frontoparietal Network Underlie Resting State Endophenotypic Markers in Schizophrenia. Hum. Brain Mapp. 2016, 38, 1741–1750. [Google Scholar] [CrossRef]
- Zhuo, C.; Wang, C.; Wang, L.; Guo, X.; Xu, Q.; Liu, Y.; Zhu, J. Altered Resting-State Functional Connectivity of the Cerebellum in Schizophrenia. Brain Imaging Behav. 2018, 12, 383–389. [Google Scholar] [CrossRef]
- Berman, R.A.; Gotts, S.J.; McAdams, H.M.; Greenstein, D.; Lalonde, F.; Clasen, L.; Watsky, R.E.; Shora, L.; Ordonez, A.E.; Raznahan, A.; et al. Disrupted Sensorimotor and Social–Cognitive Networks Underlie Symptoms in Childhood-Onset Schizophrenia. Brain 2016, 139, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Supekar, K.; Cai, W.; Krishnadas, R.; Palaniyappan, L.; Menon, V. Dysregulated Brain Dynamics in a Triple-Network Saliency Model of Schizophrenia and Its Relation to Psychosis. Biol. Psychiatry 2019, 85, 60–69. [Google Scholar] [CrossRef]
- Liang, S.; Wang, Q.; Greenshaw, A.J.; Li, X.; Deng, W.; Ren, H.; Zhang, C.; Yu, H.; Wei, W.; Zhang, Y.; et al. Aberrant Triple-Network Connectivity Patterns Discriminate Biotypes of First-Episode Medication-Naive Schizophrenia in Two Large Independent Cohorts. Neuropsychopharmacology 2021, 46, 1502–1509. [Google Scholar] [CrossRef]
- Manoliu, A.; Riedl, V.; Zherdin, A.; Mühlau, M.; Schwerthöffer, D.; Scherr, M.; Peters, H.; Zimmer, C.; Förstl, H.; Bäuml, J.; et al. Aberrant Dependence of Default Mode/Central Executive Network Interactions on Anterior Insular Salience Network Activity in Schizophrenia. Schizophr. Bull. 2014, 40, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Shen, H.; Wang, L.; Liu, Z.; Xin, W.; Hu, D.; Miao, D. Altered Default Mode and Fronto-Parietal Network Subsystems in Patients with Schizophrenia and Their Unaffected Siblings. Brain Res. 2014, 1562, 87–99. [Google Scholar] [CrossRef]
- Dixon, M.L.; De La Vega, A.; Mills, C.; Andrews-Hanna, J.; Spreng, R.N.; Cole, M.W.; Christoff, K. Heterogeneity within the Frontoparietal Control Network and Its Relationship to the Default and Dorsal Attention Networks. Proc. Natl. Acad. Sci. USA 2018, 115, E1598–E1607. [Google Scholar] [CrossRef]
- Yamashita, M.; Shimokawa, T.; Takahashi, S.; Yamada, S.; Terada, M.; Ukai, S.; Tanemura, R. Cognitive Functions Relating to Aberrant Interactions between Task-Positive and Task-Negative Networks: Resting FMRI Study of Patients with Schizophrenia. Appl. Neuropsychol. Adult 2022, 29, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- McNabb, C.B.; Sundram, F.; Soosay, I.; Kydd, R.R.; Russell, B.R. Increased Sensorimotor Network Connectivity Associated with Clozapine Eligibility in People with Schizophrenia. Psychiatry Res. Neuroimaging 2018, 275, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, W.; Deng, J.; Shi, Y.; Nie, W.; Luo, S.; Zhang, H. Exploring Dysconnectivity of the Large-Scale Neurocognitive Network across Psychiatric Disorders Using Spatiotemporal Constrained Nonnegative Matrix Factorization Method. Cereb. Cortex 2022, 32, 4576–4591. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Liu, F.; Chen, J.; Wu, R.; Zhang, Z.; Yu, M.; Xiao, C.; Zhao, J. Resting-State Cerebellar-Cerebral Networks Are Differently Affected in First-Episode, Drug-Naive Schizophrenia Patients and Unaffected Siblings. Sci. Rep. 2015, 5, 17275. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zou, F.; Shao, Y.; Ye, E.; Jin, X.; Tan, S.; Hu, D.; Yang, Z. Disruptive Changes of Cerebellar Functional Connectivity with the Default Mode Network in Schizophrenia. Schizophr. Res. 2014, 160, 67–72. [Google Scholar] [CrossRef]
- Joo, S.W.; Yoon, W.; Jo, Y.T.; Kim, H.; Kim, Y.; Lee, J. Aberrant Executive Control and Auditory Networks in Recent-Onset Schizophrenia. Neuropsychiatr. Dis. Treat. 2020, 16, 1561–1570. [Google Scholar] [CrossRef]
- Bluhm, R.; Miller, J.E.; Lanius, R.; Osuch, E.; Boksman, K.; Neufeld, R.; Théberge, J.; Schaefer, B.; Williamson, P. Spontaneous Low-Frequency Fluctuations in the BOLD Signal in Schizophrenic Patients: Anomalies in the Default Network. Schizophr. Bull. 2007, 33, 1004–1012. [Google Scholar] [CrossRef]
- Moran, L.V.; Tagamets, M.A.; Sampath, H.; O’Donnell, A.; Stein, E.A.; Kochunov, P.; Hong, L.E. Disruption of Anterior Insula Modulation of Large-Scale Brain Networks in Schizophrenia. Biol. Psychiatry 2013, 74, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, A.M.; Riedel, P.; Lee, J.; Reavis, E.A.; Green, M.F. Linking Resting-state Networks and Social Cognition in Schizophrenia and Bipolar Disorder. Hum. Brain Mapp. 2019, 40, 4703–4715. [Google Scholar] [CrossRef] [PubMed]
- Mamah, D.; Barch, D.M.; Repovš, G. Resting State Functional Connectivity of Five Neural Networks in Bipolar Disorder and Schizophrenia. J. Affect. Disord. 2013, 150, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Peterburs, J.; Desmond, J.E. The Role of the Human Cerebellum in Performance Monitoring. Curr. Opin. Neurobiol. 2016, 40, 38–44. [Google Scholar] [CrossRef]
- Doucet, G.; Naveau, M.; Petit, L.; Delcroix, N.; Zago, L.; Crivello, F.; Jobard, G.; Tzourio-Mazoyer, N.; Mazoyer, B.; Mellet, E.; et al. Brain Activity at Rest: A Multiscale Hierarchical Functional Organization. J. Neurophysiol. 2011, 105, 2753–2763. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A Functional Connectivity Toolbox for Correlated and Anticorrelated Brain Networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef]
- Behzadi, Y.; Restom, K.; Liau, J.; Liu, T.T. A Component Based Noise Correction Method (CompCor) for BOLD and Perfusion Based FMRI. NeuroImage 2007, 37, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Tu, Y.; Gollub, R.L.; Ortiz, A.; Napadow, V.; Yu, S.; Wilson, G.; Park, J.; Lang, C.; Jung, M.; et al. Visual Network Alterations in Brain Functional Connectivity in Chronic Low Back Pain: A Resting State Functional Connectivity and Machine Learning Study. NeuroImage Clin. 2019, 22, 101775. [Google Scholar] [CrossRef]
- Hur, J.-W.; Kim, T.; Cho, K.I.K.; Kwon, J.S. Attenuated Resting-State Functional Anticorrelation between Attention and Executive Control Networks in Schizotypal Personality Disorder. J. Clin. Med. 2021, 10, 312. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The Brain’s Default Network: Anatomy, Function, and Relevance to Disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Raichle, M.E. The Brain’s Default Mode Network. Annu. Rev. Neurosci. 2015, 38, 433–447. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Thermenos, H.W.; Milanovic, S.; Tsuang, M.T.; Faraone, S.V.; McCarley, R.W.; Shenton, M.E.; Green, A.I.; Nieto-Castanon, A.; LaViolette, P.; et al. Hyperactivity and Hyperconnectivity of the Default Network in Schizophrenia and in First-Degree Relatives of Persons with Schizophrenia. Proc. Natl. Acad. Sci. USA 2009, 106, 1279–1284. [Google Scholar] [CrossRef]
- Galindo, L.; Bergé, D.; Murray, G.K.; Mané, A.; Bulbena, A.; Pérez, V.; Vilarroya, O. Default Mode Network Aberrant Connectivity Associated with Neurological Soft Signs in Schizophrenia Patients and Unaffected Relatives. Front. Psychiatry 2018, 8, 298. [Google Scholar] [CrossRef]
- Liu, H.; Kaneko, Y.; Ouyang, X.; Li, L.; Hao, Y.; Chen, E.Y.H.; Jiang, T.; Zhou, Y.; Liu, Z. Schizophrenic Patients and Their Unaffected Siblings Share Increased Resting-State Connectivity in the Task-Negative Network but Not Its Anticorrelated Task-Positive Network. Schizophr. Bull. 2012, 38, 285–294. [Google Scholar] [CrossRef]
- Shim, G.; Oh, J.S.; Jung, W.H.; Jang, J.H.; Choi, C.-H.; Kim, E.; Park, H.-Y.; Choi, J.-S.; Jung, M.H.; Kwon, J.S. Altered Resting-State Connectivity in Subjects at Ultra-High Risk for Psychosis: An FMRI Study. Behav. Brain Funct. BBF 2010, 6, 58. [Google Scholar] [CrossRef]
- Exner, C.; Weniger, G.; Irle, E. Cerebellar Lesions in the PICA but Not SCA Territory Impair Cognition. Neurology 2004, 63, 2132–2135. [Google Scholar] [CrossRef]
- O’Neill, A.; Mechelli, A.; Bhattacharyya, S. Dysconnectivity of Large-Scale Functional Networks in Early Psychosis: A Meta-Analysis. Schizophr. Bull. 2019, 45, 579–590. [Google Scholar] [CrossRef]
- Laidi, C.; d’Albis, M.-A.; Wessa, M.; Linke, J.; Phillips, M.; Delavest, M.; Bellivier, F.; Versace, A.; Almeida, J.; Sarrazin, S.; et al. Cerebellar Volume in Schizophrenia and Bipolar I Disorder with and without Psychotic Features. Acta Psychiatr. Scand. 2015, 131, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.A.; Mittal, V.A. Dysfunctional Activation of the Cerebellum in Schizophrenia: A Functional Neuroimaging Meta-Analysis. Clin. Psychol. Sci. J. Assoc. Psychol. Sci. 2015, 3, 545–566. [Google Scholar] [CrossRef]
- McKiernan, K.A.; D’Angelo, B.R.; Kaufman, J.N.; Binder, J.R. Interrupting the “Stream of Consciousness”: An FMRI Investigation. NeuroImage 2006, 29, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable Intrinsic Connectivity Networks for Salience Processing and Executive Control. J. Neurosci. Off. J. Soc. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Dong, D.; Wang, Y.; Chang, X.; Luo, C.; Yao, D. Dysfunction of Large-Scale Brain Networks in Schizophrenia: A Meta-Analysis of Resting-State Functional Connectivity. Schizophr. Bull. 2018, 44, 168–181. [Google Scholar] [CrossRef]
- Wang, Y.-M.; Zou, L.-Q.; Xie, W.-L.; Yang, Z.-Y.; Zhu, X.-Z.; Cheung, E.F.C.; Sørensen, T.A.; Møller, A.; Chan, R.C.K. Altered Functional Connectivity of the Default Mode Network in Patients With Schizo-Obsessive Comorbidity: A Comparison Between Schizophrenia and Obsessive-Compulsive Disorder. Schizophr. Bull. 2019, 45, 199–210. [Google Scholar] [CrossRef]
- Menon, M.; Schmitz, T.W.; Anderson, A.K.; Graff, A.; Korostil, M.; Mamo, D.; Gerretsen, P.; Addington, J.; Remington, G.; Kapur, S. Exploring the Neural Correlates of Delusions of Reference. Biol. Psychiatry 2011, 70, 1127–1133. [Google Scholar] [CrossRef]
- Schmitz, T.W.; Johnson, S.C. Relevance to Self: A Brief Review and Framework of Neural Systems Underlying Appraisal. Neurosci. Biobehav. Rev. 2007, 31, 585–596. [Google Scholar] [CrossRef]
- Augustine, J.R. Circuitry and Functional Aspects of the Insular Lobe in Primates Including Humans. Brain Res. Brain Res. Rev. 1996, 22, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Bamiou, D.-E.; Musiek, F.E.; Luxon, L.M. The Insula (Island of Reil) and Its Role in Auditory Processing. Literature Review. Brain Res. Brain Res. Rev. 2003, 42, 143–154. [Google Scholar] [CrossRef]
- Wylie, K.P.; Tregellas, J.R. The Role of the Insula in Schizophrenia. Schizophr. Res. 2010, 123, 93–104. [Google Scholar] [CrossRef]
- Pankow, A.; Katthagen, T.; Diner, S.; Deserno, L.; Boehme, R.; Kathmann, N.; Gleich, T.; Gaebler, M.; Walter, H.; Heinz, A.; et al. Aberrant Salience Is Related to Dysfunctional Self-Referential Processing in Psychosis. Schizophr. Bull. 2016, 42, 67–76. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, Y.; Liang, X.; Li, D.; Zheng, Y.; Zhang, H.; Cui, Y.; Chen, J.; Liu, J.; Qiu, S. Altered Resting-State Functional Connectivity of Multiple Networks and Disrupted Correlation With Executive Function in Major Depressive Disorder. Front. Neurol. 2020, 11, 272. [Google Scholar] [CrossRef]
- Pearlson, G.D. Etiologic, Phenomenologic, and Endophenotypic Overlap of Schizophrenia and Bipolar Disorder. Annu. Rev. Clin. Psychol. 2015, 11, 251–281. [Google Scholar] [CrossRef]
- Hare, S.M.; Ford, J.M.; Mathalon, D.H.; Damaraju, E.; Bustillo, J.; Belger, A.; Lee, H.J.; Mueller, B.A.; Lim, K.O.; Brown, G.G.; et al. Salience-Default Mode Functional Network Connectivity Linked to Positive and Negative Symptoms of Schizophrenia. Schizophr. Bull. 2019, 45, 892–901. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E.; Garety, P.; Fowler, D.; Freeman, D.; Dunn, G.; Bebbington, P. Cognitive, Emotional, and Social Processes in Psychosis: Refining Cognitive Behavioral Therapy for Persistent Positive Symptoms. Schizophr. Bull. 2006, 32 (Suppl. 1), S24–S31. [Google Scholar] [CrossRef]
- Spreng, R.N.; Stevens, W.D.; Chamberlain, J.P.; Gilmore, A.W.; Schacter, D.L. Default Network Activity, Coupled with the Frontoparietal Control Network, Supports Goal-Directed Cognition. NeuroImage 2010, 53, 303–317. [Google Scholar] [CrossRef] [PubMed]
- Pu, W.; Luo, Q.; Palaniyappan, L.; Xue, Z.; Yao, S.; Feng, J.; Liu, Z. Failed Cooperative, but Not Competitive, Interaction between Large-Scale Brain Networks Impairs Working Memory in Schizophrenia. Psychol. Med. 2016, 46, 1211–1224. [Google Scholar] [CrossRef]
- Sha, Z.; Wager, T.D.; Mechelli, A.; He, Y. Common Dysfunction of Large-Scale Neurocognitive Networks Across Psychiatric Disorders. Biol. Psychiatry 2019, 85, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Tu, P.-C.; Lee, Y.-C.; Chen, Y.-S.; Li, C.-T.; Su, T.-P. Schizophrenia and the Brain’s Control Network: Aberrant within- and between-Network Connectivity of the Frontoparietal Network in Schizophrenia. Schizophr. Res. 2013, 147, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Williamson, P. Are Anticorrelated Networks in the Brain Relevant to Schizophrenia? Schizophr. Bull. 2007, 33, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zeng, L.-L.; Chen, Y.; Yin, H.; Tan, Q.; Hu, D. Evidence of a Dissociation Pattern in Default Mode Subnetwork Functional Connectivity in Schizophrenia. Sci. Rep. 2015, 5, 14655. [Google Scholar] [CrossRef]
- Dosenbach, N.U.F.; Fair, D.A.; Miezin, F.M.; Cohen, A.L.; Wenger, K.K.; Dosenbach, R.A.T.; Fox, M.D.; Snyder, A.Z.; Vincent, J.L.; Raichle, M.E.; et al. Distinct Brain Networks for Adaptive and Stable Task Control in Humans. Proc. Natl. Acad. Sci. USA 2007, 104, 11073–11078. [Google Scholar] [CrossRef]
- Duan, M.; Jiang, Y.; Chen, X.; Luo, C.; Yao, D. [Degree centrality of the functional network in schizophrenia patients]. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi J. Biomed. Eng. Shengwu Yixue Gongchengxue Zazhi 2017, 34, 837–841. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, W.; Sun, Y.; Hu, M.; Chen, A. Aberrant Intra-Salience Network Dynamic Functional Connectivity Impairs Large-Scale Network Interactions in Schizophrenia. Neuropsychologia 2016, 93, 262–270. [Google Scholar] [CrossRef]
- Menon, V.; Uddin, L.Q. Saliency, Switching, Attention and Control: A Network Model of Insula Function. Brain Struct. Funct. 2010, 214, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Uddin, L.Q. Salience Processing and Insular Cortical Function and Dysfunction. Nat. Rev. Neurosci. 2015, 16, 55–61. [Google Scholar] [CrossRef]
- Corbetta, M.; Shulman, G.L. Control of Goal-Directed and Stimulus-Driven Attention in the Brain. Nat. Rev. Neurosci. 2002, 3, 201–215. [Google Scholar] [CrossRef]
- Luck, S.J.; Gold, J.M. The Construct of Attention in Schizophrenia. Biol. Psychiatry 2008, 64, 34–39. [Google Scholar] [CrossRef]
- Sato, Y.; Yabe, H.; Todd, J.; Michie, P.; Shinozaki, N.; Sutoh, T.; Hiruma, T.; Nashida, T.; Matsuoka, T.; Kaneko, S. Impairment in Activation of a Frontal Attention-Switch Mechanism in Schizophrenic Patients. Biol. Psychol. 2003, 62, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Arkin, S.C.; Ruiz-Betancourt, D.; Jamerson, E.C.; Smith, R.T.; Strauss, N.E.; Klim, C.C.; Javitt, D.C.; Patel, G.H. Deficits and Compensation: Attentional Control Cortical Networks in Schizophrenia. NeuroImage Clin. 2020, 27, 102348. [Google Scholar] [CrossRef]
- Zhou, Y.; Zeidman, P.; Wu, S.; Razi, A.; Chen, C.; Yang, L.; Zou, J.; Wang, G.; Wang, H.; Friston, K.J. Altered Intrinsic and Extrinsic Connectivity in Schizophrenia. NeuroImage Clin. 2017, 17, 704–716. [Google Scholar] [CrossRef]
- Lefort-Besnard, J.; Bassett, D.S.; Smallwood, J.; Margulies, D.S.; Derntl, B.; Gruber, O.; Aleman, A.; Jardri, R.; Varoquaux, G.; Thirion, B.; et al. Different Shades of Default Mode Disturbance in Schizophrenia: Subnodal Covariance Estimation in Structure and Function. Hum. Brain Mapp. 2018, 39, 644–661. [Google Scholar] [CrossRef]
- Li, S.; Hu, N.; Zhang, W.; Tao, B.; Dai, J.; Gong, Y.; Tan, Y.; Cai, D.; Lui, S. Dysconnectivity of Multiple Brain Networks in Schizophrenia: A Meta-Analysis of Resting-State Functional Connectivity. Front. Psychiatry 2019, 10, 482. [Google Scholar] [CrossRef]
- Cauda, F.; D’Agata, F.; Sacco, K.; Duca, S.; Geminiani, G.; Vercelli, A. Functional Connectivity of the Insula in the Resting Brain. NeuroImage 2011, 55, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Bulbul, O.; Kurt, E.; Ulasoglu-Yildiz, C.; Demiralp, T.; Ucok, A. Altered Resting State Functional Connectivity and Its Correlation with Cognitive Functions at Ultra High Risk for Psychosis. Psychiatry Res. Neuroimaging 2022, 321, 111444. [Google Scholar] [CrossRef]
- Andreasen, N.C.; O’Leary, D.S.; Cizadlo, T.; Arndt, S.; Rezai, K.; Ponto, L.L.; Watkins, G.L.; Hichwa, R.D. Schizophrenia and Cognitive Dysmetria: A Positron-Emission Tomography Study of Dysfunctional Prefrontal-Thalamic-Cerebellar Circuitry. Proc. Natl. Acad. Sci. USA 1996, 93, 9985–9990. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, N.C.; Paradiso, S.; O’Leary, D.S. “Cognitive Dysmetria” as an Integrative Theory of Schizophrenia: A Dysfunction in Cortical-Subcortical-Cerebellar Circuitry? Schizophr. Bull. 1998, 24, 203–218. [Google Scholar] [CrossRef]
- Chenji, S.; Jha, S.; Lee, D.; Brown, M.; Seres, P.; Mah, D.; Kalra, S. Investigating Default Mode and Sensorimotor Network Connectivity in Amyotrophic Lateral Sclerosis. PLoS ONE 2016, 11, e0157443. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.D.; Raichle, M.E. Spontaneous Fluctuations in Brain Activity Observed with Functional Magnetic Resonance Imaging. Nat. Rev. Neurosci. 2007, 8, 700–711. [Google Scholar] [CrossRef]
- Bressler, S.L.; Menon, V. Large-Scale Brain Networks in Cognition: Emerging Methods and Principles. Trends Cogn. Sci. 2010, 14, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, L.; Halford, G.S.; Zalesky, A.; Harding, I.H.; Ramm, B.J.; Cutmore, T.; Shum, D.H.K.; Mattingley, J.B. Complexity in Relational Processing Predicts Changes in Functional Brain Network Dynamics. Cereb. Cortex 2014, 24, 2283–2296. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Kahn, I.; Snyder, A.Z.; Raichle, M.E.; Buckner, R.L. Evidence for a Frontoparietal Control System Revealed by Intrinsic Functional Connectivity. J. Neurophysiol. 2008, 100, 3328–3342. [Google Scholar] [CrossRef]
- Spadone, S.; Della Penna, S.; Sestieri, C.; Betti, V.; Tosoni, A.; Perrucci, M.G.; Romani, G.L.; Corbetta, M. Dynamic Reorganization of Human Resting-State Networks during Visuospatial Attention. Proc. Natl. Acad. Sci. USA 2015, 112, 8112–8117. [Google Scholar] [CrossRef]
- Dondé, C.; Avissar, M.; Weber, M.M.; Javitt, D.C. A Century of Sensory Processing Dysfunction in Schizophrenia. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2019, 59, 77–79. [Google Scholar] [CrossRef]
- Hoptman, M.J.; Parker, E.M.; Nair-Collins, S.; Dias, E.C.; Ross, M.E.; DiCostanzo, J.N.; Sehatpour, P.; Javitt, D.C. Sensory and Cross-Network Contributions to Response Inhibition in Patients with Schizophrenia. NeuroImage Clin. 2018, 18, 31–39. [Google Scholar] [CrossRef]
- Kebets, V.; Holmes, A.J.; Orban, C.; Tang, S.; Li, J.; Sun, N.; Kong, R.; Poldrack, R.A.; Yeo, B.T.T. Somatosensory-Motor Dysconnectivity Spans Multiple Transdiagnostic Dimensions of Psychopathology. Biol. Psychiatry 2019, 86, 779–791. [Google Scholar] [CrossRef]
- Gao, S.; Ming, Y.; Ni, S.; Kong, Z.; Wang, J.; Gu, Y.; Lu, S.; Chen, T.; Kong, M.; Sun, J.; et al. Association of Reduced Local Activities in the Default Mode and Sensorimotor Networks with Clinical Characteristics in First-Diagnosed Episode of Schizophrenia. Neuroscience 2022, 495, 47–57. [Google Scholar] [CrossRef]
- Lesh, T.A.; Tanase, C.; Geib, B.R.; Niendam, T.A.; Yoon, J.H.; Minzenberg, M.J.; Ragland, J.D.; Solomon, M.; Carter, C.S. A Multimodal Analysis of Antipsychotic Effects on Brain Structure and Function in First-Episode Schizophrenia. JAMA Psychiatry 2015, 72, 226–234. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| MNI Coordinates | ||||
|---|---|---|---|---|
| Name of RSNs | Regions of Interests (ROIs) | x | y | z |
| Default mode network (DMN) | ||||
| Medial prefrontal cortex (MPFC) | 1 | 55 | −3 | |
| Left lateral parietal (lLP) | −39 | −77 | 33 | |
| Right lateral parietal (rLP) | 47 | −67 | 29 | |
| Posterior cingulate cortex (PCC) | 1 | −61 | 38 | |
| Sensorimotor network (SMN) | ||||
| Left precentral gyrus (lPrG) | −55 | −12 | 29 | |
| Right precentral gyrus (rPrG) | 56 | −10 | 29 | |
| Middle cingulate cortex (MCC) | 0 | −31 | 67 | |
| Visual network (VN) | ||||
| Lingual gyrus (LING) | 2 | −79 | 12 | |
| Calcarine sulcus (CAL) | 0 | −93 | −4 | |
| Left middle occipital gyrus (lMOG) | −37 | −79 | 10 | |
| Right middle occipital gyrus (rMOG) | 38 | −72 | 13 | |
| Salience network (SN) | ||||
| dorsal Anterior cingulate cortex (dACC) | 0 | 22 | 35 | |
| Left anterior insula (lAI) | −44 | 13 | 1 | |
| Right anterior insula (rAI) | 47 | 14 | 0 | |
| Left rostral prefrontal cortex (lRPFC) | −32 | 45 | 27 | |
| Right rostralprefrontal cortex (rRPFC) | 32 | 46 | 27 | |
| Left supramarginal Gyrus (lSMG) | −60 | −39 | 31 | |
| Right supramarginal Gyrus (rSMG) | 62 | −35 | 32 | |
| Dorsal attention network (DAN) | ||||
| Left frontal eye field (lFEF) | −27 | −9 | 64 | |
| Right frontal eye field (rFEF) | 30 | −6 | 64 | |
| Left intraparietal sulcus (lIPS) | −39 | −43 | 52 | |
| Right intraparietal sulcus (rIPS) | 39 | −42 | 54 | |
| Frontoparietal network (FPN) | ||||
| Left lateral prefrontal cortex(lLPFC) | −43 | 33 | 28 | |
| Right lateral prefrontal cortex(rLPFC) | 41 | 38 | 30 | |
| Left posterior parietal cortex (lPPC) | −46 | −58 | 49 | |
| Right posterior parietal cortex (rPPC) | 52 | −52 | 45 | |
| Language network (LN) | ||||
| Left inferior frontal gyrus (lIFG) | −51 | 26 | 2 | |
| Right inferior frontal gyrus (rIFG) | 54 | 28 | 1 | |
| Left posterior superior temporal gyrus (lpSTG) | −57 | −47 | 15 | |
| Right posterior superior temporal gyrus (rpSTG) | 59 | −42 | 13 | |
| Cerebellar network (CN) | ||||
| Cerebellar anterior lobules (Anterior) | 0 | −63 | −30 | |
| Cerebellar posterior lobule (Posterior) | 0 | −79 | −32 | |
| SCZ | HC | p Value | |
|---|---|---|---|
| (n = 196) | (n = 169) | ||
| Gender (male/female) | 98/98 | 85/84 | 0.955 a |
| Age (years) | 25.41 ± 5.63 | 25.01 ± 4.91 | 0.63 b |
| Education (years) | 12.42 ± 2.78 | 14.79 ± 2.17 | <0.001 |
| Mean FD (mm) | 0.08 ± 0.06 | 0.07 ± 0.05 | 0.048 |
| PANSS | |||
| Total | 82.70 ± 11.62 | — | — |
| Positive symptoms | 21.21 ± 4.67 | — | — |
| Negative symptoms | 20.15 ± 5.67 | — | — |
| General psychopathology symptoms | 41.20 ± 6.81 | — | — |
| CPZ equivalents (mg/d) | 373.75 ± 283.66 | — | — |
| Duration of illness (months) | 46.23 ± 54.06 | — | — |
| Significant Connections | Functional Connectivity | T | p Value | |||
|---|---|---|---|---|---|---|
| Network | Seed Seed | Target Seed | SCZ | HC | ||
| Mean (SD) | Mean (SD) | |||||
| Intra-network Connectivity | ||||||
| DMN | MPFC | l LP | 0.2 (0.27) | 0.1 (0.25) | −3.68 | <0.01 |
| MPFC | r LP | 0.32 (0.25) | 0.22 (0.24) | −4.1 | <0.01 | |
| CN | Anterior | Posterior | 0.3 (0.25) | 0.4 (0.22) | 3.13 | <0.05 |
| Inter-network Connectivity | ||||||
| DMN-FPN | MPFC | l LPFC | −0.14 (0.24) | −0.28 (0.22) | −4.4 | <0.001 |
| MPFC | r LPFC | −0.05 (0.24) | −0.12 (0.23) | −3.77 | <0.01 | |
| MPFC | l PPC | −0.06 (0.24) | −0.17 (0.22) | −3.24 | <0.01 | |
| MPFC | r PPC | −0.01 (0.24) | −0.07 (0.23) | −2.62 | <0.05 | |
| DMN-SN | MPFC | dACC | 0.13 (0.25) | 0.23 (0.24) | 3.87 | <0.01 |
| MPFC | l AI | 0.15 (0.24) | −0.09 (0.23) | 2.56 | <0.05 | |
| MPFC | r AI | −0.13 (0.25) | −0.04 (0.23) | 2.89 | <0.05 | |
| MPFC | L RPFC | −0.08 (0.26) | −0.02 (0.22) | 2.39 | <0.05 | |
| DMN-DAN | MPFC | l IPS | −0.21 (0.22) | −0.14 (0.23) | 2.39 | <0.05 |
| MPFC | r IPS | −0.19 (0.22) | −0.11 (0.22) | 2.65 | <0.05 | |
| DMN-LN | MPFC | l IFG | −0.02 (0.26) | −0.14 (0.23) | −3.65 | <0.01 |
| PCC | l IFG | −0.14 (0.20) | −0.23 (0.21) | −3.01 | <0.05 | |
| l LP | r IFG | −0.11 (0.22) | −0.03 (0.19) | −5.3 | <0.001 | |
| r LP | r IFG | 0.07 (0.25) | −0.01 (0.22) | −2.95 | <0.05 | |
| DMN-SMN | l LP | MCC | −0.21 (0.19) | −0.11 (0.18) | 4.19 | <0.001 |
| SN-DAN | r AI | l IPS | 0.05 (0.24) | −0.05 (0.22) | −3.6 | <0.05 |
| SN-SMN | l AI | l PrG | 0.19 (0.26) | 0.08 (0.21) | −3.21 | <0.01 |
| l AI | r PrG | 0.23 (0.25) | 0.12 (0.20) | −3.73 | <0.01 | |
| l AI | MCC | −0.01 (0.21) | −0.05 (0.19) | −2.82 | <0.05 | |
| r AI | l PrG | 0.16 (0.24) | 0.08 (0.22) | −3.11 | <0.05 | |
| r AI | r PrG | 0.24 (0.25) | 0.14 (0.25) | −2.8 | <0.05 | |
| r AI | MCC | 0.02 (0.23) | −0.04 (0.20) | −2.55 | <0.05 | |
| l RPFC | l PrG | −0.04 (0.21) | −0.13 (0.19) | −3.55 | <0.05 | |
| l RPFC | r PrG | −0.01 (0.20) | −0.09 (0.19) | −2.87 | <0.05 | |
| l RPFC | MCC | −0.03 (0.21) | −0.1 (0.19) | −2.83 | <0.05 | |
| r RPFC | l PrG | −0.02 (0.21) | −0.09 (0.20) | −2.77 | <0.05 | |
| r RPFC | r PrG | −0.03 (0.22) | −0.09 (0.22) | −2.87 | <0.05 | |
| r RPFC | MCC | −0.03 (0.22) | −0.11 (0.20) | −3.31 | <0.05 | |
| l SMG | l PrG | 0.08 (0.23) | 0.01 (0.21) | −2.9 | <0.05 | |
| l SMG | r PrG | −0.13 (0.21) | 0.04 (0.22) | −3.35 | <0.05 | |
| SN-LN | r AI | r IFG | 0.29 (0.25) | 0.37 (0.25) | 3.08 | <0.05 |
| r RPFC | r IFG | 0.04 (0.24) | 0.11 (0.23) | 3.16 | <0.05 | |
| SN-CN | l RPFC | Anterior | −0.09 (0.18) | −0.04 (0.16) | 2.77 | <0.05 |
| r RPFC | Anterior | −0.09 (0.18) | −0.03 (0.18) | 3.34 | <0.05 | |
| SMN-FPN | MCC | l LPFC | −0.32 (0.19) | −0.24 (0.19) | 3.18 | <0.05 |
| SMN-DAN | MCC | r IPS | 0.3 (0.24) | 0.21 (0.24) | −2.76 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rong, B.; Huang, H.; Gao, G.; Sun, L.; Zhou, Y.; Xiao, L.; Wang, H.; Wang, G. Widespread Intra- and Inter-Network Dysconnectivity among Large-Scale Resting State Networks in Schizophrenia. J. Clin. Med. 2023, 12, 3176. https://doi.org/10.3390/jcm12093176
Rong B, Huang H, Gao G, Sun L, Zhou Y, Xiao L, Wang H, Wang G. Widespread Intra- and Inter-Network Dysconnectivity among Large-Scale Resting State Networks in Schizophrenia. Journal of Clinical Medicine. 2023; 12(9):3176. https://doi.org/10.3390/jcm12093176
Chicago/Turabian StyleRong, Bei, Huan Huang, Guoqing Gao, Limin Sun, Yuan Zhou, Ling Xiao, Huiling Wang, and Gaohua Wang. 2023. "Widespread Intra- and Inter-Network Dysconnectivity among Large-Scale Resting State Networks in Schizophrenia" Journal of Clinical Medicine 12, no. 9: 3176. https://doi.org/10.3390/jcm12093176