
A Nomogram for Predicting Surgical Timing in Neonates with Necrotizing Enterocolitis
 ,
,
Abstract
:1. Introduction
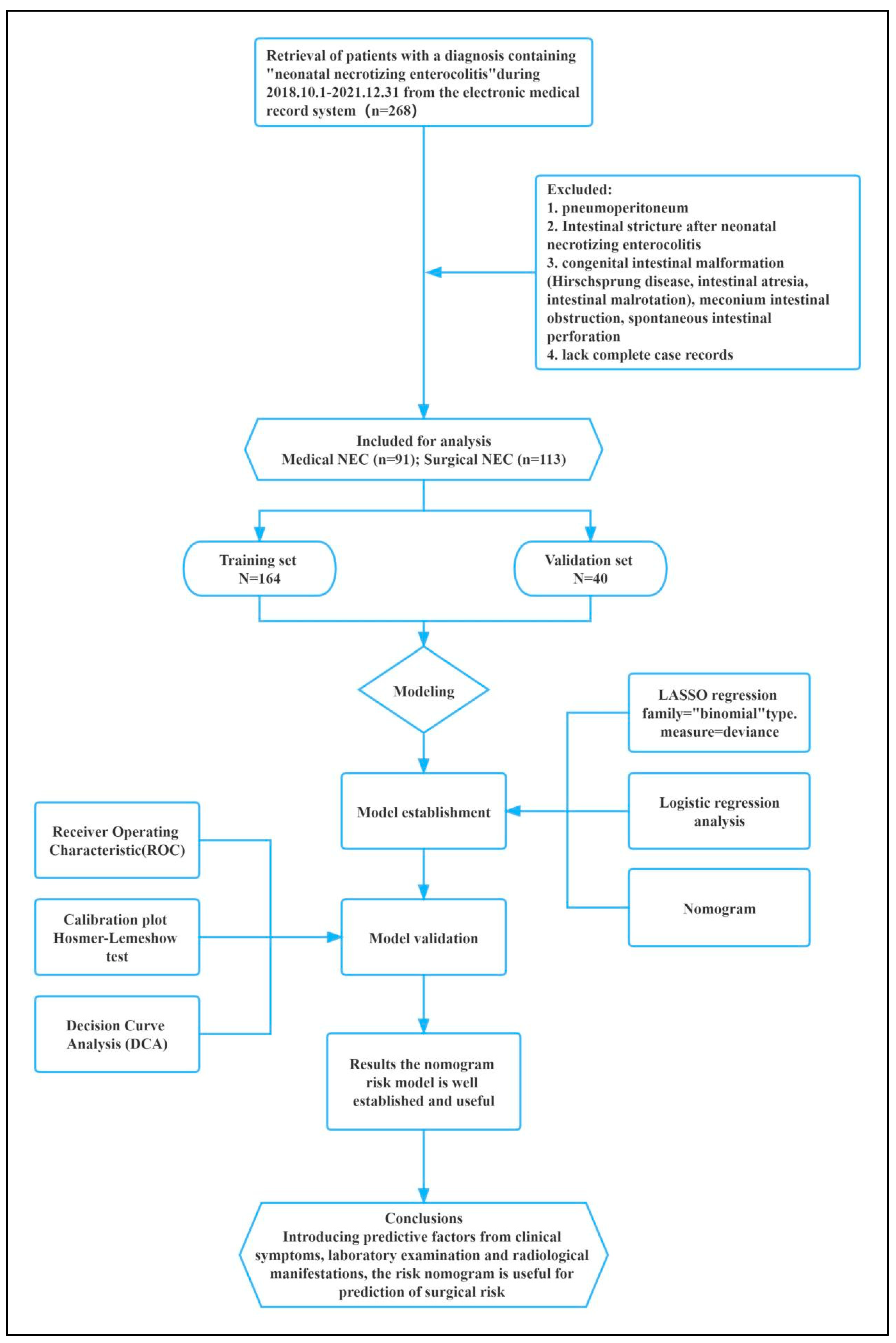
2. Materials and Methods
2.1. Patient Participants
2.2. Data Collection
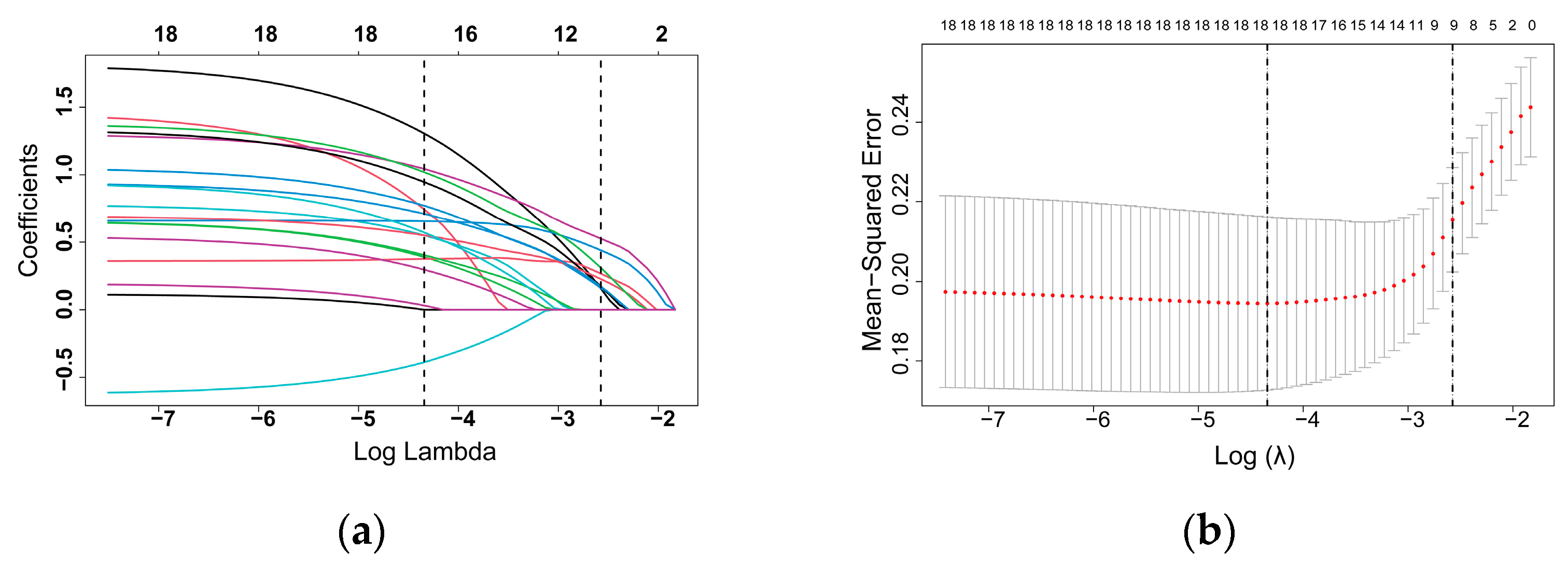
2.3. Statistical Analyses
3. Results
3.1. Patient Baseline Data
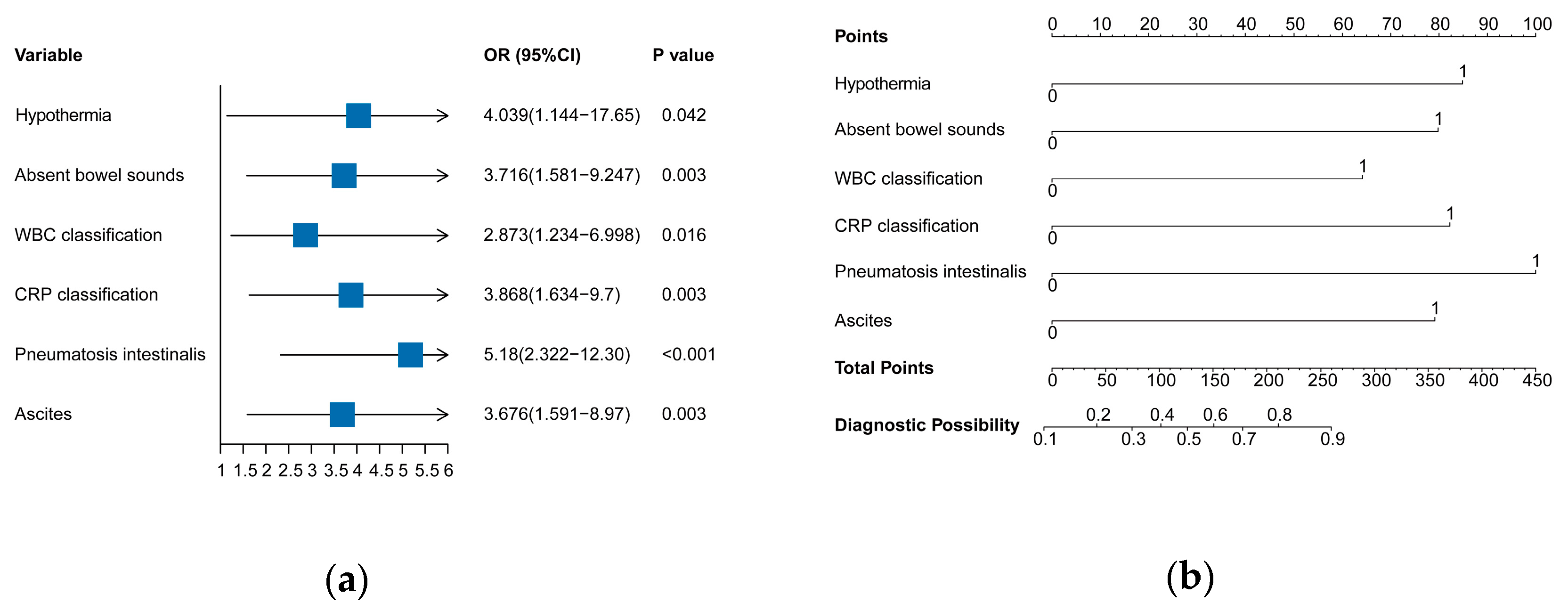
3.2. Independent Risk Factors in the Training Set
3.3. Predictive Model Construction
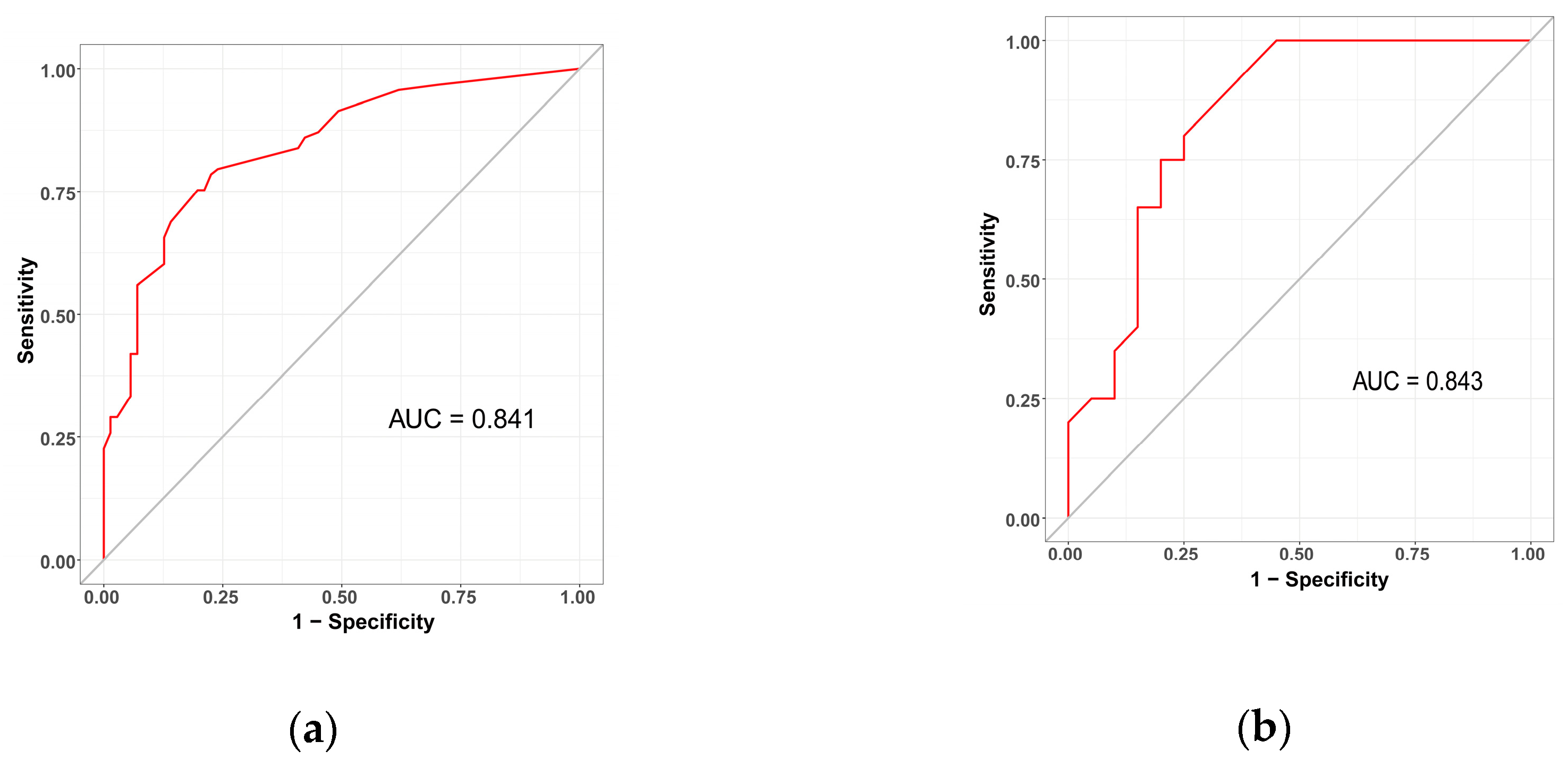
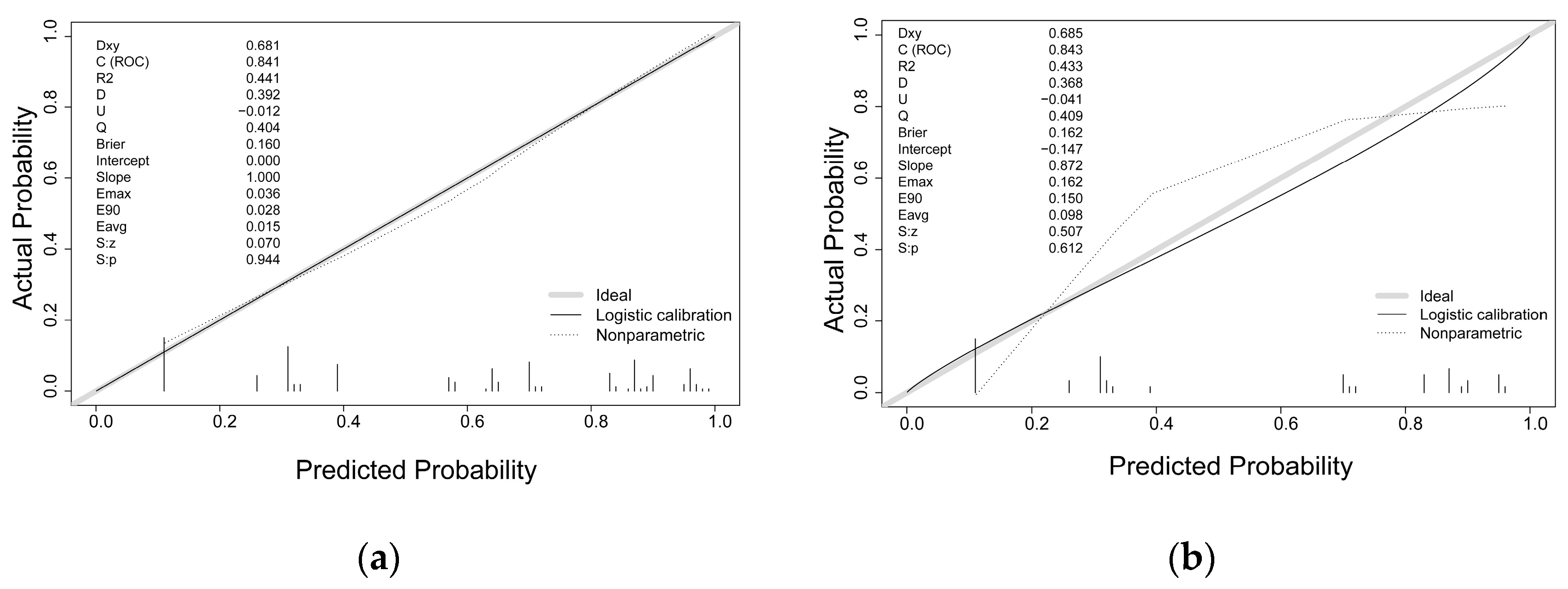
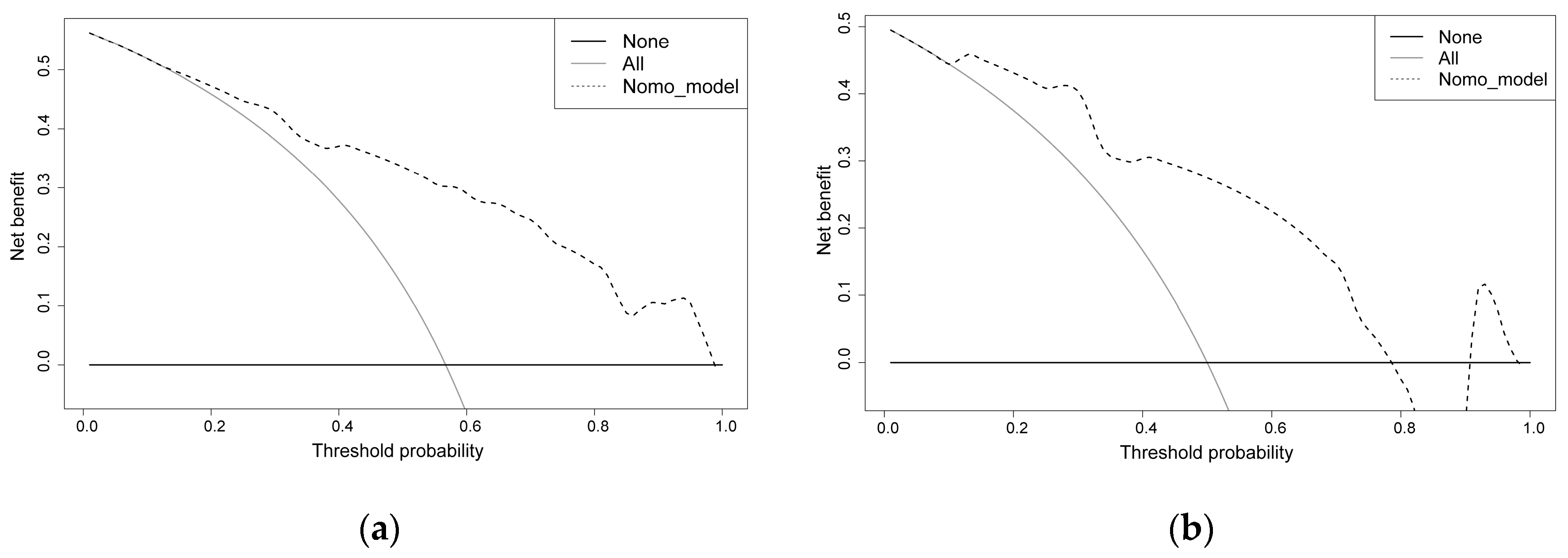
3.4. Predictive Model Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neu, J.; Walker, W.A. Necrotizing enterocolitis. N. Engl. J. Med. 2011, 364, 255–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nino, D.F.; Sodhi, C.P.; Hackam, D.J. Necrotizing enterocolitis: New insights into pathogenesis and mechanisms. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 590–600. [Google Scholar] [CrossRef] [Green Version]
- Sampah, M.; Hackam, D.J. Prenatal Immunity and Influences on Necrotizing Enterocolitis and Associated Neonatal Disorders. Front. Immunol. 2021, 12, 650709. [Google Scholar] [CrossRef] [PubMed]
- Chaaban, H.; Burge, K.; Eckert, J.; Keshari, R.S.; Silasi, R.; Lupu, C.; Warner, B.; Escobedo, M.; Caplan, M.; Lupu, F. Neutrophil extracellular trap inhibition increases inflammation, bacteraemia and mortality in murine necrotizing enterocolitis. J. Cell. Mol. Med. 2021, 25, 10814–10824. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, H.; Çetinkaya, M.; Dorum, B.A.; Köksal, N. Mesenteric tissue oxygenation status on the development of necrotizing enterocolitis. Turk. J. Pediatr. 2021, 63, 811–817. [Google Scholar] [CrossRef]
- Denning, N.L.; Prince, J.M. Neonatal intestinal dysbiosis in necrotizing enterocolitis. Mol. Med. 2018, 24, 4. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Xu, Y.; Feng, J.; Yu, J.; Huang, J.; Li, Z. Mucins and Tight Junctions are Severely Altered in Necrotizing Enterocolitis Neonates. Am. J. Perinatol. 2021, 38, 1174–1180. [Google Scholar] [CrossRef]
- Thyoka, M.; de Coppi, P.; Eaton, S.; Khoo, K.; Hall, N.J.; Curry, J.; Kiely, E.; Drake, D.; Cross, K.; Pierro, A. Advanced necrotizing enterocolitis part 1: Mortality. Eur. J. Pediatr. Surg. 2012, 22, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef]
- Jiang, S.; Yan, W.; Li, S.; Zhang, L.; Zhang, Y.; Shah, P.S.; Shah, V.; Lee, S.K.; Yang, Y.; Cao, Y. Mortality and Morbidity in Infants <34 Weeks’ Gestation in 25 NICUs in China: A Prospective Cohort Study. Front. Pediatr. 2020, 8, 33. [Google Scholar]
- Jones, I.H.; Hall, N.J. Contemporary Outcomes for Infants with Necrotizing Enterocolitis—A Systematic Review. J. Pediatr. 2020, 220, 86–92. [Google Scholar] [CrossRef]
- Zhou, J.; Ba, Y.; Du, Y.; Lin, S.B.; Chen, C. The Etiology of Neonatal Intensive Care Unit Death in Extremely Low Birth Weight Infants: A Multicenter Survey in China. Am. J. Perinatol. 2021, 38, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Hackam, D.; Caplan, M. Necrotizing enterocolitis: Pathophysiology from a historical context. Semin. Pediatr. Surg. 2018, 27, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Patel, E.U.; Wilson, D.A.; Brennan, E.A.; Lesher, A.P.; Ryan, R.M. Earlier re-initiation of enteral feeding after necrotizing enterocolitis decreases recurrence or stricture: A systematic review and meta-analysis. J. Perinatol. 2020, 40, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Arbra, C.A.; Oprisan, A.; Wilson, D.A.; Ryan, R.M.; Lesher, A.P. Time to reintroduction of feeding in infants with nonsurgical necrotizing enterocolitis. J. Pediatr. Surg. 2018, 53, 1187–1191. [Google Scholar] [CrossRef]
- Pierro, A.; Hall, N. Surgical treatments of infants with necrotizing enterocolitis. Semin. Neonatol. 2003, 8, 223–232. [Google Scholar] [CrossRef]
- Carr, B.D.; Gadepalli, S.K. Does Surgical Management Alter Outcome in Necrotizing Enterocolitis? Clin. Perinatol. 2019, 46, 89–100. [Google Scholar] [CrossRef]
- van Heesewijk, A.E.; Rush, M.L.; Schmidt, B.; Kirpalani, H.; DeMauro, S.B. Agreement between study designs: A systematic review comparing observational studies and randomized trials of surgical treatments for necrotizing enterocolitis. J. Matern. Fetal Neonatal Med. 2020, 33, 1965–1973. [Google Scholar] [CrossRef]
- Munaco, A.J.; Veenstra, M.A.; Brownie, E.; Danielson, L.A.; Nagappala, K.B.; Klein, M.D. Timing of optimal surgical intervention for neonates with necrotizing enterocolitis. Am. Surg. 2015, 81, 438–443. [Google Scholar] [CrossRef]
- Khalak, R.; D’Angio, C.; Mathew, B.; Wang, H.; Guilford, S.; Thomas, E.; Meyers, J. Physical examination score predicts need for surgery in neonates with necrotizing enterocolitis. J. Perinatol. 2018, 38, 1644–1650. [Google Scholar] [CrossRef]
- Ganji, N.; Koike, Y.; Li, B.; Zhu, H.; Lau, E.; Lok, M.J.; Lee, C.; Pierro, A. Doppler ultrasound assessment of splanchnic perfusion and heart rate for the detection of necrotizing enterocolitis. Pediatr. Surg. Int. 2021, 37, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Guang, Y.; Ying, D.; Sheng, Y.; Yiyong, F.; Jun, W.; Shuqiang, G.; Rong, J. Early Doppler Ultrasound in the Superior Mesenteric Artery and the Prediction of Necrotizing Enterocolitis in Preterm Neonates. J. Ultrasound Med. 2019, 38, 3283–3289. [Google Scholar] [CrossRef]
- Alexander, K.M.; Chan, S.S.; Opfer, E.; Cuna, A.; Fraser, J.D.; Sharif, S.; Khashu, M. Implementation of bowel ultrasound practice for the diagnosis and management of necrotising enterocolitis. Arch. Dis. Child Fetal Neonatal Ed. 2021, 106, 96–103. [Google Scholar] [CrossRef]
- Coursey, C.A.; Hollingsworth, C.L.; Wriston, C.; Beam, C.; Rice, H.; Bisset, G.R. Radiographic predictors of disease severity in neonates and infants with necrotizing enterocolitis. AJR Am. J. Roentgenol. 2009, 193, 1408–1413. [Google Scholar] [CrossRef]
- Tepas, J.R.; Sharma, R.; Leaphart, C.L.; Celso, B.G.; Pieper, P.; Esquivia-Lee, V. Timing of surgical intervention in necrotizing enterocolitis can be determined by trajectory of metabolic derangement. J. Pediatr. Surg. 2010, 45, 310–314. [Google Scholar] [CrossRef]
- Tepas, J.R.; Leaphart, C.L.; Plumley, D.; Sharma, R.; Celso, B.G.; Pieper, P.; Quilty, J.; Esquivia-Lee, V. Trajectory of metabolic derangement in infants with necrotizing enterocolitis should drive timing and technique of surgical intervention. J. Am. Coll. Surg. 2010, 210, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, J.; Ma, S.; Wang, K. Incorporating group correlations in genome-wide association studies using smoothed group Lasso. Biostatistics 2013, 14, 205–219. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zhang, L.; Liu, Z.; Wang, X.; Geng, S.; Li, J.; Li, T.; Ye, S. Predicting medication nonadherence risk in a Chinese inflammatory rheumatic disease population: Development and assessment of a new predictive nomogram. Patient Prefer. Adherence 2018, 12, 1757–1765. [Google Scholar] [CrossRef] [Green Version]
- Latti, S.; Niinivehmas, S.; Pentikainen, O.T. Rocker: Open source, easy-to-use tool for AUC and enrichment calculations and ROC visualization. J. Cheminform. 2016, 8, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inderjeeth, A.J.; Webberley, K.M.; Muir, J.; Marshall, B.J. The potential of computerised analysis of bowel sounds for diagnosis of gastrointestinal conditions: A systematic review. Syst. Rev. 2018, 7, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felder, S.; Margel, D.; Murrell, Z.; Fleshner, P. Usefulness of bowel sound auscultation: A prospective evaluation. J. Surg. Educ. 2014, 71, 768–773. [Google Scholar] [CrossRef]
- Chauhan, N.; Tiwari, S.; Jain, U. Potential biomarkers for effective screening of neonatal sepsis infections: An overview. Microb. Pathog. 2017, 107, 234–242. [Google Scholar] [CrossRef]
- Yu, L.; Tian, J.; Zhao, X.; Cheng, P.; Chen, X.; Yu, Y.; Ding, X.; Zhu, X.; Xiao, Z. Bowel Perforation in Premature Infants with Necrotizing Enterocolitis: Risk Factors and Outcomes. Gastroenterol. Res. Pract. 2016, 2016, 6134187. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Liu, G.; Feng, Z.; Huang, L. Combination of plasma white blood cell count, platelet count and C-reactive protein level for identifying surgical necrotizing enterocolitis in preterm infants without pneumoperitoneum. Pediatr. Surg. Int. 2018, 34, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Duci, M.; Fascetti-Leon, F.; Erculiani, M.; Priante, E.; Cavicchiolo, M.E.; Verlato, G.; Gamba, P. Neonatal independent predictors of severe NEC. Pediatr. Surg. Int. 2018, 34, 663–669. [Google Scholar] [CrossRef]
- Srinivasjois, R.; Nathan, E.; Doherty, D.; Patole, S. Prediction of progression of definite necrotising enterocolitis to need for surgery or death in preterm neonates. J. Matern. Fetal Neonatal Med. 2010, 23, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Eaton, S.; Puri, P.; Rintala, R.; Lukac, M.; Bagolan, P.; Kuebler, J.F.; Hoellwarth, M.E.; Wijnen, R.; Tovar, J.; et al. International survey on the management of necrotizing enterocolitis. Eur. J. Pediatr. Surg. 2015, 25, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ongun, H.; Demir, M. Mortality Caused by Late-onset Sepsis in Very Low Birth Weight Infants: Risk Analysis and the Performance of Diagnostic Tools. J. Coll. Physicians Surg. Pak. 2020, 30, 611–616. [Google Scholar] [PubMed]
- Miner, C.A.; Fullmer, S.; Eggett, D.L.; Christensen, R.D. Factors affecting the severity of necrotizing enterocolitis. J. Matern. Fetal Neonatal Med. 2013, 26, 1715–1719. [Google Scholar] [CrossRef]
- Yikilmaz, A.; Hall, N.J.; Daneman, A.; Gerstle, J.T.; Navarro, O.M.; Moineddin, R.; Pleasants, H.; Pierro, A. Prospective evaluation of the impact of sonography on the management and surgical intervention of neonates with necrotizing enterocolitis. Pediatr. Surg. Int. 2014, 30, 1231–1240. [Google Scholar] [CrossRef]
- Upadhyaya, V.D.; Gangopadhyay, A.N.; Pandey, A.; Upadhyaya, A.; Mohan, T.V.; Gopal, S.C.; Gupta, D.K. Is pneumoperitoneum an absolute indication for surgery in necrotizing enterocolitis? World J. Pediatr. 2008, 4, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Benkoe, T.; Reck, C.; Gleiss, A.; Kettner, S.; Repa, A.; Horcher, E.; Rebhandl, W. Interleukin 8 correlates with intestinal involvement in surgically treated infants with necrotizing enterocolitis. J. Pediatr. Surg. 2012, 47, 1548–1554. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Mu, F.; Gao, K.; Yan, C.; Chen, G.; Guo, C. Value of abdominal ultrasonography in predicting intestinal resection for premature infants with necrotizing enterocolitis. BMC Gastroenterol. 2022, 22, 524. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.W.; Poon, T.C.; Lam, H.S.; Cheung, H.M.; Ma, T.P.; Chan, K.Y.; Wong, R.P.; Leung, K.T.; Lam, M.M.; Li, K.; et al. Gut-associated biomarkers L-FABP, I-FABP, and TFF3 and LIT score for diagnosis of surgical necrotizing enterocolitis in preterm infants. Ann. Surg. 2013, 258, 1111–1118. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALL Patients (N = 204) | Medical NEC (N = 91) | Surgical NEC (N = 113) | p Value | |
|---|---|---|---|---|
| Basic information | ||||
| Gender, n (%) | 0.140 | |||
| Male | 115 (56.4%) | 57 (62.6%) | 58 (51.3%) | |
| Female | 89 (43.6%) | 34 (37.4%) | 55 (48.7%) | |
| Delivery method, n (%) | 0.258 | |||
| Vaginal | 71 (34.8%) | 36 (39.6%) | 35 (31.0%) | |
| Cesarean section | 133 (65.2%) | 55 (60.4%) | 78 (69.0%) | |
| Gestational age (weeks) | 32.0 [29.0;35.0] | 33.0 [30.0;35.5] | 31.0 [28.0;34.0] | 0.002 |
| Gestational age (weeks) | 0.024 | |||
| ≥37 | 31 (15.2%) | 15 (16.5%) | 16 (14.2%) | |
| 32–36 | 65 (31.9%) | 24 (26.4%) | 41 (36.3%) | |
| 28–31 | 81 (39.7%) | 45 (49.5%) | 36 (31.9%) | |
| <28 | 27 (13.2%) | 7 (7.69%) | 20 (17.7%) | |
| Birth weight (g) | 1735 [1280;2300] | 2000 [1550;2412] | 1500 [1200;2160] | 0.001 |
| Birth weight (g) | 0.002 | |||
| ≥2500 | 38 (18.6%) | 19 (20.9%) | 19 (16.8%) | |
| 1500–2499 | 50 (24.5%) | 13 (14.3%) | 37 (32.7%) | |
| 1000–1499 | 90 (44.1%) | 51 (56.0%) | 39 (34.5%) | |
| <1000 g | 26 (12.7%) | 8 (8.79%) | 18 (15.9%) | |
| Admission age (d) | 13.0 [5.00;23.2] | 12.0 [4.00;22.0] | 13.0 [8.00;25.0] | 0.116 |
| Onset age (d) | 11.0 [7.00;19.2] | 11.0 [6.50;17.5] | 12.0 [7.00;20.0] | 0.314 |
| Apgar 1 min, n (%) | 9.00 [8.00;10.0] | 9.00 [8.50;10.0] | 9.00 [8.00;10.0] | 0.026 |
| Apgar 1 min classification | 0.223 | |||
| 8–10 | 164 (80.4%) | 77 (84.6%) | 87 (77.0%) | |
| 4–7 | 37 (18.1%) | 14 (15.4%) | 23 (20.4%) | |
| 1–3 | 3 (1.47%) | 0 (0.00%) | 3 (2.65%) | |
| Asphyxia, n (%) | <0.001 | |||
| No | 102 (50.0%) | 61 (67.0%) | 41 (36.3%) | |
| Yes | 102 (50.0%) | 30 (33.0%) | 72 (63.7%) | |
| Clinical manifestations | ||||
| Hypothermia, n (%) | 0.010 | |||
| No | 181 (88.7%) | 87 (95.6%) | 94 (83.2%) | |
| Yes | 23 (11.3%) | 4 (4.40%) | 19 (16.8%) | |
| Abdominal distention, n (%) | 0.002 | |||
| No | 46 (22.5%) | 30 (33.0%) | 16 (14.2%) | |
| Yes | 158 (77.5%) | 61 (67.0%) | 97 (85.8%) | |
| Hematochezia, n (%) | 0.058 | |||
| No | 45 (22.1%) | 14 (15.4%) | 31 (27.4%) | |
| Yes | 159 (77.9%) | 77 (84.6%) | 82 (72.6%) | |
| Diarrhea, n (%) | 1.000 | |||
| No | 199 (97.5%) | 89 (97.8%) | 110 (97.3%) | |
| Yes | 5 (2.45%) | 2 (2.20%) | 3 (2.65%) | |
| Emesis, n (%) | 0.056 | |||
| No | 169 (82.8%) | 81 (89.0%) | 88 (77.9%) | |
| Yes | 35 (17.2%) | 10 (11.0%) | 25 (22.1%) | |
| Absent bowel sounds, n (%) | <0.001 | |||
| No | 141 (69.1%) | 75 (82.4%) | 66 (58.4%) | |
| Yes | 63 (30.9%) | 16 (17.6%) | 47 (41.6%) | |
| Laboratory examination | ||||
| WBC (109/L) | 7.84 [4.73;11.2] | 8.85 [6.81;11.7] | 5.91 [3.24;10.8] | <0.001 |
| WBC classification | <0.001 | |||
| 5–20 × 109/L | 137 (67.2%) | 74 (81.3%) | 63 (55.8%) | |
| >20 × 109/L or <5 × 109/L | 67 (32.8%) | 17 (18.7%) | 50 (44.2%) | |
| N, n (%) | 53.1 [40.3;69.6] | 44.1 [34.0;61.5] | 59.3 [46.9;71.8] | <0.001 |
| N classification | 0.041 | |||
| ≤75% | 176 (86.3%) | 84 (92.3%) | 92 (81.4%) | |
| >75% | 28 (13.7%) | 7 (7.69%) | 21 (18.6%) | |
| CRP (mg/L) | 23.5 [1.39;62.8] | 1.69 [0.50;22.5] | 50.0 [21.2;88.5] | <0.001 |
| CRP classification | <0.001 | |||
| <50 mg/L | 134 (65.7%) | 78 (85.7%) | 56 (49.6%) | |
| ≥50 mg/L | 70 (34.3%) | 13 (14.3%) | 57 (50.4%) | |
| PLT (109/L) | 202 [118;302] | 245 [184;367] | 177 [103;246] | <0.001 |
| PLT classification | 0.006 | |||
| ≥100 × 109/L | 171 (83.8%) | 84 (92.3%) | 87 (77.0%) | |
| <100 × 109/L | 33 (16.2%) | 7 (7.69%) | 26 (23.0%) | |
| PT * (s) | 14.1 [12.9;17.0] | 13.6 [12.8;14.9] | 15.1 [13.2;18.3] | <0.001 |
| PT * classification | <0.001 | |||
| <17 s | 140 (74.1%) | 68 (88.3%) | 72 (64.3%) | |
| ≥17 s | 49 (25.9%) | 9 (11.7%) | 40 (35.7%) | |
| APTT * (s) | 53.0 [46.1;74.4] | 49.5 [40.3;59.7] | 58.0 [49.2;80.6] | <0.001 |
| APTT * classification | 0.002 | |||
| <70 s | 138 (73.0%) | 66 (85.7%) | 72 (64.3%) | |
| ≥70 s | 51 (27.0%) | 11 (14.3%) | 40 (35.7%) | |
| pH | 7.37 [7.31;7.42] | 7.40 [7.36;7.44] | 7.34 [7.25;7.40] | <0.001 |
| Acidosis (pH < 7.35) | <0.001 | |||
| No | 125 (61.3%) | 71 (78.0%) | 54 (47.8%) | |
| Yes | 79 (38.7%) | 20 (22.0%) | 59 (52.2%) | |
| Lac (mmol/L) | 2.40 [1.50;3.40] | 2.40 [1.75;3.25] | 2.30 [1.40;3.50] | 0.377 |
| Lac classification | 0.079 | |||
| ≤1.6 mmol/L | 61 (29.9%) | 21 (23.1%) | 40 (35.4%) | |
| >1.6 mmol/L | 143 (70.1%) | 70 (76.9%) | 73 (64.6%) | |
| Radiological manifestations | ||||
| Intestinal dilation, n (%) | 0.057 | |||
| No | 57 (27.9%) | 32 (35.2%) | 25 (22.1%) | |
| Yes | 147 (72.1%) | 59 (64.8%) | 88 (77.9%) | |
| Ascites, n (%) | 0.001 | |||
| No | 129 (63.2%) | 69 (75.8%) | 60 (53.1%) | |
| Yes | 75 (36.8%) | 22 (24.2%) | 53 (46.9%) | |
| Intestinal stiffness, n (%) | <0.001 | |||
| No | 104 (51.0%) | 60 (65.9%) | 44 (38.9%) | |
| Yes | 100 (49.0%) | 31 (34.1%) | 69 (61.1%) | |
| Pneumatosis intestinalis, n (%) | <0.001 | |||
| No | 126 (61.8%) | 70 (76.9%) | 56 (49.6%) | |
| Yes | 78 (38.2%) | 21 (23.1%) | 57 (50.4%) | |
| Ileus, n (%) | 0.741 | |||
| No | 158 (77.5%) | 69 (75.8%) | 89 (78.8%) | |
| Yes | 46 (22.5%) | 22 (24.2%) | 24 (21.2%) | |
| Portal pneumatosis, n (%) | 0.021 | |||
| No | 177 (86.8%) | 85 (93.4%) | 92 (81.4%) | |
| Yes | 27 (13.2%) | 6 (6.59%) | 21 (18.6%) |
| Characteristics | Uni-B | Uni-SE | Uni-OR | Uni-CI | Uni-P | Multi-B | Multi-SE | Multi-OR | Multi-CI | Multi-P |
|---|---|---|---|---|---|---|---|---|---|---|
| Hypothermia | 1.247 | 0.58345 | 3.481 | 1.109–10.922 | 0.033 | 1.71 | 0.76935 | 5.527 | 1.224–24.968 | 0.026 |
| Absent bowel sounds | 1.214 | 0.37153 | 3.367 | 1.626–6.975 | 0.001 | 1 | 0.49527 | 2.717 | 1.029–7.173 | 0.044 |
| WBC classification | 1.123 | 0.36447 | 3.073 | 1.504–6.277 | 0.002 | 0.993 | 0.49895 | 2.698 | 1.015–7.175 | 0.047 |
| CRP classification | 1.632 | 0.38811 | 5.114 | 2.39–10.942 | <0.001 | 1.089 | 0.50494 | 2.972 | 1.105–7.996 | 0.031 |
| PT classification | 1.544 | 0.45618 | 4.684 | 1.915–11.452 | 0.001 | 0.867 | 0.57066 | 2.38 | 0.778–7.285 | 0.129 |
| Acidosis | 1.603 | 0.37054 | 4.969 | 2.403–10.272 | <0.001 | 0.903 | 0.47685 | 2.468 | 0.969–6.284 | 0.058 |
| Ascites | 1.048 | 0.3471 | 2.852 | 1.445–5.632 | 0.003 | 1.301 | 0.50546 | 3.671 | 1.363–9.887 | 0.01 |
| Intestinal stiffness | 1.087 | 0.32837 | 2.964 | 1.557–5.641 | 0.001 | 0.8 | 0.44533 | 2.225 | 0.93–5.326 | 0.073 |
| Pneumatosis intestinalis | 1.299 | 0.35176 | 3.667 | 1.84–7.306 | <0.001 | 1.347 | 0.46464 | 3.845 | 1.547–9.56 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, B.; Shen, L.; Huang, W.; Cai, L.; Yang, S.; Zhang, Y.; Tou, J.; Lai, D. A Nomogram for Predicting Surgical Timing in Neonates with Necrotizing Enterocolitis. J. Clin. Med. 2023, 12, 3062. https://doi.org/10.3390/jcm12093062
Shi B, Shen L, Huang W, Cai L, Yang S, Zhang Y, Tou J, Lai D. A Nomogram for Predicting Surgical Timing in Neonates with Necrotizing Enterocolitis. Journal of Clinical Medicine. 2023; 12(9):3062. https://doi.org/10.3390/jcm12093062
Chicago/Turabian StyleShi, Bo, Leiting Shen, Wenchang Huang, Linghao Cai, Sisi Yang, Yuanyuan Zhang, Jinfa Tou, and Dengming Lai. 2023. "A Nomogram for Predicting Surgical Timing in Neonates with Necrotizing Enterocolitis" Journal of Clinical Medicine 12, no. 9: 3062. https://doi.org/10.3390/jcm12093062